
Ozone in Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action in Chronic Inflammatory Diseases


Abstract
:1. Introduction
1.1. Ozone as Bioregulator
1.2. Indications and Applications of Systemically Administered Ozone
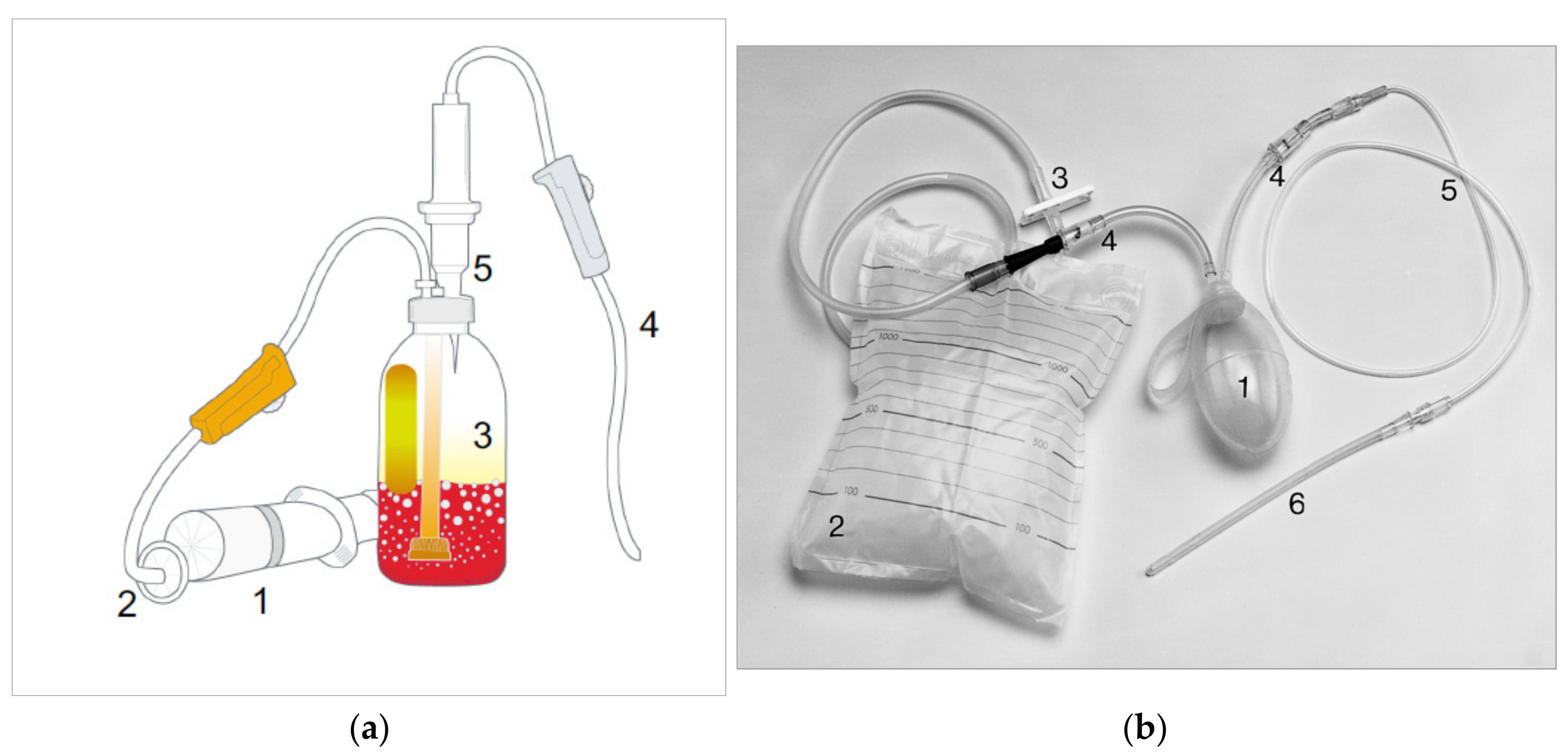
1.3. Procedures
1.4. Ozone Concentration and Dosage in MAH
- µg ozone per mL ozone/oxygen mixture which is delivered by the ozone generator,
- µg ozone per mL blood, or
- the total quantity of ozone in µg per total quantity of blood, or the total quantity of ozone in µg per treatment.
1.5. Dosage
- Systemic: 10–25 µg ozone/mL oxygen gas mixture, volume 150–300 mL; for children: 10–20 µg/mL, volume 10–30 mL; RI is the preferred systemic form of ozone application for children.
- Local: in ulcerous colitis, high O3/O2 concentrations (70–80–100 µg/mL) and small volumes (50 mL) are applied. On cessation of hemorrhage, this is reduced to 20–30 µg/mL, followed by systemic efficacy: 10–20 µg/mL, 150–300 mL volume.
- Rectal ozone application is simple, low-cost, and practically free of adverse reactions when dosages are adhered to exactly.
- As an adjuvant therapy in proctitis and proctocolitis, rectal insufflation is scientifically founded and to be recommended. Rectal O3 insufflation is increasingly being used in pediatrics, sports medicine, geriatrics, and as a complementary method in oncology.
