A Novel Formulation of Glucose-Sparing Peritoneal Dialysis Solutions with l-Carnitine Improves Biocompatibility on Human Mesothelial Cells

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
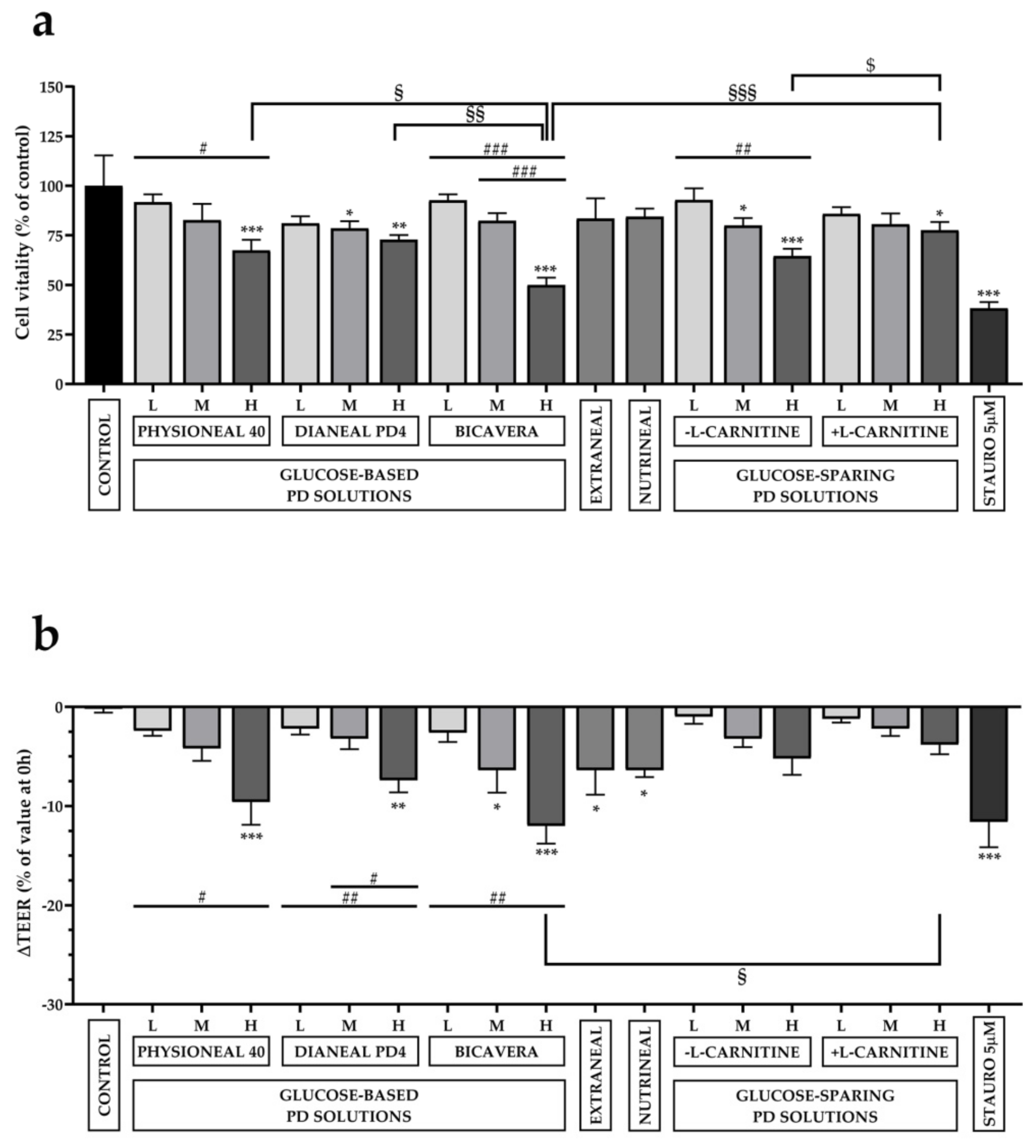
2.1. Effect of Exposure to Different PD Solutions on Cell Viability and Transepithelial Electrical Resistance (TEER)
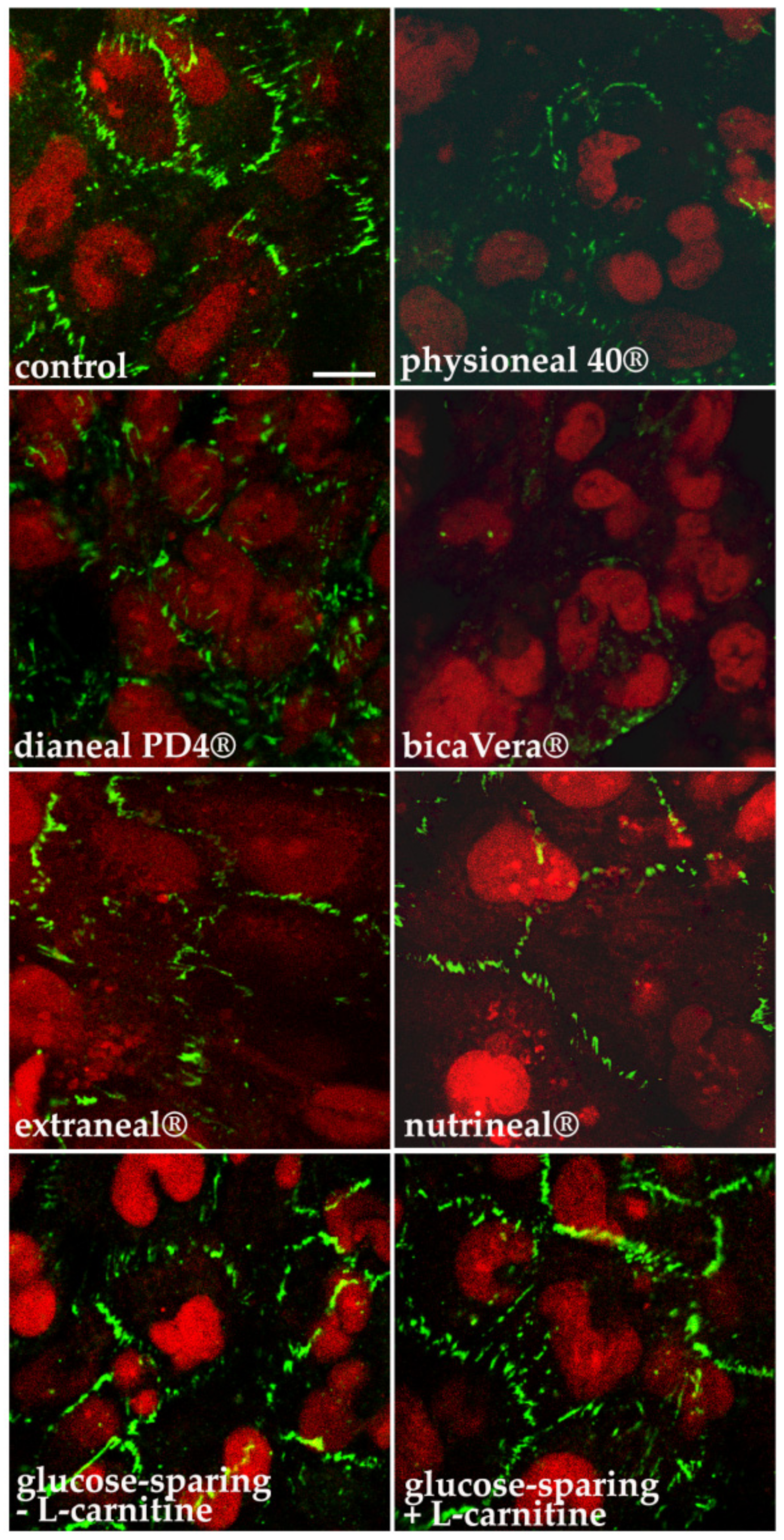
2.2. Effect of Exposure to Different PD Solution on Tight Junctions’ Integrity
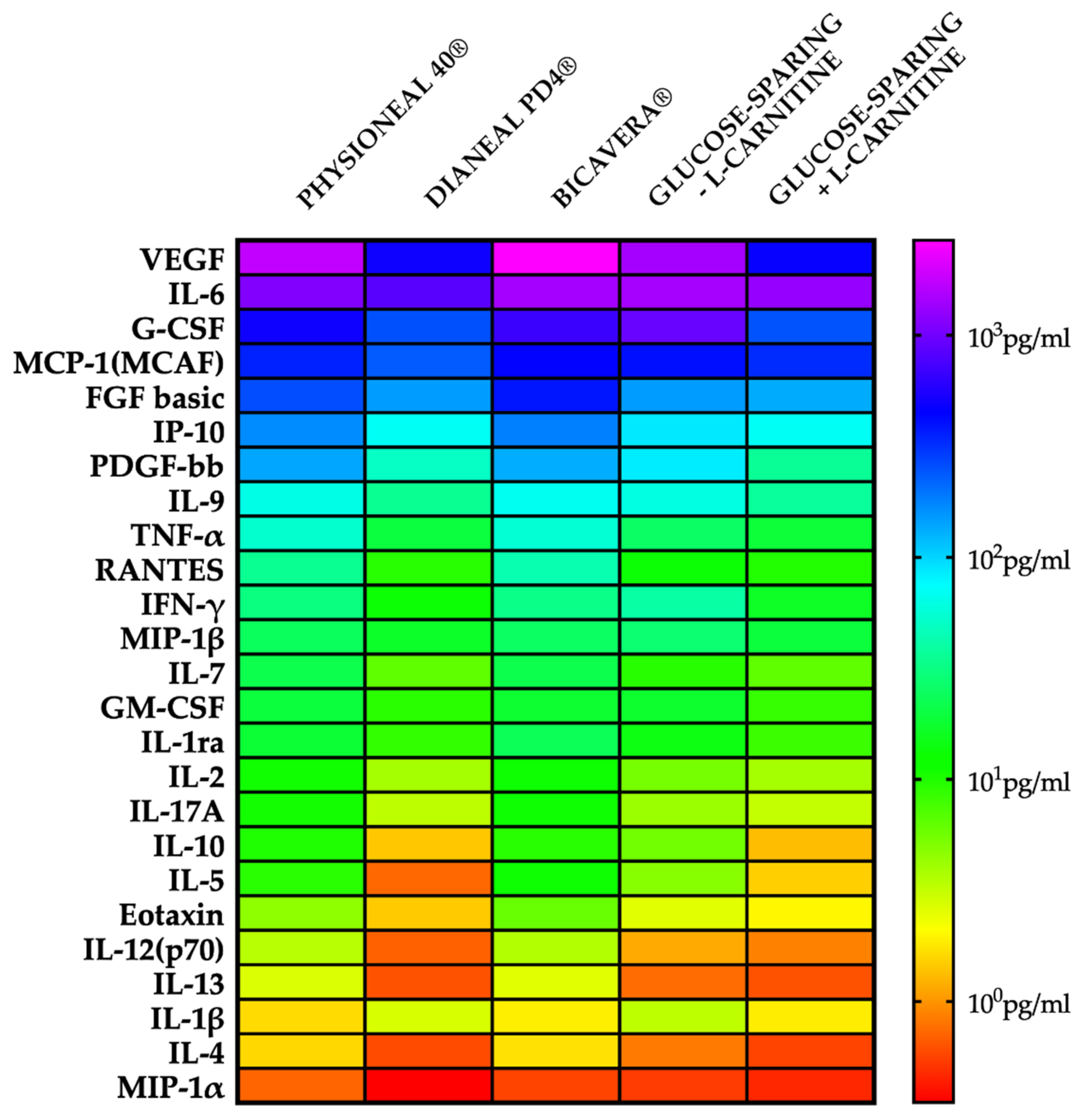
2.3. Effect of Exposure to Different PD Solution on Pro-Inflammatory Cytokines
3. Discussion
4. Materials and Methods
4.1. Cell Culture
4.2. Measurements of Transepithelial Electrical Resistance (TEER)
4.3. PD Solutions Used in the Study
4.3.1. Glucose-Based Solutions
- Physioneal 40® (Baxter Healthcare Corp., Deerfield, IL, USA); pH = 7.4, bicarbonate and lactate-buffered; Low glucose (1.36%), Medium glucose (2.27%) and High glucose (3.86%);
- Dianeal PD4® (Baxter Healthcare Corp., Deerfield, IL, USA); pH = 5–6.5, lactate-buffered; Low glucose (1.36%), Medium glucose (2.27%) and High glucose (3.86%);
- BicaVera® (Fresenius Medical Care, Bad Homburg, Germany); pH = 7.4, bicarbonate-buffered; Low glucose (1.5%), Medium glucose (2.3%) and High glucose (4.25%).
4.3.2. Glucose-Free Solutions
- Nutrineal® (Baxter Healthcare Corp., Deerfield, IL, USA), pH = 5–6, lactate-buffered, 1.1% amino acids;
- Extraneal® (Baxter Healthcare Corp., Deerfield, IL, USA), pH = 6.6, lactate-buffered, 7.5% icodextrin.
4.3.3. Glucose-Sparing Solutions
- XyloCore, pH = 5.5, lactate-buffered; Low Strength: 0.7% Xylitol, 0.5% Glucose, and ± 0.02% l-carnitine, Medium Strength: 1.5% Xylitol, 0.5% Glucose, and ± 0.02% l-carnitine, High Strength: 2.0% Xylitol, 1.5% Glucose, and ± 0.02% l-carnitine
4.4. Immunofluorescence and Confocal Microscopy
4.5. MTT Assay
4.6. Cytokines Profiling Assay
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| PD | Peritoneal Dialysis |
| ESRD | End-Stage Renal Disease |
| CAPD | Continuous Ambulatory PD |
| APD | Automated PD |
| PM | Peritoneal Membrane |
| UF | Ultrafiltration |
| EMT | Epithelial to Mesenchymal Transition |
| AA | Amino Acids |
| HMC | Human Mesothelial Cells |
| TEER | TransEpithelial Electrical Resistance |
| GDP | Glucose Degradation Products |
| Ach | Acetylcholine |
| OCTN1 | Organic Cation Transporter |
References
- Gokal, R.; Mallick, N.P. Peritoneal dialysis. Lancet 1999, 353, 823–828. [Google Scholar] [CrossRef]
- Pereira, B.; Sayegh, M.; Blake, P. Chronic Kidney Disease, Dialysis, and Transplantation: Companion to Brenner and Rector’s the Kidney, 2nd ed.; Pereira, B.J.G., Sayegh, M.H., Blake, P., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2004. [Google Scholar]
