Platelets, Thrombocytosis, and Ovarian Cancer Prognosis: Surveying the Landscape of the Literature

 ,
,
Abstract
:1. Introduction
2. Pretreatment Thrombocytosis and Associations with Survival
2.1. Pretreatment Thrombocytosis and Associations with Survival: Timing of Platelet Count Measurement
2.2. Pretreatment Thrombocytosis and Associations with Survival: Thresholds Below 400
2.3. Pretreatment Thrombocytosis and Associations with Survival: Thresholds of 400
2.4. Pretreatment Thrombocytosis and Associations with Survival: Thresholds Above 400
2.5. Pretreatment Thrombocytosis and Associations with Survival: Multiple Thresholds and Continuous Measures
2.6. Pretreatment Thrombocytosis and Associations with Survival: Multivariable Adjustment
3. Thrombocytosis after Primary Treatment and Associations with Survival
3.1. Thrombocytosis Following Chemotherapy and Associations with Survival
3.2. Thrombocytosis at Disease Recurrence and Associations with Survival
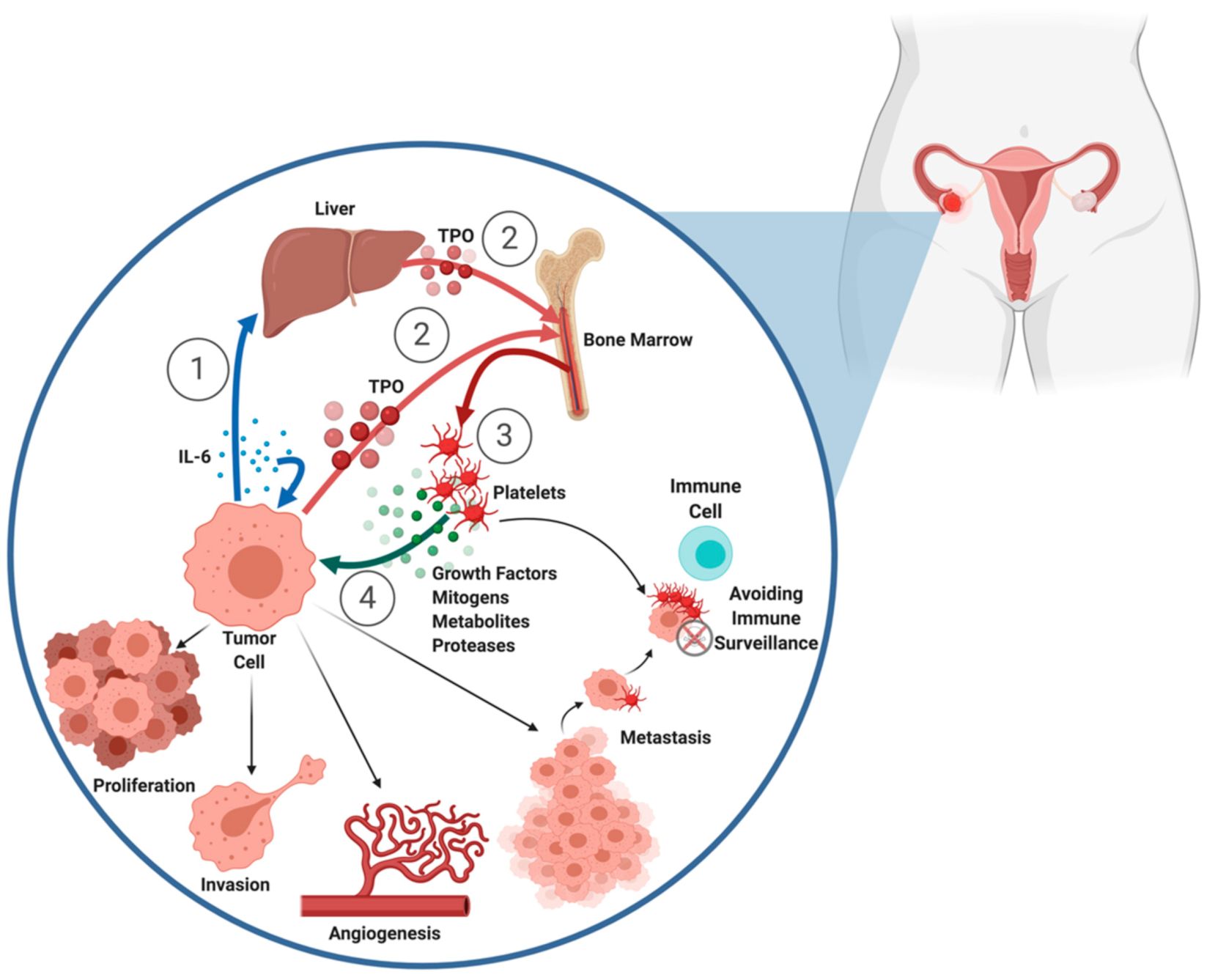
4. Mechanisms Underlying Associations of Thrombocytosis with Disease Progression
4.1. Cytokine-Driven Development of Thrombocytosis in Ovarian Cancer
4.2. Contributions of Platelets to Ovarian Cancer Progression: In Vitro and In Vivo Studies
4.3. Contributions of Platelets to Ovarian Cancer Progression: Ex Vivo Studies
4.4. Contributions of Platelets to Ovarian Cancer Progression: Clinical Data
5. Conclusions: Incorporation of Platelets into the Clinic and Future Therapeutic Targets
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nurden, A. Platelets, inflammation and tissue regeneration. Thromb. Haemost. 2011, 105 (Suppl. 6), S13–S33. [Google Scholar] [CrossRef] [PubMed]
- Mammadova-Bach, E.; Mangin, P.; Lanza, F.; Gachet, C. Platelets in cancer: From basic research to therapeutic implications. Hamostaseologie 2015, 35, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Menter, D.G.; Tucker, S.C.; Kopetz, S.; Sood, A.K.; Crissman, J.D.; Honn, K.V. Platelets and cancer: A casual or causal relationship: Revisited. Cancer Metastasis Rev. 2014, 33, 231–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlesinger, M. Role of platelets and platelet receptors in cancer metastasis 06 Biological Sciences 0601 Biochemistry and Cell Biology. J. Hematol. Oncol. 2018, 11, 125. [Google Scholar] [CrossRef] [PubMed]
- Evans, T.R.J.; Mansi, J.L.; Bevan, D.H. Trousseau’s syndrome in association with ovarian carcinoma. Cancer 1996, 77, 2544–2549. [Google Scholar] [CrossRef]
- Cognasse, F.; Laradi, S.; Berthelot, P.; Bourlet, T.; Marotte, H.; Mismetti, P.; Garraud, O.; Hamzeh-Cognasse, H. Platelet Inflammatory Response to Stress. Front. Immunol. 2019, 10, 1478. [Google Scholar] [CrossRef] [PubMed]
- Santos-Martínez, M.J.; Medina, C.; Jurasz, P.; Radomski, M.W. Role of metalloproteinases in platelet function. Thromb. Res. 2008, 121, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Seizer, P.; May, A.E. Platelets and matrix metalloproteinases. Thromb. Haemost. 2013, 110, 903–909. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Andia, I.; Ardanza, B.; Nurden, P.; Nurden, A.T. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb. Haemost. 2004, 91, 4–15. [Google Scholar] [CrossRef]
- Kim, K.H.; Park, T.Y.; Lee, J.Y.; Lee, S.-M.; Yim, J.-J.; Yoo, C.-G.; Kim, Y.W.; Han, S.K.; Yang, S.-C. Prognostic Significance of Initial Platelet Counts and Fibrinogen Level in Advanced Non-Small Cell Lung Cancer. J. Korean Med. Sci. 2014, 29, 507. [Google Scholar] [CrossRef]