2. Results
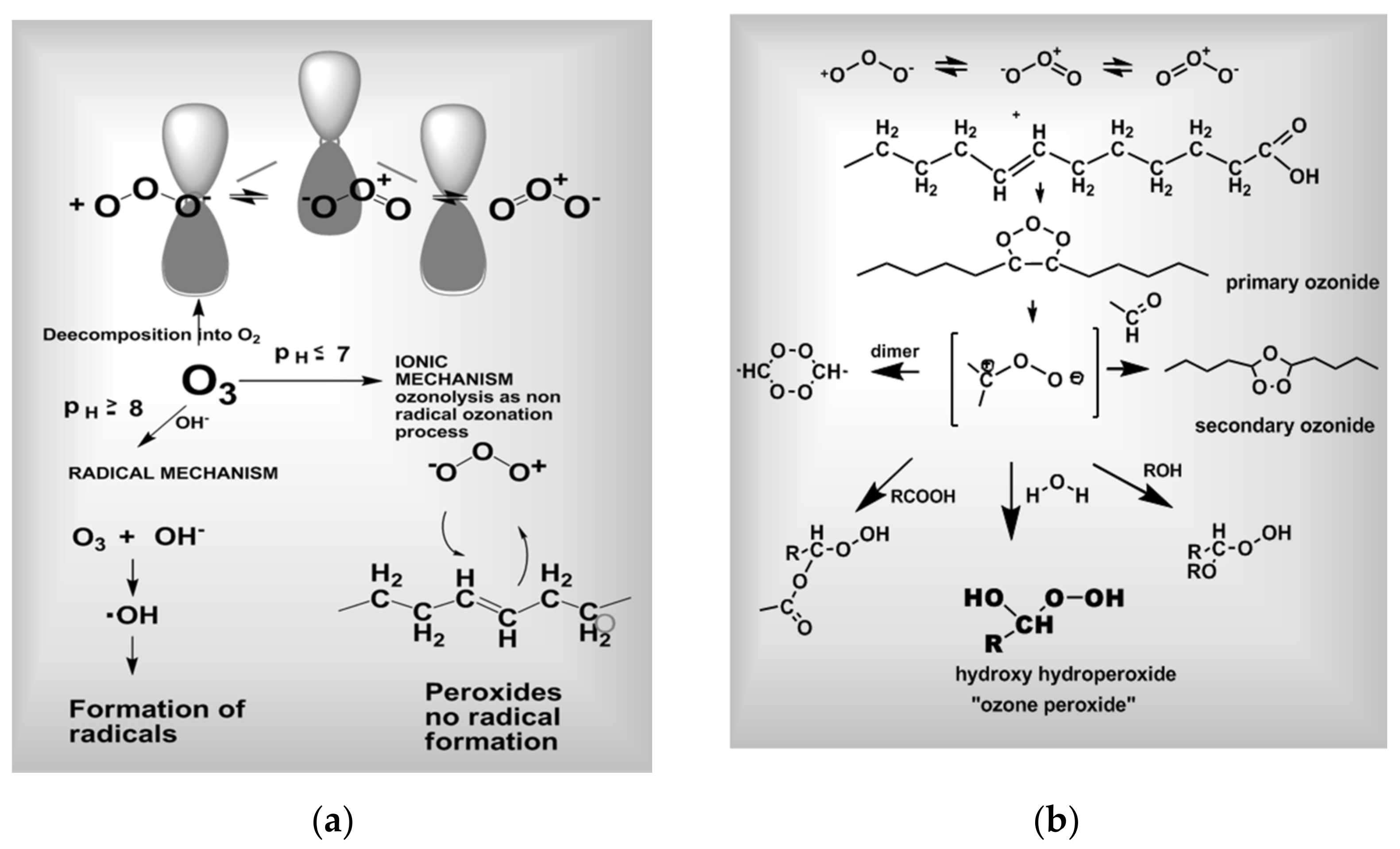
2.1. Mechanisms of Action
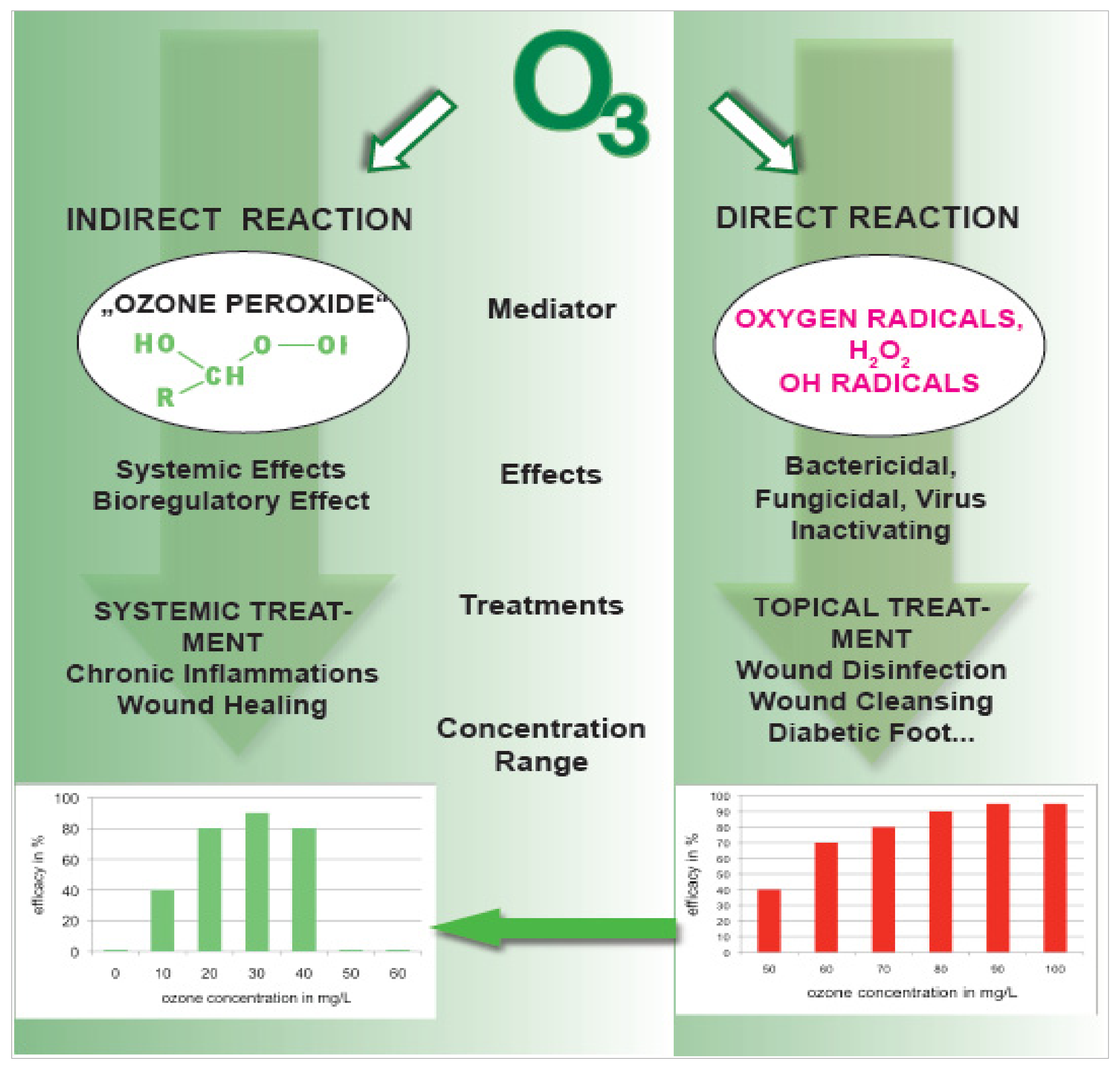
2.1.1. The Reactivity and the Effects of Ozone
2.1.2. Direct Effects: Germicidal and Virus-Inactivating Effects in Topical Ozone Applications
2.1.3. Indirect Effects in Systemic Treatments: Signal Transduction and Bioregulation
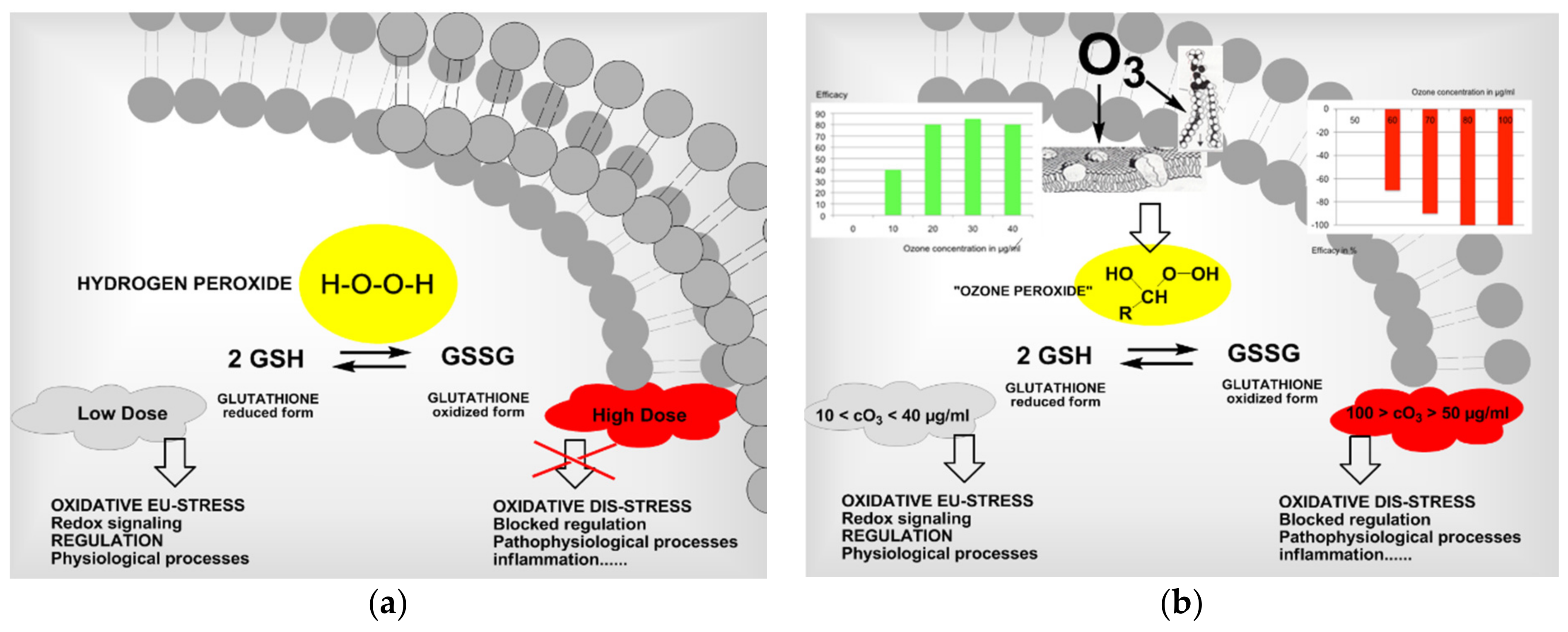
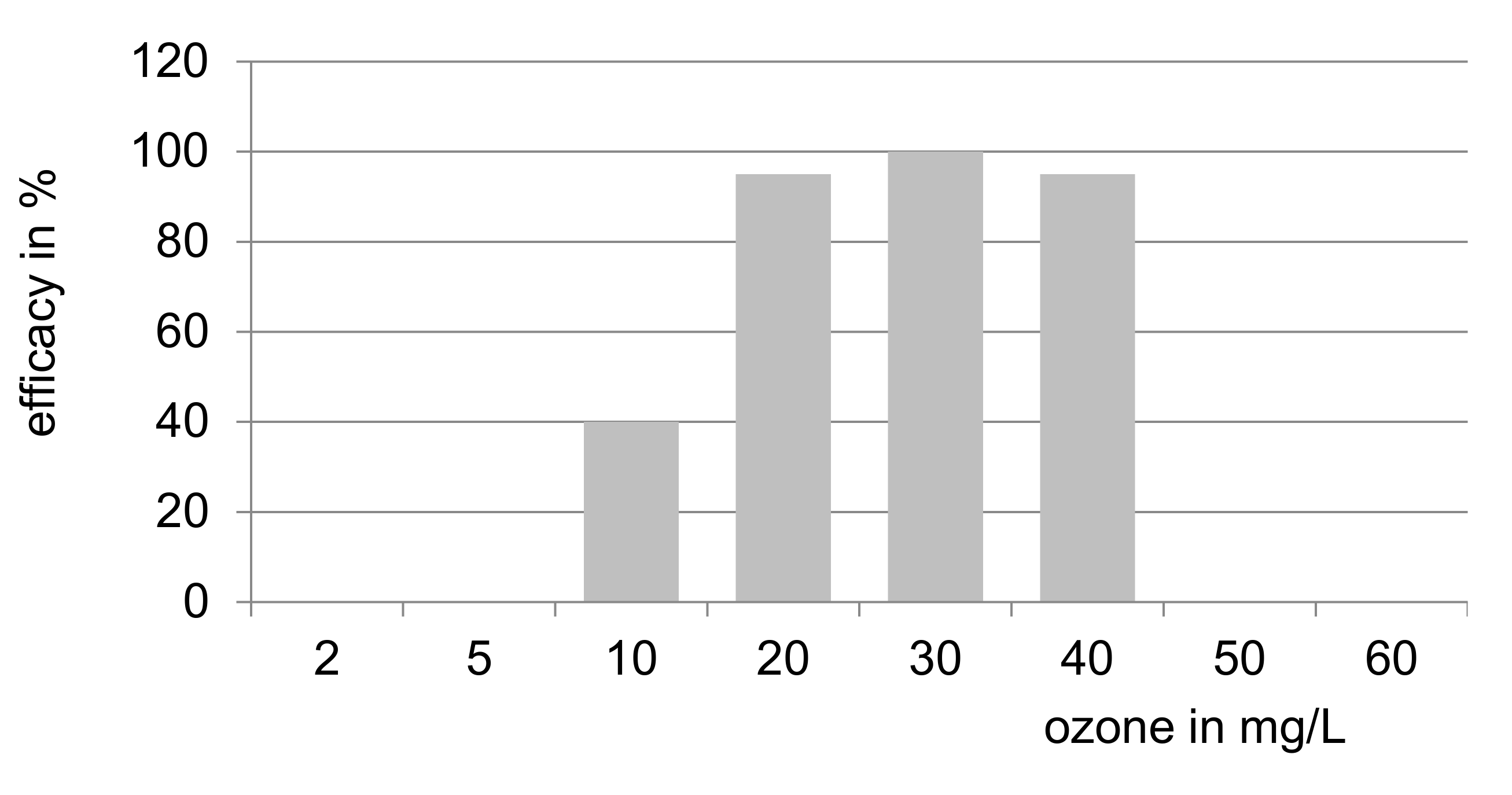
2.1.4. Dose-Response Relationship
3. Discussion
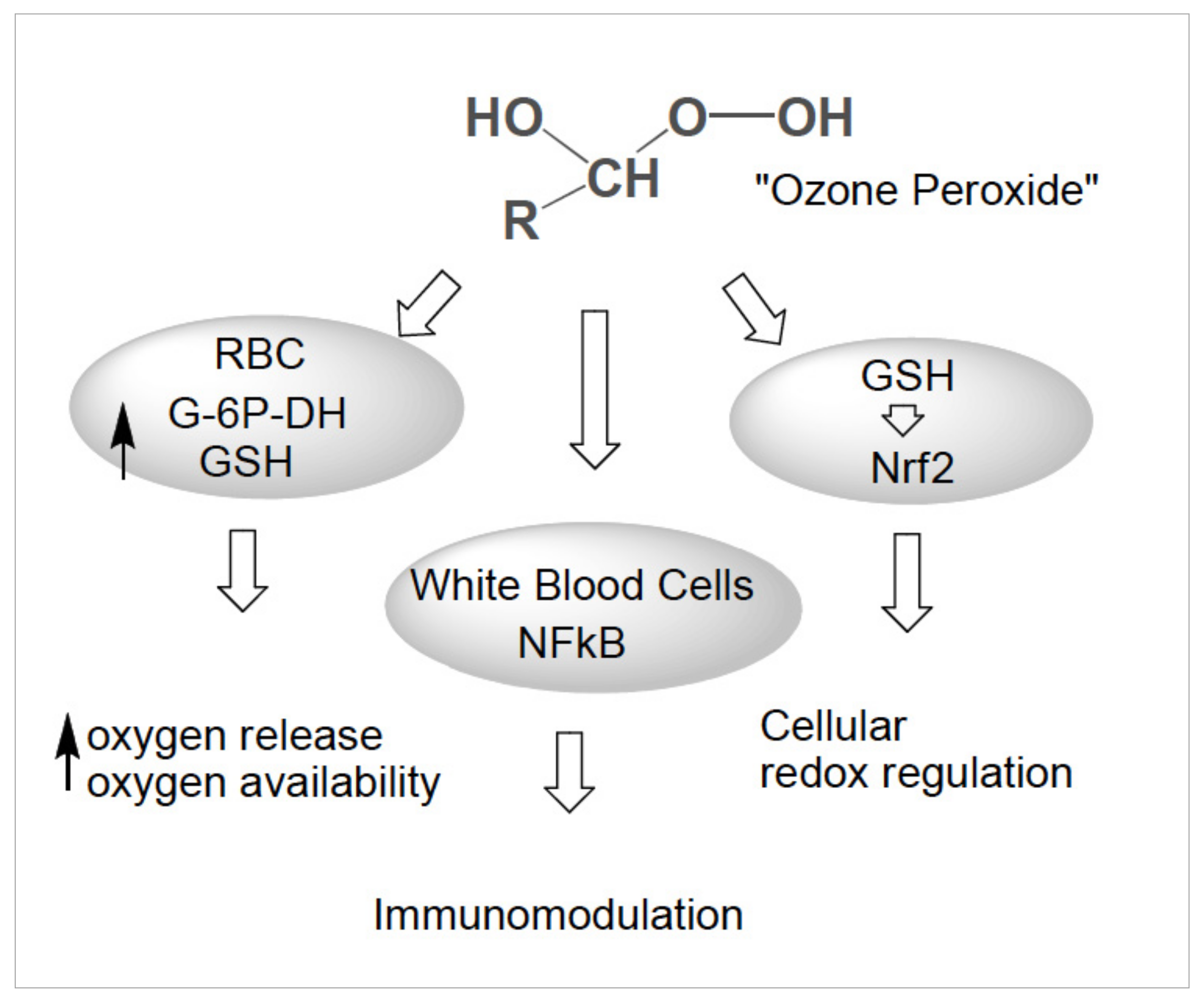
3.1. “Ozone Peroxides” as Signal Molecules
3.1.1. Oxidative Stress
3.1.2. “Ozone Peroxides” as Second Messenger Molecules
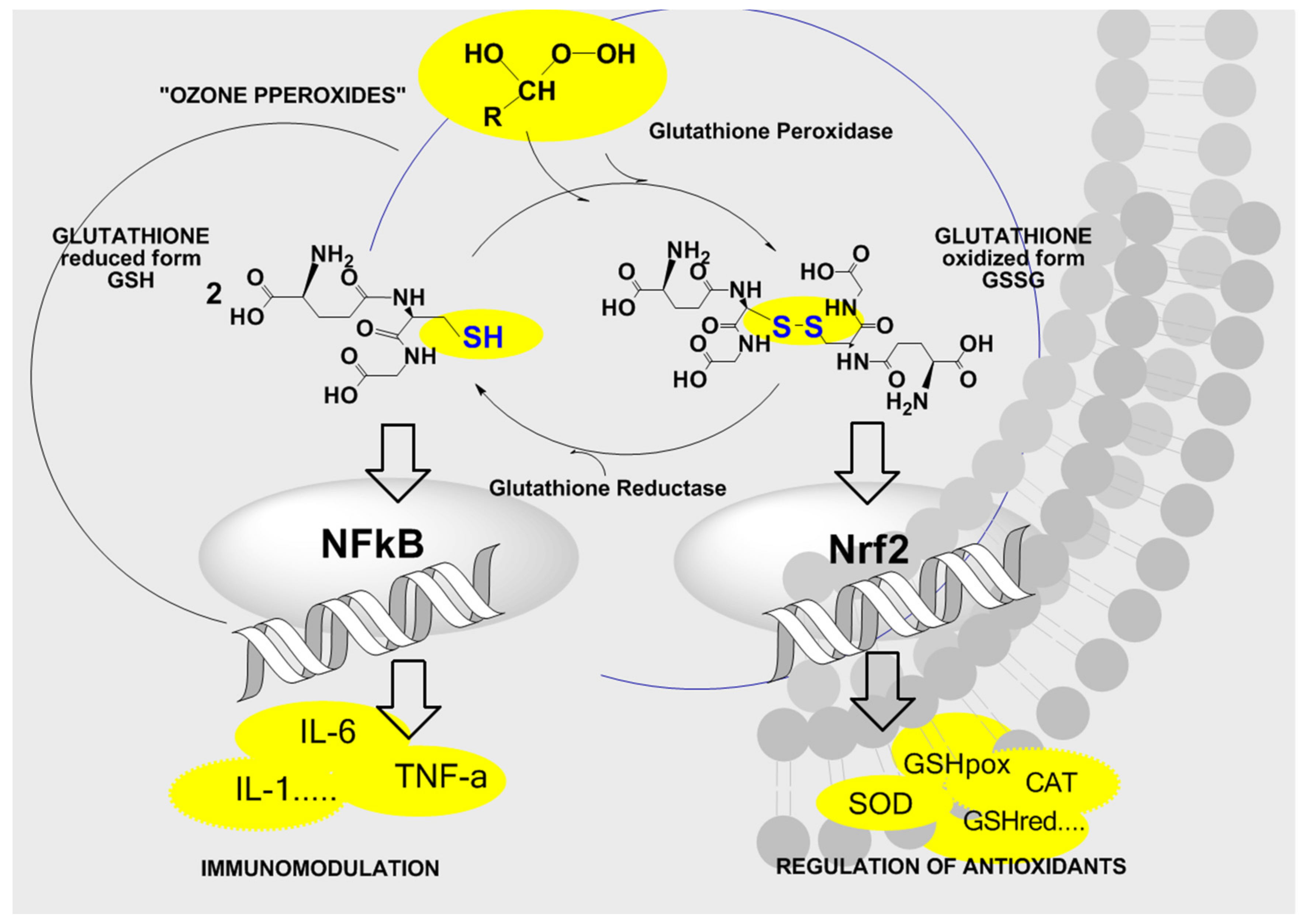
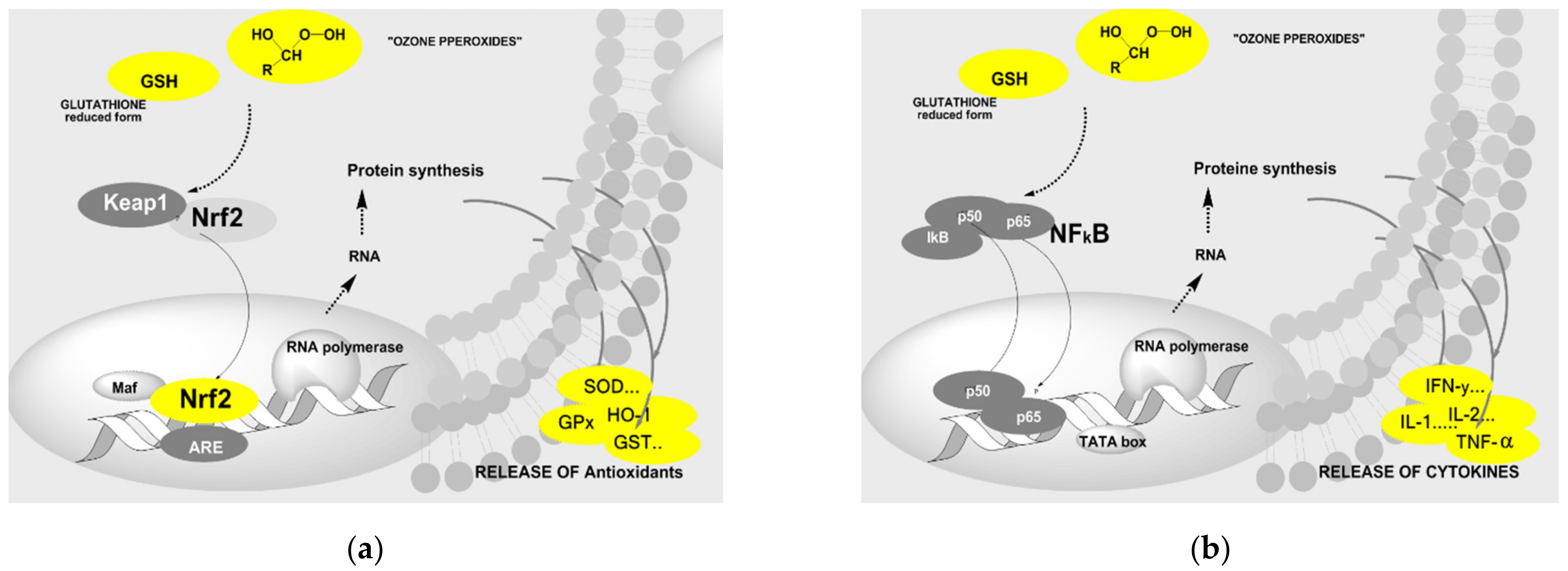
3.1.3. Signal Transduction and Bioregulation. The Role of Glutathione


3.1.4. Ozone Specific Stress Markers
4. Material and Methods
4.1. Rheumatoid Arthritis RA as a Model for Chronic Inflammatory Diseases
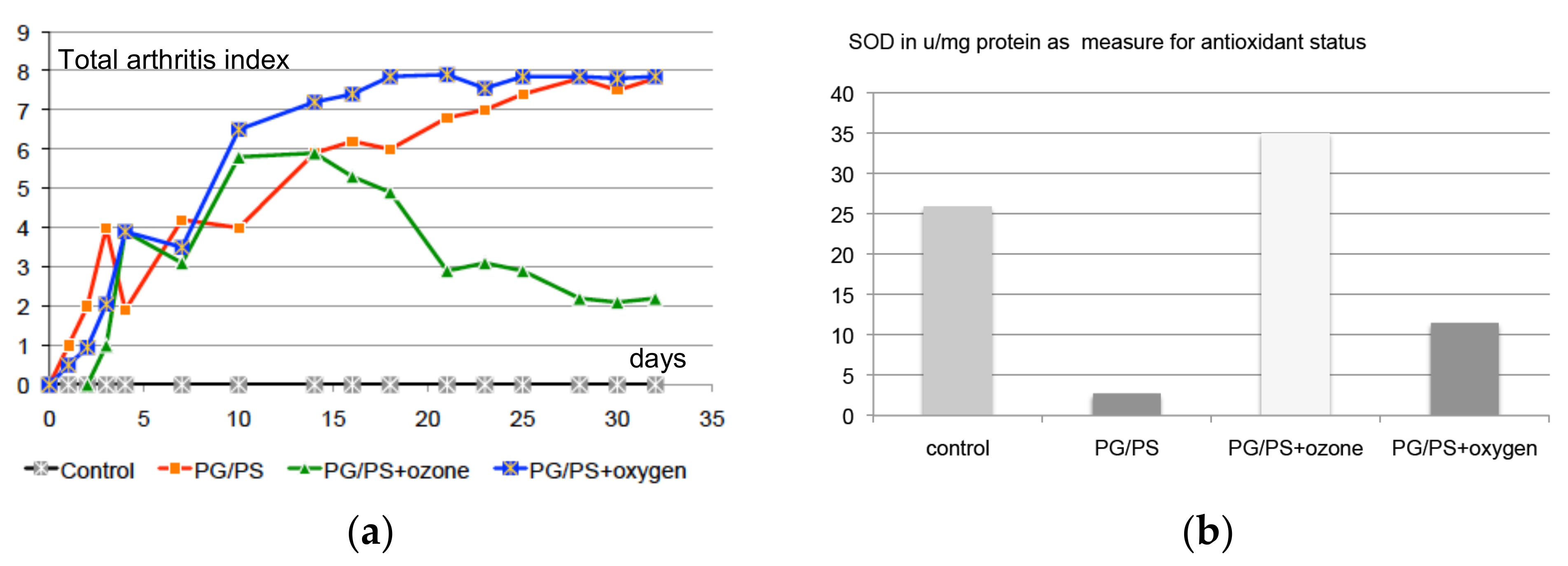
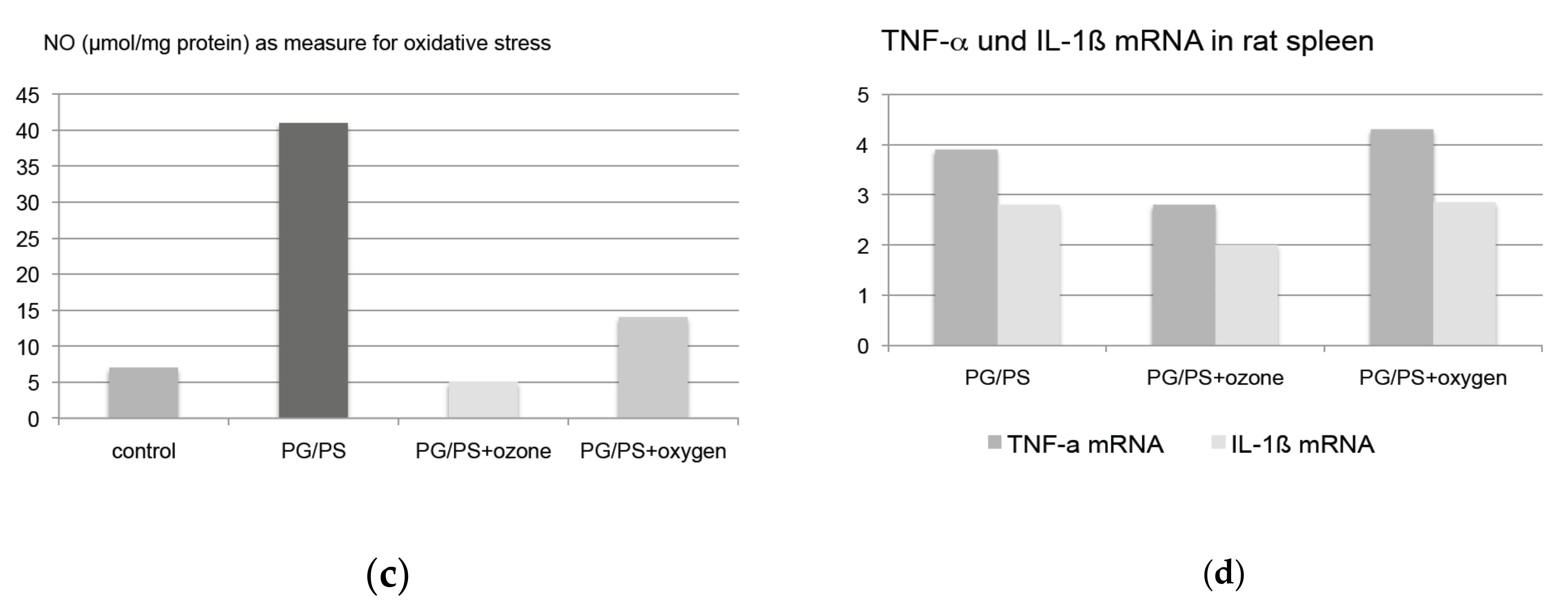
4.2. Preclinical Trials
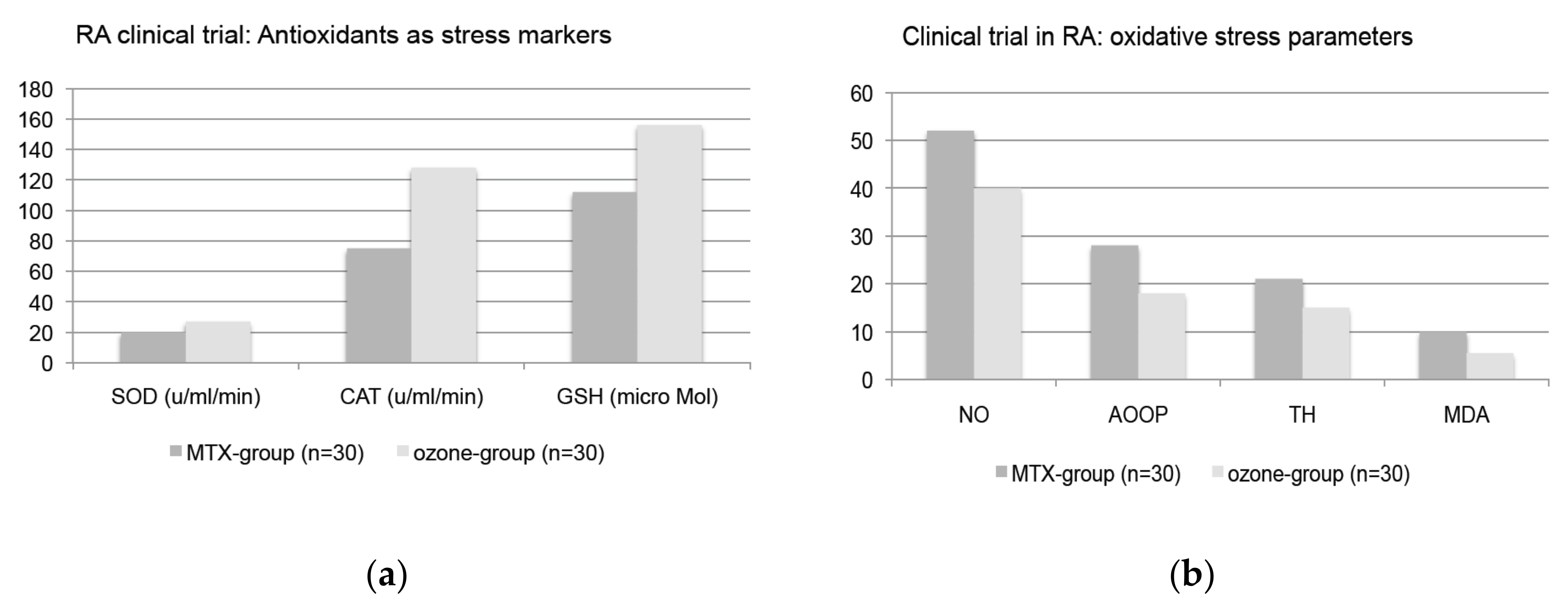
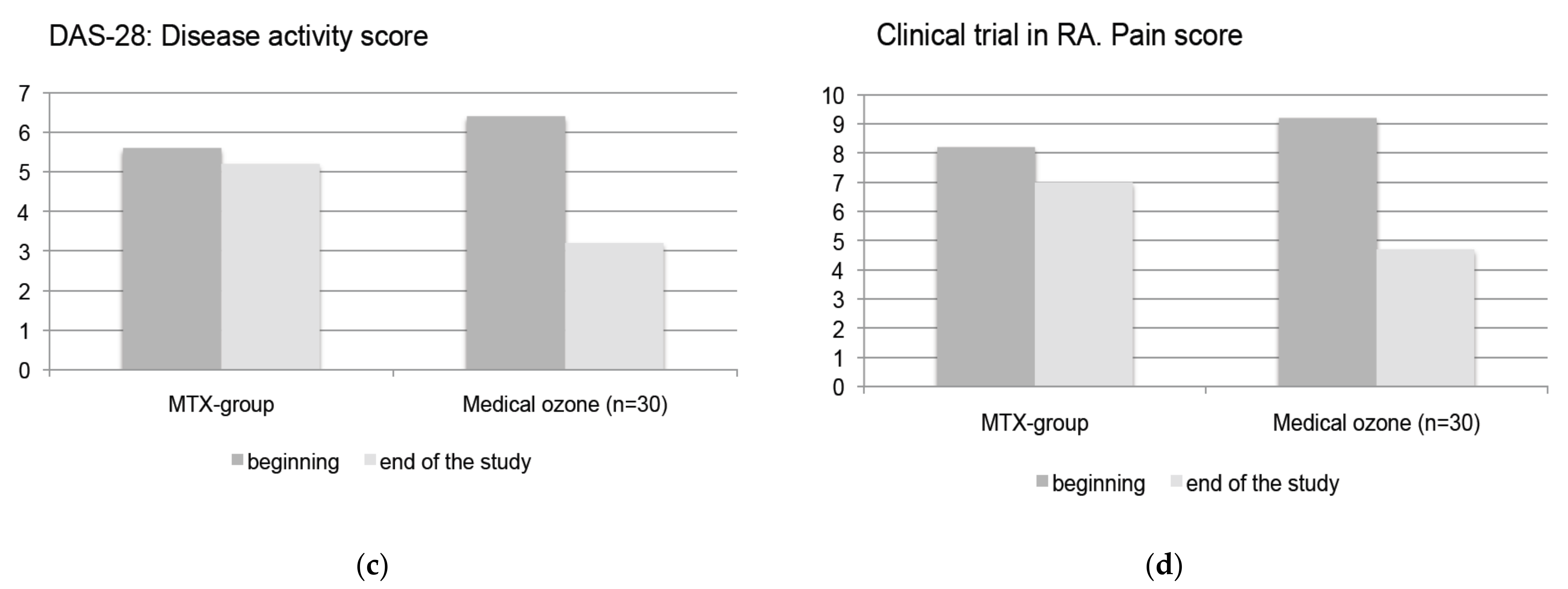
4.3. Clinical Trials
4.4. Treatment Concept
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sies, H. Hydrogen peroxide as a central redox signaling molecule in physiological oxidative stress: Oxidative eustress. Redox Biol. 2017, 11, 613–619. [Google Scholar] [CrossRef]