- Mehrotra, R.; Devuyst, O.; Davies, S.J.; Johnson, D.W. The Current State of Peritoneal Dialysis. J. Am. Soc. Nephrol. 2016, 27, 3238–3252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, A.; Pippias, M.; Noordzij, M.; Stel, V.S.; Afentakis, N.; Ambühl, P.M.; Andrusev, A.M.; Fuster, E.A.; Arribas Monzón, F.E.; Åsberg, A.; et al. The European Renal Association—European Dialysis and Transplant Association (ERA-EDTA) Registry Annual Report 2015: A summary. Clin. Kidney J. 2018, 11, 108–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krediet, R.T.; Struijk, D.G. Peritoneal changes in patients on long-term peritoneal dialysis. Nat. Rev. Nephrol. 2013, 9, 419–429. [Google Scholar] [CrossRef]
- Williams, J.D.; Craig, K.J.; Topley, N.; Von Ruhland, C.; Fallon, M.; Newman, G.R.; Mackenzie, R.K.; Williams, G.T. Morphologic Changes in the Peritoneal Membrane of Patients with Renal Disease. J. Am. Soc. Nephrol. 2002, 13, 470–479. [Google Scholar]
- Bajo, M.A.; del Peso, G.; Teitelbaum, I. Peritoneal Membrane Preservation. Semin. Nephrol. 2017, 37, 77–92. [Google Scholar] [CrossRef]
- Davies, S.J.; Phillips, L.; Griffiths, A.M.; Russell, L.H.; Naish, P.F.; Russell, G.I. What really happens to people on long-term peritoneal dialysis? Kidney Int. 1998, 54, 2207–2217. [Google Scholar] [CrossRef] [Green Version]
- Lambie, M.; Chess, J.; Donovan, K.L.; Kim, Y.L.; Do, J.Y.; Lee, H.B.; Noh, H.; Williams, P.F.; Williams, A.J.; Davison, S.; et al. Independent Effects of Systemic and Peritoneal Inflammation on Peritoneal Dialysis Survival. J. Am. Soc. Nephrol. 2013, 24, 2071–2080. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, B.; Bartosova, M.; Macher-Goeppinger, S.; Sallay, P.; Vörös, P.; Ranchin, B.; Vondrak, K.; Ariceta, G.; Zaloszyc, A.; Bayazit, A.K.; et al. Neutral pH and low–glucose degradation product dialysis fluids induce major early alterations of the peritoneal membrane in children on peritoneal dialysis. Kidney Int. 2018, 94, 419–429. [Google Scholar] [CrossRef]
- Yáñez-Mó, M.; Lara-Pezzi, E.; Selgas, R.; Ramírez-Huesca, M.; Domínguez-Jiménez, C.; Jiménez-Heffernan, J.A.; Aguilera, A.; Sánchez-Tomero, J.A.; Bajo, M.A.; Álvarez, V.; et al. Peritoneal Dialysis and Epithelial-to-Mesenchymal Transition of Mesothelial Cells. N. Engl. J. Med. 2003, 348, 403–413. [Google Scholar] [CrossRef]
- Aroeira, L.S.; Aguilera, A.; Sánchez-Tomero, J.A.; Bajo, M.A.; del Peso, G.; Jiménez-Heffernan, J.A.; Selgas, R.; López-Cabrera, M. Epithelial to Mesenchymal Transition and Peritoneal Membrane Failure in Peritoneal Dialysis Patients: Pathologic Significance and Potential Therapeutic Interventions. J. Am. Soc. Nephrol. 