
Progress in Bioengineering Strategies for Heart Regenerative Medicine


1
Department of Cell and Molecular Biology, Karolinska Institutet, 171 77 Stockholm, Sweden
2
Department of Surgery, Yale University School of Medicine, New Haven, CN 06510, USA
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2022, 23(7), 3482; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23073482
Submission received: 27 February 2022
/
Revised: 20 March 2022
/
Accepted: 21 March 2022
/
Published: 23 March 2022
(This article belongs to the Special Issue Biomaterials and Regenerative Medicine)
Abstract
:The human heart has the least regenerative capabilities among tissues and organs, and heart disease continues to be a leading cause of mortality in the industrialized world with insufficient therapeutic options and poor prognosis. Therefore, developing new therapeutic strategies for heart regeneration is a major goal in modern cardiac biology and medicine. Recent advances in stem cell biology and biotechnologies such as human pluripotent stem cells (hPSCs) and cardiac tissue engineering hold great promise for opening novel paths to heart regeneration and repair for heart disease, although these areas are still in their infancy. In this review, we summarize and discuss the recent progress in cardiac tissue engineering strategies, highlighting stem cell engineering and cardiomyocyte maturation, development of novel functional biomaterials and biofabrication tools, and their therapeutic applications involving drug discovery, disease modeling, and regenerative medicine for heart disease.
1. Introduction
Heart disease is a leading cause of mortality worldwide and still continues to be subject to poor prognosis, irrespective of development in the current diagnosis and treatment strategies involving pharmacological therapy and revascularization interventions [1,2]. Among tissues and organs, the mammalian hearts have the least regenerative capabilities, most of which are lost after 10 years of age in humans [3]. Given the drastic shortage of donor hearts for transplantation, which is only the radical treatment for severe heart failure (HF), developing new therapeutic strategies for severe forms of heart disease is urgently required but remains elusive in modern cardiac biology and medicine [4]. In this regard, recent advances in stem cell biology and biotechnologies, such as human pluripotent stem cells (hPSCs) and cardiac tissue engineering, hold great promise for opening novel therapeutic paths to heart regeneration and repair for heart disease [5,6]. To date, however, the therapeutic effects by the cell-based therapies in the preclinical and/or clinical settings remain insufficient with only modest outcomes, likely due to the reason that the benefits by cell therapies are mainly derived from the paracrine factors that are released by transplanted cells but not from direct cell engraftment replacing damaged heart tissues. A majority of cells (≈95–99%) that are delivered to the injured hearts are lost within the first 24 h, owing to mechanical washout, death due to a hostile environment (i.e., poor oxygenation and low nutrients), and host immune reaction [7,8,9,10]. On the contrary, more recent studies have revealed that combining the cell-based therapy with bioengineering technology, which is represented by functional biomaterials and biofabrication tools, can promote the engraftment of transplanted cells, thereby leading to improved therapeutic effects, although these areas are still in their infancy [11,12]. In this review, we summarize the latest progress in cardiac tissue engineering strategies, highlighting stem cell engineering and cardiomyocyte maturation, development of novel functional biomaterials (e.g., hydrogels and decellularized scaffolds) and biofabrication tools (e.g., engineered heart tissues and bioprinting), and their therapeutic applications involving drug discovery, disease modeling, and regenerative medicine for heart disease. Finally, we discuss the current challenges and future perspectives of the cardiac tissue engineering technologies from the viewpoints of their clinical significance.
2. Stem Cell Engineering and Cardiomyocyte Maturation
2.1. Cell Sources for Cardiac Bioengineering
Both human embryonic stem cells (hESCs) and human induced pluripotent stem cells (hiPSCs), namely hPSCs, have their high self-renewal capacity and capability to differentiate into any cell type of the human body [13,14]. Using the established protocols to differentiate hPSCs highly efficiently into cardiomyocytes (CMs) [15,16], vascular endothelial cells (ECs) [17,18], and vascular smooth muscle cells (SMCs) [19,20], these cardiac cells forming the human heart can be generated and obtained almost unlimitedly in vitro. Therefore, exploiting hPSCs is an attractive approach for cardiac bioengineering, disease modeling (e.g., using patient-derived hiPSCs), and regenerative medicine [6,21,22,23].
Sophisticated differentiation protocols with modulation of the Wnt signaling pathway can generate hPSC-derived CMs (hPSC-CMs) with >90% purity and scaling up to 109 cells [15,16,24,25,26]. However, these hPSC-CMs are structurally, functionally, and transcriptionally more similar to fetal rather than adult CMs [27,28,29], which hampers the broad applications of these in vitro-generated CMs in the various settings. For instance, the electrical immaturity of hPSC-CMs might cause ventricular arrhythmias that appeared following cellular engraftment after cell transplantation in animal injured hearts [30,31]. Therefore, a wide variety of the maturation strategies for hPSC-CMs have been investigated and employed [32], as described in the following section. Although the immature characteristics of hPSC-CMs are usually considered as their major demerits, some properties of the immature hPSC-CMs might be still advantageous in a specific application, such as cell transplantation after cardiac injury for therapeutic regeneration. Reinecke et al. have reported that fetal and neonatal CMs could engraft in normal and injured myocardium in rat myocardial infarction (MI) models, while adult CMs could not survive nor engraft upon transplantation into the host myocardium [33], suggesting that fully mature CMs might not be suitable for the cell therapy application. Taken together, it is essential to determine the optimal state of cellular maturity for hPSC-CMs at the timing of cell transplantation into the damaged hearts, in order to obtain the best results for cell engraftment and heart regeneration.
The recent advanced studies such as single-cell/nuclei RNA sequencing analyses have revealed a cellular heterogeneity and molecular signatures in human fetal and adult hearts [34,35,36,37]. Notably, the cellular composition, including CMs, ECs, SMCs, fibroblasts and immune cells, and their transcriptional profiles are different depending on each of the anatomical regions across the heart, suggesting differential roles and functions of the various heart regions, such as cardiac outflow tract, atria, and the ventricular septum and free wall [36,37]. This complex heterogeneity in the in vivo heart cells may affect the future strategies in cardiac tissue engineering upon the selection and employment of the ideal cell populations among hPSC-CMs.