- Marinho, H.S.; Real, C.; Cyrne, L.; Soares, H.; Antunes, F. Hydrogen peroxide sensing, signaling and regulation of transcription factors. Redox Biol. 2014, 2, 535–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Washüttl, J.; Viebahn, R. Biochemische Aspekte der Ozon-Sauerstoff Theapie. Ars Med. 1986, 5, 194–199. (In German) [Google Scholar]
- Lell, B.; Viebahn, R.; Kremsner, P. The activity of ozone against plasmodium falciparum. Ozone Sci. Eng. 2001, 23, 89–93. [Google Scholar] [CrossRef]
- Hoffmann, A.; Viebahn, R. Über den Einfluss von Ozon auf die 2,3 Diphosphoglyzerat-Synthese in Erythrozyten-Konzentraten. In Ozon-Handbuch, Grundlagen-Prävention-Therapie; Viebahn-Hänsler, R., Knoch, H.G., Eds.; Ecomed Publisher: Landsberg, Germany, 2002. [Google Scholar]
- Bocci, V.; Paulesu, L. Studies on the biological effects of ozone. 1. Induction of interferon in human leucocytes. Haematologica 1990, 75, 510–515. [Google Scholar] [PubMed]
- Bocci, V.; Luzzi, E.; Corradeschi, F.; Paulesu, L.; Rossi, R.; Cardaioli, E.; Di Simplicio, P. Studies on the biological effects of ozone: 4. Cytokine production and glutathione levels in human erythrocytes. Biol. Reg. Hom. Agents 1993, 7, 133–138. [Google Scholar]
- Léon, O.S.; Menendéz, S.; Merino, N.; Castillo, R.; Sam, S.; Pérez, L.; Cruz, E.; Bocci, V. Ozone oxidative preconditioning: A protection against cellular damage by free radicals. Mediat. Inflamm. 1998, 7, 289–294. [Google Scholar] [CrossRef]
- Viebahn-Haensler, R.; León Fernández, O.S.; Fahmy, Z. Ozone in medicine: The low-dose ozone concept. Guidelines and treatment strategies. Ozone Sci. Eng. 2012, 34, 408–424. [Google Scholar] [CrossRef]
