
Treating Prostate Cancer by Antibody–Drug Conjugates

 , , ,
, , ,
Abstract
:1. Introduction
2. Current Therapeutic Landscape of nmCRPC
3. Current Therapeutic Landscape of mCRPC
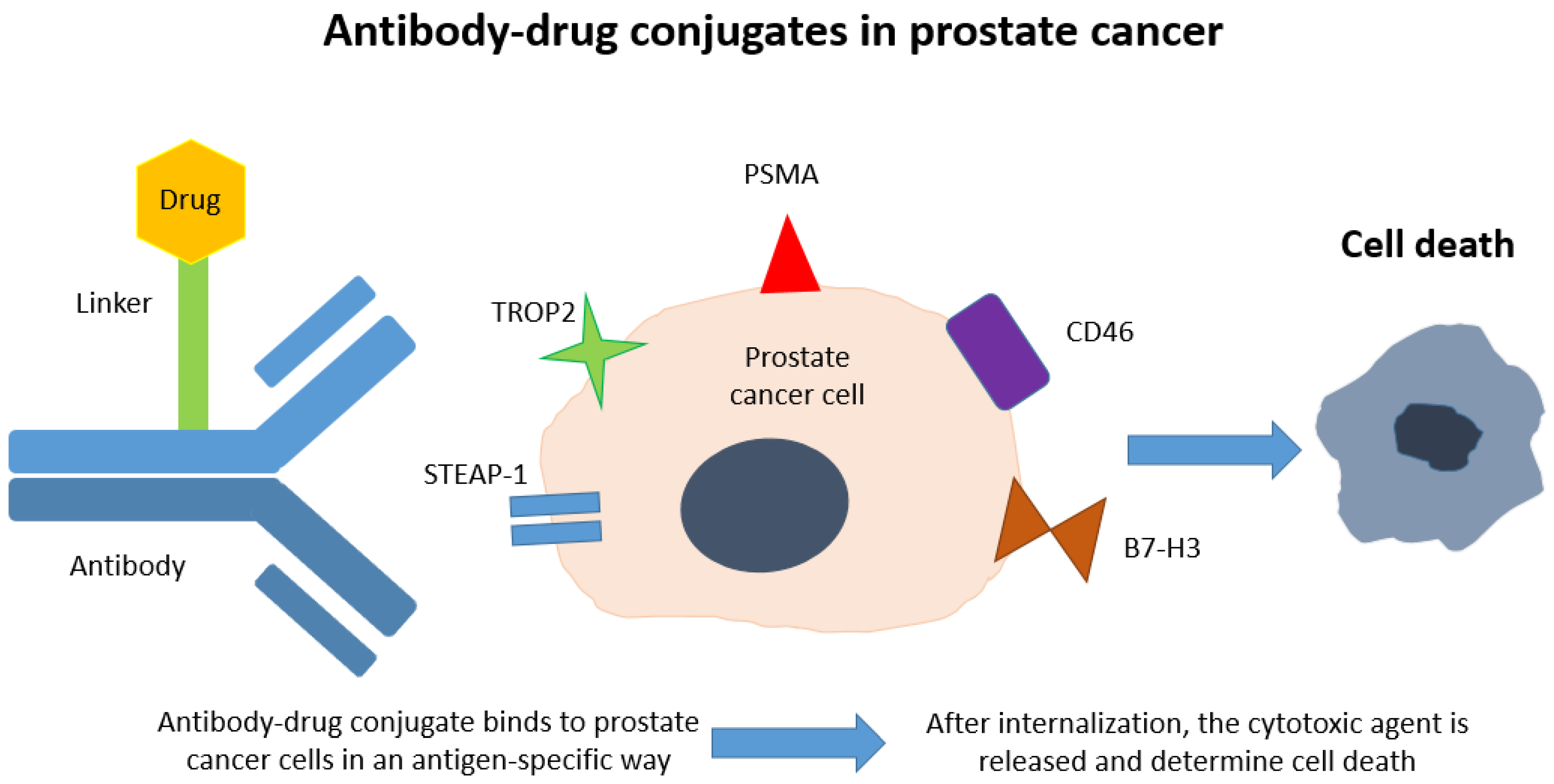
4. Treating Prostate Cancer by ADC
4.1. STEAP1
4.2. TROP2
4.3. PSMA
4.4. CD46
4.5. B7-H3
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Piva, F.; Tartari, F.; Giulietti, M.; Aiello, M.M.; Cheng, L.; Lopez-Beltran, A.; Mazzucchelli, R.; Cimadamore, A.; Cerqueti, R.; Battelli, N.; et al. Predicting future cancer burden in the United States by artificial neural networks. Future Oncol. 2021, 17, 159–168. [Google Scholar] [CrossRef]
- Teo, M.Y.; Rathkopf, D.E.; Kantoff, P. Treatment of advanced prostate cancer. Annu. Rev. Med. 2019, 70, 479–499. [Google Scholar] [CrossRef]
- Aurilio, G.; Cimadamore, A.; Santoni, M.; Nolè, F.; Scarpelli, M.; Massari, F.; Lopez-Beltran, A.; Cheng, L.; Montironi, R. New Frontiers in Prostate Cancer Treatment: Are We Ready for Drug Combinations with Novel Agents? Cells 2020, 9, 1522. [Google Scholar] [CrossRef] [PubMed]
- Nevedomskaya, E.; Baumgart, S.J.; Haendler, B. Recent advances in prostate cancer treatment and drug discovery. Int. J. Mol. Sci. 2018, 19, 1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafi, A.A.; Yen, A.E.; Weigel, N.L. Androgen receptors in hormone-dependent and castration-resistant prostate cancer. Pharmacol. Ther. 2013, 140, 223–238. [Google Scholar] [CrossRef]
- Caubet, J.F.; Tosteson, T.D.; Dong, E.W.; Naylon, E.M.; Whiting, G.W.; Ernstoff, M.S.; Ross, S.D. Maximum androgen blockade in advanced prostate cancer: A meta-analysis of published randomized controlled trials using nonsteroidal antiandrogens. Urology 1997, 49, 71–78. [Google Scholar] [CrossRef]
- Danila, D.C. Antibody–Drug Conjugates in Prostate Cancer. Clin. Adv. Hematol. Oncol. 2020, 18, 447–449. [Google Scholar]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [Green Version]
- Mateo, J.; Fizazi, K.; Gillessen, S.; Heidenreich, A.; Perez-Lopez, R.; Oyen, W.J.; Shore, N.; Smith, M.; Sweeney, C.; Tombal, B.; et al. Managing Nonmetastatic Castration-resistant Prostate Cancer. Eur. Urol. 2019, 75, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Gartrell, B.A.; Saad, F. Managing bone metastases and reducing skeletal related events in prostate cancer. Nat. Rev. Clin. Oncol. 2014, 11, 335–345. [Google Scholar] [CrossRef]
- Hussain, M.; Fizazi, K.; Saad, F.; Rathenborg, P.; Shore, N.; Ferreira, U.; Ivashchenko, P.; Demirhan, E.; Modelska, K.; Phung, D.; et al. Enzalutamide in Men with Nonmetastatic, Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2018, 378, 2465–2474. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Fizazi, K.; Saad, F.; Shore, N.D.; De Giorgi, U.; Penson, D.F.; Ferreira, U.; Efstathiou, E.; Madziarska, K.; Kolinsky, M.P.; et al. Enzalutamide and Survival in Nonmetastatic, Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Antonarakis, E.S.; Ryan, C.J.; Berry, W.R.; Shore, N.D.; Liu, G.; Alumkal, J.J.; Higano, C.S.; Maneval, E.C.; Bandekar, R.; et al. Phase 2 Study of the Safety and Antitumor Activity of Apalutamide (ARN-509), a Potent Androgen Receptor Antagonist, in the High-risk Nonmetastatic Castration-resistant Prostate Cancer Cohort. Eur. Urol. 2016, 70, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.R.; Saad, F.; Chowdhury, S.; Oudard, S.; Hadaschik, B.A.; Graff, J.N.; Olmos, D.; Mainwaring, P.N.; Lee, J.Y.; Uemura, H.; et al. Apalutamide Treatment and Metastasis-free Survival in Prostate Cancer. N. Engl. J. Med. 2018, 378, 1408–1418. [Google Scholar] [CrossRef]
- Small, E.; Saad, F.; Chowdhury, S.; Oudard, S.; Hadaschik, B.; Graff, J.; Olmos, D.; Mainwaring, P.; Lee, J.; Uemura, H.; et al. Apalutamide and overall survival in non-metastatic castration-resistant prostate cancer. Ann. Oncol. 2019, 30, 1813–1820. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Shore, N.; Tammela, T.L.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; Kuss, I.; et al. Darolutamide in Nonmetastatic, Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2019, 380, 1235–1246. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Shore, N.D.; Tammela, T.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; Kuss, I.; et al. Overall survival (OS) results of phase III ARAMIS study of darolutamide (DARO) added to androgen deprivation therapy (ADT) for nonmetastatic castration-resistant prostate cancer (nmCRPC). J. Clin. Oncol. 2020, 38, 5514. [Google Scholar] [CrossRef]
- Hird, A.E.; Magee, D.E.; Bhindi, B.; Ye, X.Y.; Chandrasekar, T.; Goldberg, H.; Klotz, L.; Fleshner, N.; Satkunasivam, R.; Klaassen, Z.; et al. A Systematic Review and Network Meta-analysis of Novel Androgen Receptor Inhibitors in Non-metastatic Castration-resistant Prostate Cancer. Clin. Genitourin. Cancer 2020, 18, 343–350. [Google Scholar] [CrossRef]
- Tannock, I.F.; Osoba, D.; Stockler, M.R.; Ernst, D.; Neville, A.J.; Moore, M.J.; Armitage, G.R.; Wilson, J.J.; Venner, P.M.; Coppin, C.M.; et al. Chemotherapy with mitoxantrone plus prednisone or prednisone alone for symptomatic hormone-resistant prostate cancer: A Canadian randomized trial with palliative end points. J. Clin. Oncol. 1996, 14, 1756–1764. [Google Scholar] [CrossRef] [PubMed]
- Quinn, D.I.; Sandler, H.M.; Horvath, L.G.; Goldkorn, A.; Eastham, J.A. The evolution of chemotherapy for the treatment of prostate cancer. Ann. Oncol. 2017, 28, 2658–2669. [Google Scholar] [CrossRef]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for Advanced Prostate Cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [Green Version]
- Petrylak, D.P.; Tangen, C.M.; Hussain, M.H.A.; Lara, P.N.; Jones, J.A.; Taplin, M.E.; Burch, P.A.; Berry, D.; Moinpour, C.; Kohli, M.; et al. Docetaxel and Estramustine Compared with Mitoxantrone and Prednisone for Advanced Refractory Prostate Cancer. N. Engl. J. Med. 2004, 351, 1513–1520. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef]