2007, 18, 2004–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, C.J. Glucotoxicity in Peritoneal Dialysis—Solutions for the Solution! Adv. Chronic Kidney Dis. 2007, 14, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Dousdampanis, P.; Musso, C.G.; Trigka, K. Icodextrin and peritoneal dialysis: Advantages and new applications. Int. Urol. Nephrol. 2018, 50, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Goossen, K.; Becker, M.; Marshall, M.R.; Bühn, S.; Breuing, J.; Firanek, C.A.; Hess, S.; Nariai, H.; Sloand, J.A.; Yao, Q.; et al. Icodextrin Versus Glucose Solutions for the Once-Daily Long Dwell in Peritoneal Dialysis: An Enriched Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Kidney Dis. 2020, 75, 830–846. [Google Scholar] [CrossRef] [Green Version]
- Moriishi, M.; Kawanishi, H. Icodextrin and Intraperitoneal Inflammation. Perit. Dial. Int. 2008, 28, S96–S100. [Google Scholar] [CrossRef] [PubMed]
- Velloso, M.S.S.; Otoni, A.; de Paula Sabino, A.; de Castro, W.V.; Pinto, S.W.L.; Marinho, M.A.S.; Rios, D.R.A. Peritoneal dialysis and inflammation. Clin. Chim. Acta 2014, 430, 109–114. [Google Scholar] [CrossRef]
- Arfeen, S.; Goodship, T.H.; Kirkwood, A.; Ward, M.K. The nutritional/metabolic and hormonal effects of 8 weeks of continuous ambulatory peritoneal dialysis with a 1% amino acid solution. Clin. Nephrol. 1990, 33, 192–199. [Google Scholar]
- Bartosova, M.; Schmitt, C.P. Biocompatible Peritoneal Dialysis: The Target Is Still Way Off. Front. Physiol. 2019, 9. [Google Scholar] [CrossRef]
- Bonomini, M.; Zammit, V.; Divino-Filho, J.C.; Davies, S.J.; Di Liberato, L.; Arduini, A.; Lambie, M. The osmo-metabolic approach: A novel and tantalizing glucose-sparing strategy in peritoneal dialysis. J. Nephrol. 2020, 1–17. [Google Scholar] [CrossRef]
- Bonomini, M.; Di Silvestre, S.; Di Tomo, P.; Di Pietro, N.; Mandatori, D.; Di Liberato, L.; Sirolli, V.; Chiarelli, F.; Indiveri, C.; Pandolfi, A.; et al. Effect of peritoneal dialysis fluid containing osmo-metabolic agents on human endothelial cells. Drug Des. Dev. Ther. 2016, 10, 3925–3932. [Google Scholar] [CrossRef] [Green Version]
- Bonomini, M.; Di Liberato, L.; Zammit, V.; Arduini, A. Current Opinion on Usage of L-Carnitine in End-Stage Renal Disease Patients on Peritoneal Dialysis. Molecules 2019, 24, 3449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonomini, M.; Pandolfi, A.; Di Liberato, L.; Di Silvestre, S.; Cnops, Y.; Di Tomo, P.; D’Arezzo, M.; Monaco, M.P.; Giardinelli, A.; Di Pietro, N.; et al. l-Carnitine is an osmotic agent suitable for peritoneal dialysis. Kidney Int. 2011, 80, 645–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonomini, M.; Di Liberato, L.; Del Rosso, G.; Stingone, A.; Marinangeli, G.; Consoli, A.; Bertoli, S.; De Vecchi, A.; Bosi, E.; Russo, R.; et al. Effect of an l-Carnitine–Containing Peritoneal Dialysate on Insulin Sensitivity in Patients Treated