- Kim, M.; Chang, H.; Yang, H.C.; Kim, Y.J.; Lee, C.T.; Lee, J.H.; Jheon, S.; Kim, K.; Chung, J.H.; Lee, J.S. Preoperative thrombocytosis is a significant unfavorable prognostic factor for patients with resectable non-small cell lung cancer. World J. Surg. Oncol. 2014, 12, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taucher, S.; Salat, A.; Gnant, M.; Kwasny, W.; Mlineritsch, B.; Menzel, R.C.; Schmid, M.; Smola, M.G.; Stierer, M.; Tausch, C.; et al. Impact of pretreatment thrombocytosis on survival in primary breast cancer. Thromb. Haemost. 2003, 89, 1098–1106. [Google Scholar] [PubMed]
- Stravodimou, A.; Voutsadakis, I.A. Pretreatment Thrombocytosis as a Prognostic Factor in Metastatic Breast Cancer. Int. J. Breast Cancer 2013, 2013, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Chadha, A.S.; Kocak-Uzel, E.; Das, P.; Minsky, B.D.; Delclos, M.E.; Mahmood, U.; Guha, S.; Ahmad, M.; Varadhachary, G.R.; Javle, M.; et al. Paraneoplastic thrombocytosis independently predicts poor prognosis in patients with locally advanced pancreatic cancer. Acta Oncol. (Madr.) 2015, 54, 971–978. [Google Scholar] [CrossRef]
- Suzuki, K.; Aiura, K.; Kitagou, M.; Hoshimoto, S.; Takahashi, S.; Ueda, M.; Kitajima, M. Platelets counts closely correlate with the disease-free survival interval of pancreatic cancer patients. Hepatogastroenterology 2004, 51, 847–853. [Google Scholar] [PubMed]
- Zhao, J.-M.; Wang, Y.-H.; Yao, N.; Wei, K.-K.; Jiang, L.; Hanif, S.; Wang, Z.-X. Poor Prognosis Significance of Pretreatment Thrombocytosis in Patients with Colorectal Cancer: A Meta-Analysis. Asian Pac. J. Cancer Prev. 2016, 17, 4295–4300. [Google Scholar]
- Hu, C.Y.; Chen, R.P.; Chen, W.J.; Pang, W.Y.; Xue, X.Y.; Zhu, G.B.; Shen, X. Thrombocytosis is a significant indictor of hypercoagulability, prognosis and recurrence in gastric cancer. Exp. Ther. Med. 2014, 8, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Hwang, S.G.; Kim, K.M.; Cheong, J.H.; Kim, H.I.; An, J.Y.; Hyung, W.J.; Noh, S.H. Impact of pretreatment thrombocytosis on blood-borne metastasis and prognosis of gastric cancer. Eur. J. Surg. Oncol. 2012, 38, 562–567. [Google Scholar] [CrossRef]
- Lin, R.J.; Afshar-Kharghan, V.; Schafer, A.I. Paraneoplastic thrombocytosis: The secrets of tumor self-promotion. Blood 2014, 124, 184–187. [Google Scholar] [CrossRef]
- Eggemann, H.; Ehricke, J.; Ignatov, T.; Fettke, F.; Semczuk, A.; Costa, S.D.; Ignatov, A. Platelet count after chemotherapy is a predictor for outcome for ovarian cancer patients. Cancer Investig. 2015, 33, 193–196. [Google Scholar] [CrossRef]
- Torre, L.A.; Trabert, B.; DeSantis, C.E.; Miller, K.D.; Samimi, G.; Runowicz, C.D.; Gaudet, M.M.; Jemal, A.; Siegel, R.L. Ovarian cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 284–296. [Google Scholar] [CrossRef]
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian cancer. Lancet 2014, 384, 1376–1388. [Google Scholar] [CrossRef]
- Kurman, R.J.; Shih, I.M. Pathogenesis of ovarian cancer: Lessons from morphology and molecular biology and their clinical implications. Int. J. Gynecol. Pathol. 2008, 27, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sant, M.; Chirlaque Lopez, M.D.; Agresti, R.; Sánchez Pérez, M.J.; Holleczek, B.; Bielska-Lasota, M.; Dimitrova, N.; Innos, K.; Katalinic, A.; Langseth, H.; et al. Survival of women with cancers of breast and genital organs in Europe 1999–2007: Results of the EUROCARE-5 study. Eur. J. Cancer 2015, 51, 2191–2205. [Google Scholar] [CrossRef]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupaimoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic thrombocytosis in ovarian cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef] [Green Version]