- De Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; MacHiels, J.P.; Kocak, I.; Gravis, G.; Bodrogi, I.; MacKenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- de Wit, R.; de Bono, J.; Sternberg, C.N.; Fizazi, K.; Tombal, B.; Wülfing, C.; Kramer, G.; Eymard, J.-C.; Bamias, A.; Carles, J.; et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 2506–2518. [Google Scholar] [CrossRef]
- de Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B.J.; Saad, F.; et al. Abiraterone and increased survival in metastatic prostate cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef]
- Ryan, C.J.; Smith, M.R.; de Bono, J.S.; Molina, A.; Logothetis, C.J.; de Souza, P.; Fizazi, K.; Mainwaring, P.; Piulats, J.M.; Ng, S.; et al. Abiraterone in Metastatic Prostate Cancer without Previous Chemotherapy. N. Engl. J. Med. 2013, 368, 138–148. [Google Scholar] [CrossRef] [Green Version]
- Ryan, C.J.; Smith, M.R.; Fizazi, K.; Saad, F.; Mulders, P.F.A.; Sternberg, C.N.; Miller, K.; Logothetis, C.J.; Shore, N.D.; Small, E.J.; et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): Final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015, 16, 152–160. [Google Scholar] [CrossRef]
- Fizazi, K.; Tran, N.P.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroglu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.-E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in Metastatic Prostate Cancer before Chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy with Enzalutamide or Placebo in Men with Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Ciccarese, C.; Santoni, M.; Brunelli, M.; Buti, S.; Modena, A.; Nabissi, M.; Artibani, W.; Martignoni, G.; Montironi, R.; Tortora, G.; et al. AR-V7 and prostate cancer: The watershed for treatment selection? Cancer Treat. Rev. 2016, 43, 27–35. [Google Scholar] [CrossRef]
- Sydes, M.R.; Spears, M.R.; Mason, M.D.; Clarke, N.W.; Dearnaley, D.P.; de Bono, J.S.; Attard, G.; Chowdhury, S.; Cross, W.; Gillessen, S.; et al. Adding abiraterone or docetaxel to long-term hormone therapy for prostate cancer: Directly randomised data from the STAMPEDE multi-arm, multi-stage platform protocol. Ann. Oncol. 2018, 29, 1235–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Nunno, V.; Santoni, M.; Mollica, V.; Conti, A.; Montironi, R.; Battelli, N.; Ardizzoni, A.; Massari, F. Systemic Treatment for Metastatic Hormone Sensitive Prostate Cancer: A Comprehensive Meta-Analysis Evaluating Efficacy and Safety in Specific Sub-Groups of Patients. Clin. Drug Investig. 2020, 40, 211–226. [Google Scholar] [CrossRef]
- Kinsey, E.N.; Zhang, T.; Armstrong, A.J. Metastatic Hormone-Sensitive Prostate Cancer: A Review of the Current Treatment Landscape. Cancer J. 2020, 26, 64–75. [Google Scholar] [CrossRef]
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N. Engl. J. Med. 2016. [Google Scholar] [CrossRef]