With CAPD: A 4-Month, Prospective, Multicenter Randomized Trial. Am. J. Kidney Dis. 2013, 62, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Livesey, G. Health potential of polyols as sugar replacers, with emphasis on low glycaemic properties. Nutr. Res. Rev. 2003, 16, 163–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazzato, G.; Coli, U.; Landini, S.; Fracasso, A.; Morachiello, P.; Righetto, F.; Scanferla, F.; Onesti, G. Xylitol as osmotic agent in CAPD: An alternative to glucose for uremic diabetic patients? Trans. Am. Soc. Artif. Intern. Organs 1982, 28, 280–286. [Google Scholar] [PubMed]
- Bensinger, S.J.; Walsh, P.T.; Zhang, J.; Carroll, M.; Parsons, R.; Rathmell, J.C.; Thompson, C.B.; Burchill, M.A.; Farrar, M.A.; Turka, L.A. Distinct IL-2 Receptor Signaling Pattern in CD4 + CD25 + Regulatory T Cells. J. Immunol. 2004, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, U.; Walther-Jallow, L.; Hofmann, A.; Spetz, A.L. Dendritic cells are able to produce IL-12p70 after uptake of apoptotic cells. Immunobiology 2011, 216. [Google Scholar] [CrossRef]
- Blanco, P.; Palucka, A.K.; Pascual, V.; Banchereau, J. Dendritic cells and cytokines in human inflammatory and autoimmune diseases. Cytokine Growth Factor Rev. 2008, 19. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Guo, S.; Hibbert, J.M.; Jain, V.; Singh, N.; Wilson, N.O.; Stiles, J.K. CXCL10/IP-10 in infectious diseases pathogenesis and potential therapeutic implications. Cytokine Growth Factor Rev. 2011, 22, 121–130. [Google Scholar] [CrossRef]
- Marques, R.E.; Guabiraba, R.; Russo, R.C.; Teixeira, M.M. Targeting CCL5 in inflammation. Expert Opin. Ther. Targets 2013, 17, 1439–1460. [Google Scholar] [CrossRef]
- Kumar-Singh, S.; Weyler, J.; Martin, M.J.H.; Vermeulen, P.B.; Van Marck, E. Angiogenic cytokines in mesothelioma: A study of VEGF, FGF-1 and -2, and TGFβ expression. J. Pathol. 1999, 189. [Google Scholar] [CrossRef]
- Chaudhary, K.; Khanna, R. Biocompatible peritoneal dialysis solutions: Do we have one? Clin. J. Am. Soc. Nephrol. 2010, 5, 723–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.K.; Chan, L.Y.Y.; Woo, J.C.Y.; Ho, S.K.N.; Lo, W.K.; Lai, K.N.; Chan, T.M. A 3-year, prospective, randomized, controlled study on amino acid dialysate in patients on CAPD. Am. J. Kidney Dis. 2003, 42, 173–183. [Google Scholar] [CrossRef]
- Hoff, C.M. In vitro biocompatibility performance of Physioneal. Kidney Int. 2003, 64, S57–S74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, H.; Lee, H.B. Effect of high glucose on peritoneal mesothelial cell biology. Perit. Dial. Int. 2000, 20, 15–18. [Google Scholar] [CrossRef]
- Bahl Lee, H.; Yu, M.R.A.; Sook Song, J. Reactive oxygen species amplify protein kinase C signaling in high glucose-induced fibronectin expression by human peritoneal mesothelial cells. Kidney Int. 2004, 65, 1170–1179. [Google Scholar]
