Altered Phosphorylation of Cytoskeleton Proteins in Peripheral Blood Mononuclear Cells Characterizes Chronic Antibody-Mediated Rejection in Kidney Transplantation

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Results
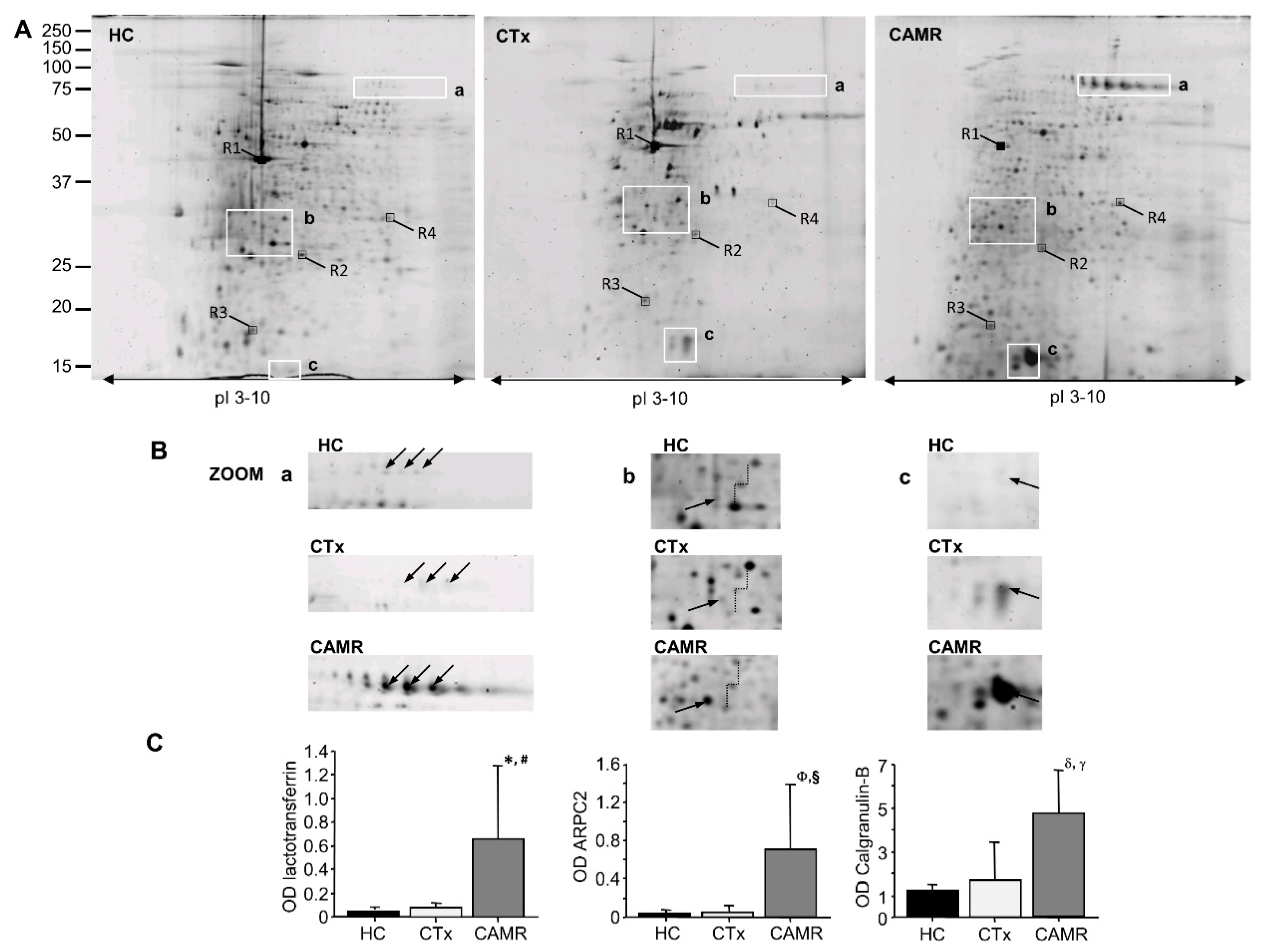
2.1. Phosphorylation of ARPC2 Was Increased in Patients with Chronic Antibody-Mediated Rejection
2.2. ARPC2 Phosphorylation Is Correlated to Derangement of F-Actin Filaments in Patients with Chronic Antibody-Mediated Rejection
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Patients
4.3. PBMCs Isolation and Total Proteins Extraction
4.4. Phosphoproteins Isolation
4.5. Western Blot Analysis
4.6. Confocal Microscopy
4.7. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Sellarés, J.; De Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P. Understanding the Causes of Kidney Transplant Failure: The Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Einecke, G.; Sis, B.; Reeve, J.; Mengel, M.; Campbell, P.M.; Hidalgo, L.G.; Kaplan, B.; Halloran, P. Antibody-Mediated Microcirculation Injury Is the Major Cause of Late Kidney Transplant Failure. Am. J. Transplant. 2009, 9, 2520–2531. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Sis, B.; Racusen, L.C.; Solez, K.; Glotz, D.; Colvin, R.B.; De Castro, M.C.R.; David, D.S.R.; David-Neto, E.; Bagnasco, S.M.; et al. Banff 2013 Meeting Report: Inclusion of C4d-Negative Antibody-Mediated Rejection and Antibody-Associated Arterial Lesions. Am. J. Transplant. 2014, 14, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Ivanyi, B. Transplant capillaropathy and transplant glomerulopathy: Ultrastructural markers of chronic renal allograft rejection. Nephrol. Dial. Transplant. 2003, 18, 655–660. [Google Scholar] [CrossRef] [Green Version]
- Naik, R.H.; Shawar, S.H. Renal Transplantation Rejection; StatPearls Publishing LLC: Treasure Island, FL, USA, 2020. [Google Scholar]
- Colvin, R.B. Antibody-Mediated Renal Allograft Rejection: Diagnosis and Pathogenesis. J. Am. Soc. Nephrol. 2007, 18, 1046–1056. [Google Scholar] [CrossRef] [Green Version]
- Sablik, K.A.; Jordanova, E.S.; Pocorni, N.; Groningen, M.C.C.-V.; Betjes, M.G.H. Immune Cell Infiltrate in Chronic-Active Antibody-Mediated Rejection. Front. Immunol. 2020, 10. [Google Scholar] [CrossRef] [Green Version]
- Rascio, F.; Pontrelli, P.; Accetturo, M.; Oranger, A.; Gigante, M.; Castellano, G.; Gigante, M.; Zito, A.; Zaza, G.; Lupo, A.; et al. A type I interferon signature characterizes chronic antibody-mediated rejection in kidney transplantation. J. Pathol. 2015, 237, 72–84. [Google Scholar] [CrossRef]