- Cozzi, G.D.; Samuel, J.M.; Fromal, J.T.; Keene, S.; Crispens, M.A.; Khabele, D.; Beeghly-Fadiel, A. Thresholds and timing of pre-operative thrombocytosis and ovarian cancer survival: Analysis of laboratory measures from electronic medical records. BMC Cancer 2016, 16, 612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Digklia, A.; Voutsadakis, I.A. Thrombocytosis as a prognostic marker in stage III and IV serous ovarian cancer. Obstet. Gynecol. Sci. 2014, 57, 457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Z.; Wen, H.; Bi, R.; Duan, Y.; Yang, W.; Wu, X. Thrombocytosis and hyperfibrinogenemia are predictive factors of clinical outcomes in high-grade serous ovarian cancer patients. BMC Cancer 2016, 16, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allensworth, S.K.; Langstraat, C.L.; Martin, J.R.; Lemens, M.A.; McGree, M.E.; Weaver, A.L.; Dowdy, S.C.; Podratz, K.C.; Bakkum-Gamez, J.N. Evaluating the prognostic significance of preoperative thrombocytosis in epithelial ovarian cancer. Gynecol. Oncol. 2013, 130, 499–504. [Google Scholar] [CrossRef] [Green Version]
- Li, A. The prognostic significance of thrombocytosis in epithelial ovarian carcinoma. Gynecol. Oncol. 2004, 92, 211–214. [Google Scholar] [CrossRef]
- Ma, X.; Wang, Y.; Sheng, H.; Tian, W.; Qi, Z.; Teng, F.; Xue, F. Prognostic significance of thrombocytosis, platelet parameters and aggregation rates in epithelial ovarian cancer. J. Obstet. Gynaecol. Res. 2014, 40, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Man, Y.N.; Wang, Y.N.; Hao, J.; Liu, X.; Liu, C.; Zhu, C.; Wu, X.Z. Pretreatment plasma D-dimer, fibrinogen, and platelet levels significantly impact prognosis in patients with epithelial ovarian cancer independently of venous thromboembolism. Int. J. Gynecol. Cancer 2015, 25, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Kim, S.W.; Nam, E.J.; Yim, G.W.; Kim, S.; Kim, Y.T. The impact of pretreatment thrombocytosis and persistent thrombocytosis after adjuvant chemotherapy in patients with advanced epithelial ovarian cancer. Gynecol. Oncol. 2011, 122, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Bottsford-Miller, J.; Choi, H.J.; Dalton, H.J.; Stone, R.L.; Cho, M.S.; Haemmerle, M.; Nick, A.M.; Pradeep, S.; Zand, B.; Previs, R.A.; et al. Differential platelet levels affect response to taxane-based therapy in ovarian cancer. Clin. Cancer Res. 2015, 21, 602–610. [Google Scholar] [CrossRef] [Green Version]
- Crasta, J.A.; Premlatha, T.S.; Krishnan, S.M.; Vallikad, E.; Rameshkumar, K. Significance of preoperative thrombocytosis in epithelial ovarian cancer. Indian J. Pathol. Microbiol. 2010, 53, 54–56. [Google Scholar] [CrossRef]
- Haddad, L.B.; Laufer, M.R. Thrombocytosis Associated with Malignant Ovarian Lesions within a Pediatric/Adolescent Population. J. Pediatr. Adolesc. Gynecol. 2008, 21, 243–246. [Google Scholar] [CrossRef]
- Watrowski, R.; Heinze, G.; Jäger, C.; Forster, J.; Zeillinger, R. Usefulness of the preoperative platelet count in the diagnosis of adnexal tumors. Tumor Biol. 2016, 37, 12079–12087. [Google Scholar] [CrossRef]
- Atacag, T. Diagnostic value of thrombocytosis and high CA 125 level in women with adnexal masses. Eur. J. Gynaecol. Oncol. 2012, 33, 517–520. [Google Scholar]
- Barber, E.L.; Boggess, J.F.; Van Le, L.; Kim, K.H.; Bae-Jump, V.L.; Brewster, W.R.; Soper, J.T.; Gehrig, P.A. Association of Preoperative Thrombocytosis and Leukocytosis With Postoperative Morbidity and Mortality Among Patients With Ovarian Cancer. Obstet. Gynecol. 2015, 126, 1191–1197. [Google Scholar] [CrossRef]
- ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2000 Feb 29. Identifier NCT03378297, IMPACT: A Randomized WOO Study of Novel Therapeutic Agents in Women Triaged to Primary Surgery for EOC. 19 December 2017. Available online: https://clinicaltrials.gov (accessed on 16 September 2020).