- Ito, T.; Yorioka, N.; Yamamoto, M.; Kataoka, K.; Yamakido, M. Effect of Glucose on Intercellular Junctions of Cultured Human Peritoneal Mesothelial Cells. J. Am. Soc. Nephrol. 2000, 11, 1969–1979. [Google Scholar] [CrossRef]
- Leung, J.C.K.; Chan, L.Y.Y.; Li, F.F.K.; Tang, S.C.W.; Chan, K.W.; Chan, T.M.; Lam, M.F.; Wieslander, A.; Lai, K.N. Glucose degradation products downregulate ZO-1 expression in human peritoneal mesothelial cells: The role of VEGF. Nephrol. Dial. Transplant. 2005, 20, 1336–1349. [Google Scholar] [CrossRef] [Green Version]
- Cendoroglo, M.; Sundaram, S.; Jaber, B.L.; Pereira, B.J. Effect of glucose concentration, osmolality, and sterilization process of peritoneal dialysis fluids on cytokine production by peripheral blood mononuclear cells and polymorphonuclear cell functions in vitro. Am. J. Kidney Dis. 1998, 31, 273–282. [Google Scholar] [CrossRef]
- Wong, T.Y.H.; Phillips, A.O.; Witowski, J.; Topley, N. Glucose-mediated induction of TGF-β1 and MCP-1 in mesothelial cells in vitro is osmolality and polyol pathway dependent. Kidney Int. 2003, 63, 1404–1416. [Google Scholar] [CrossRef] [Green Version]
- Pochini, L.; Scalise, M.; Di Silvestre, S.; Belviso, S.; Pandolfi, A.; Arduini, A.; Bonomini, M.; Indiveri, C. Acetylcholine and acetylcarnitine transport in peritoneum: Role of the SLC22A4 (OCTN1) transporter. Biochim. Biophys. Acta Biomembr. 2016, 1858, 653–660. [Google Scholar] [CrossRef]
- Trombino, S.; Cesario, A.; Margaritora, S.; Granone, P.; Motta, G.; Falugi, C.; Russo, P. α7-Nicotinic Acetylcholine Receptors Affect Growth Regulation of Human Mesothelioma Cells. Cancer Res. 2004, 64, 135–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, P.; Sekhon, H.S.; Jia, Y.; Keller, J.A.; Blusztajn, J.K.; Mark, G.P.; Spindel, E.R. Acetylcholine Is Synthesized by and Acts as an Autocrine Growth Factor for Small Cell Lung Carcinoma. Cancer Res. 2003, 63, 214–221. [Google Scholar] [PubMed]
- Proskocil, B.J.; Sekhon, H.S.; Jia, Y.; Savchenko, V.; Blakely, R.D.; Lindstrom, J.; Spindel, E.R. Acetylcholine is an autocrine or paracrine hormone synthesized and secreted by airway bronchial epithelial cells. Endocrinology 2004, 145, 2498–2506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihara, T.; Otsubo, W.; Horiguchi, K.; Mikawa, S.; Kaji, N.; Iino, S.; Ozaki, H.; Hori, M. The anti-inflammatory pathway regulated via nicotinic acetylcholine receptors in rat intestinal mesothelial cells. J. Vet. Med. Sci. 2017, 79, 1795–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, C.; Tong, Y.; Li, J.; Lu, Z.; Yao, Y. The Protective Effect of Alpha 7 Nicotinic Acetylcholine Receptor Activation on Critical Illness and Its Mechanism. Int. J. Biol. Sci. 2017, 13, 46–56. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Yorioka, N. Peritoneal damage by peritoneal dialysis solutions. Clin. Exp. Nephrol. 2008, 12, 243–249. [Google Scholar] [CrossRef]
