
Dickkopf-1 Promotes Angiogenesis and is a Biomarker for Hepatic Stem Cell-like Hepatocellular Carcinoma

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
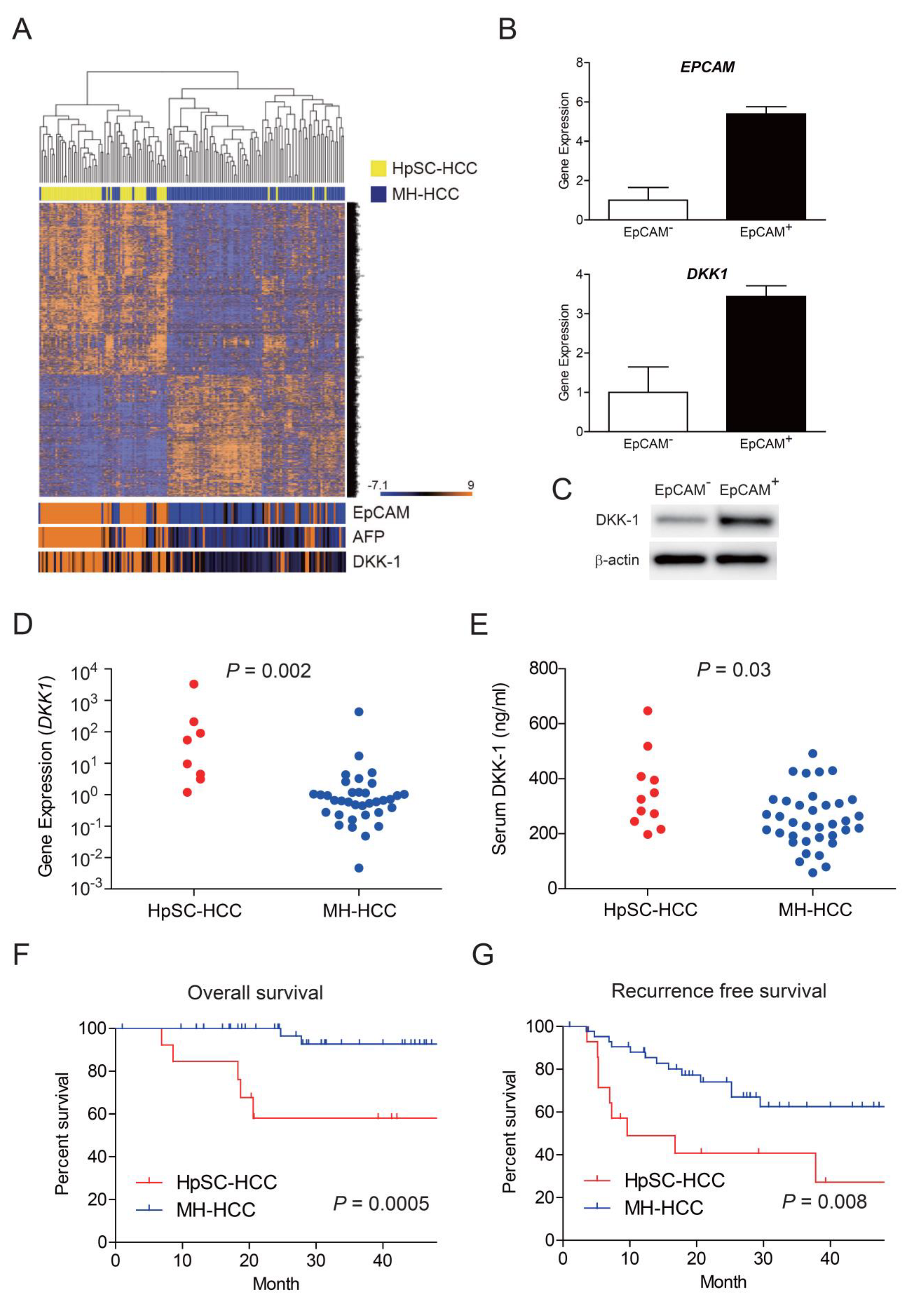
2.1. Elevation of Serum DKK-1 Levels in HpSC-HCC
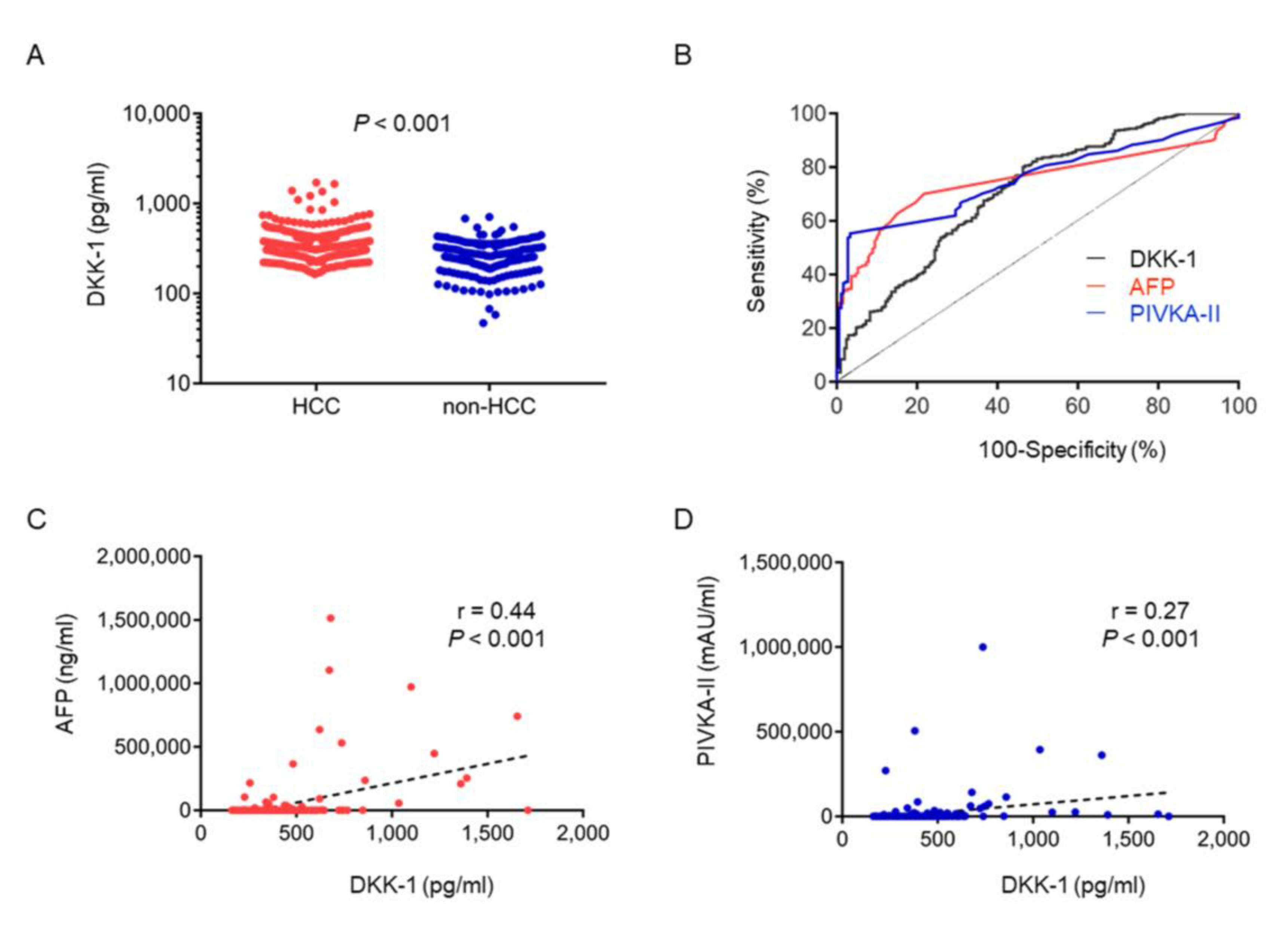
2.2. Serum DKK-1 as a Diagnostic Marker for HCC
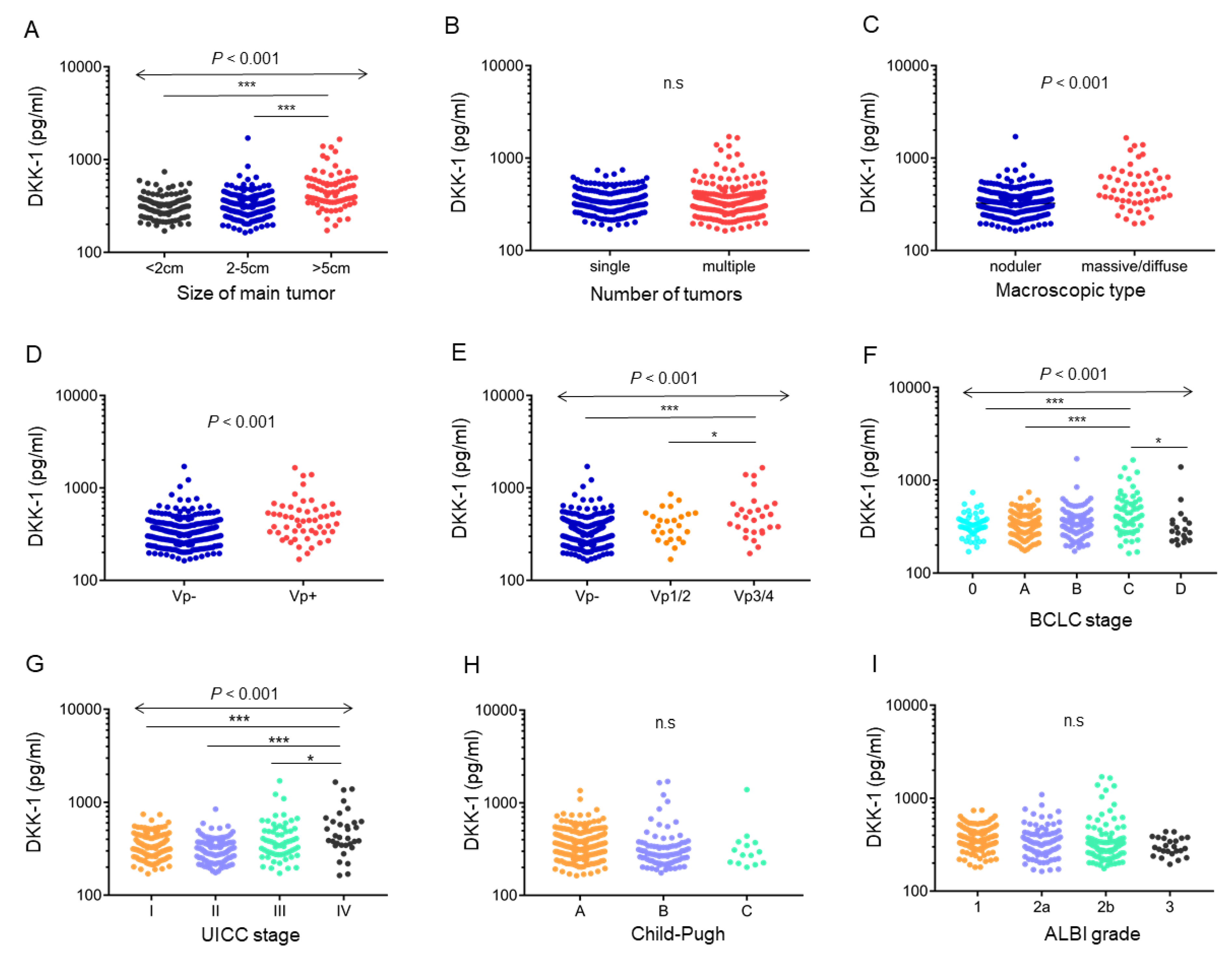
2.3. Serum DKK-1 Levels and Clinicopathological Characteristics of HCC
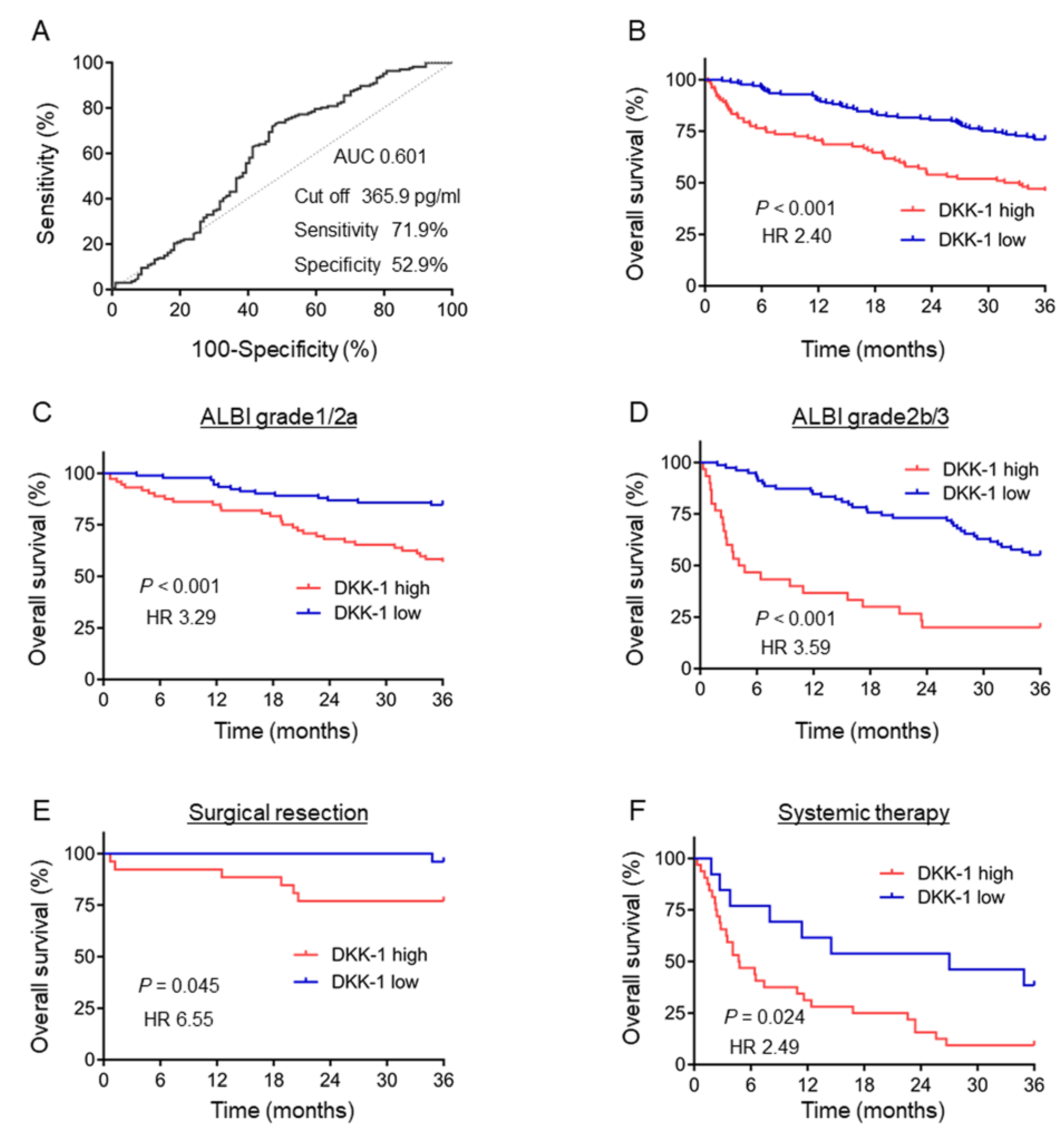
2.4. Serum DKK-1 Level as a Prognostic Marker of HCC
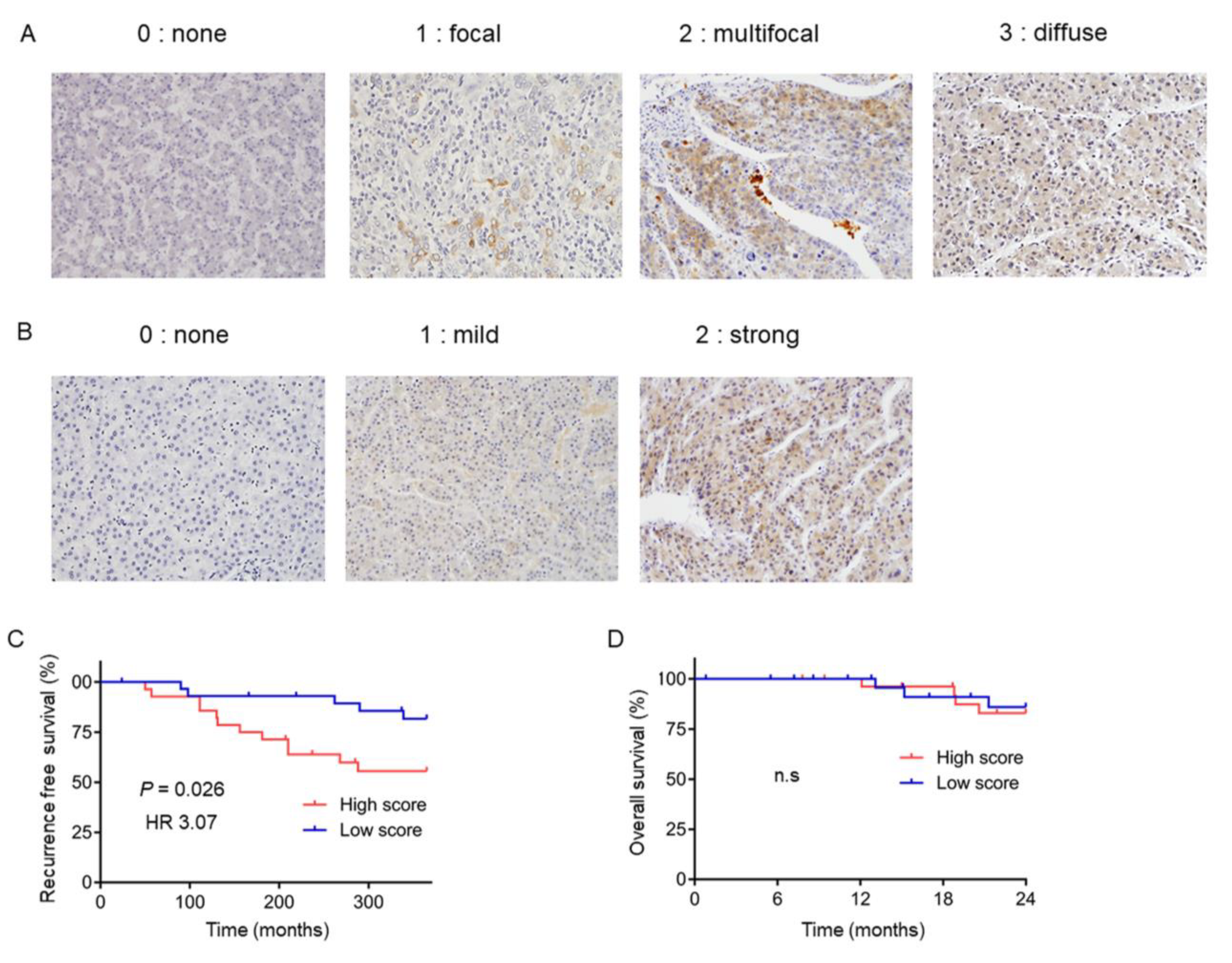
2.5. DKK-1 Expression in HCC Tissues is Correlated with Recurrence
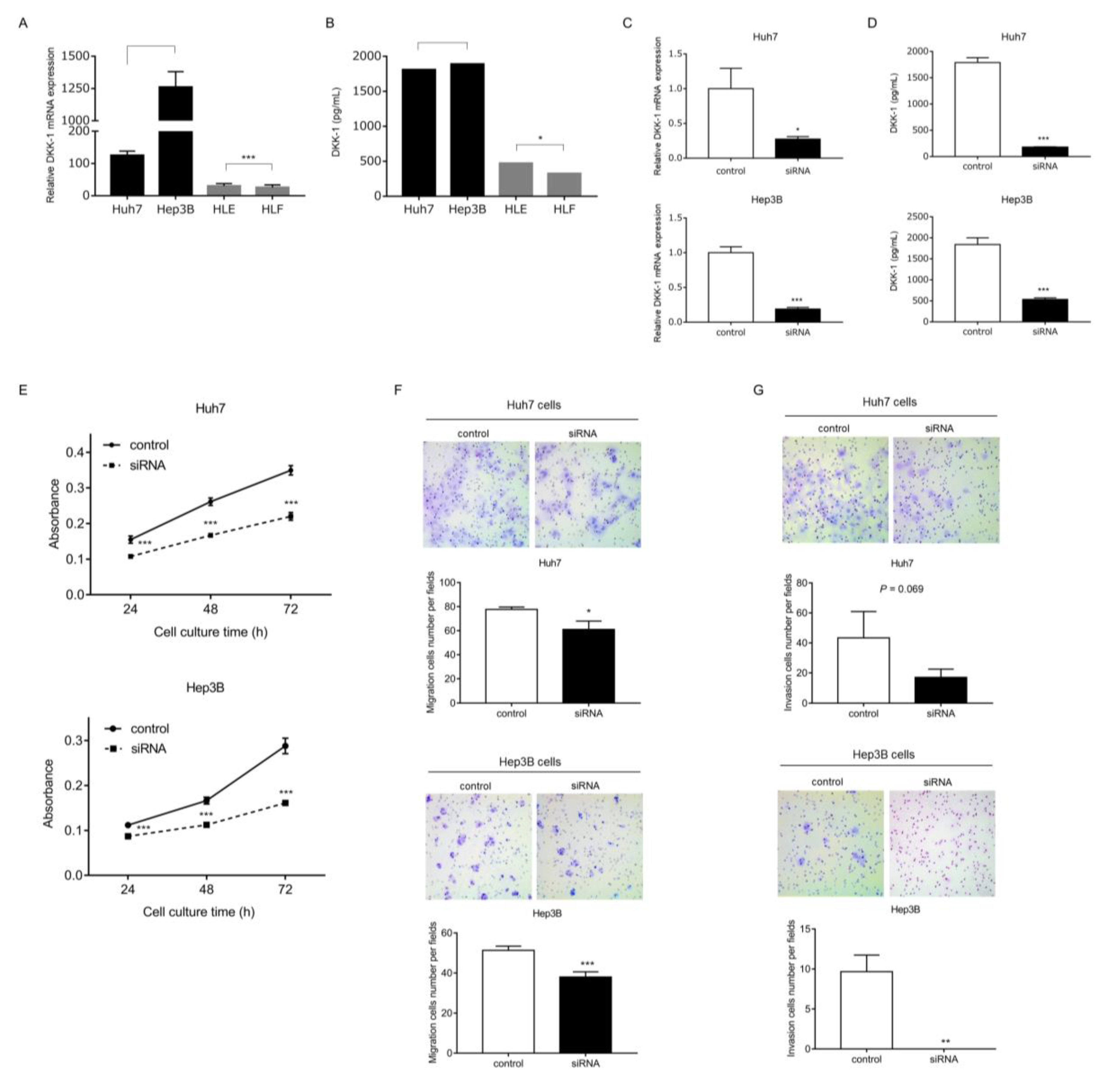
2.6. The Role of DKK-1 in HCC Growth
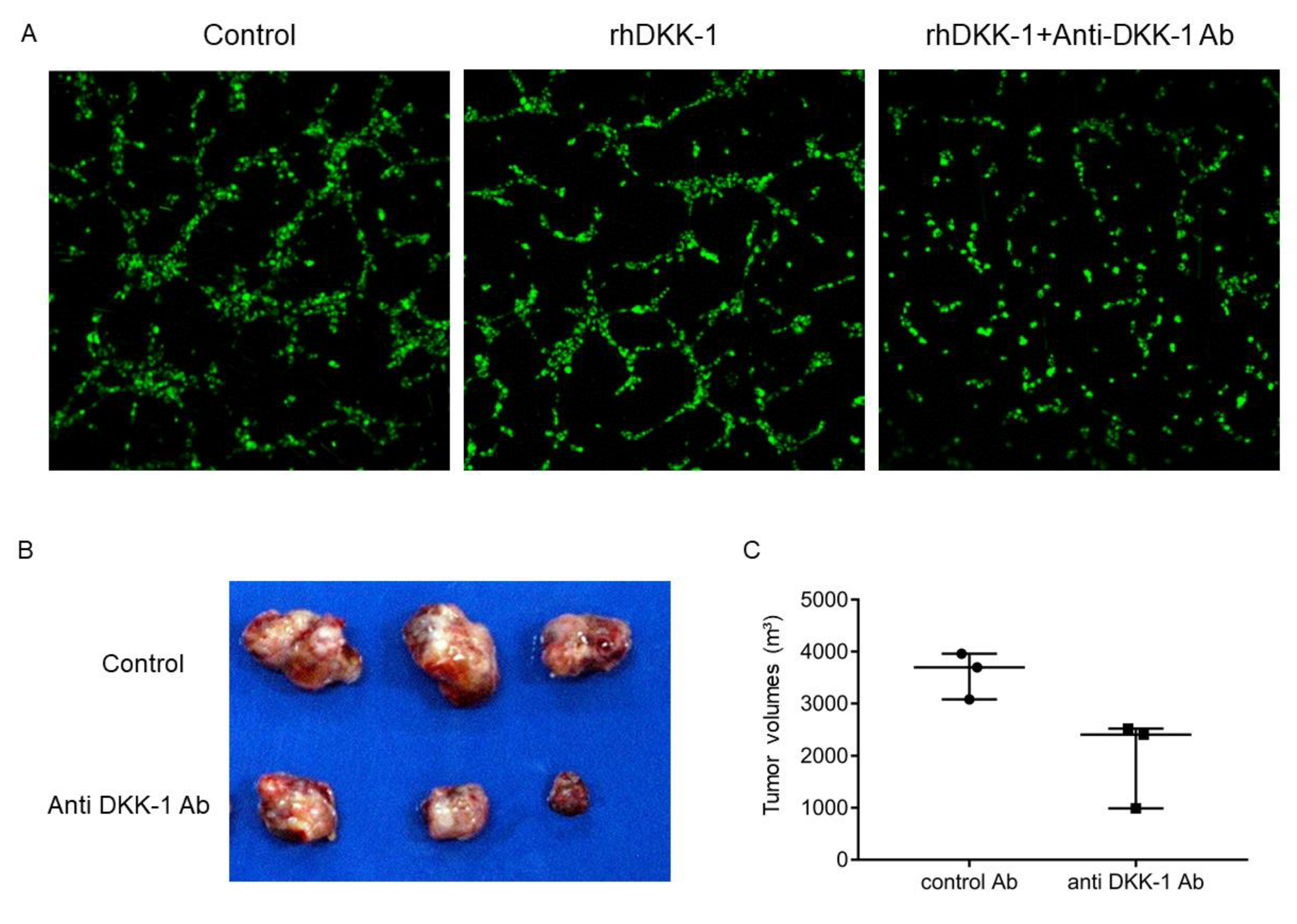
2.7. Anti-DKK-1 Antibody as a Treatment Option for EpCAM-Positive DKK-1-Positive HCC
3. Discussion
4. Materials and Methods
4.1. Patients and Measurement of Serum DKK-1 Levels
4.2. Microarray Analysis
4.3. Western Blot Analysis
4.4. Immunohistochemical Staining
4.5. Cell Lines and Reagents
4.6. Cell Sorting
4.7. Real-Time Quantitative PCR
4.8. RNA Interference
4.9. Cell Proliferation Assay
4.10. Transwell Invasion/Migration Assay
4.11. Tube Formation Assay
4.12. Animal Studies
4.13. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singal, A.G.; Lampertico, P.; Nahon, P. Epidemiology and surveillance for hepatocellular carcinoma: New trends. J. Hepatol. 2020, 72, 250–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangiovanni, A.; Colombo, M. Treatment of hepatocellular carcinoma: Beyond international guidelines. Liver Int. 2016, 36 (Suppl. S1), 124–129. [Google Scholar] [CrossRef] [Green Version]
- Aghoram, R.; Cai, P.; Dickinson, J.A. Alpha-foetoprotein and/or liver ultrasonography for screening of hepatocellular carcinoma in patients with chronic hepatitis B. Cochrane Database Syst. Rev. 2012, 2012, CD002799. [Google Scholar] [CrossRef]