- Merritt, M.A.; Rice, M.S.; Barnard, M.E.; Hankinson, S.E.; Matulonis, U.A.; Poole, E.M.; Tworoger, S.S. Pre-diagnosis and post-diagnosis use of common analgesics and ovarian cancer prognosis (NHS/NHSII): A cohort study. Lancet Oncol. 2018, 19, 1107–1116. [Google Scholar] [CrossRef]
- Verdoodt, F.; Dehlendorff, C.; Friis, S.; Kjaer, S.K. Non-aspirin NSAID use and ovarian cancer mortality. Gynecol. Oncol. 2018, 150, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Wield, A.M.; Walsh, C.S.; Rimel, B.J.; Cass, I.; Karlan, B.Y.; Li, A.J. Aspirin use correlates with survival in women with clear cell ovarian cancer. Gynecol. Oncol. Rep. 2018, 25, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Cheng, J.; Ye, M.; Liu, D.; Zhang, Y. Association of pretreatment thrombocytosis with prognosis in ovarian cancer: A systematic review and meta-analysis. J. Gynecol. Oncol. 2019, 30, e5. [Google Scholar] [CrossRef] [PubMed]
- Menczer, J. Preoperative elevated platelet count and thrombocytosis in gynecologic malignancies. Arch. Gynecol. Obstet. 2017, 295, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.L.; Eskelund, C.W.; Siersma, V.D.; Felding, P.; Lind, B.; Palmblad, J.; Bjerrum, O.W.; Friis, S.; Hasselbalch, H.C.; De Fine Olivarius, N. Is thrombocytosis a valid indicator of advanced stage and high mortality of gynecological cancer? Gynecol. Oncol. 2015, 139, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Słabuszewska-Jóźwiak, A.; Dmoch-Gajzlerska, E.; Kozakiewicz, B.; Jakiel, G. The prognostic significance of thrombocytosis in ovarian cancer. Ann. Agric. Environ. Med. 2015, 22, 731–735. [Google Scholar] [CrossRef]
- Hu, Q.; Hada, A.; Han, L. Platelet count as a biomarker for monitoring treatment response and disease recurrence in recurrent epithelial ovarian cancer. J. Ovarian Res. 2020, 13, 78. [Google Scholar] [CrossRef]
- Menczer, J.; Schejter, E.; Geva, D.; Ginath, S.; Zakut, H. Ovarian carcinoma associated thrombocytosis. Correlation with prognostic factors and with survival. Eur. J. Gynaecol. Oncol. 1998, 19, 82–84. [Google Scholar]
- Zeimet, A.G.; Marth, C.; Müller-Holzner, E.; Daxenbichler, G.; Dapunt, O. Significance of thrombocytosis in patients with epithelial ovarian cancer. Am. J. Obstet. Gynecol. 1994, 170, 549–554. [Google Scholar] [CrossRef]
- Qiu, J.; Yu, Y.; Fu, Y.; Ye, F.; Xie, X.; Lu, W. Preoperative plasma fibrinogen, platelet count and prognosis in epithelial ovarian cancer. J. Obstet. Gynaecol. Res. 2012, 38, 651–657. [Google Scholar] [CrossRef]
- Nakao, S.; Minaguchi, T.; Itagaki, H.; Hosokawa, Y.; Shikama, A.; Tasaka, N.; Akiyama, A.; Ochi, H.; Matsumoto, K.; Satoh, T. Pretreatment thrombocytosis as an independent predictive factor for chemoresistance and poor survival in epithelial ovarian cancer. J. Ovarian Res. 2020, 13, 55. [Google Scholar] [CrossRef]
- Gungor, T.; Kanat-Pektas, M.; Sucak, A.; Mollamahmutoglu, L. The role of thrombocytosis in prognostic evaluation of epithelial ovarian tumors. Arch. Gynecol. Obstet. 2009, 279, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, L.; Liu, W.X.; Liu, X.Y. Prognostic significance of preoperative anemia, leukocytosis and thrombocytosis in chinese women with epithelial ovarian cancer. Asian Pac. J. Cancer Prev. 2015, 16, 933–939. [Google Scholar] [CrossRef]
- Matsuo, K.; Hasegawa, K.; Yoshino, K.; Murakami, R.; Hisamatsu, T.; Stone, R.L.; Previs, R.A.; Hansen, J.M.; Ikeda, Y.; Miyara, A.; et al. Venous thromboembolism, interleukin-6 and survival outcomes in patients with advanced ovarian clear cell carcinoma. Eur. J. Cancer 2015, 51, 1978–1988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.P.; Huang, Q.D.; Wan, T.; Tu, H.; Gu, H.F.; Cao, J.Y.; Liu, J.H. Combined score of pretreatment platelet count and CA125 level (PLT-CA125) stratified prognosis in patients with FIGO stage IV epithelial ovarian cancer. J. Ovarian Res. 2019, 12, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okunade, K.S.; Dawodu, O.; Adenekan, M.; Nwogu, C.M.; Awofeso, O.; Ugwu, A.O.; Salako, O.; John-Olabode, S.; Olowoselu, O.F.; Anorlu, R.I. Prognostic impact of pretreatment thrombocytosis in epithelial ovarian cancer. Niger. J. Clin. Pract. 2020, 23, 1141–1147. [Google Scholar] [CrossRef]
- Soonthornthum, T.; Suraseraneewong, V.; Kengsakol, K.; Wijaithum, K.; Kasemsan, P.; Prommatt, S. Thrombocytosis in advanced epithelial ovarian cancer. J. Med. Assoc. Thail. 2007, 90, 1495–1500. [Google Scholar]
- Komura, N.; Mabuchi, S.; Yokoi, E.; Shimura, K.; Kawano, M.; Matsumoto, Y.; Kimura, T. Pre-treatment prognostic nutritional index is superior to platelet count in predicting disease-specific survival in patients with epithelial ovarian cancer. Int. J. Gynecol. Cancer 2019, 29, 1057–1063. [Google Scholar] [CrossRef]
- Tang, M.; Jiang, L.; Lin, Y.; Wu, X.; Wang, K.; He, Q.; Wang, X.; Li, W. Platelet microparticle-mediated transfer of miR-939 to epithelial ovarian cancer cells promotes epithelial to mesenchymal transition. Oncotarget 2017, 8, 97464–97475. [Google Scholar] [CrossRef] [Green Version]