- Tobioka, H.; Sawada, N.; Zhong, Y.; Mori, M. Enhanced paracellular barrier function of rat mesothelial cells partially protects against cancer cell penetration. Br. J. Cancer 1996, 74, 439–445. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Yorioka, N.; Kyuden, Y.; Asakimori, Y.; Kiribayashi, K.; Ogawa, T.; Kohno, N. Effect of glucose polymer on the intercellular junctions of cultured human peritoneal mesothelial cells. Nephron Clin. Pract. 2003, 93. [Google Scholar] [CrossRef]
- Correa-Rotter, R.; Cueto-Manzano, A. The Problem of the High Transporter: Is Survival Decreased? Perit. Dial. Int. 2001, 21, 75–79. [Google Scholar] [CrossRef]
- Selgas, R.; Bajo, A.; Jiménez-Heffernan, J.A.; Sánchez-Tomero, J.A.; del Peso, G.; Aguilera, A.; López-Cabrera, M. Epithelial-to-mesenchymal transition of the mesothelial cell—Its role in the response of the peritoneum to dialysis. Nephrol. Dial. Transplant. 2006, 21. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Lu, Y.; Li, Y.; Gao, L.; Shen, H.; Song, K. Hydrogen sulfide inhibits epithelial-mesenchymal transition in peritoneal mesothelial cells. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.H.; Jung, J.Y.; Yoon, M.O.; Song, A.; Lee, H.; Ro, H.; Hwang, Y.H.; Kim, D.K.; Margetts, P.; Ahn, C. Intra-peritoneal interleukin-6 system is a potent determinant of the baseline peritoneal solute transport in incident peritoneal dialysis patients. Nephrol. Dial. Transplant. 2010, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witowski, J.; Jörres, A.; Coles, G.A.; Williams, J.D.; Topley, N. Superinduction of IL-6 synthesis in human peritoneal mesothelial cells is related to the induction and stabilization of IL-6 mRNA. Kidney Int. 1996, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, V.; Platell, C.; Hall, J.C. Peritoneal mesothelial cells produce inflammatory related cytokines. ANZ J. Surg. 2004, 74, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues-Díez, R.; Aroeira, L.S.; Orejudo, M.; Bajo, M.A.; Heffernan, J.J.; Rodrigues-Díez, R.R.; Rayego-Mateos, S.; Ortiz, A.; Gonzalez-Mateo, G.; López-Cabrera, M.; et al. IL-17A is a novel player in dialysis-induced peritoneal damage. Kidney Int. 2014, 86, 303–315. [Google Scholar] [CrossRef] [Green Version]
- Liappas, G.; González-Mateo, G.T.; Sánchez-Díaz, R.; Lazcano, J.J.; Lasarte, S.; Matesanz-Marín, A.; Zur, R.; Ferrantelli, E.; Ramírez, L.G.; Aguilera, A.; et al. Immune-regulatory molecule CD69 controls peritoneal fibrosis. J. Am. Soc. Nephrol. 2016, 27. [Google Scholar] [CrossRef] [Green Version]