- Modena, A.; Ciccarese, C.; Iacovelli, R.; Brunelli, M.; Montironi, R.; Fiorentino, M.; Tortora, G.; Massari, F. Immune checkpoint inhibitors and prostate cancer: A new frontier? Oncol. Rev. 2016, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massari, F.; Ciccarese, C.; Caliò, A.; Munari, E.; Cima, L.; Porcaro, A.B.; Novella, G.; Artibani, W.; Sava, T.; Eccher, A.; et al. Magnitude of PD-1, PD-L1 and T Lymphocyte Expression on Tissue from Castration-Resistant Prostate Adenocarcinoma: An Exploratory Analysis. Target. Oncol. 2015, 11, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Abida, W.; Cheng, M.L.; Armenia, J.; Middha, S.; Autio, K.A.; Vargas, H.A.; Rathkopf, D.; Morris, M.J.; Danila, D.C.; Slovin, S.F.; et al. Analysis of the Prevalence of Microsatellite Instability in Prostate Cancer and Response to Immune Checkpoint Blockade. JAMA Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hubert, R.S.; Vivanco, I.; Chen, E.; Rastegar, S.; Leong, K.; Mitchell, S.C.; Madraswala, R.; Zhou, Y.; Kuo, J.; Raitano, A.B.; et al. STEAP: A prostate-specific cell-surface antigen highly expressed in human prostate tumors. Proc. Natl. Acad. Sci. USA 1999, 96, 14523–14528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oosterheert, W.; Gros, P. Cryo-Electron microscopy structure and potential enzymatic function of human six-transmembrane epithelial antigen of the prostate 1 (STEAP1). J. Biol. Chem. 2020, 295, 9502–9512. [Google Scholar] [CrossRef]
- Gomes, I.M.; Rocha, S.M.; Gaspar, C.; Alvelos, M.I.; Santos, C.R.; Socorro, S.; Maia, C.J. Knockdown of STEAP1 inhibits cell growth and induces apoptosis in LNCaP prostate cancer cells counteracting the effect of androgens. Med. Oncol. 2018, 35. [Google Scholar] [CrossRef] [PubMed]
- Esmaeili, S.-A.; Nejatollahi, F.; Sahebkar, A. Inhibition of Intercellular Communication between Prostate Cancer Cells by A Specific Anti-STEAP-1 Single Chain Antibody. Anticancer Agents Med. Chem. 2017, 18, 1674–1679. [Google Scholar] [CrossRef] [PubMed]
- Carrasquillo, J.A.; Fine, B.M.; Pandit-Taskar, N.; Larson, S.M.; Fleming, S.E.; Fox, J.J.; Cheal, S.M.; O’Donoghue, J.A.; Ruan, S.; Ragupathi, G.; et al. Imaging patients with metastatic castration-resistant prostate cancer using 89Zr-DFO-MSTP2109A anti-STEAP1 antibody. J. Nucl. Med. 2019, 60, 1517–1523. [Google Scholar] [CrossRef] [Green Version]
- Danila, D.C.; Szmulewitz, R.Z.; Vaishampayan, U.; Higano, C.S.; Baron, A.D.; Gilbert, H.N.; Brunstein, F.; Milojic-Blair, M.; Wang, B.; Kabbarah, O.; et al. Phase i Study of DSTP3086S, an antibody–drug conjugate targeting six-transmembrane epithelial antigen of prostate 1, in metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2019, 37, 3518–3527. [Google Scholar] [CrossRef]
- Shvartsur, A.; Bonavida, B. Trop2 and its overexpression in cancers: Regulation and clinical/therapeutic implications. Genes Cancer 2014, 6, 84–105. [Google Scholar] [CrossRef] [Green Version]
