
CRISPR/Cas12-Based Ultra-Sensitive and Specific Point-of-Care Detection of HBV


 , and
, and
Abstract
:1. Introduction
2. Results
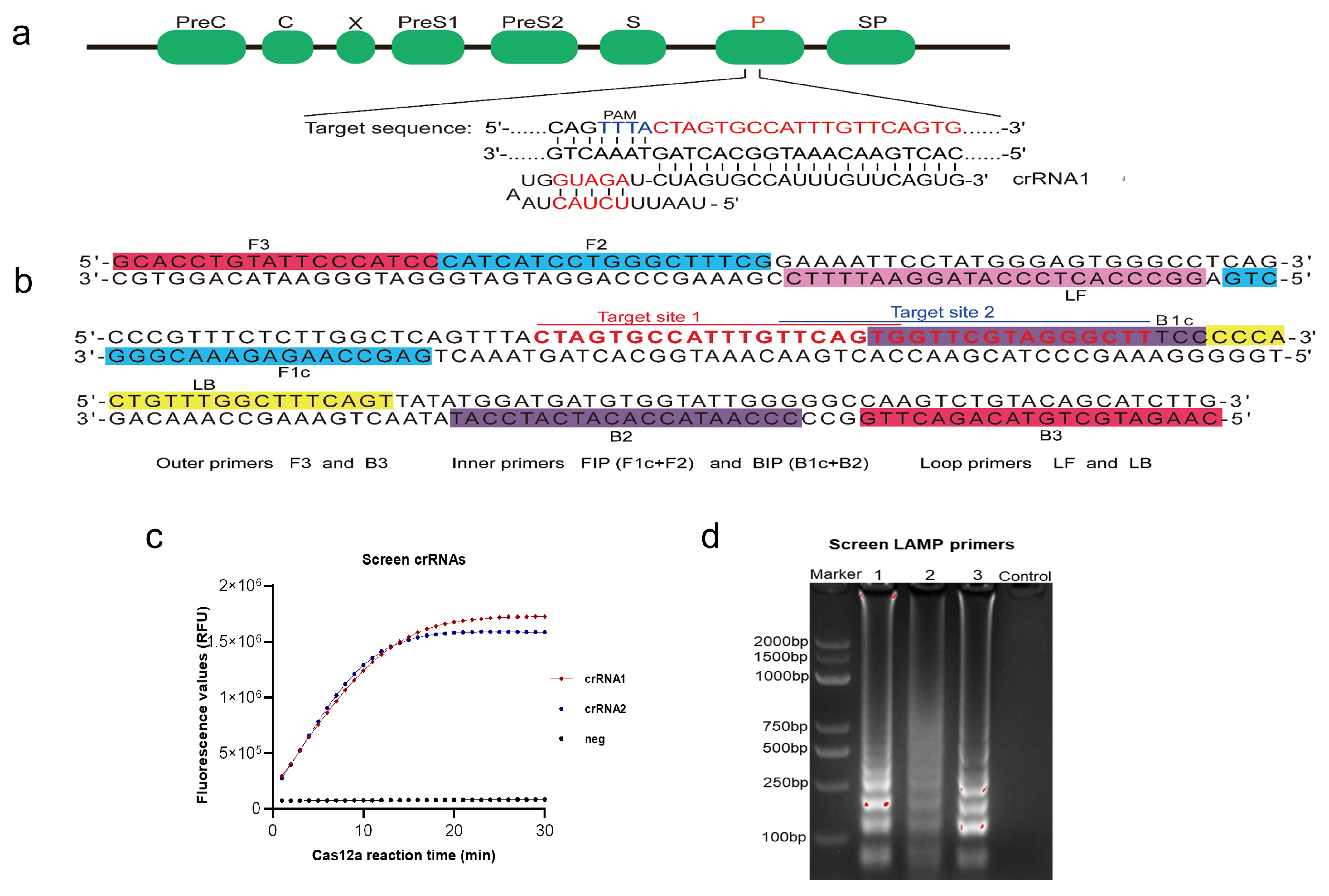
2.1. Construction of Cas12a-DETECTR System for HBV Detection
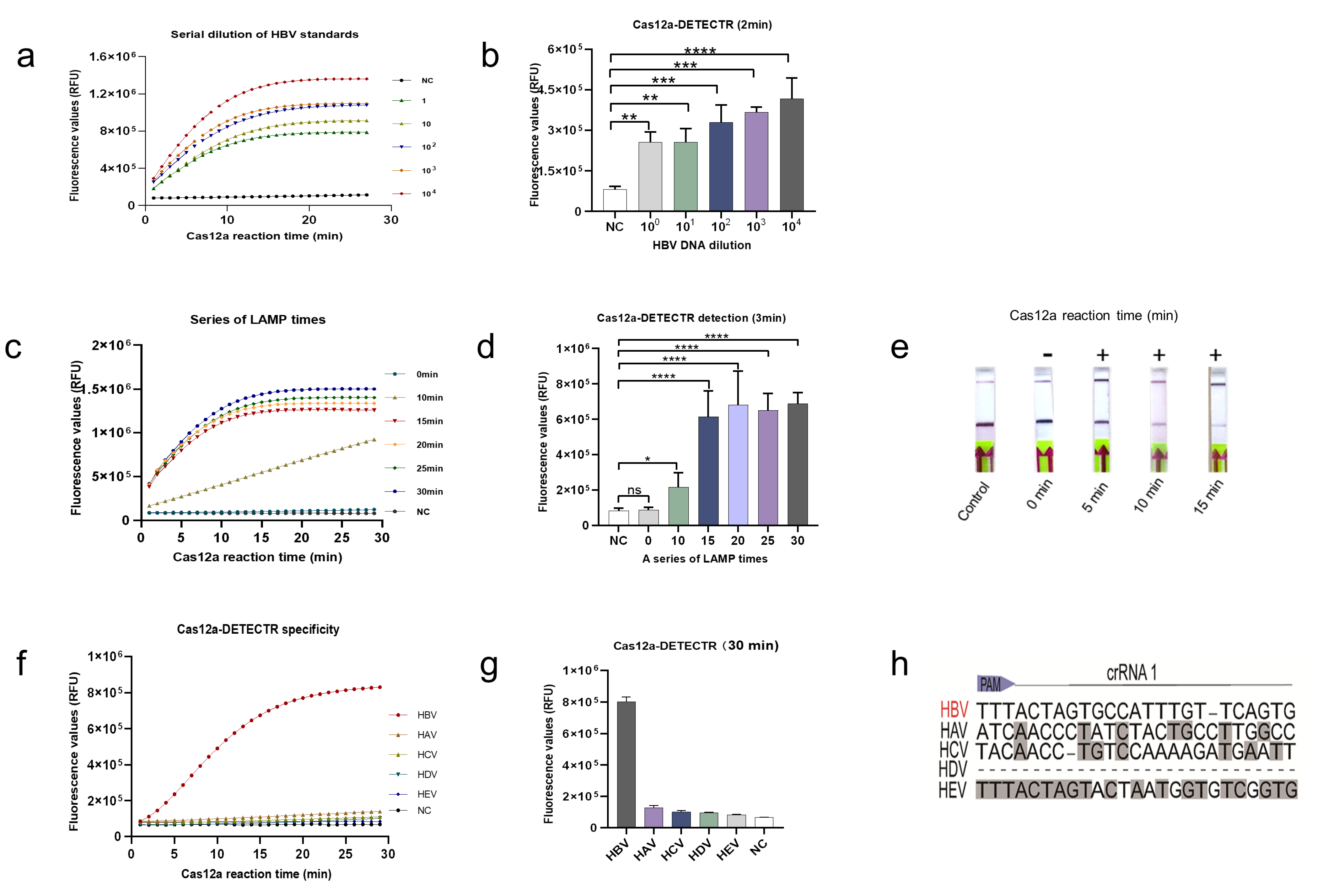
2.2. Analysis of the LoD and Specificity of the Cas12a-DETECTR System
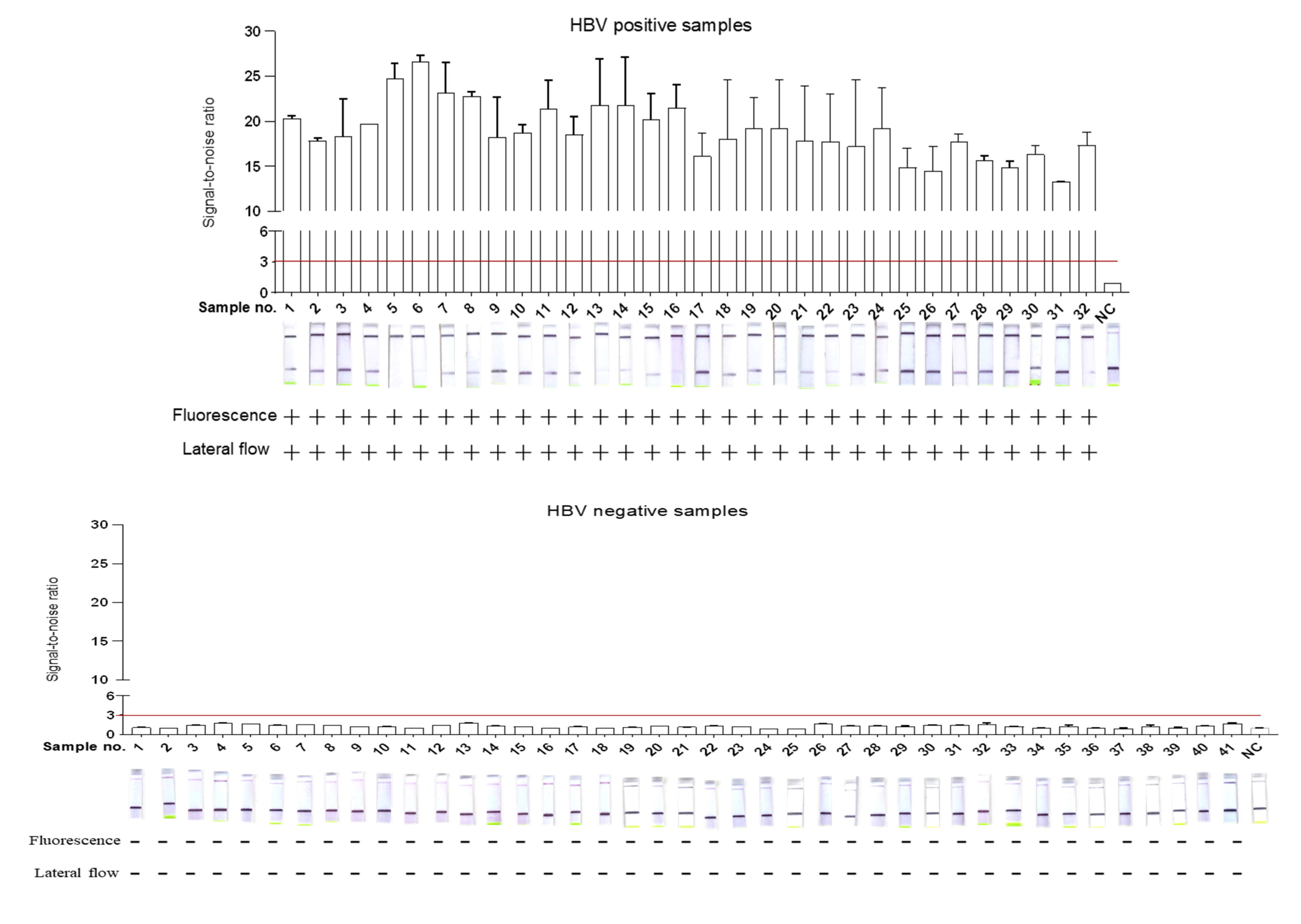
2.3. Validation of DETECTR-Based HBV Assay for Clinical Samples
3. Discussion
4. Materials and Methods
4.1. Nucleic Acid Preparations
4.2. Loop-Mediated Isothermal Amplification (LAMP)
4.3. HBV DNA Detection Based on Cas12a-DETECTR
4.4. Clinical Sample Collection and DNA Extraction
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Liaw, Y.-F. Antiviral therapy of chronic hepatitis B: Opportunities and challenges in Asia. J. Hepatol. 2009, 51, 403–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzãlez, R.; Torres, P.; Castro, E.; Barbolla, L.; Candotti, D.; Koppelman, M.; Zaaijer, H.L.; Lelie, N.; Allain, J.-P.; Echevarrãa, J.-M. Efficacy of hepatitis B virus (HBV) DNA screening and characterization of acute and occult HBV infections among blood donors from Madrid, Spain. Transfusion 2009, 50, 221–230. [Google Scholar] [CrossRef]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prev-alence of chronic hepatitis B virus 279 infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Tan, M.; Bhadoria, A.S.; Cui, F.; Tan, A.; Van Holten, J.; Easterbrook, P.; Ford, N.; Han, Q.; Lu, Y.; Bulterys, M.; et al. Estimating the proportion of people with chronic hepatitis B virus infection eligible for hepatitis B antiviral treatment worldwide: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 106–119. [Google Scholar] [CrossRef]
- Hellard, M.E.; Chou, R.; Easterbrook, P. WHO guidelines on testing for hepatitis B and C-meeting targets for testing. BMC Infect. Dis. 2017, 17, 703. [Google Scholar] [CrossRef] [Green Version]