- Vila Cuenca, M.; Keuning, E.D.; Talhout, W.; Paauw, N.J.; van Ittersum, F.J.; ter Wee, P.M.; Beelen, R.H.J.; Vervloet, M.G.; Ferrantelli, E. Differences in peritoneal response after exposure to low-GDP bicarbonate/lactate-buffered dialysis solution compared to conventional dialysis solution in a uremic mouse model. Int. Urol. Nephrol. 2018, 50. [Google Scholar] [CrossRef] [Green Version]
- Visser, C.E.; Tekstra, J.; Brouwer-Steenbergen, J.J.E.; Tuk, C.W.; Boorsma, D.M.; Sampat-Sardjoepersad, S.C.; Meijer, S.; Krediet, R.T.; Beelen, R.H.J. Chemokines produced by mesothelial cells: huGRO-α, IP-10, MCP-1 and RANTES. Clin. Exp. Immunol. 1998, 112. [Google Scholar] [CrossRef]
- Li, F.K.; Davenport, A.; Robson, R.L.; Loetscher, P.; Rothlein, R.; Williams, J.D.; Topley, N. Leukocyte migration across human peritoneal mesothelial cells is dependent on directed chemokine secretion and ICAM-1 expression. Kidney Int. 1998, 54, 2170–2183. [Google Scholar] [CrossRef] [Green Version]
- Aroeira, L.S.; Aguilera, A.; Selgas, R.; Ramírez-Huesca, M.; Pérez-Lozano, M.L.; Cirugeda, A.; Bajo, M.A.; del Peso, G.; Sánchez-Tomero, J.A.; López-Cabrera, M.; et al. Mesenchymal conversion of mesothelial cells as a mechanism responsible for high solute transport rate in peritoneal dialysis: Role of vascular endothelial growth factor. Am. J. Kidney Dis. 2005, 46, 938–948. [Google Scholar] [CrossRef] [PubMed]
- Ogata, S.; Yorioka, N.; Kohno, N. Glucose and prednisolone alter basic fibroblast growth factor expression in peritoneal mesothelial cells and fibroblasts. J. Am. Soc. Nephrol. 2001, 12, 2787–2796. [Google Scholar] [PubMed]
- Patel, P.; West-Mays, J.; Kolb, M.; Rodrigues, J.C.; Hoff, C.M.; Margetts, P.J. Platelet derived growth factor B and epithelial mesenchymal transition of peritoneal mesothelial cells. Matrix Biol. 2010, 29, 97–106. [Google Scholar] [CrossRef]
- Misra, P.S.; Nessim, S.J.; Perl, J. “Biocompatible” Neutral pH Low-GDP Peritoneal Dialysis Solutions: Much Ado About Nothing? Semin. Dial. 2017, 30. [Google Scholar] [CrossRef] [PubMed]
- Blake, P.G. Is the peritoneal dialysis biocompatibility hypothesis dead? Kidney Int. 2018, 94, 246–248. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| GLUCOSE- BASED PD SOLUTIONS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Physioneal 40® | Dianeal PD4® | BicaVera® | |||||||
| mMol/L | LOW | MEDIUM | HIGH | LOW | MEDIUM | HIGH | LOW | MEDIUM | HIGH |
| Sodium | 132 | 132 | 132 | 132 | 132 | 132 | 134 | 134 | 134 |
| Calcium | 1.25 | 1.25 | 1.25 | 1.25 | 1.25 | 1.25 | 1.75 | 1.75 | 1.75 |
| Magnesium | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.5 | 0.5 | 0.5 |
| Chloride | 95 | 95 | 95 | 95 | 95 | 95 | 104.5 | 104.5 | 104.5 |