- Trerotola, M.; Ganguly, K.K.; Fazli, L.; Fedele, C.; Lu, H.; Dutta, A.; Liu, Q.; De Angelis, T.; Riddell, L.W.; Riobo, N.A.; et al. Trop-2 is up-regulated in invasive prostate cancer and displaces FAK from focal contacts. Oncotarget 2015, 6, 14318–14328. [Google Scholar] [CrossRef] [Green Version]
- Hsu, E.C.; Rice, M.A.; Bermudez, A.; Marques, F.J.G.; Aslan, M.; Liu, S.; Ghoochani, A.; Zhang, C.A.; Chen, Y.S.; Zlitni, A.; et al. Trop2 is a driver of metastatic prostate cancer with neuroendocrine phenotype via PARP1. Proc. Natl. Acad. Sci. USA 2020, 117, 2032–2042. [Google Scholar] [CrossRef] [Green Version]
- Ge, R.; Wang, Z.; Montironi, R.; Jiang, Z.; Cheng, M.; Santoni, M.; Huang, K.; Massari, F.; Lu, X.; Cimadamore, A.; et al. Epigenetic modulations and lineage plasticity in advanced prostate cancer. Ann. Oncol. 2020, 31, 470–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santoni, M.; Conti, A.; Burattini, L.; Berardi, R.; Scarpelli, M.; Cheng, L.; Lopez-Beltran, A.; Cascinu, S.; Montironi, R. Neuroendocrine differentiation in prostate cancer: Novel morphological insights and future therapeutic perspectives. Biochim. Biophys. Acta Rev. Cancer 2014, 1846, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Sacituzumab Govitecan: First Approval. Drugs 2020, 80, 1019–1025. [Google Scholar] [CrossRef]
- Mollica, V.; Rizzo, A.; Montironi, R.; Cheng, L.; Giunchi, F.; Schiavina, R.; Santoni, M.; Fiorentino, M.; Montironi, R.; Brunocilla, E.; et al. Current Strategies and Novel Therapeutic Approaches for Metastatic Urothelial Carcinoma. Cancers 2020, 12, 1449. [Google Scholar] [CrossRef]
- Barve, A.; Jin, W.; Cheng, K. Prostate cancer relevant antigens and enzymes for targeted drug delivery. J. Control. Release 2014, 187, 118–132. [Google Scholar] [CrossRef] [Green Version]
- Olson, W.C.; Israel, R.J. Antibody–drug conjugates targeting prostate-specific membrane antigen. Front. Biosci. Landmark 2014, 19, 12–33. [Google Scholar] [CrossRef]
- Fendler, W.P.; Rahbar, K.; Herrmann, K.; Kratochwil, C.; Eiber, M. 177Lu-PSMA raDioligand therapy for prostate cancer. J. Nucl. Med. 2017, 58, 1196–1200. [Google Scholar] [CrossRef] [Green Version]
- Niaz, M.O.; Sun, M.; Ramirez-Fort, M.; Niaz, M.J. Prostate-Specific Membrane Antigen Based Antibody–drug Conjugates for Metastatic Castration-resistance Prostate Cancer. Cureus 2020. [Google Scholar] [CrossRef] [Green Version]
- Galsky, M.D.; Eisenberger, M.; Moore-Cooper, S.; Kelly, W.K.; Slovin, S.F.; Delacruz, A.; Lee, Y.; Webb, I.J.; Scher, H.I. Phase I trial of the prostate-specific membrane antigen-directed immunoconjugate MLN2704 in patients with progressive metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2008, 26, 2147–2154. [Google Scholar] [CrossRef] [PubMed]
