
High Risk of Viral Reactivation in Hepatitis B Patients with Systemic Lupus Erythematosus

 , ,
, ,
Abstract
:1. Introduction
2. Results
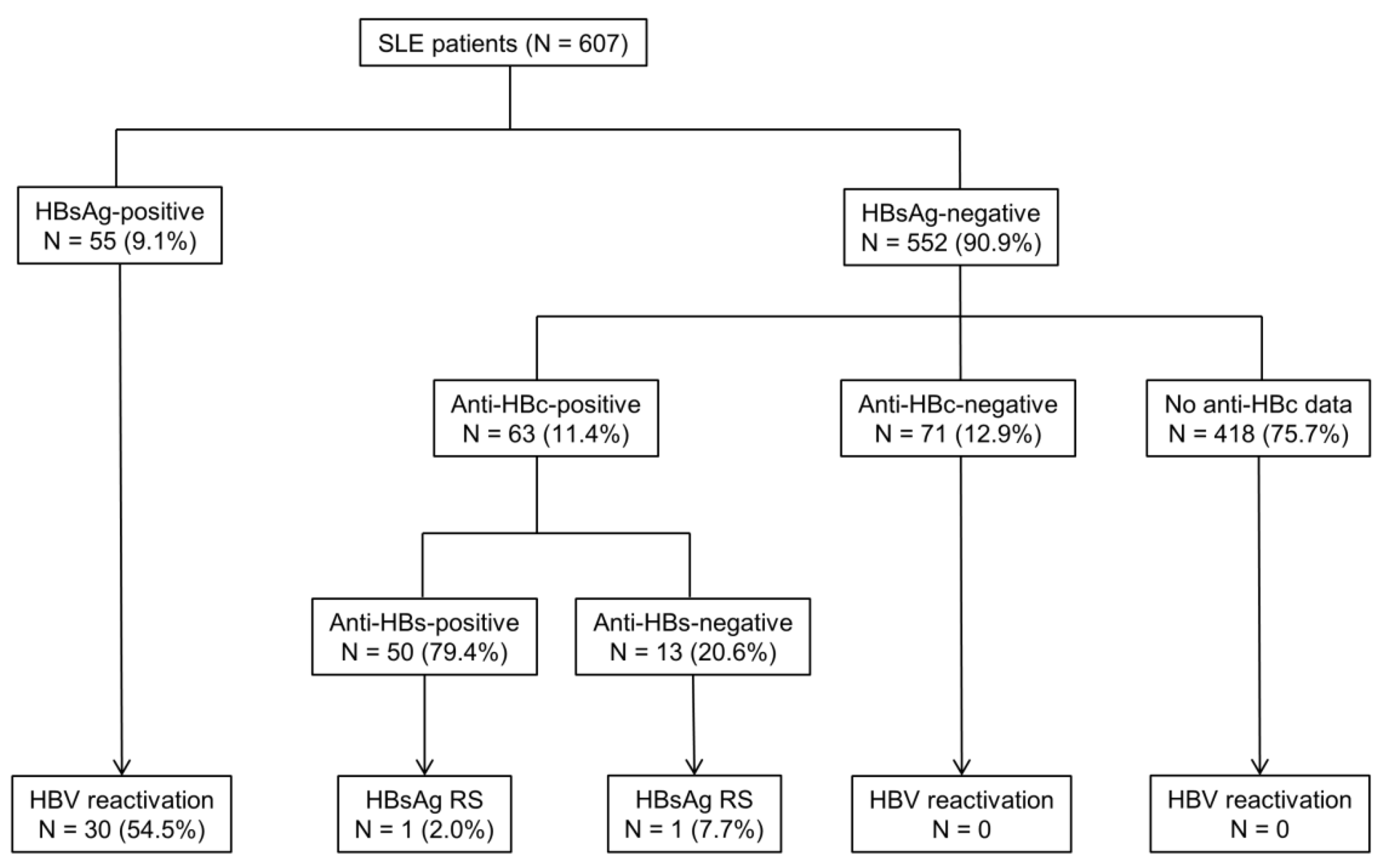
2.1. Hepatitis B Status and Immunologic Profiles of Patients
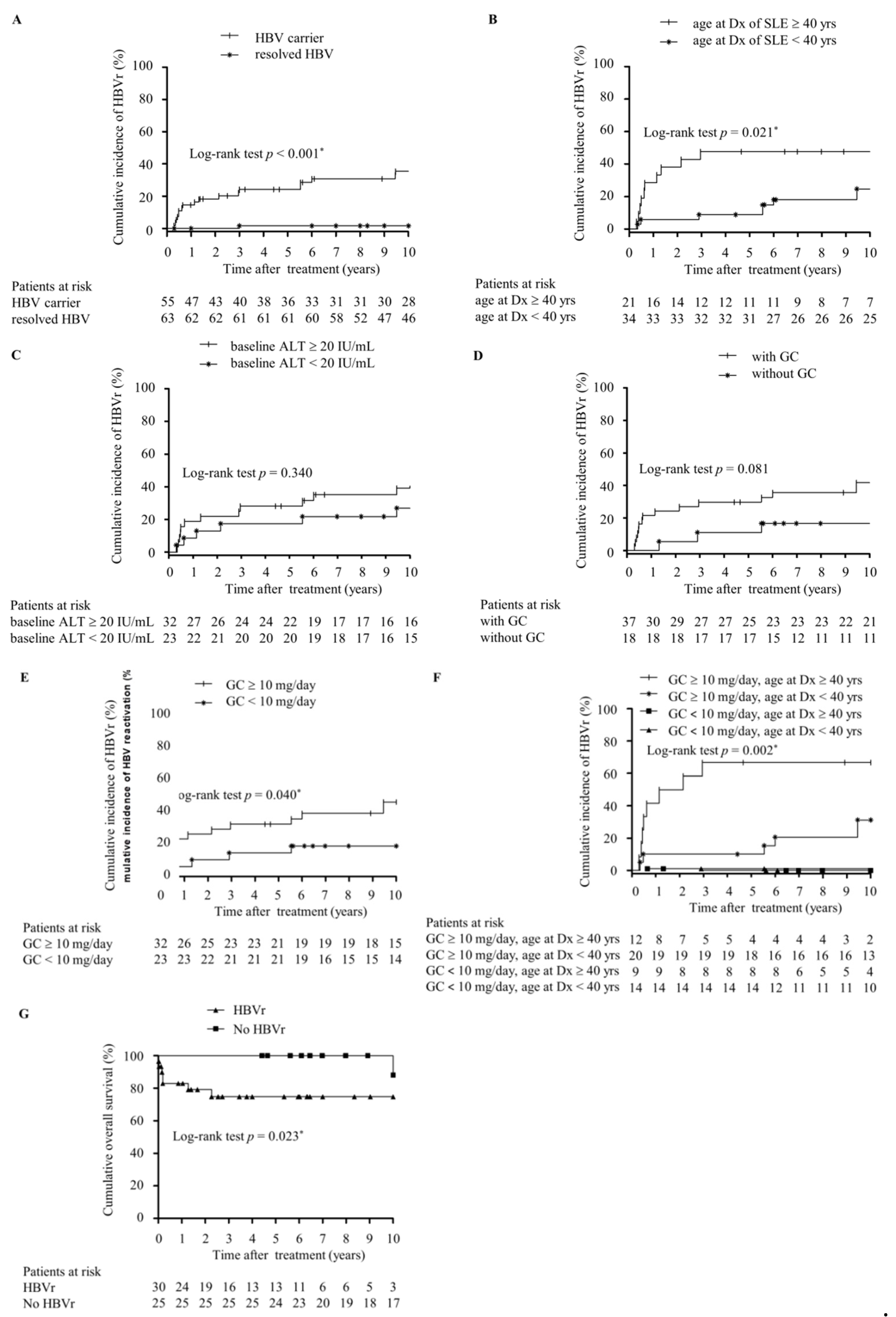
2.2. Incidence of HBVr in SLE Patients
2.3. Clinical Features of HBVr in HBsAg-Positive SLE Patients
2.4. Outcome of HBsAg-Positive SLE Patients with HBVr
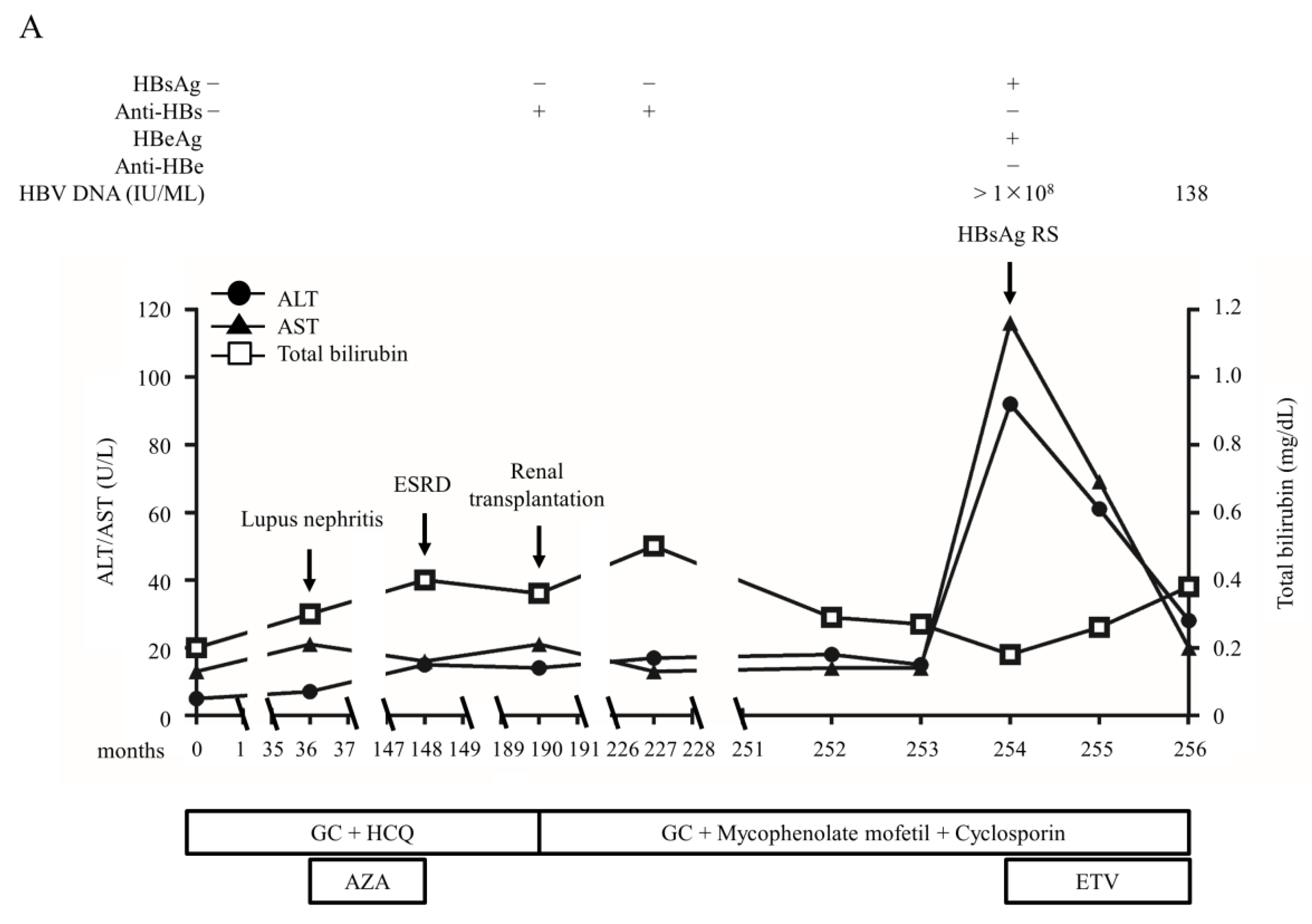
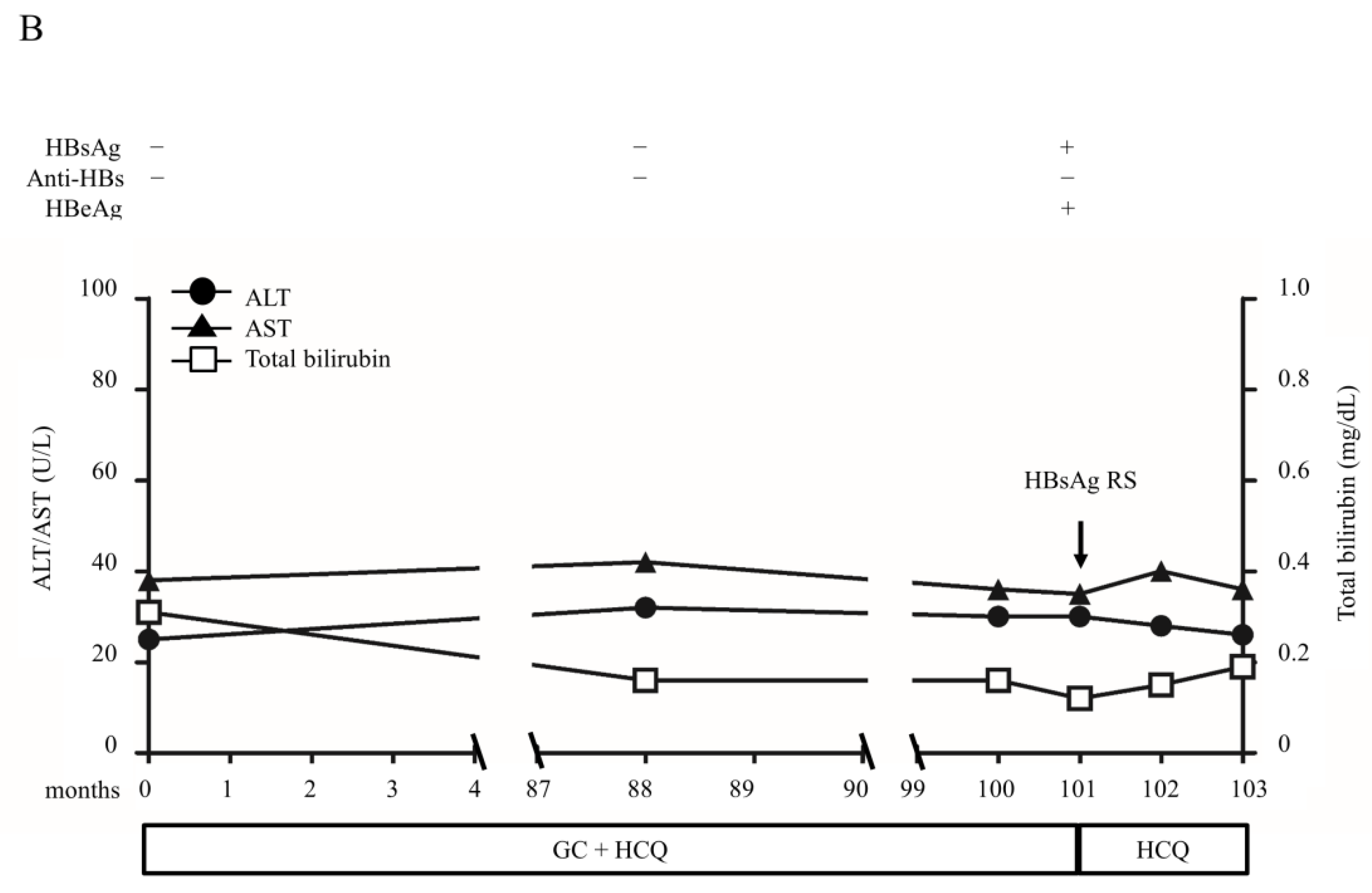
2.5. Clinical Features of HBVr in RHB Patients
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Definition
4.3. Liver Function and Immunologic Tests
4.4. Serological Tests of Viral Hepatitis Markers
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Merican, I.; Guan, R.; Amarapuka, D.; Alexander, M.J.; Chutaputti, A.; Chien, R.N.; Hasnian, S.S.; Leung, N.; Lesmana, L.; Phiet, P.H.; et al. Chronic hepatitis B virus infection in Asian countries. J. Gastroenterol. Hepatol. 2000, 15, 1356–1361. [Google Scholar] [CrossRef] [PubMed]
- Hoofnagle, J.H. Reactivation of hepatitis B. Hepatology 2009, 49, S156–S165. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Bae, S.C.; Song, G.G. Hepatitis B virus reactivation in HBsAg-positive patients with rheumatic diseases undergoing anti-tumor necrosis factor therapy or DMARDs. Int. J. Rheum. Dis. 2013, 16, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Liu, C.Y.; Tsai, C.Y.; Huang, D.F.; Lin, H.Y.; Lee, M.H.; Huang, Y.H. Hepatitis B Virus Reactivation in Rheumatoid Arthritis Patients Undergoing Biologics Treatment. J. Infect. Dis. 2017, 215, 566–573. [Google Scholar] [CrossRef]
- Hsu, P.I.; Lai, K.H.; Cheng, J.S.; Kao, S.S.; Li, Y.R.; Sun, W.C.; Chen, W.C.; Lin, K.H.; Shin, C.A.; Chiang, P.H.; et al. Prevention of acute exacerbation of chronic hepatitis B infection in cancer patients receiving chemotherapy in a hepatitis B virus endemic area. Hepatology 2015, 62, 387–396. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.H.; Lin, H.C.; Lee, S.D. Management of chemotherapy-induced hepatitis B virus reactivation. J. Chin. Med. Assoc. 2012, 75, 359–362. [Google Scholar] [CrossRef]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B: Update 2009. Hepatology 2009, 50, 661–662. [Google Scholar] [CrossRef]