- Marrero, J.A.; Feng, Z.; Wang, Y.; Nguyen, M.H.; Befeler, A.S.; Roberts, L.R.; Reddy, K.R.; Harnois, D.; Llovet, J.M.; Normolle, D.; et al. Alpha-fetoprotein, des-gamma carboxyprothrombin, and lectin-bound alpha-fetoprotein in early hepatocellular carcinoma. Gastroenterology 2009, 137, 110–118. [Google Scholar] [CrossRef] [Green Version]
- El-Shayeb, A.F.; El-Habachi, N.M.; Mansour, A.R.; Zaghloul, M.S. Serum midkine is a more sensitive predictor for hepatocellular carcinoma than Dickkopf-1 and alpha-L-fucosidase in cirrhotic HCV patients. Medicine (Baltimore) 2021, 100, e25112. [Google Scholar] [CrossRef]
- Rizzo, A.; Dadduzio, V.; Ricci, A.D.; Massari, F.; Di Federico, A.; Gadaleta-Caldarola, G.; Brandi, G. Lenvatinib plus pembrolizumab: The next frontier for the treatment of hepatocellular carcinoma? Expert. Opin. Investig. Drugs. 2021, 1–8. [Google Scholar] [CrossRef]
- Rizzo, A.; Brandi, G. Biochemical predictors of response to immune checkpoint inhibitors in unresectable hepatocellular carcinoma. Cancer Treat. Res. Commun. 2021, 27, 100328. [Google Scholar] [CrossRef]
- Glinka, A.; Wu, W.; Delius, H.; Monaghan, A.P.; Blumenstock, C.; Niehrs, C. Dickkopf-1 is a member of a new family of secreted proteins and functions in head induction. Nature 1998, 391, 357–362. [Google Scholar] [CrossRef]
- Niehrs, C. Function and biological roles of the Dickkopf family of Wnt modulators. Oncogene 2006, 25, 7469–7481. [Google Scholar] [CrossRef] [Green Version]
- Mao, B.; Wu, W.; Davidson, G.; Marhold, J.; Li, M.; Mechler, B.M.; Delius, H.; Hoppe, D.; Stannek, P.; Walter, C.; et al. Kremen proteins are Dickkopf receptors that regulate Wnt/beta-catenin signalling. Nature 2002, 417, 664–667. [Google Scholar] [CrossRef]
- Sakabe, T.; Azumi, J.; Umekita, Y.; Toriguchi, K.; Hatano, E.; Hirooka, Y.; Shiota, G. Expression of cancer stem cell-associated DKK1 mRNA serves as prognostic marker for hepatocellular carcinoma. Anticancer Res. 2017, 37, 4881–4888. [Google Scholar] [CrossRef]
- Choi, S.H.; Kim, H.; Lee, H.G.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.H.; Kim, S.U. Dickkopf-1 induces angiogenesis via VEGF receptor 2 regulation independent of the Wnt signaling pathway. Oncotarget 2017, 8, 58974–58984. [Google Scholar] [CrossRef] [Green Version]