- Sharbafi, M.H.; Assadiasl, S.; Pour-Reza-Gholi, F.; Barzegari, S.; Torbati, P.M.; Samavat, S.; Nicknam, M.H.; Amirzargar, A. TLR-2, TLR-4 and MyD88 genes expression in renal transplant acute and chronic rejections. Int. J. Immunogenet. 2019, 46, 427–436. [Google Scholar] [CrossRef]
- Danger, R.; Paul, C.; Giral, M.; Lavault, A.; Foucher, Y.; Degauque, N.; Pallier, A.; Durand, M.; Castagnet, S.; Van Huyen, J.-P.D.; et al. Expression of miR-142-5p in Peripheral Blood Mononuclear Cells from Renal Transplant Patients with Chronic Antibody-Mediated Rejection. PLoS ONE 2013, 8, e60702. [Google Scholar] [CrossRef] [Green Version]
- Cravatt, B.F.; Simon, G.M.; Iii, J.R.Y. The biological impact of mass-spectrometry-based proteomics. Nature 2007, 450, 991–1000. [Google Scholar] [CrossRef]
- Lo, D.J.; Kaplan, B.; Kirk, A.D. Biomarkers for kidney transplant rejection. Nat. Rev. Nephrol. 2014, 10, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Su, W.; Chen, H.; Chen, D.-Q.; Wang, M.; Guo, Y.; Zhao, Y.-Y. Proteomics for Biomarker Identification and Clinical Application in Kidney Disease. Adv. Clin. Chem. 2018, 85, 91–113. [Google Scholar] [PubMed]
- Hirt-Minkowski, P.; De Serres, S.; Ho, J. Developing renal allograft surveillance strategies-urinary biomarkers of cellular rejection. Can. J. Kidney Health Dis. 2015, 2, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, T. Signaling—2000 and Beyond. Cell 2000, 100, 113–127. [Google Scholar] [CrossRef] [Green Version]
- Siqueiros-Cendón, T.; Arévalo-Gallegos, S.; Iglesias-Figueroa, B.F.; García-Montoya, I.A.; Salazar-Martínez, J.; Rascón-Cruz, Q. Immunomodulatory effects of lactoferrin. Acta Pharmacol. Sin. 2014, 35, 557–566. [Google Scholar] [CrossRef]
- Actor, J.K.; Hwang, S.-A.; Kruzel, M.L. Lactoferrin as a Natural Immune Modulator. Curr. Pharm. Des. 2009, 17, 1956–1973. [Google Scholar] [CrossRef] [Green Version]
- Pavón, E.J.; García-Rodríguez, S.; Zumaquero, E.; Perandrés-López, R.; Rosal-Vela, A.; Lario, A.; Longobardo, V.; Carrascal, M.; Abian, J.; Callejas-Rubio, J.-L.; et al. Increased expression and phosphorylation of the two S100A9 isoforms in mononuclear cells from patients with systemic lupus erythematosus: A proteomic signature for circulating low-density granulocytes. J. Proteom. 2012, 75, 1778–1791. [Google Scholar] [CrossRef] [Green Version]
- Nakorchevsky, A.; Hewel, J.A.; Kurian, S.; Mondala, T.S.; Campbell, D.; Head, S.R.; Marsh, C.L.; Yates, J.R.; Salomon, D.R. Molecular mechanisms of chronic kidney transplant rejection via large-scale proteogenomic analysis of tissue biopsies. J. Am. Soc. Nephrol. 2010, 21, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, L.A.; Svane, A.M.; Burton, M.; Bistrup, C.; Thiesson, H.C.; Marcussen, N.; Beck, H.C. Proteomic Analysis of Renal Biomarkers of Kidney Allograft Fibrosis—A Study in Renal Transplant Patients. Int. J. Mol. Sci. 2020, 21, 2371. [Google Scholar] [CrossRef] [Green Version]