- Huang, Y.H.; Hsiao, L.T.; Hong, Y.C.; Chiou, T.J.; Yu, Y.B.; Gau, J.P.; Liu, C.Y.; Yang, M.H.; Tzeng, C.H.; Lee, P.C.; et al. Randomized controlled trial of entecavir prophylaxis for rituximab-associated hepatitis B virus reactivation in patients with lymphoma and resolved hepatitis B. J. Clin. Oncol. 2013, 31, 2765–2772. [Google Scholar] [CrossRef]
- Chen, M.H.; Chen, M.H.; Chou, C.T.; Hou, M.C.; Tsai, C.Y.; Huang, Y.H. Low but Long-lasting Risk of Reversal of Seroconversion in Patients with Rheumatoid Arthritis Receiving Immunosuppressive Therapy. Clin. Gastroenterol. Hepatol. 2020, 18, 2573–2581. [Google Scholar] [CrossRef]
- Yeo, W.; Zee, B.; Zhong, S.; Chan, P.K.; Wong, W.L.; Ho, W.M.; Lam, K.C.; Johnson, P.J. Comprehensive analysis of risk factors associating with Hepatitis B virus (HBV) reactivation in cancer patients undergoing cytotoxic chemotherapy. Br. J. Cancer. 2004, 90, 1306–1311. [Google Scholar] [CrossRef]
- Bagavant, H.; Deshmukh, U.S.; Gaskin, F.; Fu, S.M. Lupus glomerulonephritis revisited 2004: Autoimmunity and end-organ damage. Scand. J. Immunol. 2004, 60, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Hsiao, L.T.; Tsai, C.Y.; Huang, Y.H.; Chou, C.T. Clinical significance of chronic hepatitis B virus infection in patients with primary Sjogren’s syndrome. Clin. Rheumatol. 2012, 31, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Ram, M.; Anaya, J.M.; Barzilai, O.; Izhaky, D.; Porat Katz, B.S.; Blank, M.; Shoenfeld, Y. The putative protective role of hepatitis B virus (HBV) infection from autoimmune disorders. Autoimmun. Rev. 2008, 7, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.L.; Tsai, S.T.; Chan, C.Y.; Hwang, S.J.; Tsai, C.Y.; Wu, J.C.; Lu, R.H.; Lin, B.C.; Lee, S.D. Hepatitis B infection and changes in interferon-alpha and -gamma production in patients with systemic lupus erythematosus in Taiwan. J. Gastroenterol. Hepatol. 