- Clements, C.J.; Baoping, Y.; Crouch, A.; Hipgrave, D.; Mansoor, O.; Nelson, C.B.; Treleaven, S.; van Konkelenberg, R.; Wiersma, S. Progress in the control of hepatitis B infection in the Western Pacific Region. Vaccine 2006, 24, 1975–1982. [Google Scholar] [CrossRef]
- Rybicka, M.; Bielawski, K.P. Recent Advances in Understanding, Diagnosing, and Treating Hepatitis B Virus Infection. Microorganisms 2020, 8, 1416. [Google Scholar] [CrossRef]
- Datta, S.; Chatterjee, S.; Veer, V. Recent advances in molecular diagnostics of hepatitis B virus. World J. Gastroenterol. 2014, 20, 14615–14625. [Google Scholar] [CrossRef]
- Costa, C.I.; Delgado, I.F.; da Costa, J.A.C.; de Carvalho, R.F.; Júnior, S.D.S.M.E.; Vianna, C.O.A.; de Moraes, M.T.B. Establishment and validation of an ELISA for the quantitation of HBsAg in recombinant hepatitis B vaccines. J. Virol. Methods 2011, 172, 32–37. [Google Scholar] [CrossRef]
- Pfefferkorn, M.; Böhm, S.; Schott, T.; Deichsel, D.; Bremer, C.M.; Schröder, K.; Gerlich, W.H.; Glebe, D.; Berg, T.; Van Bömmel, F. Quantification of large and middle proteins of hepatitis B virus surface antigen (HBsAg) as a novel tool for the identification of inactive HBV carriers. Gut 2018, 67, 2045–2053. [Google Scholar] [CrossRef]
- Liu, W.; Liu, L.; Kou, G.; Zheng, Y.; Ding, Y.; Ni, W.; Wang, Q.; Tan, L.; Wu, W.; Tang, S.; et al. Evaluation of Nucleocapsid and Spike Protein-Based Enzyme-Linked Immunosorbent Assays for Detecting Antibodies against SARS-CoV-2. J. Clin. Microbiol. 2020, 58, 00461-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knott, G.J.; Doudna, J.A. CRISPR-Cas guides the future of genetic engineering. Science 2018, 361, 866–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myhrvold, C.; Freije, C.A.; Gootenberg, J.S.; Abudayyeh, O.O.; Metsky, H.C.; Durbin, A.F.; Kellner, M.J.; Tan, A.L.; Paul, L.M.; Parham, L.A.; et al. Field-deployable viral diagnostics using CRISPR-Cas13. Science 2018, 360, 444–448. [Google Scholar] [CrossRef] [Green Version]