- Hoigné, J.; Bader, H. Rate constants of reactions of ozone with organic and inorganic compounds in water I/II. Water Res. 1983, 17, 173–194. [Google Scholar] [CrossRef]
- Criegee, R. Die Ozonolyse. Liebigs Ann. Chem. 1953, 538, 9. [Google Scholar] [CrossRef]
- Criegee, R. Mechanism of Ozone. Angew. Chem. Int. Ed. 1975, 14, 745–752. [Google Scholar] [CrossRef]
- Werkmeister, H. Dekubitalgeschwüre und Die Behandlung Mit der Ozon-Unterdruck-Begasung (German) in Ozon- Handbuch, Grundlagen-Prävention-Therapie; Viebahn-Hänsler, R., Knoch, H.G., Eds.; Ecomed Publisher: Landsberg, Germany, 1995. [Google Scholar]
- Haddad, E.B.; Salmon, M.; Koto, H.; Barnes, P.J.; Adcock, I.; Chung, K.F. Ozone induction of cytokin-induced neutrophil chemotractant and nuclear factor-kB in Rat Lung: Inhibition by Corticosteroids. FEBS Lett. 1996, 379, 265–268. [Google Scholar] [CrossRef] [Green Version]
- Sagai, M.; Bocci, V. Mechanisms of action involved in ozone therapy: Is healing induced via a mild oxidative stress? Med. Gas Res. 2011, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- Bocci, V.; Zanardi, I.; Travagli, V. Oxygen/Ozone as a Medical gas mixture. A Critical evaluation. Med. Gas Res. 2011, 1, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Re, L.; Martinez-Sanchez, G.; Bordicchia, M.; Malcangi, G.; Pocognoli, A.; Morales-Segura, M.A.; Rothchild, J.A.; Rojas, A. Is ozone pre-conditioning effect linked to Nrf2/EpRE activation pathway in vivo? A preliminary result. Eur. J. Pharmacol. 