1997, 12, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Qiu, M.; Li, M.; Lu, C.; Gu, J. Low prevalence of hepatitis B virus infection in patients with systemic lupus erythematosus in southern China. Rheumatol. Int. 2010, 30, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Bertsias, G.; Ioannidis, J.P.; Boletis, J.; Bombardieri, S.; Cervera, R.; Dostal, C.; Font, J.; Gilboe, I.M.; Houssiau, F.; Huizinga, T.; et al. EULAR recommendations for the management of systemic lupus erythematosus. Report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics. Ann. Rheum. Dis. 2008, 67, 195–205. [Google Scholar] [CrossRef]
- Tur-Kaspa, R.; Burk, R.D.; Shaul, Y.; Shafritz, D.A. Hepatitis B virus DNA contains a glucocorticoid-responsive element. Proc. Natl. Acad. Sci. USA 1986, 83, 1627–1631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, C.K.; Wang, L.H.; Lin, H.M.; Chi, C.W. Glucocorticoid stimulates hepatitis B viral gene expression in cultured human hepatoma cells. Hepatology 1992, 16, 13–18. [Google Scholar] [CrossRef]
- Fessler, B.J.; Boumpas, D.T. Severe major organ involvement in systemic lupus erythematosus: Diagnosis and management. Rheum. Dis. Clin. N. Am. 1995, 21, 81–98. [Google Scholar] [CrossRef]
- Bertsias, G.K.; Salmon, J.E.; Boumpas, D.T. Therapeutic opportunities in systemic lupus erythematosus: State of the art and prospects for the new decade. Ann. Rheum. Dis. 2010, 69, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Li, J.B.; Sun, Q.L.; Li, X. Reactivation of hepatitis B virus after steroid treatment in rheumatic diseases. J. Rheumatol. 2011, 38, 181–182. [Google Scholar] [CrossRef]
- Perrillo, R.P.; Gish, R.; Falck-Ytter, Y.T. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology 2015, 148, 221–244. [Google Scholar] [CrossRef]
- Kim, T.W.; Kim, M.N.; Kwon, J.W.; Kim, K.M.; Kim, S.H.; Kim, W.; Park, H.W.; Chang, Y.S.; Cho, S.H.; Min, K.U.; et al. Risk of hepatitis B virus reactivation in patients with asthma or chronic obstructive pulmonary disease treated with corticosteroids. Respirology 2010, 15, 1092–1097. [Google Scholar] [CrossRef]