| Glucose | 75.5 | 126 | 214 | 75.5 | 126 | 214 | 83.25 | 126.1 | 235.9 |
| Xylitol | - | - | - | - | - | - | - | - | - |
| Lactate | 15 | 15 | 15 | 40 | 40 | 40 | - | - | - |
| Bicarbonate | 25 | 25 | 25 | - | - | - | 34 | 34 | 34 |
| Icodextrin | - | - | - | - | - | - | - | - | - |
| Aminoacids | - | - | - | - | - | - | - | - | - |
| l-carnitine | - | - | - | - | - | - | - | - | - |
| Osmolarity (mOsmol/L) | 344 | 395 | 483 | 344 | 395 | 483 | 358 | 401 | 511 |
| pH | 7.4 | 7.4 | 7.4 | 5–6.5 | 5–6.5 | 5–6.5 | 7.4 | 7.4 | 7.4 |
| GLUCOSE- FREE PD SOLUTIONS | GLUCOSE-SPARING PD SOLUTIONS | ||||||||
| Extraneal® | Nutrineal® | − l-CARNITINE | + l-CARNITINE | ||||||
| mMol/L | Icodextrin 7.5% | Amino acids 1.1% | LOW | MEDIUM | HIGH | LOW | MEDIUM | HIGH | |
| Sodium | 133 | 132 | 134 | 134 | 134 | 134 | 134 | 134 | |
| Calcium | 1.75 | 1.25 | 1.75 | 1.75 | 1.75 | 1.75 | 1.75 | 1.75 | |
| Magnesium | 0.25 | 0.25 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | |
| Chloride | 96 | 105 | 103.5 | 103.5 | 103.5 | 103.5 | 103.5 | 103.5 | |
| Glucose | - | - | 27.7 | 27.7 | 83 | 27.7 | 27.7 | 83 | |
| Xylitol | - | - | 46 | 98.6 | 125 | 46 | 98.6 | 125 | |
| Lactate | 40 | 40 | 35 | 35 | 35 | 35 | 35 | 35 | |
| Bicarbonate | - | - | - | - | - | - | - | - | |
| Icodextrin | 7.5 (%) | - | - | - | - | - | - | - | |
| Aminoacids | - | 87.16 | - | - | - | - | - | - | |
| l-carnitine | - | - | - | - | - | 1.24 | 1.24 | 1.24 | |
| Osmolarity (mOsmol/L) | 284 | 365 | 351.9 | 404.5 | 486.2 | 351.9 | 404.5 | 486.2 | |
| pH | 5–6 | 6.6 | 5.5 ± 0.5 | 5.5 ± 0.5 | 5.5 ± 0.5 | 5.5 ± 0.5 | 5.5 ± 0.5 | 5.5 ± 0.5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccapane, F.; Bonomini, M.; Castellano, G.; Gerbino, A.; Carmosino, M.; Svelto, M.; Arduini, A.; Procino, G. A Novel Formulation of Glucose-Sparing Peritoneal Dialysis Solutions with l-Carnitine Improves Biocompatibility on Human Mesothelial Cells. Int. J. Mol. Sci. 2021, 22, 123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010123
Piccapane F, Bonomini M, Castellano G, Gerbino A, Carmosino M, Svelto M, Arduini A, Procino G. A Novel Formulation of Glucose-Sparing Peritoneal Dialysis Solutions with l-Carnitine Improves Biocompatibility on Human Mesothelial Cells. International Journal of Molecular Sciences. 2021; 22(1):123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010123
Chicago/Turabian StylePiccapane, Francesca, Mario Bonomini, Giuseppe Castellano, Andrea Gerbino, Monica Carmosino, Maria Svelto, Arduino Arduini, and Giuseppe Procino. 2021. "A Novel Formulation of Glucose-Sparing Peritoneal Dialysis Solutions with l-Carnitine Improves Biocompatibility on Human Mesothelial Cells" International Journal of Molecular Sciences 22, no. 1: 123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22010123