- Hefler-Frischmuth, K.; Grimm, C.; Gensthaler, L.; Reiser, E.; Schwameis, R.; Hefler, L.A. Prognostic value of preoperative hyponatremia and thrombocytosis in patients with epithelial ovarian cancer. Wien. Klin. Wochenschr. 2018, 130, 575–580. [Google Scholar] [CrossRef]
- Gerestein, C.G.; Eijkemans, M.J.C.; De Jong, D.; Van Der Burg, M.E.L.; Dykgraaf, R.H.M.; Kooi, G.S.; Baalbergen, A.; Burger, C.W.; Ansink, A.C. The prediction of progression-free and overall survival in women with an advanced stage of epithelial ovarian carcinoma. BJOG An Int. J. Obstet. Gynaecol. 2009, 116, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.G.; Tran, A.Q.; Rimel, B.J.; Cass, I.; Walsh, C.S.; Karlan, B.Y.; Li, A.J. Thrombocytosis at secondary cytoreduction for recurrent ovarian cancer predicts suboptimal resection and poor survival. Gynecol. Oncol. 2014, 132, 556–559. [Google Scholar] [CrossRef]
- Canzler, U.; Lück, H.J.; Neuser, P.; Sehouli, J.; Burges, A.; Harter, P.; Schmalfeldt, B.; Aminossadati, B.; Mahner, S.; Kommoss, S.; et al. Prognostic role of thrombocytosis in recurrent ovarian cancer: A pooled analysis of the AGO Study Group. Arch. Gynecol. Obstet. 2020, 301, 1267–1274. [Google Scholar] [CrossRef]
- Bozkurt, N.; Yuce, K.; Basaran, M.; Kose, F.; Ayhan, A. Correlation of platelet count with second-look laparotomy results and disease progression in patients with advanced epithelial ovarian cancer. Obstet. Gynecol. 2004, 103, 82–85. [Google Scholar] [CrossRef]
- Gastl, G.; Plante, M.; Finstad, C.L.; Wong, G.Y.; Federici, M.G.; Bander, N.H.; Rubin, S.C. High IL-6 levels in ascitic fluid correlate with reactive thrombocytosis in patients with epithelial ovarian cancer. Br. J. Haematol. 1993, 83, 433–441. [Google Scholar] [CrossRef]
- Besbes, S.; Shah, S.; Al-Dybiat, I.; Mirshahi, S.; Helfer, H.; Najah, H.; Fourgeaud, C.; Pocard, M.; Ghedira, I.; Soria, J.; et al. Thrombopoietin Secretion by Human Ovarian Cancer Cells. Int. J. Cell Biol. 2017, 2017, 1873834. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.-X.; Qiao, Y.-H.; Zhou, Y.; Li, L.-X.; Shi, H.-R.; Chen, K.-S. Increased staining for phosphorylated AKT and nuclear factor-κB p65 and their relationship with prognosis in epithelial ovarian cancer. Pathol. Int. 2008, 58, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Darb-Esfahani, S.; Sinn, B.V.; Weichert, W.; Budczies, J.; Lehmann, A.; Noske, A.; Buckendahl, A.C.; Müller, B.M.; Sehouli, J.; Koensgen, D.; et al. Expression of classical NF-κB pathway effectors in human ovarian carcinoma. Histopathology 2010, 56, 727–739. [Google Scholar] [CrossRef]
- Annunziata, C.M.; Stavnes, H.T.; Kleinberg, L.; Berner, A.; Hernandez, L.F.; Birrer, M.J.; Steinberg, S.M.; Davidson, B.; Kohn, E.C. Nuclear factor κB transcription factors are coexpressed and convey a poor outcome in ovarian cancer. Cancer 2010, 116, 3276–3284. [Google Scholar] [CrossRef] [Green Version]
- Kleinberg, L.; Dong, H.P.; Holth, A.; Risberg, B.; Trope’, C.G.; Nesland, J.M.; Flørenes, V.A.; Davidson, B. Cleaved caspase-3 and nuclear factor-κB p65 are prognostic factors in metastatic serous ovarian carcinoma. Hum. Pathol. 2009, 40, 795–806. [Google Scholar] [CrossRef]
- Shuang, T.; Wang, M.; Zhou, Y.; Shi, C. Over-expression of nuclear NF-κB1 and c-Rel correlates with chemoresistance and prognosis of serous epithelial ovarian cancer. Exp. Mol. Pathol. 2016, 100, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Hufnagel, D.H.; Wilson, A.J.; Saxon, J.; Blackwell, T.S.; Watkins, J.; Khabele, D.; Crispens, M.A.; Yull, F.E.; Beeghly-Fadiel, A. Expression of p52, a non-canonical NF-kappaB transcription factor, is associated with poor ovarian cancer prognosis. Biomark. Res. 2020, 8, 45. [Google Scholar] [CrossRef] [PubMed]
- Hutti, J.E.; Pfefferle, A.D.; Russell, S.C.; Sircar, M.; Perou, C.M.; Baldwin, A.S. Oncogenic PI3K mutations lead to NF-κB-dependent cytokine expression following growth factor deprivation. Cancer Res. 2012, 72, 3260–3269. [Google Scholar] [CrossRef] [Green Version]
- Holmes, C.E.; Levis, J.E.; Ornstein, D.L. Activated platelets enhance ovarian cancer cell invasion in a cellular model of metastasis. Clin. Exp. Metastasis 2009, 26, 653–661. [Google Scholar] [CrossRef]
- Cho, M.S.; Bottsford-Miller, J.; Vasquez, H.G.; Stone, R.; Zand, B.; Kroll, M.H.; Sood, A.K.; Afshar-Kharghan, V. Platelets increase the proliferation of ovarian cancer cells. Blood 2012, 120, 4869–4872. [Google Scholar] [CrossRef] [Green Version]
- Cooke, N.M.; Spillane, C.D.; Sheils, O.; O’Leary, J.; Kenny, D. Aspirin and P2Y12 inhibition attenuate platelet-induced ovarian cancer cell invasion. BMC Cancer 2015, 15, 627. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.; Kabir, S.M.; Dong, Y.; Lee, E.; Rice, V.M.; Khabele, D.; Son, D.S. Aspirin blocks EGF-stimulated cell viability in a COX-1 dependent manner in ovarian cancer cells. J. Cancer 2013, 4, 671–678. [Google Scholar] [CrossRef] [Green Version]
- Selvendiran, K.; Bratasz, A.; Tong, L.; Ignarro, L.J.; Kuppusamy, P. NCX-4016, a nitro-derivative of aspirin, inhibits EGFR and STAT3 signaling and modulates Bcl-2 proteins in cisplatin-resistant human ovarian cancer cells and xenografts. Cell Cycle 2008, 7, 81–88. [Google Scholar] [CrossRef]