2.2. Cardiomyocyte Maturation Strategies
As noted above, a major obstacle for the use of hPSC-CMs in various applications is their immature characteristics with respect to their structural morphology (i.e., lacking a rod-like cell shape, less aligned sarcomeres, undeveloped myofibrils and T-tubules, no/less polyploidy or binucleation, no/less polarized intercalated discs, and a low density of mitochondria); contractile force (e.g., their negative force-frequency relationship [FFR]); metabolism (mainly employing anaerobic glycolysis, but not β-oxidation of fatty acids, as a major source of ATP production); cell cycle (active cycling and division); electrophysiology (e.g., less negative resting membrane potential, slower upstroke velocity, and a faster repolarization phase without a plateau phase); calcium handling (i.e., slower action potential propagation due to inefficient excitation-concentration coupling); and transcriptomic levels [27,28,29,32,38,39]. To overcome these immaturity issues and promote maturation in hPSC-CMs, various bioengineering strategies have been investigated and employed to date, and several effective approaches are briefly described below and listed in Table 1. These strategies involve mechanical loading and electrical stimulation, three-dimensional (3D) cultures including engineered heart tissues (EHTs) with a scaffold protein (e.g., a hydrogel, an extracellular matrix [ECM], etc.) or cardiac cellular aggregates (spheroids) without scaffold proteins, intercellular crosstalk via co-culturing with non-cardiac cells, metabolic and hormonal interventions, genetic regulation, and in vivo transplantation (Table 1).
hPSC-CMs are responsive to external stimuli such as mechanical force and electrical pacing, and in fact, these mechanical and electrical stimuli are demonstrated to promote functional and structural maturation of hPSC-CMs in vitro, respectively [40,41,44,45]. Further, a recent study has proven that hPSC-CMs, which were electrically- and mechanically-stimulated simultaneously in a combination with cyclic stretch and electrical pacing (from 2 to 6 Hz) for two weeks, resulted in the more matured CMs with adult-like characteristics, such as a broad network of T-tubules, a positive FFR, and enhanced responses to a β-adrenergic stimulator [42]. Nowadays, 3D culture systems, including EHTs and cardiac spheroids/organoids, are recognized as one of the most successful approaches to promote the maturation of hPSC-CMs in vitro [46,47,48,49], as described in the following sections. The presence of non-cardiac cells, such as vascular ECs and SMCs and fibroblasts (including epicardial cells) also promotes CM maturation via intercellular crosstalk and paracrine signals [55,56,57,58]. The co-culture and/or co-administration of hPSC-CMs with ECs, SMCs, and/or fibroblasts resulted in the more developed muscle constructs with enhanced CM maturity and improved an efficacy of CM engraftment upon transplantation into the host myocardium, compared to hPSC-CMs alone [52,53,54]. One of the main characteristics for CM maturation in vivo is a metabolic shift from glycolysis to β-oxidation of fatty acids, mirroring a morphological change to cellular hypertrophy and increased energetic demands [66]. In line with this notion, the modified culture medium with high fatty-acids and low glucose contents was proven to drive metabolic, functional, and structural maturation of hPSC-CMs in vitro [59,60]. Among the hormones whose levels in the body peak around the time of birth, a thyroid hormone tri-iodothyronine (T3) and a glucocorticoid hormone (e.g., dexamethasone) have been shown to improve the maturation of hPSC-CMs in vitro, respectively. When these two hormones were simultaneously applied to the cultured hPSC-CMs, they exerted further maturation of the CMs in a synergistic manner [61,62,63].
3. Development of Functional Biomaterials for Cardiac Tissue Engineering
Biomaterial-based strategies for tissue engineering have recently attracted much attention in cardiac biology and medicine, since they are known to be effective for not only promoting the maturation of hPSC-CMs in vitro but also improving the cardiac regenerative effects of cell-based and/or cell-free therapies against heart disease models in vivo [11,12]. Biomaterials, represented by hydrogels and decellularized scaffolds, have various advantages for regenerative therapies, including enhancing cell survival and cell retention/engraftment into the host tissue; promoting protective paracrine signaling responses by containing and releasing functional bioactive molecules such as angiogenic, anti-apoptotic, and/or immunomodulatory factors; and providing mechanical support for the damaged tissues [64,67,68]. Ideal biomaterials in tissue engineering are usually considered as being biocompatible, biodegradable, less immunogenic, and biomimetic products resembling properties of the target native tissue.
3.1. Hydrogels
Hydrogels are the most popular and widely used polymers among the various bioengineering materials [69,70]. They can absorb a high amount of water and biofluids, similar to human tissue, and be swollen maintaining their shapes until being degraded by hydrolysis [70,71]. Hydrogels also have several beneficial properties for the use in tissue engineering as follows: injectable fluid in a less invasive fashion [72], efficient transfer of oxygen and metabolites [73,74], ability to encapsulate cells and bioactive molecules [75], and providing casting molds of several geometries [40,76] and anchoring/mechanical support [42,77]. Three types of hydrogels, i.e., ones derived from either natural, synthetic, or hybrid biomaterials are known and used in a wide variety of applications in tissue engineering. Natural hydrogels include fibrin, collagen, gelatin, alginate, chitosan, hyaluronic acid, and elastin [78,79,80,81,82,83], while synthetic hydrogels include poly(ethylene glycol) (PEG), poly(lactic-co-glycolic acid) (PLGA), polycaprolactone (PCL), poly(N-isopropylacrylamide) (PNIPAAm), etc. [84,85,86,87]. Recently, hybrid hydrogels that contain the natural and synthetic biomaterials combined with covalent binding or crosslinking have been developed as an alternative option [88,89].
Early studies reported that acellular injectable hydrogels alone provided efficient mechanical support to the infarcted heart muscles and elicited therapeutic effects through attenuating pathological ventricular remodeling in small and large animal models [69,90,91,92]. Fibrin, a biodegradable coagulation-related protein, is a natural biomaterial that has been broadly used in cardiac tissue engineering [82,93,94,95]. Christman et al. demonstrated the therapeutic effects of fibrin glue as an acellular injectable biomaterial in rat MI models via mechanical support and induction of angiogenesis by recruiting ECs [94,96]. Fibrin gels/patches are also manufactured frequently encapsulating hPSC-CMs with or without other cell types, such as ECs and/or SMCs. For instance, the cardiac patches created from hiPSC-CMs and human pericytes entrapped in a fibrin gel reduced infarct sizes and improved cardiac function in a rat MI model, together with survived and proliferated human CMs and pericytes upon transplantation [95]. Another group reported that transplantation of insulin-like growth factor (IGF)-loaded 3D fibrin patches combined with hiPSC-CMs, hiPSC-ECs, and hiPSC-SMCs resulted in significant improvements in left ventricular function, infarct size, myocardial wall stress, and myocardial hypertrophy without inducing malignant arrhythmias in a porcine MI model [82,97]. Interestingly, in their system, the cell engraftment rate was relatively high (11 ± 2%) at four weeks after the transplantation, indicating the strong potential of the fibrin gels to promote transplanted cells’ survival and retention into the host environment.