- Liang, L.; He, H.; Lv, R.; Zhang, M.; Huang, H.; An, Z.; Li, S. Preliminary mechanism on the methylation modification of Dkk-1 and Dkk-3 in hepatocellular carcinoma. Tumour Biol. 2015, 36, 1245–1250. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, X.; Zhao, F.; Shen, Q.; Wang, Z.; Lv, X.; Hu, B.; Yu, B.; Fan, J.; Qin, W. Overexpression of Dickkopf-1 predicts poor prognosis for patients with hepatocellular carcinoma after orthotopic liver transplantation by promoting cancer metastasis and recurrence. Med. Oncol. 2014, 31, 966. [Google Scholar] [CrossRef]
- Yamashita, T.; Forgues, M.; Wang, W.; Kim, J.W.; Ye, Q.; Jia, H.; Budhu, A.; Zanetti, K.A.; Chen, Y.; Qin, L.X.; et al. EpCAM and alpha-fetoprotein expression defines novel prognostic subtypes of hepatocellular carcinoma. Cancer Res. 2008, 68, 1451–1461. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, T.; Ji, J.; Budhu, A.; Forgues, M.; Yang, W.; Wang, H.Y.; Jia, H.; Ye, Q.; Qin, L.X.; Wauthier, E.; et al. EpCAM-positive hepatocellular carcinoma cells are tumor-initiating cells with stem/progenitor cell features. Gastroenterology 2009, 136, 1012–1024. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Peng, J.X.; Yang, J.Q.; Yang, L.Y. Identification of gene expression profiling in hepatocellular carcinoma using cDNA microarrays. Dig. Dis. Sci. 2009, 54, 2729–2735. [Google Scholar] [CrossRef]
- Choi, Y.W.; Park, J.S.; Han, J.H.; Kim, J.H.; Ahn, M.S.; Lee, H.W.; Kang, S.Y.; Choi, J.H.; Jeong, S.H. Strong immunoexpression of dickkopf-1 is associated with response to bortezomib in multiple myeloma. Leuk. Lymphoma 2018, 59, 2670–2678. [Google Scholar] [CrossRef] [PubMed]