- Grammatikos, A.P.; Tsokos, G.C. Immunodeficiency and autoimmunity: Lessons from systemic lupus erythematosus. Trends Mol. Med. 2012, 18, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.Y.; Suh, C.H. Infection in systemic lupus erythematosus, similarities, and differences with lupus flare. Korean J. Intern. Med. 2017, 32, 429–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makin, A.J.; Wendon, J.; Fitt, S.; Portmann, B.C.; Williams, R. Fulminant hepatic failure secondary to hydroxychloroquine. Gut 1994, 35, 569–570. [Google Scholar] [CrossRef] [PubMed]
- Anelli, M.G.; Scioscia, C.; Grattagliano, I.; Lapadula, G. Old and new antirheumatic drugs and the risk of hepatotoxicity. Ther. Drug Monit. 2012, 34, 622–628. [Google Scholar] [CrossRef]
- Loomba, R.; Liang, T.J. Hepatitis B Reactivation Associated with Immune Suppressive and Biological Modifier Therapies: Current Concepts, Management Strategies, and Future Directions. Gastroenterology 2017, 152, 1297–1309. [Google Scholar] [CrossRef] [Green Version]
- Tohme, R.A.; Bulkow, L.; Homan, C.E.; Negus, S.; McMahon, B.J. Rates and risk factors for hepatitis B reactivation in a cohort of persons in the inactive phase of chronic hepatitis B-Alaska, 2001–2010. J. Clin. Virol. 2013, 58, 396–400. [Google Scholar] [CrossRef] [Green Version]
- Yeo, W.; Chan, T.C.; Leung, N.W.; Lam, W.Y.; Mo, F.K.; Chu, M.T.; Chan, H.L.; Hui, E.P.; Lei, K.I.; Mok, T.S.; et al. Hepatitis B virus reactivation in lymphoma patients with prior resolved hepatitis B undergoing anticancer therapy with or without rituximab. J. Clin. Oncol. 2009, 27, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.A.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Thong, B.Y.; Koh, E.T.; Chng, H.H.; Chow, W.C. Outcomes of chronic hepatitis B infection in Oriental patients with rheumatic diseases. Ann. Acad. Med. Singap. 2007, 36, 100–105. [Google Scholar]
- Fontana, R.J.; Hann, H.W.; Perrillo, R.P.; Vierling, J.M.; Wright, T.; Rakela, J.; Anschuetz, G.; Davis, R.; Gardner, S.D.; Brown, N.A. Determinants of early mortality in patients with decompensated chronic hepatitis B treated with antiviral therapy. Gastroenterology 2002, 123, 719–727. [Google Scholar] [CrossRef]