Collagen is a natural fibrous protein that is abundant in the ECM and is also used widely in tissue engineering [81,98,99]. Engineered heart muscles that were generated by casting hESC-CMs with collagen in preformed molds successfully improved regional ventricular wall movement and preserved left ventricular (LV) systolic function upon transplantation into damaged rat hearts one month after ischemia reperfusion injury, which was measured with cardiac tagged magnetic resonance imaging [99].
Alginate, a natural linear polysaccharide that is derived from seaweed algae, has recently attracted much interest due to its ECM-like properties and biocompatibility. In fact, it has been used in various applications for tissue engineering [100,101]. Intramyocardial or intracoronary injection of alginate hydrogels was shown to be a feasible, safe, and effective acellular strategy that attenuated adverse cardiac remodeling and ventricular dysfunction in recent and late MI models in rats and pigs [102,103]. Further, a commercially available calcium alginate hydrogel (Algisyl-LVRTM) was tested for its ability to reduce LV wall stress and improve LV function in HF patients (ejection fraction [EF] <40%) that were undergoing coronary artery bypass grafting (CABG) [91]. This first-in-man pilot study also showed the clinical benefits such as decreased end-systolic volume and increased LV wall thickness and EF three months after treatment, moving forward into the randomized clinical trials, as described below.
Chitosan is another natural polysaccharide and recently it is often used in tissue engineering, since it has biocompatible and biodegradable natures, as well as anti-microbial and pro-angiogenic properties [104,105]. Chitosan thermosensitive hydrogels are liquid at 25 °C but gel at 37 °C. Importantly, intramyocardial injection of chitosan hydrogels could efficiently increase LV myocardial wall thickness, decrease infarct size, attenuate pathological LV remodeling, and preserve LV contractility in a rat MI model [106].
Synthetic hydrogels have also been examined for their tissue engineering properties and therapeutic potential in the forms of acellular or cell-containing injectable materials [84,85,86,87]. PEG is the most often used synthetic polymer in tissue engineering, due to its lower immunogenicity. In fact, PEG was shown to elicit ventricular protective effects and its functional improvement when injected as an acellular injectable material in rodent MI models [90,107,108]. Further, PEG hydrogels containing hiPSC-CMs and/or erythropoietin attenuated LV remodeling and improved LV function in a rat MI model, although no engrafted cells were detected, implying that the observed beneficial results were derived from paracrine effects that were induced by the injected cell/biomolecule-encapsulating PEG hydrogels [85].
Micro-grooved thin and biodegradable PLGA film (≈30 μm in thickness) with hPSC-CMs can be used for the construction of a biomimetic cardiac patch. Chen et al. demonstrated that this biomimetic cardiac patch showed steady-state contraction, easily developed under regular electrical stimuli, and recapitulated the anisotropic electrophysiological feature of native cardiac tissues, indicating the remarkable biocompatibility of PLGA [109]. As proved by the reduced incidence of arrhythmia, the micro-grooved PLGA film-derived cardiac patch was much more refractory to premature stimuli than the non-grooved PLGA film-derived patch, highlighting the therapeutic potential of this system for injured hearts. Another group has reported that multilayered hiPSC-CMs that were cultured and organized on aligned nanofibers made of PLGA polymer successfully engrafted into the damaged host hearts and improved the LV function four weeks after treatment in a rat MI model [110].
PNIPAAm is a thermosensitive polymer that holds its liquid state at room temperature and forms a gel at human body temperature [111]. The intramyocardial injection of biodegradable PNIPAAm-based hydrogels reduced collagen deposition, preserved LV wall thickness, and increased neovascularization in the injured heart environment, leading to the improvement of LV function in rat MI models [87,112]. Further, Navaei et al. reported that a biohybrid thermosensitive PNIPAAm-gelatin-based hydrogel promoted the survival and maturation of the encapsulated neonatal rat CMs that were co-cultured with cardiac fibroblasts (2:1 ratio) in vitro, as demonstrated by their superior structural organization, beating behavior, and cell-cell coupling [89]. As such, this study highlighted the well-organized bioactivity and mechanical robustness of the PNIPAAm-gelatin hybrid hydrogel system for cardiac tissue engineering.
Overall, various injectable hydrogels with or without containing cells to date have successfully treated the infarcted heart muscles by preventing pathological remodeling and preserving LV function in animal MI models. Further, because hydrogels can serve as a delivery vehicle to encapsulate the bioactive factors, the combination approach of injectable hydrogels with the delivery of biomolecules, such as angiogenic (e.g., vascular endothelial growth factor [VEGF], basic fibroblast growth factor [bFGF]) and anti-apoptotic/pro-proliferative (e.g., stromal cell-derived factor 1 [SDF-1], IGF-1, neuregulin-1β) factors holds great promise as an attractive strategy of the new bioengineering therapies [64,113]. Hydrogels can also be modified and functionalized with cell-responsive and cell-binding peptide sequences, such as the Arg-Gly-Asp (RGD), Arg-Gly-Asp-D-Phe-Lys (RGDFK), and Tyr-Ile-Gly-Ser-Arg (YIGSR) peptides, which are derived from ECM molecules including collagen, fibronectin, and laminin, and may thereby exert multiple bioactive responses [114,115,116,117].
Despite the benefits and promising results of the biomaterial-based hydrogel therapies for heart disease in preclinical models, a number of obstacles and limitations still hinder their clinical translation. One disadvantage of the biomaterials, in particular natural ones, is that they may retain some surface antigens to exert unignorable foreign body reaction in the host [64,118,119]. As controlling with this immune response is essential for successful functionality and sustainability of implanted hydrogels, there are a lot of attempts to develop biomaterials that can modulate these immunologic reactions, which involve functionalization with appropriate bioactive molecules of immunomodulatory factors (e.g., interleukin-10 [IL-10], tissue inhibitor of metalloproteinase-3 [TIMP-3]) [120,121,122]. Another concern when transplanting a hydrogel into the myocardial wall is its potential effect causing arrhythmias. In this regard, interestingly, Suarez et al. reported that a PEG-based highly spreading hydrogel with its slow gelation time did not cause any conduction abnormalities when it was injected into normal and infarcted rat hearts, while a hydrogel exhibiting minimal interstitial spread due to its quicker gelation time created a substrate for arrhythmia shortly after injection, indicating the site of delivery and interstitial spread characteristics as strong factors to predict possible arrhythmias after biomaterial therapies for damaged hearts [123]. This type of a validation study of biomaterials is important and needs to be repeated in large animal models for their further clinical translation. Other concerns around the use of biomaterial-based hydrogels include low availability of the required clinical-grade biomaterials, batch–batch variability, difficulty for sterilization and standardization operating procedures, and uncertainty of the optimal time window and delivery route. For a more in-depth review about this subject, we direct the readers to other reviews [67,124,125,126].