- Patchsung, M.; Jantarug, K.; Pattama, A.; Aphicho, K.; Suraritdechachai, S.; Meesawat, P.; Sappakhaw, K.; Leelahakorn, N.; Ruenkam, T.; Wongsatit, T.; et al. Clinical validation of a Cas13-based assay for the detection of SARS-CoV-2 RNA. Nat. Biomed. Eng. 2020, 4, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Gootenberg, J.S.; Abudayyeh, O.O.; Lee, J.W.; Essletzbichler, P.; Dy, A.J.; Joung, J.; Verdine, V.; Donghia, N.; Daringer, N.M.; Freije, C.A.; et al. Nucleic acid detection with CRISPR-Cas13a/C2c2. Science 2017, 356, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.S.; Ma, E.; Harrington, L.B.; Da Costa, M.; Tian, X.; Palefsky, J.M.; Doudna, J.A. CRISPR-Cas12a target binding unleashes indiscriminate single-stranded DNase activity. Science 2018, 360, 436–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrington, L.B.; Burstein, D.; Chen, J.S.; Paez-Espino, D.; Ma, E.; Witte, I.P.; Cofsky, J.C.; Kyrpides, N.C.; Banfield, J.F.; Doudna, J.A. Programmed DNA destruction by miniature CRISPR-Cas14 enzymes. Science 2018, 362, 839–842. [Google Scholar] [CrossRef] [Green Version]
- Teng, F.; Guo, L.; Cui, T.; Wang, X.-G.; Xu, K.; Gao, Q.; Zhou, Q.; Li, W. CDetection: CRISPR-Cas12b-based DNA detection with sub-attomolar sensitivity and single-base specificity. Genome Biol. 2019, 20, 132. [Google Scholar] [CrossRef]
- Joung, J.; Ladha, A.; Saito, M.; Kim, N.-G.; Woolley, A.E.; Segel, M.; Barretto, R.P.; Ranu, A.; Macrae, R.K.; Faure, G.; et al. Detection of SARS-CoV-2 with SHERLOCK One-Pot Testing. N. Engl. J. Med. 2020, 383, 1492–1494. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.; Yano, Y. Short- and long-term outcome of interferon therapy for chronic hepatitis B infection. World J. Gastroenterol. 2014, 20, 13284–13292. [Google Scholar] [CrossRef]