- Trost, M.; Sauvageau, M.; Herault, O.; Deleris, P.; Pomiès, C.; Chagraoui, J.; Mayotte, N.; Meloche, S.; Sauvageau, G.; Thibault, P. Posttranslational regulation of self-renewal capacity: Insights from proteome and phosphoproteome analyses of stem cell leukemia. Blood 2012, 120, e17–e27. [Google Scholar] [CrossRef]
- Rigbolt, K.T.G.; Prokhorova, T.A.; Akimov, V.; Henningsen, J.; Johansen, P.T.; Kratchmarova, I.; Kassem, M.; Mann, M.; Olsen, J.V.; Blagoev, B. System-Wide Temporal Characterization of the Proteome and Phosphoproteome of Human Embryonic Stem Cell Differentiation. Sci. Signal. 2011, 4, rs3. [Google Scholar] [CrossRef] [PubMed]
- Welch, M.D.; DePace, A.H.; Verma, S.; Iwamatsu, A.; Mitchison, T.J. The Human Arp2/3 Complex Is Composed of Evolutionarily Conserved Subunits and Is Localized to Cellular Regions of Dynamic Actin Filament Assembly. J. Cell Biol. 1997, 138, 375–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, M.D.; Mullins, R.D. Cellular Control of Actin Nucleation. Annu. Rev. Cell Dev. Biol. 2002, 18, 247–288. [Google Scholar] [CrossRef] [PubMed]
- Egile, C.; Rouiller, I.; Xu, X.-P.; Volkmann, N.; Li, R.; Hanein, D. Mechanism of filament nucleation and branch stability revealed by the structure of the Arp2/3 complex at actin branch junctions. PLoS Biol. 2005, 3, e383. [Google Scholar] [CrossRef]
- Burat, B.; Faucher, Q.; Čechová, P.; Arnion, H.; Di Meo, F.; Sauvage, F.; Marquet, P.; Essig, M. Cyclosporine A inhibits MRTF-SRF signaling through Na+/K+ ATPase inhibition and actin remodeling. FASEB BioAdv. 2019, 1, 561–578. [Google Scholar] [CrossRef] [Green Version]
- Goley, E.D.; Welch, M.D. The ARP2/3 complex: An actin nucleator comes of age. Nat. Rev. Mol. Cell Biol. 2006, 7, 713–726. [Google Scholar] [CrossRef]
- Thrasher, A.J.; Burns, S.O. WASP: A key immunological multitasker. Nat. Rev. Immunol. 2010, 10, 182–192. [Google Scholar] [CrossRef]
- Bosticardo, M.; Marangoni, F.; Aiuti, A.; Villa, A.; Roncarolo, M.G. Recent advances in understanding the pathophysiology of Wiskott-Aldrich syndrome. Blood 2009, 113, 6288–6295. [Google Scholar] [CrossRef] [Green Version]
- Dustin, M.L. The Cellular Context of T Cell Signaling. Immunity 2009, 30, 482–492. [Google Scholar] [CrossRef] [Green Version]
- Batista, F.D.; Harwood, N.E. The who, how and where of antigen presentation to B cells. Nat. Rev. Immunol. 2009, 9, 15–27. [Google Scholar] [CrossRef]