3.2. Decellularized Bioscaffolds
Another effective approach to generate bioscaffolds in cardiac tissue engineering is to obtain inherent ECM ultrastructure and composition directly from the native heart tissues by decellularizing and removing resident genetic materials in them [127,128]. Several protocols for decellularization are developed using physical, chemical, and/or enzymatic approaches, and among them, ionic and nonionic detergents such as sodium dodecyl sulfate (SDS) are commonly used for the decellularization of cardiac tissues [127,129,130]. In early studies, decellularized cardiac ECM hydrogels, that were specifically derived from porcine heart ventricles, were administered into infarcted rats and pigs via percutaneous trans-endocardial injections two weeks after MI [131,132]. These studies showed the decellularized ECM hydrogel therapy increased the endogenous CMs in the infarct areas and preserved LV function post-MI without inducing arrhythmias, highlighting the feasibility, safety, and efficacy of this novel treatment strategy for MI. Further, D’Amore et al. reported that a bi-layered polyurethane-decellularized ECM cardiac patch attenuated ischemic ventricular wall remodeling such as scar formation and LV wall thinning and dilation, along with promoting angiogenesis [133]. Interestingly, the ECM patch material promoted recruitment of the anti-inflammatory M2 macrophages into the ischemic border zones of the infarct heart muscles, rather than the proinflammatory M1 macrophages, possibly explaining the mechanism behind the observed beneficial effects in part. More recently, a decellularized porcine cardiac ECM scaffold was engineered with biodegradable PLGA microcarriers and human cardiac stromal cell-secreted factors [134]. This hybrid acellular cardiac patch maintained its properties after long-term cryopreservation and showed therapeutic regenerative effects by reducing scarring, promoting angiomyogenesis, and preserving LV function in rat and porcine MI models.
Compared to decellularization, i.e., removing all cellular materials in the native tissue, recellularization into the decellularized matrix remains challenging. In a recent study, for recellularization of a human heart, 500 million hiPSC-CMs were injected in a ≈5 cm3 volume of the LV free wall of a decellularized human heart [135]. This approach resulted in the survival of approximately half of the injected cells that formed an immature cardiac tissue in the matrix. Although the input cell density (100 million/cm3) was much higher than a normal CM density in the human heart (10–28 million/cm3) [3], these injected cells yielded only a small area of contracting tissue generating a pressure of <3 mm Hg [135], indicating the limitation of the current recellularization technology. Irrespectively, decellularized human cardiac ECM scaffolds also have another intractable issue, i.e., few opportunities to be used due to the shortage of donor organs.
4. Implementation of Biofabrication Tools for Cardiac Tissue Engineering
4.1. Microfabrication Technologies for Generating Engineered Heart Tissues
The hydrogel system (i.e., a water-swollen polymer network) is simple and the most used technology for generating EHTs, as noted above. Besides, a wide variety of other microfabrication technologies for EHTs, including cell sheets [136,137], muscle strips [40,43,45,76,138,139], cardiac patches [140,141], spheroids [50,51] and organoids [142,143,144], and electrospinning [145,146], have been developed and allowed more advanced cardiac bioengineering to resemble the in vivo native cardiac tissues (Figure 1).
Initial pioneering works showed that 3D reconstitution of embryonic chick [159] or neonatal rat [40] CMs in a collagen matrix generated the rod-type [159] or ring-shaped [40] EHTs that displayed more physiological and morphologically organized characteristics of intact differentiated heart tissues than monolayer cultures, serving as promising materials for in vitro assessments of cardiac function. Afterwards, the same and other groups further developed engineered cardiac microtissues on synthetic polymer polydimethylsiloxane (PDMS) racks [41] or on fluorescent pillars [160], highlighting the potential usefulness of these EHT models for various applications, such as in vitro drug screening and disease modeling. Another simple way of microfabrication is to pattern material substrates with biomimetic approaches, so that the cultured CMs are well organized and aligned. Feinberg et al. used PDMS thin films and assembled biohybrid materials by culturing neonatal rat CMs on the films that were micropatterned with alternating 20-μm-wide lines of a large amount of ECM proteins (fibronectin) [148]. This hybrid centimeter-scale construct improved the CM alignment and performed diverse biomimetic cardiac functions with fine spatial and temporal control, which served as a model for investigating the biomechanics and physiology of in vitro myocardial sheets. Ma et al. established more advanced culture systems, i.e., self-organizing human cardiac microchambers that were regulated by geometric cellular confinement [142]. They adopted PEG- and PDMS-patterned substrates to geometrically confine the hPSC colonies in circular chambers (200,400, and 600 μm in diameter), and provided cells with the biochemical and biophysical cues to induce self-organizing cardiac lineage specification and the creation of a beating human cardiac microchamber, which could be used to study early cardiac development and drug-induced developmental toxicity. Another good example of patterning culture chambers is the “BiowireTM” platforms, reported by Radisic’s group [45,151,152]. They combined 3D cell cultivation of hPSC-derived CMs and fibroblasts in hydrogel-coated microwells containing two flexible wires that were fabricated from a poly(octamethylene maleate (anhydride) citrate) (POMaC) polymer with electrical stimulation to mature hPSC-derived cardiac tissues. They demonstrated that the engineered platform markedly induced CM maturation, such as increased myofibril ultrastructural organization, elevated conduction velocity, and improved both electrophysiological and calcium handling properties when the cells were subjected to high-frequency electrical stimulation, compared to the non-stimulated or low frequency-stimulated controls. This platform has been further shown to be a suitable tool for studying in vitro drug testing and disease modeling of cardiac tissues [152].