2014, 742, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Roche, L.; Riera-Romo, M.; Mesta, F.; Hernández-Matos, Y.; Barrios, J.M.; Martínez-Sánchez, G.; Al-Dalaien, S.M. Medical ozone promotes Nrf2 phosphorylation reducing oxidative stress and pro-inflammatory cytokines in multiple sclerosis patients. Eur. J. Pharmacol. 2017, 811, 148–154. [Google Scholar] [CrossRef]
- Togi, S.; Togi, M.; Nagashima, S.; Kitay, Y.; Muromoto, R.; Kashiwakura, J.; Miura, T.; Matsuda, T. Implication of NF-kB Activation on Ozone-Induced HO-1 Activation. BPB Rep. 2021, 4, 59–63. [Google Scholar] [CrossRef]
- Kansanen, E.; Kuosmanen, S.M.; Leinonen, H.; Levonen, A.L. The Keap1-Nrf2 pathway: Mechanisms of activation and dysregulation in cancer. Redox Biol. 2013, 1, 45–49. [Google Scholar] [CrossRef] [Green Version]
- Costanzo, M.; Romeo, A.; Cisterna, B.; Calderan, L.; Bernardi, P.; Covi, V.; Tabaracci, G.; Malatesta, M. Ozone at low concentrations does not affect motility and proliferation of cancer cells in vitro. Eur. J. Histochem. 2020, 64, 3119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scassellati, C.; Costanzo, M.; Cisterna, B.; Nodari, A.; Galiè, M.; Cattaneo, A.; Covi, V.; Tabaracci, G.; Bonvicini, C.; Malatesta, M. Effects of mild ozonisation on gene expression and nuclear domains organization in vitro. Toxicol Vitr. 2017, 44, 100–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viebahn-Haensler, R.; León, F.O.S.; Fahmy, Z. Ozone in medicine: Clinical evaluation and evidence classification of the systemic ozone applications, major autohemotherapy and rectal insufflation, according to the requirements for evidence-based medicine. Ozone Sci. Eng. 2016, 38, 322–345. [Google Scholar] [CrossRef]