- Milowsky, M.I.; Galsky, M.D.; Morris, M.J.; Crona, D.J.; George, D.J.; Dreicer, R.; Tse, K.; Petruck, J.; Webb, I.J.; Bander, N.H.; et al. Phase 1/2 multiple ascending dose trial of the prostate-specific membrane antigen-targeted antibody drug conjugate MLN2704 in metastatic castration-resistant prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 530.e15–530.e21. [Google Scholar] [CrossRef] [Green Version]
- Petrylak, D.P.; Kantoff, P.; Vogelzang, N.J.; Mega, A.; Fleming, M.T.; Stephenson, J.J.; Frank, R.; Shore, N.D.; Dreicer, R.; McClay, E.F.; et al. Phase 1 study of PSMA ADC, an antibody–drug conjugate targeting prostate-specific membrane antigen, in chemotherapy-refractory prostate cancer. Prostate 2019, 79, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Cardone, J.; Le Friec, G.; Kemper, C. CD46 in innate and adaptive immunity: An update. Clin. Exp. Immunol. 2011, 164, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Elvington, M.; Liszewski, M.K.; Atkinson, J.P. CD46 and Oncologic Interactions: Friendly Fire against Cancer. Antibodies 2020, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Liu, Y.; Behrens, C.R.; Bidlingmaier, S.; Lee, N.K.; Aggarwal, R.; Sherbenou, D.W.; Burlingame, A.L.; Hann, B.C.; Simko, J.P.; et al. Targeting CD46 for both adenocarcinoma and neuroendocrine prostate cancer. JCI Insight 2018, 3, e121497. [Google Scholar] [CrossRef] [Green Version]
- Kontos, F.; Michelakos, T.; Kurokawa, T.; Sadagopan, A.; Schwab, J.H.; Ferrone, C.R.; Ferrone, S. B7-H3: An attractive target for antibody-based immunotherapy. Clin. Cancer Res. 2020, clincanres.2584.2020. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, G.; Zhang, W.; Wei, X.; Hou, J.; Huang, Y. B7-H3 Promotes Prostate Cancer Progression in Mice by Antagonizing Myeloid-Derived Suppressor Cell Apoptosis. Technol. Cancer Res. Treat. 2020, 19, 1533033820971649. [Google Scholar] [CrossRef]
- Bonk, S.; Tasdelen, P.; Kluth, M.; Hube-Magg, C.; Makrypidi-Fraune, G.; Möller, K.; Höflmayer, D.; Dwertmann Rico, S.; Büscheck, F.; Minner, S.; et al. High B7-H3 expression is linked to increased risk of prostate cancer progression. Pathol. Int. 2020, 70, 733–742. [Google Scholar] [CrossRef]
- Scribner, J.A.; Brown, J.G.; Sharma, S.; Li, H.; Chiechi, M.; Li, P.; Son, T.; De Costa, A.; Chen, Y.; Chen, F.; et al. Abstract 820: Preclinical development of MGC018, a duocarmycin-based antibody–drug conjugate targeting B7-H3 for solid cancer. Cancer Res. 2018, 78 (Suppl. 13). [Google Scholar] [CrossRef] [Green Version]
- García-Alonso, S.; Ocaña, A.; Pandiella, A. Resistance to Antibody–Drug Conjugates. Cancer Res. 2018, 78, 2159–2165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khongorzul, P.; Ling, C.J.; Khan, F.U.; Ihsan, A.U.; Zhang, J. Antibody–Drug Conjugates: A Comprehensive Review. Mol. Cancer Res. 2020, 18, 3–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chau, C.H.; Steeg, P.S.; Figg, W.D. Antibody–drug conjugates for cancer. Lancet 2019, 394, 793–804. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study [Author, Year] | Treatment | Clinical Setting | MFS Benefit | OS Benefit | Adverse Events of Any Grade |