- Pamuk, G.E.; Uyanik, M.S.; Pamuk, O.N.; Maden, M.; Tapan, U. Decreased dickkopf-1 levels in chronic lymphocytic leukemia and increased osteopontin levels in non-Hodgkin’s lymphoma at initial diagnosis: Could they be playing roles in pathogenesis? Hematology 2015, 20, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Sun, B.; Qi, L.; Li, Y.; Zhao, X.; Zhang, D.; Zhang, Y. Dickkopf-1 expression is down-regulated during the colorectal adenoma-carcinoma sequence and correlates with reduced microvessel density and VEGF expression. Histopathology 2015, 67, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Han, S.X.; Zhou, X.; Sui, X.; He, C.C.; Cai, M.J.; Ma, J.L.; Zhang, Y.Y.; Zhou, C.Y.; Ma, C.X.; Varela-Ramirez, A.; et al. Serum dickkopf-1 is a novel serological biomarker for the diagnosis and prognosis of pancreatic cancer. Oncotarget 2015, 6, 19907–19917. [Google Scholar] [CrossRef] [Green Version]
- Shen, Q.; Fan, J.; Yang, X.R.; Tan, Y.; Zhao, W.; Xu, Y.; Wang, N.; Niu, Y.; Wu, Z.; Zhou, J.; et al. Serum DKK1 as a protein biomarker for the diagnosis of hepatocellular carcinoma: A large-scale, multicentre study. Lancet Oncol. 2012, 13, 817–826. [Google Scholar] [CrossRef]
- Yang, H.; Chen, G.D.; Fang, F.; Liu, Z.; Lau, S.H.; Zhang, J.F.; Lau, W.Y.; Yang, L.Y. Dickkopf-1: As a diagnostic and prognostic serum marker for early hepatocellular carcinoma. Int. J. Biol. Markers 2013, 28, 286–297. [Google Scholar] [CrossRef]
- Mao, L.; Wang, Y.; Wang, D.; Han, G.; Fu, S.; Wang, J. TEMs but not DKK1 could serve as complementary biomarkers for AFP in diagnosing AFP-negative hepatocellular carcinoma. PLoS ONE 2017, 12, e0183880. [Google Scholar] [CrossRef] [Green Version]
- Jang, E.S.; Jeong, S.H.; Kim, J.W.; Choi, Y.S.; Leissner, P.; Brechot, C. Diagnostic performance of alpha-fetoprotein, protein induced by vitamin K absence, osteopontin, Dickkopf-1 and its combinations for hepatocellular carcinoma. PLoS ONE 2016, 11, e0151069. [Google Scholar] [CrossRef]
- Ge, T.; Shen, Q.; Wang, N.; Zhang, Y.; Ge, Z.; Chu, W.; Lv, X.; Zhao, F.; Zhao, W.; Fan, J.; et al. Diagnostic values of alpha-fetoprotein, dickkopf-1, and osteopontin for hepatocellular carcinoma. Med. Oncol. 2015, 32, 59. [Google Scholar] [CrossRef]