- Huang, Y.; Lichtenberger, L.M.; Taylor, M.; Bottsford-Miller, J.N.; Haemmerle, M.; Wagner, M.J.; Lyons, Y.; Pradeep, S.; Hu, W.; Previs, R.A.; et al. Antitumor and antiangiogenic effects of aspirin-PC in ovarian cancer. Mol. Cancer Ther. 2016, 15, 2894–2904. [Google Scholar] [CrossRef] [Green Version]
- Cho, M.S.; Noh, K.; Haemmerle, M.; Li, D.; Park, H.; Hu, Q.; Hisamatsu, T.; Mitamura, T.; Mak, S.L.C.; Kunapuli, S.; et al. Role of ADP receptors on platelets in the growth of ovarian cancer. Blood 2017, 130, 1235–1242. [Google Scholar] [CrossRef]
- Egan, K.; Crowley, D.; Smyth, P.; O’Toole, S.; Spillane, C.; Martin, C.; Gallagher, M.; Canney, A.; Norris, L.; Conlon, N.; et al. Platelet adhesion and degranulation induce pro-survival and pro-angiogenic signalling in ovarian cancer cells. PLoS ONE 2011, 6, e26125. [Google Scholar] [CrossRef] [PubMed]
- Möhle, R.; Green, D.; Moore, M.A.S.; Nachman, R.L.; Rafii, S. Constitutive production and thrombin-induced release of vascular endothelial growth factor by human megakaryocytes and platelets. Proc. Natl. Acad. Sci. USA 1997, 94, 663–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, L.; Liu, X. Platelets are associated with xenograft tumor growth and the clinical malignancy of ovarian cancer through an angiogenesis-dependent mechanism. Mol. Med. Rep. 2015, 11, 2449–2458. [Google Scholar] [CrossRef] [PubMed]
- Erices, R.; Cubillos, S.; Aravena, R.; Santoro, F.; Marquez, M.; Orellana, R.; Ramírez, C.; González, P.; Fuenzalida, P.; Bravo, M.L.; et al. Diabetic concentrations of metformin inhibit platelet-mediated ovarian cancer cell progression. Oncotarget 2017, 8, 20865–20880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haemmerle, M.; Bottsford-Miller, J.; Pradeep, S.; Taylor, M.L.; Choi, H.J.; Hansen, J.M.; Dalton, H.J.; Stone, R.L.; Cho, M.S.; Nick, A.M.; et al. FAK regulates platelet extravasation and tumor growth after antiangiogenic therapy withdrawal. J. Clin. Investig. 2016, 126, 1885–1896. [Google Scholar] [CrossRef] [Green Version]
- Nieswandt, B.; Hafner, M.; Echtenacher, B.; Männel, D.N. Lysis of tumor cells by natural killer cells in mice is impeded by platelets. Cancer Res. 1999, 59, 1295–1300. [Google Scholar]
- Orellana, R.; Kato, S.; Erices, R.; Bravo, M.L.; Gonzalez, P.; Oliva, B.; Cubillos, S.; Valdivia, A.; Ibañez, C.; Brañes, J.; et al. Platelets enhance tissue factor protein and metastasis initiating cell markers, and act as chemoattractants increasing the migration of ovarian cancer cells. BMC Cancer 2015, 15, 290. [Google Scholar] [CrossRef] [Green Version]
- Gasic, G.J.; Gasic, T.B.; Stewart, C.C. Antimetastatic effects associated with platelet reduction. Proc. Natl. Acad. Sci. USA 1968, 61, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Stone, R.L.; Kaelber, J.T.; Rochat, R.H.; Nick, A.M.; Vijayan, K.V.; Afshar-Kharghan, V.; Schmida, M.F.; Sood, A.K.; Chiu, W. Electron cryotomography reveals ultrastructure alterations in platelets from patients with ovarian cancer. Proc. Natl. Acad. Sci. USA 2015, 112, 14266–14271. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Kroll, M.H.; Nick, A.M.; Sood, A.K.; Afshar-Kharghan, V. Platelets are not hyperreactive in patients with ovarian cancer. Platelets 2016, 27, 716–718. [Google Scholar] [CrossRef] [Green Version]
- Li, A.J.; Karlan, B.Y. Androgen mediation of thrombocytosis in epithelial ovarian cancer biology. Clin. Cancer Res. 2005, 11, 8015–8018. [Google Scholar] [CrossRef] [Green Version]
- Coward, J.; Kulbe, H.; Chakravarty, P.; Leader, D.; Vassileva, V.; Leinster, D.A.; Thompson, R.; Schioppa, T.; Nemeth, J.; Vermeulen, J.; et al. Interleukin-6 as a therapeutic target in human ovarian cancer. Clin. Cancer Res. 2011, 17, 6083–6096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslan, J.E.; Tormoen, G.W.; Loren, C.P.; Pang, J.; McCarty, O.J.T. S6K1 and mTOR regulate Rac1-driven platelet activation and aggregation. Blood 2011, 118, 3129–3136. [Google Scholar] [CrossRef] [Green Version]
- Fang, D.; Chen, H.; Zhu, J.Y.; Wang, W.; Teng, Y.; Ding, H.F.; Jing, Q.; Su, S.B.; Huang, S. Epithelial-mesenchymal transition of ovarian cancer cells is sustained by Rac1 through simultaneous activation of MEK1/2 and Src signaling pathways. Oncogene 2017, 36, 1546–1558. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Villasana, V.; Fuentes-Mattei, E.; Ivan, C.; Dalton, H.J.; Rodriguez-Aguayo, C.; Fernandez-De Thomas, R.J.; Aslan, B.; Monroig, P.D.C.; Velazquez-Torres, G.; Previs, R.A.; et al. Rac1/Pak1/p38/MMP-2 axis regulates angiogenesis in ovarian cancer. Clin. Cancer Res. 2015, 21, 2127–2137. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Kenney, S.R.; Muller, C.Y.; Adams, S.; Rutledge, T.; Romero, E.; Murray-Krezan, C.; Prekeris, R.; Sklar, L.A.; Hudson, L.G.; et al. R-ketorolac targets Cdc42 and Rac1 and alters ovarian cancer cell behaviors critical for invasion and metastasis. Mol. Cancer Ther. 2015, 14, 2215–2227. [Google Scholar] [CrossRef] [Green Version]