- Cotta-De-Almeida, V.; Westerberg, L.S.; Maillard, M.H.; Onaldi, D.; Wachtel, H.; Meelu, P.; Chung, U.-I.; Xavier, R.; Alt, F.W.; Snapper, S.B. Wiskott Aldrich syndrome protein (WASP) and N-WASP are critical for T cell development. Proc. Natl. Acad. Sci. USA 2007, 104, 15424–15429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westerberg, L.S.; Larsson, M.; Hardy, S.J.; Fernández, C.; Thrasher, A.J.; Severinson, E. Wiskott-Aldrich syndrome protein deficiency leads to reduced B-cell adhesion, migration, and homing, and a delayed humoral immune response. Blood 2005, 105, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.L.; Burkhardt, J.K. Differential roles for Wiskott-Aldrich syndrome protein in immune synapse formation and IL-2 production. J. Immunol. 2004, 173, 1658–1662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castiello, M.C.; Bosticardo, M.; Pala, F.; Catucci, M.; Chamberlain, N.; Van Zelm, M.C.; Driessen, G.J.; Pac, M.; Bernatowska, E.; Scaramuzza, S.; et al. Wiskott-Aldrich Syndrome protein deficiency perturbs the homeostasis of B-cell compartment in humans. J. Autoimmun. 2013, 50, 42–50. [Google Scholar] [CrossRef]
- Lisik, W.; Tejpal, N.; Gong, Y.; Skelton, T.S.; Ganachari, M.; Bremer, E.G.; Kloc, M.; Ghobrial, R.M. Down Regulation of Genes Involved in T Cell Polarity and Motility during the Induction of Heart Allograft Tolerance by Allochimeric MHC I. PLoS ONE 2009, 4, e8020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, S.; Xie, S.; Lv, D.; Zhang, Y.; Deng, J.; Zeng, L.; Chen, Y. A reduction in the butyrate producing species Roseburia spp. and Faecalibacterium prausnitzii is associated with chronic kidney disease progression. Antonie van Leeuwenhoek Int. J. Gen. Mol. Microbiol. 2016, 109, 1389–1396. [Google Scholar] [CrossRef] [PubMed]
- Mengel, M.; Sis, B.; Haas, M.; Colvin, R.B.; Halloran, P.; Racusen, L.C.; Solez, K.; Cendales, L.; Demetris, A.J.; Drachenberg, C.B.; et al. Banff 2011 Meeting report: New concepts in antibody-mediated rejection. Am. J. Transplant. 2012, 12, 563–570. [Google Scholar] [CrossRef]
- Rocchetti, M.T.; Alfarano, M.; Varraso, L.; Di Paolo, S.; Papale, M.; Ranieri, E.; Grandaliano, G.; Gesualdo, L. Two dimensional gel phosphoproteome of peripheral blood mononuclear cells: Comparison between two enrichment methods. Proteome Sci. 2014, 12, 46. [Google Scholar] [CrossRef] [Green Version]
- Rocchetti, M.T.; Centra, M.; Papale, M.; Bortone, G.; Palermo, C.; Centonze, D.; Ranieri, E.; Di Paolo, S.; Gesualdo, L. Urine protein profile of IgA nephropathy patients may predict the response to ACE-inhibitor therapy. Proteomics 2008, 8, 206–216. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CAMR-GROUP | CTRL-GROUP | p-Value | |
|---|---|---|---|
| Number (patients) | 16 | 11 | |
| Age (years) | 44.4 ± 8.7 | 53.1 ± 14.2 | NS |