- Tung, E.K.; Mak, C.K.; Fatima, S.; Lo, R.C.; Zhao, H.; Zhang, C.; Dai, H.; Poon, R.T.; Yuen, M.F.; Lai, C.L.; et al. Clinicopathological and prognostic significance of serum and tissue Dickkopf-1 levels in human hepatocellular carcinoma. Liver Int. 2011, 31, 1494–1504. [Google Scholar] [CrossRef]
- Younis, Y.S.; Alegaily, H.S.; Elagawy, W.; Semeya, A.A.; Abo-Amer, Y.E.; El-Abgeegy, M.; Mostafa, S.M.; Elsergany, H.F.; Abd-Elsalam, S. Serum Dickopff 1 as a novel biomarker in hepatocellular carcinoma diagnosis and follow up after ablative therapy. Cancer Manag. Res. 2019, 11, 10555–10562. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhao, Y.; Yang, Q. Sensitivity and specificity of Dickkopf-1 protein in serum for diagnosing hepatocellular carcinoma: A meta-analysis. Int. J. Biol. Markers 2014, 29, e403–e410. [Google Scholar] [CrossRef]
- Li, Z.; Mou, L.; Gao, H.; Zeng, Y.; Tang, X.; Deng, X.; Pu, Z.; Ni, Y.; Zhan, Y. Diagnostic accuracy of serum dickkopf-1 protein in diagnosis hepatocellular carcinoma: An updated meta-analysis. Medicine (Baltimore) 2019, 98, e16725. [Google Scholar] [CrossRef]
- Bruix, J.; Cheng, A.L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Poté, N.; Cauchy, F.; Albuquerque, M.; Voitot, H.; Belghiti, J.; Castera, L.; Puy, H.; Bedossa, P.; Paradis, V. Performance of Pivka-II for early hepatocellular carcinoma diagnosis and prediction of microvascular invasion. J. Hepatol. 2015, 62, 848–854. [Google Scholar] [CrossRef]
- Kudo, A.; Shinoda, M.; Ariizumi, S.; Kumamoto, T.; Katayama, M.; Otsubo, T.; Endo, I.; Kitagawa, Y.; Tanabe, M.; Yamamoto, M.; et al. Des-gamma-carboxy prothrombin affects the survival of HCC patients with marginal liver function and curative treatment: ACRoS1402. J. Cancer Res. Clin. Oncol. 2020, 146, 2949–2956. [Google Scholar] [CrossRef]
- Yamashita, T.; Wang, X.W. Cancer stem cells in the development of liver cancer. J. Clin. Invest. 2013, 123, 1911–1918. [Google Scholar] [CrossRef]
- Yamashita, T.; Kaneko, S. Orchestration of hepatocellular carcinoma development by diverse liver cancer stem cells. J. Gastroenterol. 2014, 49, 1105–1110. [Google Scholar] [CrossRef]