|---|---|---|---|---|---|
| PROSPER [Hussain et al., 2018] [12,13] | Enzalutamide + ADT (vs. placebo + ADT) | nmCRPC | 36.6 months vs. 14.7 months (p < 0.001) | 67.0 months vs. 56.3 months (p = 0.001) | More frequently (Enza vs. placebo):
|
| SPARTAN [Smith et al., 2018] [15,16] | Apalutamide + ADT (vs. placebo + ADT) | High-risk nmCRPC | 40.5 months vs. 16.2 months (p < 0.001) | Median OS not reached in the Apa or the placebo group. 25% reduction in the risk of death (HR for Apa vs. placebo, 0.75; 95% CI 0.59–0.96; p = 0.0197) [16] | More frequently (Apa vs. placebo):
|
| ARAMIS [Fizazi et al., 2019] [17,18] | Darolutamide + ADT (vs. placebo + ADT) | High-risk nmCRPC | 40.4 months vs. 18.4 months (p < 0.001) | Percentage of pts alive at 3 years: 83% vs. 77% (p = 0.003) [18] | More frequently (Daro vs. placebo):
|
| Study [Author, Year] | Treatment | Clinical Setting | OS Benefit | PFS Benefit | Adverse Events of any Grade |
|---|---|---|---|---|---|
| TAX 327 [Tannock et al., 2004] [22] | Docetaxel * (vs. mitoxantrone) | mCRPC | 18.9 months vs. 16.4 months (p = 0.009) | - | More frequently (dtx vs. mtx):
|
| SWOG 99–16 [Petrylak et al., 2004] [23] | Docetaxel + estramustine (vs. mitoxantrone) | mCRPC | 17.5 months vs. 15.6 months (p = 0.02) | 6.3 months vs. 3.2 months (p < 0.001) in terms of TTP | More toxicity due to the addition of estramustine |
| CHARTEED [Sweeney et al., 2015] [24] | Docetaxel + ADT (vs. ADT alone) | High volume mHSPC | 57.6 months vs. 44.0 months (p < 0.001) | 33.0 months vs. 19.8 months (p < 0.001) in terms of cPFS | More frequently with dtx + ADT (only high grade described):
|
| TROPIC [De Bono et al., 2010] [25] | Cabazitaxel (vs. mitoxantrone) | mCRPC post- docetaxel | 15.1 months vs. 12.7 months (p < 0.0001) | 2.8 months vs. 1.4 months (p < 0.0001) | More frequently (caba vs. mtx):
|
| CARD [De Wit et al., 2019] [26] | Cabazitaxel (vs. abiraterone acetate + prednisone or enzalutamide) | mCRPC after docetaxel and abiraterone acetate + prednisone or enzalutamide | 13.6 months vs. 11.0 months (p = 0.008) | 8.0 months vs. 3.7 months (p < 0.001) | More frequently (caba vs. abi/enza):
|
| COU-AA-301 [De Bono et al., 2011] [27] | Abiraterone acetate + prednisone (vs. placebo) | mCRPC post- docetaxel | 15.8 months vs. 11.2 months (p < 0.001) | 5.6 months vs. 3.6 months (p < 0.001) in terms of rPFS | More frequently (abi vs. placebo):
|
| COU-AA-302 [Ryan et al., 2013] [28,29] | Abiraterone acetate + prednisone (vs. placebo) | mCRPC pre- docetaxel | 34.7 months vs. 30.3 months (p = 0.003) | 16.5 months vs. 8.3 months (p < 0.001) in terms of rPFS | More frequently (abi vs. placebo):
|
| LATITUDE [Fizazi et al., 2017] [30] | Abiraterone acetate + prednisone (vs. placebo) | High-risk mHSPC | 53.5 months vs. 36.5 months (p < 0.0001) | 33.0 months vs. 14.8 months (p < 0.001) in terms of rPFS | More frequently (abi vs. placebo):
|