- Wolff, H. Textbook Das Medizinische Ozon (German); Verlag für Medizin: Heidelberg, Germany, 1979. [Google Scholar]
- Dranguet, V.J.; Fraga, A.; Diaz, M.T.; Mallok, A.; Viebahn-Hänsler, R.; Fahmy, Z.; Barbera, A.; Delgado, L.; Menendez, S.; Leon, F.O.S. Ozone oxidative postconditioning ameliorates joint damage and decreases proinflammatory cytokine levels and oxidative stress in PG/PS-induced arthritis in rats. Eur. J. Pharmacol. 2013, 714, 318–324. [Google Scholar] [CrossRef]
- León, F.O.S.; Viebahn-Haensler, R.; López, C.G.; Serrano, E.I.; Hernández, M.Y.; Delgado, R.L.; Tamargo, S.B.; Takon, O.G.; Polo, V.J.C. Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 2016, 789, 313–318. [Google Scholar] [CrossRef]
- Takon, O.G.; Viebahn-Haensler, R.; López, C.G.; Serrano, E.I.; Tamargo, S.B.; Polo, V.J.C.; Sánchez, S.S.; León, F.O.S. Medical Ozone Reduces the Risk of GGT and Alkaline Phosphatase Abnormalities and Oxidative Stress in Rheumatoid Arthritis Patients treated with Methotrexate. SMJ. Arthritis Res. 2017, 1, 1004. [Google Scholar]
- Takon Oru, G.; Viebahn-Haensler, R.; García Fernández, E.; Alvarez Almiñaque, D.; Polo Vega, J.C.; Tamargo Santos, B.; López Cabreja, G.; Serrano Espinosa, I.; Tabares Nápoles, N.; León Fernández, O.S. Medical Ozone Effects and Innate Immune Memory in Rheumatoid Arthritis Patients Treated with Methotrexate+Ozone After a Second Cycle of Ozone Exposure. Chronic Pain Manag. 2019, 2, 114. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Applications | Indications | Mechanims of Action |