With a sophisticated approach using engineered epicardial mimetics, Bian et al. developed a large 3D cardiac patch (2.5 cm × 2.5 cm) with human epicardial fiber orientations that were derived from diffusion tensor magnetic resonance imaging (DTMRI) maps of the human ventricle [140,150]. After three weeks in the culture of rat neonatal CMs on a PDMS mold with hexagonal posts corresponding to the designed porous photomask, they obtained the advanced structural and functional maturation of the engineered 3D cardiac tissues with CM alignment that replicated human epicardial fiber orientations. The same group also developed another versatile EHT, termed “cardiobundles”, on a PDMS frame, which was fabricated on dynamic, free-floating culture conditions with neonatal rat- or hPSC-CMs embedded in a fibrin-based hydrogel [43]. Notably, the cardiobundles showed a near-adult functional and structural characteristics without loading exogenous electrical or mechanical stimulation in vitro. Recently, the advanced microelectronic cardiac patch that integrated neonatal rat CMs with flexible, freestanding electronics and a 3D nanocomposite scaffold has been reported [147]. In the system, the electronic mesh device was designed to contain electrodes for the sensing of tissue electrical activities, which enabled it to provide online monitoring of tissue physiological functions, to stimulate cells and tissues electrically, and to also regulate the release of biomolecules in accordance with the tissue microenvironment. Thus, this complex cardiac patch that was integrated with microelectronics holds great promise for therapeutic monitoring and regulation of cardiac function on demand.
One of the key issues in cardiac tissue engineering is how to acquire and maintain the supply of oxygen and nutrients into the thick cardiac muscles. Recent development to resolve this issue is utilizing perfusable 3D microfluidics/microchannel devices, which are fabricated with human ECs and form the biomimetic microvasculature, functioning as engineered heart- or vasculature-on-a-chip [149,157]. The AngioChip platform has been shown to support the assembly of parenchymal cells on a mechanically-tunable matrix surrounding a perfusable and branched microchannel network, and to allow functional vascularization and perfusion through a maintained open-vessel lumen, generating both in vitro cardiac and hepatic tissue models with defined vasculature and in vivo cardiac tissue implants with direct surgical anastomosis in rat hindlimbs [149]. During the last decade, human heart organoids have attracted much attention as novel promising EHT models, although progress in this arena has been hampered and delayed significantly, compared to other organ organoid models [161,162,163]. Recent attempts have tackled this issue of the shortage of relevant heart-on-a-chip and/or heart organoid models, and thereafter, self-assembling organoid technologies have been established and become available for the heart [151,164,165,166]. For instance, Drakhlis et al. have reported hPSC-derived hybrid cardiac-foregut organoids, which resembled early native heart development before heart tube formation through an interaction with foregut endoderm tissues [143]. Interestingly, Hofbauer et al. have reported the self-organizing “cardioids” from hPSCs, which built chamber-like structures containing a cavity with isolated CM and EC layers and mimicked epicardial spreading, inward migration, and differentiation [144]. For a more in-depth review about the topics in regards to organ (heart)-on-a-chip and/or heart organoid models, we direct the readers to other reviews on these topics [151,164,165,166,167,168].
4.2. Bioprinting
The basic 3D scaffold fabrication techniques, such as hydrogels and decellularization, have been broadly used for tissue engineering of various organs, however, the construction of highly vascularized and dynamic organs such as heart is still challenging by using such conventional methodologies. Alternatively, 3D bioprinting is an emerging fabrication technique that creates biomimetic products with precise control over the positioning of living cells, biomaterials, and biomolecules, collectively termed bioinks [169,170]. In bioprinting of cardiac tissues, synthetic and/or natural materials, including collagen, gelatin, fibrin, alginate, hyaluronic acid, PCL, PLGA, and decellularized ECM scaffolds, are processed together with cardiac cells and/or biomolecules to pattern and recreate heart tissues precisely at high resolution (micro ~ nanoscale) with computer-aided designing modalities such as computer tomography and magnetic resonance imaging [68,154,171,172,173]. Based on the used technology, cost, speed, and resolution, there are different types to conduct the 3D bioprinting processes, namely inkjet, extrusion, laser-assisted, stereolithography, and droplet bioprinting, among which the extrusion bioprinting is the most frequently used approach to print cell-laden hydrogel-mixed cardiac tissues directly through a layer-by-layer deposition technique [68,169,171,174].
Using the extrusion-based multi-material bioprinting with flexible thermoplastic polyurethane (TPU) and conductive carbon black nanoparticles, Lind et al. manufactured a cardiac microphysiological device, in which soft strain gauge sensors were integrated within TPU microfilaments that guided the self-assembly and alignment of laminar cardiac tissues, providing non-invasive, electronic measurement of tissue contraction and an efficient platform to study drug responses [153]. Feinberg’s group developed an extrusion-based freeform printing methodology, termed “FRESH” (i.e., Freeform Reversible Embedding of Suspended Hydrogels), to bioprint collagen for engineering components of the human heart from multiscale vasculature and tri-leaflet heart valve to acellular neonatal-scale human heart (37 mm in diameter, 55 mm in height) [154,155]. In their system, controlling pH-driven gelation of collagen provided up to 10 μm resolution on printing, and hESC-CMs with cardiac fibroblasts (in a 49:1 ratio) could be embedded in the collagen and cellular bioinks. Importantly, using this approach, the authors also demonstrated successful 3D printing of a contractile human cardiac ventricle model (an ellipsoidal shell-shape; 6.6 mm in diameter, 8 mm in height). On the other hand, Gao et al. advanced a novel multiphoton-excited 3D printing technique to produce a native-like ECM scaffold with submicron resolution, in which multiple cell types including hiPSC-derived CMs, SMCs, and ECs (in a 2:1:1 ratio) could be seeded to generate a human cardiac muscle patch [79]. Notably, the engineered cardiac patch began producing calcium transients and beating synchronously within one day after seeding, and in vitro electrophysiological and contractile parameters of the patch were significantly developed and matured over the next seven days. The authors also showed the regenerative therapeutic potential of the engineered cardiac patch with successful cell engraftment when transplanted into damaged hearts in a murine MI model.