- Yamashita, T.; Kitao, A.; Matsui, O.; Hayashi, T.; Nio, K.; Kondo, M.; Ohno, N.; Miyati, T.; Okada, H.; Yamashita, T.; et al. Gd-EOB-DTPA-enhanced magnetic resonance imaging and alpha-fetoprotein predict prognosis of early-stage hepatocellular carcinoma. Hepatology 2014, 60, 1674–1685. [Google Scholar] [CrossRef]
- Zhang, R.; Lin, H.M.; Broering, R.; Shi, X.D.; Yu, X.H.; Xu, L.B.; Wu, W.R.; Liu, C. Dickkopf-1 contributes to hepatocellular carcinoma tumorigenesis by activating the Wnt/β-catenin signaling pathway. Signal Transduct. Target. Ther. 2019, 4, 54. [Google Scholar] [CrossRef]
- Kuang, H.B.; Miao, C.L.; Guo, W.X.; Peng, S.; Cao, Y.J.; Duan, E.K. Dickkopf-1 enhances migration of HEK293 cell by beta-catenin/E-cadherin degradation. Front. Biosci. (Landmark Ed). 2009, 14, 2212–2220. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Li, M.; Li, Q.; Wang, C.J.; Xie, S.Q. DKK1 promotes hepatocellular carcinoma cell migration and invasion through β-catenin/MMP7 signaling pathway. Mol. Cancer. 2013, 12, 157. [Google Scholar] [CrossRef] [Green Version]
- Glaw, J.T.; Skalak, T.C.; Peirce, S.M. Inhibition of canonical Wnt signaling increases microvascular hemorrhaging and venular remodeling in adult rats. Microcirculation 2010, 17, 348–357. [Google Scholar] [CrossRef] [Green Version]
- Tian, E.; Zhan, F.; Walker, R.; Rasmussen, E.; Ma, Y.; Barlogie, B.; Shaughnessy, J.D., Jr. The role of the Wnt-signaling antagonist DKK1 in the development of osteolytic lesions in multiple myeloma. N. Engl. J. Med. 2003, 349, 2483–2494. [Google Scholar] [CrossRef]
- Gavriatopoulou, M.; Dimopoulos, M.A.; Christoulas, D.; Migkou, M.; Iakovaki, M.; Gkotzamanidou, M.; Terpos, E. Dickkopf-1: A suitable target for the management of myeloma bone disease. Expert Opin. Ther. Targets 2009, 13, 839–848. [Google Scholar] [CrossRef]
- Huang, A.; Yang, X.R.; Chung, W.Y.; Dennison, A.R.; Zhou, J. Targeted therapy for hepatocellular carcinoma. Signal Transduct. Target. Ther. 2020, 5, 146. [Google Scholar] [CrossRef]