|---|---|---|
| Systemic applications | ||
| 1. Major autohemotherapy MAH as an extracorporeal blood treatment and iv reinfusion of the patients own blood via pressure-free drip infusion 2. Rectal insufflation RI | Arterial circulatory disorders Chronic inflammatory processes - Angiopathia, diabetic in particular - Chronic inflammation in orthopedics and rheumatology - Rheumatoid arthritis RA - Chronic intestinal diseases - Chronic forms of hepatitis B and C - Complementary oncology - Age-related diseases | - Activation of RBC metabolism, increase of 2,3-DPG, of ATP, improvement of oxygen release - Activation of immunocompetent cells with regulation of cytokine production, such as interferons and interleukines. - Downregulation of oxidative stress - Regulation of the anti-oxidative capacity by signal transduction |
| Contraindications |
| |
| MaH Standard Procedure: 50 mL of Blood + 50 mL of O2/O3 (or 100 mL of O2/O3 per 100 mL of Blood) | |||
|---|---|---|---|
| Ozone concentration per mL of gas | 10–20 µg/mL gas | 30 µg/mL gas | maximum 40 µg/mL gas |
| Ozone concentration per mL of blood = biologically relevant concentration | 10–20 µg/mL blood | 30 µg/mL blood | 40 µg/mL blood |
| Total ozone amount per 50 (100) mL blood | 500–1000 µg per treatment | 1500 µg per treatment | 2000 µg per treatment |
| Oxidative Stress | Antioxidant Status | Cytokines |
|---|---|---|
| TH total hydroperoxides MDA malondialdehyde NO nitrogen oxide -GT -glutamyl transferase | total SOD superoxide dismutase | interleukine IL-1, IL-6, |