One of the advantages in the biofabrication by bioprinting is the high feasibility to create perfusable vasculature that is essential for successfully maintaining the structure and function of the engineered tissues and organs. Using a novel hybrid strategy with extrusion-based bioprinting, Zhang et al. engineered one of the first endothelialized myocardium that was capable of spontaneous and synchronous contraction through sequential steps, including bioprinting of a microfibrous scaffold encapsulating human ECs, formation of the vascular bed through EC migration, and seeding of human CMs onto a layer of endothelium [157]. The authors further embedded the organoids into a microfluidic perfusion device to successfully produce the heart (endothelialized myocardium)-on-a-chip platform for the purpose of testing cardiovascular toxicity. On the other hand, using a laser/visible light-assisted stereolithography technique that enables higher resolution bioprinting than extrusion-based methods, Grigoryan et al. manufactured high-fidelity multivascular networks within photopolymerizable hydrogels by using a new set of biocompatible photo-absorbers [156]. Although not in cardiac tissue engineering, they further showed the potential translational utility of their 3D-printed capillary vascular networks both in an engineered alveolar model and in a murine liver injury model. Another new biomanufacturing method that relied on sacrificial writing into functional tissue (SWIFT) has recently been reported by Skylar-Scott et al. [158]. They first assembled hundreds of thousands of hiPSC-derived organ building blocks (OBBs) in the forms of embryoid bodies, organoids, or multicellular spheroids, which were then placed into a mold and compacted via centrifugation to form a living OBB matrix, followed by quick patterning of a sacrificial ink within this matrix via embedded 3D bioprinting and induction of perfusable vascular channels after ink evacuation. As an interesting example, the authors created a perfusable cardiac tissue (top width, 6 mm; bottom width, 4.2 mm; depth, 4.2 mm; and height, 12 mm) that fused and beat synchronously over a seven-day period. More recently, Kupfer et al. have developed a photo-crosslinkable bioink formulation that is composed of ECM proteins and hiPSCs (instead of CMs), which were 3D-printed into complex geometries with a perfusable structure and, thereafter, enabled robust expansion and subsequent in situ differentiation of hiPSCs into electromechanically functional and chambered cardiac muscle organoids [175]. This method provides an advance in terms of in situ hPSC proliferation and differentiation at high density and a platform for achieving thick layers of contiguous cardiac muscles.
Overall, although fully functional whole organ (heart) reconstruction is not yet feasible, the bioprinting technologies are rapidly developing and continuously hold great promise now and in the future. However, several obstacles and limitations need to be addressed for further advancing this technology. First, similarly to hydrogels, there are issues in relation to foreign body reaction and arrhythmias upon transplantation of biofabricated/bioprinted constructs, which needs to be fully elucidated to ensure their functional and safe engraftment [176,177,178]. Second, vascularization as well as innervation of engineered/bioprinted tissues will be the key milestones for the generation of functionally engrafted constructs, however, only limited progress has been made in the design of innervation to date [179,180]. The development of an ideal bioink is essential to enhance the cell-cell and cell-biomaterial/environment interactions for obtaining increased sustainability of the bioprinted constructs. Printing speed also needs to be improved, since additive printing with a high level of detail requires a slow printing velocity, affecting the scalability of the current methods [181]. Other issues around the use of bioprinted constructs include the lack of standardized methods across these systems, the need of further improved image acquisition with high resolution, and costs. For a more in-depth review about bioprinting in cardiac tissue engineering, we direct the readers to other reviews [68,171,182,183].
5. Clinical Applications of Cardiac Tissue Engineering-Based Technologies
5.1. Drug Screening and Disease Modeling
The current hPSC and cardiac tissue engineering technologies can provide in vitro sophisticated 3D culture models of the human heart, which is more advanced resembling the native heart compared to the conventional 2D monolayer culture system. Therefore, in recent years, applications of these technologies have been widely expanded into generating various disease settings, in order to test drug effects to cardiac function and toxicity preclinically and to model cardiovascular diseases in combination with patient-derived hiPSCs.
Drug screening using hPSC-CMs is conducted to predict human cardiac responses against drugs and determine the potential functions of the drugs, such as proarrhythmic, (positive and negative) inotropic, and cardiotoxic effects [42,152,184,185]. For drug testing, animal models, primarily rodents, have been commonly used so far; however, that platform often failed to precisely predict the human drug responses due to differences in cardiac physiology and biology between rodents and humans (e.g., differential roles of the rapid delayed rectifier IKr, such as “no role” in rodents vs. “strongly functioning” in humans) [186,187]. Therefore, hPSC-derived EHTs or similar 3D constructs, such as spheroids/organoids, microtissues, and microfluidic devices (“heart-on-a-chip”), have been emerging as better solutions for more precise drug screening in the heart, overcoming the deficits in the traditional 2D in vitro culture platforms [51,76,160,188]. In fact, using these advanced 3D culture systems, several higher predictive insights have been shown with regard to inotropic effects (e.g., isoprenaline) [189,190,191], contractile function [185], conduction disturbance [42,152], IKr blockade [77], and multifaceted proarrhythmic effects [41]. Despite these promising outcomes, the cardiac tissue engineering-based drug screening approach is still in its infancy and needs to be further improved for their reliability, reproducibility, and robustness. For instance, considering the larger costs and time-consuming efforts with the specific and expensive equipment that is required in the 3D EHT culture platforms, direct comparisons of drug screening between 2D and the various 3D systems are necessary to obtain insights and fair judgements about the benefits, demerits, and cost-effectiveness in both methods [6,192]. Another concern is that the 3D EHT models are not appropriate for high-throughput drug screening, since their complexity and bigger size than the 2D system likely make it incompatible for rapid screening of compounds in large libraries [160,193,194].
The 3D EHT models combined with hPSC-CMs have also advanced cardiac disease modeling to understand disease-specific phenotypes. In addition to the use of patient-derived hiPSCs with known disease-causing gene mutations, the recent gene editing technology such as CRISPR-Cas9 has enabled the quick generation of genetically-modified hPSCs (wild-type hESC- or hiPSC-derived) harboring a specific mutation, which can be also applied to disease modeling [195,196]. Importantly, this technology can correct a disease-causing gene mutation in patient-derived cells and thereby generate an isogenic control that provides validity and robustness of the obtained findings [197,198]. The hPSC-CM and 3D EHT-combined platforms harboring disease-causing genetic mutations, including hypertrophic cardiomyopathy (HCM) [199], dilated cardiomyopathy (DCM) [200], and Barth syndrome with mitochondrial cardiomyopathy [198] have successfully modeled in vitro disease phenotypes such as abnormal contractile properties, which were in accordance with each of the clinical phenotypes. It is crucial to consider that these disease-carrying hPSC-CMs, as well as mutation-corrected isogenic control hPSC-CMs, that are used in the disease-modeling platforms are still immature and thus may not reflect the characteristics in adult diseased CMs. In fact, hiPSC-CMs harboring a mutation truncating the sarcomere protein titin (TTN), a known common cause of DCM, did not show any abnormal contractile function and were comparable with wild-type hiPSC-CMs in a 2D culture platform but exhibited significantly reduced contractility and decreased sarcomere length when fabricated in 3D constructs of self-assembling cardiac microtissues that worked against the elastic resistance between two PDMS pillars [200]. Another insightful example to apply the findings that were obtained from disease modeling with the hPSC-CM and 3D EHT-combined platforms is their clinical translation for patient treatment in a way of personalized medicine. More recently, Prondzynski et al. have reported that HCM patient (harboring a rare mutation in the α-actinin 2 [ACTN2] gene)-derived hiPSC-CMs and engineered 3D muscle strips recapitulated several hallmarks of HCM, such as myofibrillar disarray, hypercontractility, impaired relaxation, and prolonged action potential duration, and that an L-type calcium channel blocker diltiazem improved these disease-specific cardiac abnormalities more significantly in the HCM models than in an isogenic control in their systems (Figure 2) [201]. The authors further translated their findings to patient care and showed that diltiazem application ameliorated the prolonged QTc interval in the HCM-affected son and sister of the index patient after one month treatment, providing a proof of concept for the use of the hPSC-CM and 3D EHT-combined platforms for personalized treatment of cardiomyopathies.