- Hudson, L.G.; Gillette, J.M.; Kang, H.; Rivera, M.R.; Wandinger-Ness, A. Ovarian tumor microenvironment signaling: Convergence on the Rac1 GTPase. Cancers (Basel) 2018, 10, 358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudson, L.G.; Cook, L.S.; Grimes, M.M.; Muller, C.Y.; Adams, S.F.; Wandinger-ness, A. Dual actions of ketorolac in metastatic ovarian cancer. Cancers (Basel) 2019, 11, 1049. [Google Scholar] [CrossRef] [Green Version]
- Brasky, T.M.; Liu, J.; White, E.; Peters, U.; Potter, J.D.; Walter, R.B.; Baik, C.S.; Lane, D.S.; Manson, J.E.; Vitolins, M.Z.; et al. Non-steroidal anti-inflammatory drugs and cancer risk in women: Results from the Women’s Health Initiative. Int. J. Cancer 2014, 135, 1869–1883. [Google Scholar] [CrossRef] [PubMed]
- Trabert, B.; Ness, R.B.; Lo-Ciganic, W.H.; Murphy, M.A.; Goode, E.L.; Poole, E.M.; Brinton, L.A.; Webb, P.M.; Nagle, C.M.; Jordan, S.J.; et al. Aspirin, nonaspirin nonsteroidal anti-inflammatory drug, and acetaminophen use and risk of invasive epithelial ovarian cancer: A pooled analysis in the ovarian cancer association consortium. J. Natl. Cancer Inst. 2014, 106, djt431. [Google Scholar] [CrossRef] [Green Version]
- Trabert, B.; Poole, E.M.; White, E.; Visvanathan, K.; Adami, H.O.; Anderson, G.L.; Brasky, T.M.; Brinton, L.A.; Fortner, R.T.; Gaudet, M.; et al. Analgesic use and ovarian cancer risk: An analysis in the Ovarian Cancer Cohort Consortium. J. Natl. Cancer Inst. 2019, 111, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Ylikorkala, O.; Kauppila, A.; Viinikka, L. Prostacyclin and thromboxane in ovarian cancer: Effect of cytostatics and prostaglandin synthesis inhibitors. Gynecol. Oncol. 1983, 16, 340–345. [Google Scholar] [CrossRef]
- Altinoz, M.A.; Korkmaz, R. NF-κB, macrophage migration inhibitory factor and cyclooxygenase-inhibitions as likely mechanisms behind the acetaminophen- and NSAID-prevention of the ovarian cancer. Neoplasma 2004, 51, 239–247. [Google Scholar]
- Mulder, F.I.; Candeloro, M.; Kamphuisen, P.W.; Di Nisio, M.; Bossuyt, P.M.; Guman, N.; Smit, K.; Buller, H.R.; Van Es, N. The khorana score for prediction of venous thromboembolism in cancer patients: A systematic review and meta-analysis. Haematologica 2019, 104, 1277–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 29 Feb 2000. Identifier NCT02122185, Metformin and Chemotherapy in Treating Patients With Stage III-IV Ovarian, Fallopian Tube, or Primary Peritoneal Cancer. 24 April 2014. Available online: https://clinicaltrials.gov/ct2/show/NCT02122185?term=NCT02122185&draw=2&rank=1 (accessed on 16 September 2020).
- ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2000 Feb 29. Identifier NCT02437812, Study of Paclitaxel, Carboplatin and Oral Metformin in the Treatment of Advanced Stage Ovarian Carcinoma. 8 May 2015. Available online: https://clinicaltrials.gov/ct2/show/NCT02437812?term=NCT02437812&draw=2&rank=1 (accessed on 16 September 2020).


{kind=link}
| Author | Year | Platelet Measurement Timeframe(s) | Thrombocytosis Threshold(s) | Study Population | Statistical Analysis | Prognostic Association(s) * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Description | Pretreatment | Additional | Patients | Description | Source (Country) | Outcome | Approach | PFS/DFS | OS/DSS | |||
| Allensworth | 2013 | Preoperative (NOS) | Yes | 450 | 578 | epithelial ovarian cancer | United States | DFS, OS | KM, PHreg | Worse (unadj, adj) | Worse * (unadj) | |
| Andersen | 2014 | Up to 3-years prior to diagnosis | Yes | 400 (mild), 550 (severe) | 224 | ovarian cancer (NOS) | Denmark | All-Cause and Cancer-Specific Mortality | KM, PHreg | Worse (unadj, adj) | ||
| Barber | 2015 | Preoperative (NOS) | Yes | 450 | 1072 | ovarian cancer (NOS) | ACS NSQIP (US) | 30-Day Outcomes | Logistic Regression | Worse for major complications (unadj, adj) | ||
| Bottsford-Miller | 2015 | Pretreatment (at diagnosis) and at disease recurrence | Yes | Yes | 450 | 341 | recurrent epithelial ovarian cancer | United States | PFS, OS | KM | NS (P = 0.05) | Worse |
| Bozkurt | 2004 | Second-look laparotomy after chemotherapy (up to 5 days prior) | Yes | 380 (ROC), continuous | 37 | advanced stage (III/IV) epithelial ovarian cancer | Turkey | Presence of Disease | Wilcoxon Signed Rank Test | Worse (P = 0.025) | ||
| Canzler | 2020 | Pretreatment for recurrent disease | Yes | 400 | 300 | recurrent epithelial ovarian cancer | Germany | PFS, OS | KM, PHreg | NS (unadj) | Worse * (unadj) | |
| Chen, JP | 2019 | Pretreatment (NOS) | Yes | 400 | 108 | advanced stage (IV) epithelial ovarian cancer | China | PFS, OS | KM, PHreg | NS (KM), Worse in combination with CA-125 (unadj, adj) | Worse (KM), Worse in combination with CA-125 (unadj, adj) | |
| Chen, Y | 2015 | Pretreatment (NOS) | Yes | 400 | 816 | epithelial ovarian cancer | China | PFS, OS | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) | |
| Cohen | 2014 | Cytoreductive surgery for recurrent disease | Yes | 350 | 107 | recurrent epithelial ovarian cancer | United States | OS | KM, PHreg | Worse (unadj, adj) | ||