- Tseng, P.L.; Lu, S.N.; Tung, H.D.; Wang, J.H.; Changchien, C.S.; Lee, C.M. Determinants of early mortality and benefits of lamivudine therapy in patients with hepatitis B virus-related decompensated liver cirrhosis. J. Viral. Hepat. 2005, 12, 386–392. [Google Scholar] [CrossRef]
- Khokhar, O.S.; Farhadi, A.; McGrail, L.; Lewis, J.H. Oncologists and hepatitis B: A survey to determine current level of awareness and practice of antiviral prophylaxis to prevent reactivation. Chemotherapy 2009, 55, 69–75. [Google Scholar] [CrossRef]
- Tran, T.T.; Rakoski, M.O.; Martin, P.; Poordad, F. Screening for hepatitis B in chemotherapy patients: Survey of current oncology practices. Aliment. Pharmacol. Ther. 2010, 31, 240–246. [Google Scholar] [CrossRef]
- Hwang, J.P.; Somerfield, M.R.; Alston-Johnson, D.E.; Cryer, D.R.; Feld, J.J.; Kramer, B.S.; Sabichi, A.L.; Wong, S.L.; Artz, A.S. Hepatitis B Virus Screening for Patients with Cancer Before Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update. J. Clin. Oncol. 2015, 33, 2212–2220. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.M.; Alarcon, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Lan, J.L.; Chen, Y.M.; Hsieh, T.Y.; Chen, Y.H.; Hsieh, C.W.; Chen, D.Y.; Yang, S.S. Kinetics of viral loads and risk of hepatitis B virus reactivation in hepatitis B core antibody-positive rheumatoid arthritis patients undergoing anti-tumour necrosis factor alpha therapy. Ann. Rheum. Dis. 2011, 70, 1719–1725. [Google Scholar] [CrossRef] [Green Version]
- Maria, V.A.; Victorino, R.M. Development and validation of a clinical scale for the diagnosis of drug-induced hepatitis. Hepatology 1997, 26, 664–669. [Google Scholar] [CrossRef]
- Andrade, R.J.; Aithal, G.P.; Björnsson, E.S.; Kaplowitz, N.; Kullak-Ublick, G.A.; Larrey, D.; Karlsen, T.H. EASL clinical practice guidelines: Drug-induced liver injury. J. Hepatol. 2019, 70, 1222–1261. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.; Tsou, H.H.; Lin, S.J.; Wang, M.C.; Yao, M.; Hwang, W.L.; Kao, W.Y.; Chiu, C.F.; Lin, S.F.; Lin, J.; et al. Chemotherapy-induced hepatitis B reactivation in lymphoma patients with resolved HBV infection: A prospective study. Hepatology 2014, 59, 2092–2100. [Google Scholar] [CrossRef]