- Yamashita, T.; Honda, M.; Takatori, H.; Nishino, R.; Minato, H.; Takamura, H.; Ohta, T.; Kaneko, S. Activation of lipogenic pathway correlates with cell proliferation and poor prognosis in hepatocellular carcinoma. J. Hepatol. 2009, 50, 100–110. [Google Scholar] [CrossRef]
- Shimizu, M.; Saitoh, Y.; Itoh, H. Immunohistochemical staining of Ha-ras oncogene product in normal, benign, and malignant human pancreatic tissues. Hum. Pathol. 1990, 21, 607–612. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with HCC (n = 391) | |
|---|---|
| Age, years | 68 (61–74) |
| Sex, male, n (%) | 260 (66.5) |
| Etiology, HCV/HBV/HBV+HCV/Alcohol/Others, n (%) | 216 (55.5)/69 (17.6)/3 (0.8)/48 (12.3)/54 (13.8) |
| Child–Pugh, A/B+C, n (%) | 286 (73.1)/105 (26.9) |
| ALBI grade, 1/2a/2b/3, n (%) | 156 (39.9)/89 (22.8)/122 (31.2)/24 (6.1) |
| UICC (8th) stage, I/II/III/IV, n (%) | 164 (41.9)/131 (33.5)/63 (16.1)/33 (8.4) |
| BCLC stage, 0/A/B/C/D, n (%) | 54 (13.8)/149 (38.2)/109 (27.9)/59 (15.1)/19 (4.9) |
| Serum DKK-1 (pg/mL) | 330.8 (272.8–409.5) |
| Serum AFP (ng/mL) | 24.0 (10.0–200.0) |
| Serum PIVKA-II (mAU/mL) | 50.0 (23.0–74.0) |
| Patients without HCC (n = 205) | |
|---|---|
| Age, years | 58 (50–64) |
| Sex, male, n (%) | 114 (55.6) |
| Etiology, HCV/HBV/Alcohol/Others, n (%) | 131 (63.9)/40 (19.5)/6 (2.9)/28 (13.7) |
| Liver cirrhosis, n (%) | 28 (13.7) |
| Serum DKK-1 (pg/mL) | 253.8 (204.3–331.5) |
| Serum DKK-1 < 365.9 (n = 169) | Serum DKK-1 ≥ 365.9 (n = 102) | p | |
|---|---|---|---|
| Age, years | 65.0 (61.0–74.0) | 65.0 (58.0–74.0) | n.s. |
| Sex, male, n (%) | 106 (62.7) | 81 (79.4) | ** 0.007 |
| Etiology, HCV/HBV/HBV+HCV/Alcohol/Others, n (%) | 111 (65.7)/24 (14.2)/3 (1.8)/20 (11.8)/11 (6.5) | 37 (36.3)/28 (27.5)/0 (0.0)/16 (15.7)/21 (20.6) | *** < 0.001 |
| UICC (8th) stage, I/II/III/IV, n (%) | 75 (44.4)/64 (37.9)/24 (14.2)/6 (3.6) | 28 (27.5)/27 (26.5)/25 (24.5)/22 (21.6) | *** < 0.001 |
| BCLC stage, 0/A/B/C/D, n (%) | 26 (15.4)/71 (42.0)/46 (24.2)/17 (10.1)/9 (5.3) | 9 (8.8)/27 (26.5)/30 (29.4)/32 (31.4)/4 (3.9) | *** < 0.001 |