| Cozzi | 2016 | Date of diagnosis and up to 1, 2, 4, and 8 weeks prior | Yes | 350, 400, 450 | 304 | epithelial ovarian cancer | United States | OS | KM, PHreg | Worse (unadj, adj) | ||
| Digklia | 2014 | Pretreatment (at diagnosis) | Yes | 350 | 91 | stage III/IV serous ovarian cancer | Switzerland | PFS, OS | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) | |
| Eggemann | 2015 | At diagnosis, after surgery, before and after chemotherapy, and disease recurrence | Yes | Yes | 350 | 132 | ovarian cancer (NOS) | Germany | PFS, OS | KM, PHreg | Worse for <25% reduction (unadj, adj) | Worse for <25% reduction (unadj, adj) |
| Feng | 2016 | Preoperative (NOS) | Yes | 450 | 874 | high-grade serous ovarian cancer | China | PFS, OS | KM | NS | NS | |
| Gerestein | 2009 | Preoperative (within 1 week of surgery) | Yes | continuous | 118 | advanced stage (IIB-IV) epithelial ovarian cancer | The Netherlands | PFS, OS | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) | |
| Gungor | 2009 | Preoperative (within 14 days of surgery) | Yes | 400 | 292 | epithelial ovarian cancer | Turkey | OS | KM, PHreg | Worse (unadj, adj) | ||
| Hefler-Frischmuth | 2018 | Preoperative (24–72 h prior to initial surgery) | Yes | 450, continuous | 498 | epithelial ovarian cancer | Austria | OS | KM, PHreg | Worse * (unadj) | ||
| Hu | 2020 | Pretreatment, 14 days after chemotherapy, and disease recurrence | Yes | Yes | 300 | 104 | recurrent epithelial ovarian cancer | China | PFS, OS | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) |
| Komura | 2019 | Lowest measure between diagnosis and treatment | Yes | 427 (ROC) | 308 | epithelial ovarian cancer | Japan | DSS | KM, PHreg | Worse (unadj, adj) | ||
| Lee | 2011 | Preoperative (within 7 days prior to surgery) and after adjuvant chemotherapy | Yes | Yes | 400 | 179 | advanced stage (III/IV) epithelial ovarian cancer | Korea | PFS, OS | KM, PHreg | NS (unadj) | Worse (unadj, adj) |
| Li | 2004 | Preoperative (within 14 days of surgery) | Yes | 400 | 144 | advanced stage (III/IV) epithelial ovarian cancer | United States | DFS, OS | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) | |
| Ma | 2013 | Preoperative (within 7 days prior to surgery) | Yes | 400 | 182 | epithelial ovarian cancer | China | PFS, OS | KM, PHreg | Worse in combination with MAR (unadj, adj) | Worse in combination with MAR (unadj, adj) | |
| Man | 2015 | Pretreatment (up to 7 days prior) | Yes | 300 | 190 | epithelial ovarian cancer | China | PFS, OS (3-year) | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) | |
| Matsuo | 2015 | At diagnosis and at disease progression or recurrence | Yes | Yes | 400 | 1308 | clear cell and serous ovarian cancer | 10 academic institutions (US, Japan, England) | PFS, OS | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) |
| Menczer | 1998 | Preoperative (NOS) | Yes | 400 | 70 | epithelial ovarian cancer | Israel | OS | KM | Worse | ||
| Nakao | 2020 | Pretreatment (mean of initial and pre-treatment evaluations) | Yes | 400 | 280 | epithelial ovarian cancer | Japan | PFS, OS | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) | |
| Okunade | 2020 | Pretreatment (at diagnosis) | Yes | 450 | 72 | epithelial ovarian cancer | Nigeria | PFS, OS (3-year) | KM, PHreg | Worse (unadj, adj) | Worse (unadj, adj) | |
| Qiu | 2012 | Preoperative (2–4 days prior) | Yes | 400 | 136 | epithelial ovarian cancer | China | PFS, OS | KM, PHreg | Worse * (unadj) | Worse * (unadj) | |
| Słabuszewska-Jóźwiak | 2015 | Preoperative (1 day before surgery) | Yes | 350 | 97 | ovarian cancer (not all epithelial) | Poland | DFS, OS | Mann-Whitney U Test | NS | Worse | |
| Soonthornthum | 2007 | Preoperative (within 14 days of surgery) | Yes | 305 (ROC), 400 | 74 | epithelial ovarian cancer | Thailand | OS | KM | Worse | ||
| Stone | 2012 | Preoperative (NOS) | Yes | 450 | 619 | epithelial ovarian cancer | United States | PFS, OS | KM, PHreg | Worse (unadj) | Worse (unadj, adj) | |
| Tang | 2017 | Preoperative (NOS) | Yes | 300, 327 (ROC), 350, 400 | 171 | epithelial ovarian cancer | China | OS | KM | Worse | ||
| Zeimet | 1994 | Preoperative (NOS) | Yes | 400 | 130 | epithelial ovarian cancer | Austria | OS (4-year) | KM | NS | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hufnagel, D.H.; Cozzi, G.D.; Crispens, M.A.; Beeghly-Fadiel, A. Platelets, Thrombocytosis, and Ovarian Cancer Prognosis: Surveying the Landscape of the Literature. Int. J. Mol. Sci. 2020, 21, 8169. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218169
Hufnagel DH, Cozzi GD, Crispens MA, Beeghly-Fadiel A. Platelets, Thrombocytosis, and Ovarian Cancer Prognosis: Surveying the Landscape of the Literature. International Journal of Molecular Sciences. 2020; 21(21):8169. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218169
Chicago/Turabian StyleHufnagel, Demetra H., Gabriella D. Cozzi, Marta A. Crispens, and Alicia Beeghly-Fadiel. 2020. "Platelets, Thrombocytosis, and Ovarian Cancer Prognosis: Surveying the Landscape of the Literature" International Journal of Molecular Sciences 21, no. 21: 8169. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21218169