- Sheen, I.S.; Liaw, Y.F.; Tai, D.I.; Chu, C.M. Hepatic decompensation associated with hepatitis B e antigen clearance in chronic type B hepatitis. Gastroenterology 1985, 89, 732–735. [Google Scholar] [CrossRef]
- Jeng, W.J.; Sheen, I.S.; Liaw, Y.F. Hepatitis B virus DNA level predicts hepatic decompensation in patients with acute exacerbation of chronic hepatitis B. Clin. Gastroenterol. Hepatol. 2010, 8, 541–545. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | All | HBsAg-Positive | Resolved HBV | p-Value |
|---|---|---|---|---|
| N = 118 | N = 55 | N = 63 | ||
| Age at diagnosis of SLE (years) | 35.2 ± 14.7 | 37.0 ± 15.2 | 33.6 ± 14.2 | 0.213 |
| Female | 97 (82.2) | 44 (80.0) | 53 (84.1) | 0.559 |
| Baseline ALT (IU/mL) | 23.4 ± 12.3 | 25.0 ± 12.3 | 22.1 ± 12.2 | 0.200 |
| Baseline AST (IU/mL) | 24.7 ± 10.3 | 26.3 ± 10.5 | 23.4 ± 10.0 | 0.125 |
| Baseline total bilirubin (mg/dL) | 0.42 ± 0.19 | 0.45 ± 0.19 | 0.40 ± 0.19 | 0.166 |
| HBeAg-positive | 10/64 (15.6) | 10/47 (21.3) | 0/17 (0.0) | - |
| Anti-HBs positive | 50 (42.4) | 0 (0.0) | 50 (79.4) | - |
| Immunologic profiles | ||||
| ANA titer > 1:80 | 118 (100.0) | 55 (100.0) | 63 (100.0) | - |
| Anti-SSA/Ro positive | 50/94 (53.2) | 17/42 (40.5) | 33/52 (63.5) | 0.026 * |
| Anti-SSB/La positive | 17/89 (19.1) | 5/41 (12.2) | 12/48 (25.0) | 0.120 |
| Anti-Smith positive | 11/78 (14.1) | 2/39 (5.1) | 9/39 (23.1) | 0.018 * |
| Anti-RNP positive | 23/74 (31.1) | 7/36 (19.4) | 16/38 (42.1) | 0.028 * |
| Anti-dsDNA positive | 105 (89.0) | 47 (85.5) | 58 (92.1) | 0.252 |
| Clinical manifestations | ||||
| Hematologic disorder | 81 (68.6) | 34 (61.8) | 47 (74.6) | 0.174 |
| Kidney involvement | 49 (41.5) | 20 (36.4) | 29 (46.0) | 0.287 |
| CNS involvement | 20 (16.9) | 10 (18.2) | 10 (15.9) | 0.739 |
| Psychosis | 4 (3.4) | 2 (3.6) | 2 (3.2) | 0.890 |