- Yeo, Y.H.; Nguyen, M.H. Review article: Current gaps and opportunities in HBV prevention, testing and linkage to care in the United States-a call for action. Aliment Pharmacol. Ther. 2020, 53, 63–78. [Google Scholar]
- Sciuto, E.L.; Petralia, S.; Calabrese, G.; Conoci, S. An integrated biosensor platform for extraction and detection of nucleic acids. Biotechnol. Bioeng. 2020, 117, 1554–1561. [Google Scholar] [CrossRef]
- Akram, A.; Islam, S.M.R.; Munshi, S.U.; Tabassum, S. Detection of Hepatitis B Virus DNA among Chronic and potential Occult HBV patients in resource-limited settings by Loop-Mediated Isothermal Amplification assay. J. Viral Hepat. 2018, 25, 1306–1311. [Google Scholar] [CrossRef]
- Wang, S.; Li, H.; Kou, Z.; Ren, F.; Jin, Y.; Yang, L.; Dong, X.; Yang, M.; Zhao, J.; Dong, N.; et al. Highly sensitive and specific detection of hepatitis B virus DNA and drug resistance mutations utilizing the PCR-based CRISPR-Cas13a system. Clin. Microbiol. Infect. 2021, 27, 443–450. [Google Scholar] [CrossRef]
- Wang, R.; Qian, C.; Pang, Y.; Li, M.; Yang, Y.; Ma, H.; Zhao, M.; Qian, F.; Yu, H.; Liu, Z.; et al. opvCRISPR: One-pot visual RT-LAMP-CRISPR platform for SARS-cov-2 detection. Biosens. Bioelectron. 2021, 172, 112766. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.S.; Pan, J.; Li, F.; Zhu, M.; Xu, M.; Zhu, H.; Yu, Y.; Su, G. Reverse Transcription Recombinase Polymerase Amplification 336 Coupled with CRISPR-Cas12a for Facile and Highly Sensitive Colorimetric SARS-CoV-2 Detection. Anal. Chem. 2021, 337. [Google Scholar] [CrossRef]