| Serum AFP (ng/mL) | 25.0 (11.0–170) | 49.1 (10.0–1918) | n.s. |
| Serum PIVKA-II (mAU/mL) | 40.0 (22.0–215) | 397.0 (36.3–8555) | *** < 0.001 |
| Univariate | HR (95% CI) | Multivariate | HR (95% CI) | |
|---|---|---|---|---|
| Sex | n.s. | — | ||
| Age ≥ 65 | n.s. | — | ||
| Etiology | n.s. | — | ||
| Child–Pugh (A/B+C) | *** < 0.001 | 2.08 (1.40–3.08) | n.s. | — |
| ALBI grade (1/2a/2b/3) | *** < 0.001 | 1.64 (1.34–2.00) | *** < 0.001 | 1.78 (1.45–2.17) |
| UICC (8th) stage (I/II/III/IV) | *** < 0.001 | 2.46 (2.02–3.00) | *** < 0.001 | 1.93 (1.55–2.40) |
| BCLC stage (0/A/B/C/D) | *** < 0.001 | 2.21 (1.76–2.49) | n.s. | — |
| DKK-1 (<365.9/≥365.9) | *** < 0.001 | 2.4 (1.64–3.54) | ** 0.0015 | 2.02 (1.31–3.12) |
| AFP (<400/≥400) | ** 0.0017 | 2.21 (1.46–3.35) | n.s. | — |
| PIVKA-II (<90/≥90) | *** < 0.001 | 3.76 (2.49–5.67) | *** < 0.001 | 2.59 (1.68–4.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suda, T.; Yamashita, T.; Sunagozaka, H.; Okada, H.; Nio, K.; Sakai, Y.; Yamashita, T.; Mizukoshi, E.; Honda, M.; Kaneko, S. Dickkopf-1 Promotes Angiogenesis and is a Biomarker for Hepatic Stem Cell-like Hepatocellular Carcinoma. Int. J. Mol. Sci. 2022, 23, 2801. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23052801
Suda T, Yamashita T, Sunagozaka H, Okada H, Nio K, Sakai Y, Yamashita T, Mizukoshi E, Honda M, Kaneko S. Dickkopf-1 Promotes Angiogenesis and is a Biomarker for Hepatic Stem Cell-like Hepatocellular Carcinoma. International Journal of Molecular Sciences. 2022; 23(5):2801. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23052801
Chicago/Turabian StyleSuda, Tsuyoshi, Taro Yamashita, Hajime Sunagozaka, Hikari Okada, Kouki Nio, Yoshio Sakai, Tatsuya Yamashita, Eishiro Mizukoshi, Masao Honda, and Shuichi Kaneko. 2022. "Dickkopf-1 Promotes Angiogenesis and is a Biomarker for Hepatic Stem Cell-like Hepatocellular Carcinoma" International Journal of Molecular Sciences 23, no. 5: 2801. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23052801