| Serositis | 13 (11.0) | 7 (12.7) | 6 (14.3) | 0.580 |
| Joint involvement | 86 (72.9) | 37 (67.3) | 49 (77.8) | 0.201 |
| Skin involvement | 105 (89.0) | 47 (85.5) | 58 (92.1) | 0.252 |
| Follow up (years) | 15.4 ± 10.3 | 11.7 ± 9.4 | 18.6 ± 10.2 | <0.001 * |
| Demographics | HBV Reactivation | No HBV Reactivation | p-Value |
|---|---|---|---|
| N = 30 | N = 25 | ||
| Age at diagnosis of SLE (years) | 37.6 ± 16.5 | 36.3 ± 13.8 | 0.758 |
| Female | 21 (70.0) | 23 (92.0) | 0.035 * |
| Baseline ALT (IU/mL) | 26.3 ± 10.8 | 23.4 ± 14.0 | 0.400 |
| Baseline AST (IU/mL) | 26.8 ± 8.9 | 25.7 ± 12.4 | 0.718 |
| Baseline TBIL (mg/dL) | 0.45 ± 0.22 | 0.44 ± 0.15 | 0.776 |
| HBeAg positive | 9/28 (32.1) | 0/19 (0.0) | - |
| Immunosuppressive treatment | 0.046 * | ||
| No treatment | 3 | 7 | |
| GC alone | 7 | 3 | |
| Immunosuppressants † alone | 2 | 6 | |
| GC in combination with other immunosuppressants † | 18 | 9 | |
| Any GC containing regiments | 25 (83.3) | 12 (48.0) | 0.005 * |
| Duration of GC (days) | 212 (50–833) | 0 (0–1522) | 0.768 |
| Cumulative GC use (gm) ‡ | 3.6 (0.5–16.4) | 3.9 (0–27.5) | 0.654 |
| GC ‡ ≥ 10 mg/day | 22 (73.3) | 10 (40.0) | 0.012 * |
| Number of immunosuppressants † | 0.137 | ||
| 1 | 11 | 11 | |
| 2 | 5 | 3 | |
| ≥3 | 4 | 1 | |
| Peak HBV viral load during HBVr (IU/mL) | 1,048,000 (41,500–13,700,000) | - | - |
| Peak ALT during HBVr (IU/mL) | 281 (151–560) | - | - |
| Peak T. Bili during HBVr (mg/dL) | 2.2 (0.8–4.8) | - | - |
| Rescue antiviral treatment | 26 (86.7) | - | - |
| Predictors | Total (n = 55) Number (%) | HBVr (n = 30) Number (%) | Observed Period (Person-Year) | Crude HR (95% CI) | p-Value | Adjusted HR 1 (95% CI) | p-Value | Adjusted HR 2 (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Age at diagnosis of SLE | |||||||||
| <40 years | 34 (61.82) | 18 (60.00) | 519.7 | 1.00 | 1.00 | 1.0 | |||
| ≥40 years | 21 (38.18) | 12 (40.00) | 122.2 | 2.85 (1.26–6.45) | 0.012 * | 5.30 (2.12–13.25) | <0.001 * | 4.12 (1.68–10.08) | 0.002 * |
| Gender | |||||||||
| Male | 11 (20.00) | 9 (30.00) | 92.8 | 1.00 | 1.0 | ||||