| AFFIRM [Scher et al., 2012] [31] | Enzalutamide (vs. placebo) | mCRPC post- docetaxel | 18.4 months vs. 13.6 months (p < 0.001) | 8.3 months vs. 2.9 months (p < 0.001) in terms of rPFS | More frequently (enza vs. placebo):
|
| PREVAIL [Beer et al. 2014] [32] | Enzalutamide (vs. placebo) | mCRPC pre- docetaxel | 36.0 months vs. 31.0 months (p < 0.001) | 65% vs. 14% at 12 months (p < 0.001) in terms of rPFS | More frequently (enza vs. placebo):
|
| ARCHES [Armstrong et al., 2019] [33] | Enzalutamide + ADT (vs. placebo + ADT) | mHSPC | OS data still immature | NR vs. 19.0 months (p < 0.001) | More frequently (enza vs. placebo):
|
| ENZAMET [Davis et al., 2019] [34] | Enzalutamide + ADT (vs. 1st generation NSAA + ADT) | mHSPC | 80% vs. 72% at 3 years according to Kaplan–Meier estimates (p = 0.002) | 68% vs. 41% at 3 years according to Kaplan–Meier estimates (p < 0.001) in terms of cPFS | More frequently (enza vs. 1st generation NSAA):
|
| PROFOUND [De Bono et al., 2020] [35] | Olaparib (vs. abiraterone acetate + prednisone or enzalutamide) | mCRPC (Cohort A: at least one alteration in BRCA1/2, or ATM; cohort B: alterations in any of 12 other prespecified genes) |
|
| More frequently (Ola vs. placebo):
|
| Drug | Target | Cured Disease | Strategy | Phase | NCT Number | Estimated Completion Date |
|---|---|---|---|---|---|---|
| AMG 509 | STEAP1 | Prostate cancer refractory to a novel antiandrogen therapy and not more than 2 taxane regimens | Single agent | 1 | NCT04221542 | October 2025 |
| Sacituzumab govitecan (IMMU-132) | TROP2 | mCRPC progressing on ARSI | Single agent | 2 | NCT03725761 | October 2021 |
| ARX517 | PSMA | mCRPC | Single agent | 1 | NCT04662580 | August 2024 |
| FOR46 | CD46 | mCRPC | Single agent | 1 | NCT03575819 | December 2021 |
| MGC018 | B7-H3 | Advanced solid tumors including prostate cancer | Single agent or with anti-PD-1 antibody MGA012 | 1/2 | NCT03729596 | May 2025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosellini, M.; Santoni, M.; Mollica, V.; Rizzo, A.; Cimadamore, A.; Scarpelli, M.; Storti, N.; Battelli, N.; Montironi, R.; Massari, F. Treating Prostate Cancer by Antibody–Drug Conjugates. Int. J. Mol. Sci. 2021, 22, 1551. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22041551
Rosellini M, Santoni M, Mollica V, Rizzo A, Cimadamore A, Scarpelli M, Storti N, Battelli N, Montironi R, Massari F. Treating Prostate Cancer by Antibody–Drug Conjugates. International Journal of Molecular Sciences. 2021; 22(4):1551. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22041551
Chicago/Turabian StyleRosellini, Matteo, Matteo Santoni, Veronica Mollica, Alessandro Rizzo, Alessia Cimadamore, Marina Scarpelli, Nadia Storti, Nicola Battelli, Rodolfo Montironi, and Francesco Massari. 2021. "Treating Prostate Cancer by Antibody–Drug Conjugates" International Journal of Molecular Sciences 22, no. 4: 1551. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22041551