| Gender (M/F) | 9/7 | 6/5 | |
| Time since transplantation (months) | 7 ± 5.8 | 8.9 ± 6.9 | NS |
| Serum creatinine (mg/dl) | 1.9 ± 0.6 | 1.2 ± 0.4 | 0.02 |
| Proteinuria (g/24h) | 2.6 ± 2.5 | 0.42 ± 0.7 | 0.01 |
| Cyclosporine | 7 | 3 | - |
| Tacrolimus | 9 | 8 | - |
| Number of mismatches HLA | 3 ± 0.6 | 2.5 ± 0.5 | NS |
| Anti HLA antibodies (%) | 100% | 15% | - |
| Banff Score Chronic Glomerulopathy | 0: 38%; 1: 9%; 2:15%; 3: 38% | 0: 100% | - |
| Banf Score Peritubular Capillaries | 0: 65%; 1: 14%; 2: 21%; 3: 0% | 0: 100% | - |
| Glomerulitis Banff Lesion Score | 0: 45%; 1: 25%; 2: 20%; 3: 10% | 0: 100% | - |
| Interstitial Fibrosis Banff Lesion Score | 0: 0%; 1: 40%; 2: 50%; 3: 10% | 0:80%; 1: (20%) | - |
| Tubular atrophy Banff Lesion Score | 0: 0%; 1: 41%; 2: 50%; 3: 9% | 0:80%; 1: (20%) | - |
| C4d positive | 65% | 0% |
| Protein Name (GENE Name) | Accession Number | Molecular Weight (Da) | Mascot Score | Seq. Cov. (%) | P Value a CAMR vs. CTx (Fold Change) | P Value a CAMR vs. HC (Fold Change) |
|---|---|---|---|---|---|---|
| Lactotransferrin (LTF) | P02788 | 80014 | 257 | 41 | 0.01 (10.1) | 0.01 (19.1) |
| Actin-related protein 2/3 complex subunit 2 (ARPC2) | O15144 | 34333 | 97 | 30 | 0.0005 (3.4) | 0.0006 (3.2) |
| Calgranulin-B (S10A9) | P06702 | 13291 | 122 | 79 | 0.03 (2.7) | 0.02 (3.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocchetti, M.T.; Rascio, F.; Castellano, G.; Fiorentino, M.; Netti, G.S.; Spadaccino, F.; Ranieri, E.; Gallone, A.; Gesualdo, L.; Stallone, G.; et al. Altered Phosphorylation of Cytoskeleton Proteins in Peripheral Blood Mononuclear Cells Characterizes Chronic Antibody-Mediated Rejection in Kidney Transplantation. Int. J. Mol. Sci. 2020, 21, 6509. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186509
Rocchetti MT, Rascio F, Castellano G, Fiorentino M, Netti GS, Spadaccino F, Ranieri E, Gallone A, Gesualdo L, Stallone G, et al. Altered Phosphorylation of Cytoskeleton Proteins in Peripheral Blood Mononuclear Cells Characterizes Chronic Antibody-Mediated Rejection in Kidney Transplantation. International Journal of Molecular Sciences. 2020; 21(18):6509. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186509
Chicago/Turabian StyleRocchetti, Maria Teresa, Federica Rascio, Giuseppe Castellano, Marco Fiorentino, Giuseppe Stefano Netti, Federica Spadaccino, Elena Ranieri, Anna Gallone, Loreto Gesualdo, Giovanni Stallone, and et al. 2020. "Altered Phosphorylation of Cytoskeleton Proteins in Peripheral Blood Mononuclear Cells Characterizes Chronic Antibody-Mediated Rejection in Kidney Transplantation" International Journal of Molecular Sciences 21, no. 18: 6509. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186509