| Female | 44 (80.00) | 21 (70.00) | 549.1 | 2.41 (1.09–5.31) | 0.030 * | 2.11 (0.93–4.78) | 0.072 | ||
| Baseline ALT | |||||||||
| <20 IU/mL | 23 (41.82) | 9 (30.00) | 290.7 | 1.00 | 1.00 | 1.00 | |||
| ≥20 IU/mL | 32 (58.18) | 21 (70.00) | 351.2 | 1.80 (0.82–3.93) | 0.142 | 2.44 (1.07–5.58) | 0.034 * | 2.73 (1.17–6.38) | 0.020 * |
| Baseline AST | |||||||||
| <20 IU/mL | 15 (27.27) | 7 (23.33) | 177.1 | 1.00 | |||||
| ≥20 IU/mL | 40 (72.73) | 23 (76.67) | 464.9 | 1.13 (0.48–2.67) | 0.775 | ||||
| GC | |||||||||
| No | 18 (32.73) | 5 (16.67) | 242.3 | 1.00 | 1.00 | ||||
| Yes | 37 (67.27) | 25 (83.33) | 399.6 | 3.01 (1.15–7.88) | 0.025 * | 4.78 (1.72–13.28) | 0.003 * | ||
| GC ‡ ≥ 10 mg/day | |||||||||
| No | 23 (41.8) | 8 (26.7) | 313.7 | 1.00 | 1.00 | ||||
| Yes | 32 (58.2) | 22 (73.3) | 328.2 | 2.58 (1.15–5.82) | 0.022 * | 3.68 (1.56–8.65) | 0.003 * | ||
| Drug group | |||||||||
| No treatment | 10 (18.18) | 3 (10.00) | 141.2 | 1.00 | |||||
| GC alone | 10 (18.18) | 7 (23.33) | 79.8 | 3.06 (0.79–11.89) | 0.107 | ||||
| ISD † alone | 8 (14.55) | 2 (6.67) | 101.1 | 0.93 (0.15–5.69) | 0.940 | ||||
| GC + ISD † | 27 (49.09) | 18 (60.0) | 319.9 | 2.52 (0.74–8.65) | 0.141 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.-H.; Wu, C.-S.; Chen, M.-H.; Tsai, C.-Y.; Lee, F.-Y.; Huang, Y.-H. High Risk of Viral Reactivation in Hepatitis B Patients with Systemic Lupus Erythematosus. Int. J. Mol. Sci. 2021, 22, 9116. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22179116
Chen M-H, Wu C-S, Chen M-H, Tsai C-Y, Lee F-Y, Huang Y-H. High Risk of Viral Reactivation in Hepatitis B Patients with Systemic Lupus Erythematosus. International Journal of Molecular Sciences. 2021; 22(17):9116. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22179116
Chicago/Turabian StyleChen, Ming-Han, Chien-Sheng Wu, Ming-Huang Chen, Chang-Youh Tsai, Fa-Yauh Lee, and Yi-Hsiang Huang. 2021. "High Risk of Viral Reactivation in Hepatitis B Patients with Systemic Lupus Erythematosus" International Journal of Molecular Sciences 22, no. 17: 9116. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22179116