These personalized approaches are promising but at the same time, require a great amount of efforts and elevated costs. Thus, it is important to verify whether the larger costs and efforts in a personalized treatment approach compared to conventional approaches are outweighed by better sensitivity, specificity, robustness, and thereby outcomes.
5.2. Heart Regenerative Therapy
One of the most promising applications in cardiac tissue engineering is to use the technologies for therapeutic purposes such as regeneration and repair of the diseased hearts. Firstly, cell-based therapies for heart regeneration using i.e., bone marrow-derived mononuclear cells, mesenchymal stem cells, cardiac progenitor cells, or hPSC-CMs, have been developed and applied in the preclinical and clinical studies during the last two to three decades [9,203,204,205,206]; however, the therapeutic effects of these approaches are still undetermined and under debate. For a more in-depth review about cell therapies for heart regeneration, including the latest hPSC-CM strategies [30,31,207,208], we direct the readers to other reviews [5,22,209,210,211].
The main common bottleneck in cell-based approaches for heart regeneration is the low engraftment and survival rate of the transplanted cells in the host heart, which results in the fact that the transplanted cells cannot engraft into or replace the damaged cardiac tissues in a functionally sufficient manner [7,8,9,10,212]. In this regard, the recent advanced cardiac tissue engineering technologies are generating a lot of attention since they have been shown to attenuate pathological ventricular remodeling after heart injury, and when combined with cell therapies, to promote engraftment of the transplanted cells in the host tissue, leading to improvement of the LV function of the damaged hearts [6,11,12,23]. The main devices that are used for regenerative tissue-engineering purposes to date are hydrogel/ECM-based constructs (epicardial patches, or in situ gelling systems via intramyocardial or intracoronary injections), engineered muscle strips (applied on epicardium), and cell sheets (applied on epicardium) [81,132,137,213,214,215]. Related cardiac regenerative bioengineering studies in the preclinical settings using animal models are already described in the above sections and also highlighted in Table 2. Overall, these regenerative tissue-engineering approaches have showed the beneficial outcomes, including higher percentages of cell retention and improved ventricular morphology and function, when applied into infarcted or defected hearts in small and large animal models [82,97,139,213,214,215,216], and therefore, hold great promise for future heart regenerative medicine. However, several important issues, involving induction of arrhythmias due to inadequate electric coupling to the host myocardium, potential tumorigenicity when combined with hPSC-based cell therapies, long-term safety, adverse host immune responses attacking the cells and/or materials that are employed in the bioengineered constructs, and the side effects that are derived from the accompanied long-term immunosuppressive therapies, need to be addressed for further applying these technologies to the clinical settings [208,217,218,219,220].
Nonetheless, after obtaining promising results in preclinical settings, several cardiac bioengineering-based therapies have been and are being tested for their safety, feasibility, and (preliminary) efficacy in clinical settings (Table 2). The first-in-man clinically prospective randomized trials evaluating the therapeutic effects of acellular alginate-based hydrogels to the damaged hearts in patients with ischemic or nonischemic HF were PRESERVATION I [221,222,223] and AUGMENT-HF [224,225,226]. In these trials, the alginate-based hydrogels were administered via intracoronary (PRESERVATION I) or intramyocardial (AUGMENT-HF) injections in patients with acute ST-segment elevation MI two to five days after successful primary percutaneous coronary intervention (PRESERVATION I) or in patients with advanced chronic HF (57% ischemic and 43% nonischemic; AUGMENT-HF). Despite prior expectations, these approaches could not attenuate pathological LV remodeling or improve the LV function with only minor improvements in symptoms and clinical status, compared to the control [223,226], suggesting that a cell-free strategy may possibly have limitations and be insufficient to effectively regenerate and repair damaged hearts in humans. Focusing on the restoration of ECM homeostasis and structure in the heart environment, other clinical trials evaluating the therapeutic effects of ECM epicardial patches (CorMatrixTM-ECM; porcine small intestinal submucosa-derived) [227,228,229] or cardiac ECM hydrogels (VentriGel; decellularized porcine myocardium-derived) [230] to the recent or late infarcted hearts have recently been completed. The former was delivered on epicardium in patients that were undergoing CABG surgery within six weeks after acute MI as an adjunct therapy to surgical revascularization. The latter was delivered via intramyocardial (transendocardial) injections using the NOGA-MyoStar catheter system [234] in patients with LV dysfunction, who had experienced a first, large ST-segment elevation MI that was treated by percutaneous coronary intervention in the past 60-day to three-year window. The results for these studies have not yet been published to date, and therefore are awaited.
The first clinical application of cardiac bioengineered constructs containing hPSC-derived cells, namely clinical-grade hESC-derived CD15 (SSEA-1)+ISL-1+ cardiac progenitors that were embedded into a fibrin patch, has been employed during concomitant CABG or mitral valve surgery for the treatment of patients with severe ischemic HF (LV EF ≤ 35%) due to a history of MI (older than six months) [231,232]. The transplantation procedures of the progenitor cell-fibrin hybrid epicardial patches were all safely conducted in six patients with no adverse complications in the follow-up periods (a median of 18 months), i.e., no detection of tumors such as teratomas, no occurrence of arrhythmias, and no major alloimmunization events even if the immunosuppressive therapy was ceased one month after the surgery [232]. Although no significantly beneficial results with regard to efficacy such as LV EF were achieved, the symptoms in all of the hybrid patch-transplanted patients were improved along with an increased systolic motion of the treated heart segments, indicating that this cell-fibrin hybrid patch would be a promising strategy as a novel alternative therapy for ischemic heart disease. Other active and recently recruiting clinical trials will evaluate the efficacies of hiPSC-derived engineered heart muscle (EHM) for advanced HF (LV EF ≤ 35%) (NCT04396899) and hiPSC-CM sheets for ischemic cardiomyopathy (NCT04696328). The EHM in the former trial is constructed from hiPSC-derived CMs and stromal cells that are embedded into a bovine collagen type I hydrogel, aiming the myocardial remuscularization and the improvement of ventricular wall motion upon transplantation. The latter trial is based on promising results in the preclinical studies showing that allogenic transplantation of induced pluripotent stem cell-derived CM sheets improved cardiac function and remodeling with a concomitant immunosuppressive therapy in non-human primate MI models [217,233].