- Choi, J.-H.; Lim, J.; Shin, M.; Paek, S.-H.; Choi, J.-W. CRISPR-Cas12a-Based Nucleic Acid Amplification-Free DNA Biosensor via Au Nanoparticle-Assisted Metal-Enhanced Fluorescence and Colorimetric Analysis. Nano Lett. 2021, 21, 693–699. [Google Scholar] [CrossRef]
- Larkin, M.A.; Blackshields, G.; Brown, N.P.; Chenna, R.; Mcgettigan, P.A.; McWilliam, H.; Valentin, F.; Wallace, I.M.; Wilm, A.; Lopez, R.; et al. Clustal W and Clustal X version 2.0. Bioinformatics 2007, 23, 2947–2948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamano, T.; Zetsche, B.; Ishitani, R.; Zhang, F.; Nishimasu, H.; Nureki, O. Structural Basis for the Canonical and Non-canonical PAM Recognition by CRISPR-Cpf1. Mol. Cell 2017, 67, 633–645.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.-Y.; Cheng, Q.-X.; Wang, J.-M.; Li, X.-Y.; Zhang, Z.-L.; Gao, S.; Cao, R.-B.; Zhao, G.-P.; Wang, J. CRISPR-Cas12a-assisted nucleic acid detection. Cell Discov. 2018, 4. [Google Scholar] [CrossRef] [Green Version]
- Kellner, M.J.; Koob, J.G.; Gootenberg, J.S.; Abudayyeh, O.O.; Zhang, F. SHERLOCK: Nucleic acid detection with CRISPR nucleases. Nat. Protoc. 2019, 14, 2986–3012. [Google Scholar] [CrossRef] [PubMed]
- Broughton, J.P.; Deng, X.; Yu, G.; Fasching, C.L.; Servellita, V.; Singh, J.; Miao, X.; Streithorst, J.A.; Granados, A.; Sotomayor Gonzalez, A.; et al. CRISPR-Cas12-based detection of SARS-CoV-2. Nat. Biotechnol. 2020, 38, 870–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| qPCR | Sensitivity | Specificity | PPA | NPA | YI | |||
|---|---|---|---|---|---|---|---|---|
| Positive | Negative | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | ||
| Cas12a-DETECTR fluorescence readout | Positive | 32 | 0 | 100% | 100% | 100% | 100% | 100% |
| Negative | 0 | 41 | (86.7–100%) | (89.3–100%) | (86.7–100%) | (89.3–100%) | (76–100%) | |
| Total | 32 | 41 | ||||||
| Cas12a-DETECTR lateral-flow readout | Positive | 32 | 0 | 100% | 100% | 100% | 100% | 100% |