| GSH reduced glutathione | TNFα tumor necrosis factor-α |
| Major Auto Hemotherapy | Ozone Concentration | Ozone Volume | Ozone Amount | Treatment Frequency | Number of Treatments |
|---|---|---|---|---|---|
| Rheumatoid arthritis | |||||
| acute stage | 30–35 µg/mL | 50 mL (100 mL) | 1500–1750 µg (3000–3500 µg per 100 mL of blood) | daily | as per control |
| non acute stage | 20–25 µg/mL | 50 mL | 1000–1250 µg | 1× per week, then every 2nd week | in compliance with the patient |
| Rectal Insufflation | 25–30 µg/mL | 150–300 mL | 3750–9000 | Daily in the beginning, then 2× or 1× per week | in compliance with the patient |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viebahn-Haensler, R.; León Fernández, O.S. Ozone in Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action in Chronic Inflammatory Diseases. Int. J. Mol. Sci. 2021, 22, 7890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22157890
Viebahn-Haensler R, León Fernández OS. Ozone in Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action in Chronic Inflammatory Diseases. International Journal of Molecular Sciences. 2021; 22(15):7890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22157890
Chicago/Turabian StyleViebahn-Haensler, Renate, and Olga Sonia León Fernández. 2021. "Ozone in Medicine. The Low-Dose Ozone Concept and Its Basic Biochemical Mechanisms of Action in Chronic Inflammatory Diseases" International Journal of Molecular Sciences 22, no. 15: 7890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22157890