| Negative | 0 | 41 | (86.7–100%) | (89.3–100%) | (86.7–100%) | (89.3–100%) | (76–100%) | |
| Total | 32 | 41 | ||||||
| qPCR a | ELISA b | PCR-Cas13a | LAMP-Cas12a | |
|---|---|---|---|---|
| Assay type | Nucleic acid assay | Antigen and antibody assay | Nucleic acid assay | Nucleic acid assay |
| LoD | 30 IU/mL | Poor sensitivity | 1 copy/μL | 1 copy/μL |
| Nucleic acid extraction | Yes | No | Yes | No |
| Equipment requirements | qPCR | Enzyme-labeled instrument | PCR, qPCR | Metal bath |
| Complex operations | Yes | Yes | Yes | No |
| Cross-reactivity | No | Yes | No | No |
| Assay cost | Expensive | Economic | Economic | Economic |
| Sample-to-result time (approximate) | 4 h | 1–2 h | 2–3 h | 60–70 min |
| point-of-care testing | No | No | No | Yes |
| Clinical Application | Quantitative HBV DNA assay | Assisted qualitative assay | Pending clinical validation | Pending clinical validation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, R.; Long, J.; Yuan, M.; Zheng, X.; Shen, Y.; Jin, Y.; Yang, H.; Li, H.; Chen, S.; Duan, G. CRISPR/Cas12-Based Ultra-Sensitive and Specific Point-of-Care Detection of HBV. Int. J. Mol. Sci. 2021, 22, 4842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094842
Ding R, Long J, Yuan M, Zheng X, Shen Y, Jin Y, Yang H, Li H, Chen S, Duan G. CRISPR/Cas12-Based Ultra-Sensitive and Specific Point-of-Care Detection of HBV. International Journal of Molecular Sciences. 2021; 22(9):4842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094842
Chicago/Turabian StyleDing, Ronghua, Jinzhao Long, Mingzhu Yuan, Xue Zheng, Yue Shen, Yuefei Jin, Haiyan Yang, Hao Li, Shuaiyin Chen, and Guangcai Duan. 2021. "CRISPR/Cas12-Based Ultra-Sensitive and Specific Point-of-Care Detection of HBV" International Journal of Molecular Sciences 22, no. 9: 4842. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094842