Collectively, the positive outcomes that were obtained in these clinical trials have been marginal or elusive to date, and therefore, development of the cardiac tissue engineering-based regenerative therapies is still in its infancy. Further advanced technologies and a better understanding of the underlying mechanisms through which these applied biomaterials and tools can elicit their cardiac regenerative properties would pave the way towards more improved bioengineering therapies for heart regeneration and repair.
6. Future Perspectives of Cardiac Tissue Engineering
Cardiac tissue engineering is a remarkably developing research field year by year, in particular during the last decade, enabling the generation of constructs that resemble the human native heart. As described above, it holds great potential for applications in drug screening, disease modeling, and heart regenerative therapies towards personalized medicine. For instance, using the combined technologies of advanced 3D bioprinting with hybrid material bioinks, high-resolution cardiac imaging modalities, and developed computational image processing, several universities and hospitals have already demonstrated patient-specific models of various cardiovascular diseases and pathologies [235,236]. Although such personalized bioengineering technologies and medicine are expected to become reality in the near future, continuous efforts are needed to assure the accuracy, relevance, reproducibility, and robustness in these engineered technologies and constructs. Since the cardiac tissue engineering field holds interdisciplinary aspects, the clinical translation and medical application of the engineered heart tissues will require tight collaborations across many disciplines, involving stem cell biology, material science, biofabrication technology, cardiovascular medicine, and also business administration [67,68,237].
One of the keys for generation and engraftment of the engineered functional cardiac tissues is to create perfusable vasculature that is accompanied with heart muscles. Scaling up the engineered constructs to human-sized tissues is also an essential milestone for success in cardiac bioengineering medicine. For efficient vascularization and scalability, as well as the modulation of the host immune response and attenuation of pathological ventricular remodeling, developing well-controlled biomolecule release systems via biomaterials is likely to provide a promising solution. For those purposes, using the novel delivery systems with e.g., chemically-modified mRNA [238,239,240] or exosome such as extracellular vesicles [241,242,243] may offer an alternative option, which will need to be proven by further investigation.
In conclusion, the state-of-the-art cardiac tissue engineering technologies hold unlimited potential and their broad applications to drug screening, cardiovascular disease modeling, and heart regenerative medicine. Although the clinical-grade effects of the technologies to remuscularize failing hearts and to improve the cardiac function and survival in patients with severe HF are still uncertain, the advanced cardiac bioengineering technologies definitely not only provide novel insights in cardiac biology and medicine but will open new therapeutic paths of regeneration and repair for heart disease on the horizon.
Author Contributions
T.H. and M.S. conducted careful reading of references, writing of a manuscript, drawing of figures, and reviewing and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by research grants to M.S. from: the Swedish Research Council (Dnr: 2019-01359); the Swedish Heart and Lung Foundation (20190380); and the SFO StratRegen in Karolinska Institutet.
Acknowledgments
We would like to be grateful to Department of Cell and Molecular Biology (CMB) and Karolinska Institutet for their constant support.
Conflicts of Interest
The authors declare that they have no conflict of interest in relation to this work.
References
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Zhang, Q.; Much, A.A.; Maor, E.; Segev, A.; Beinart, R.; Adawi, S.; Lu, Y.; Bragazzi, N.L.; Wu, J. Global, regional, and national prevalence, incidence, mortality, and risk factors for atrial fibrillation, 1990–2017: Results from the Global Burden of Disease Study 2017. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, O.; Zdunek, S.; Felker, A.; Salehpour, M.; Alkass, K.; Bernard, S.; Sjostrom, S.L.; Szewczykowska, M.; Jackowska, T.; Dos Remedios, C.; et al. Dynamics of cell generation and turnover in the human heart. Cell 2015, 161, 1566–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tajabadi, M.; Goran Orimi, H.; Ramzgouyan, M.R.; Nemati, A.; Deravi, N.; Beheshtizadeh, N.; Azami, M. Regenerative strategies for the consequences of myocardial infarction: Chronological indication and upcoming visions. Biomed. Pharmacother. 2022, 146, 112584. [Google Scholar] [CrossRef] [PubMed]
- Witman, N.; Zhou, C.; Beverborg, N.G.; Sahara, M.; Chien, K.R. Cardiac progenitors and paracrine mediators in cardiogenesis and heart regeneration. Semin. Cell Dev. Biol. 2020, 100, 29–51. [Google Scholar] [CrossRef] [PubMed]
- Florian, W.; Ingra, M.; Thomas, E. Engineering cardiac muscle tissue: A maturating field of research. Circ. Res. 2017, 120, 1487–1500. [Google Scholar]
- Sheikh, A.Y.; Lin, S.A.; Cao, F.; Cao, Y.; van der Bogt, K.E.; Chu, P.; Chang, C.P.; Contag, C.H.; Robbins, R.C.; Wu, J.C. Molecular imaging of bone marrow mononuclear cell homing and engraftment in ischemic myocardium. Stem Cells 2007, 25, 2677–2684. [Google Scholar] [CrossRef] [Green Version]
- van den Akker, F.; Feyen, D.A.; van den Hoogen, P.; van Laake, L.W.; van Eeuwijk, E.C.; Hoefer, I.; Pasterkamp, G.; Chamuleau, S.A.; Grundeman, P.F.; Doevendans, P.A.; et al. Intramyocardial stem cell injection: Go(ne) with the flow. Eur. Heart J. 2017, 38, 184–186. [Google Scholar] [CrossRef] [Green Version]
- Madonna, R.; Van Laake, L.W.; Davidson, S.M.; Engel, F.B.; Hausenloy, D.J.; Lecour, S.; Leor, J.; Perrino, C.; Schulz, R.; Ytrehus, K.; et al. Position paper of the european society of cardiology working group cellular biology of the heart: Cell-based therapies for myocardial repair and regeneration in ischemic heart disease and heart failure. Eur. Heart J. 2016, 37, 1789–1798. [Google Scholar] [CrossRef]
- Gaetani, R.; Rizzitelli, G.; Chimenti, I.; Barile, L.; Forte, E.; Ionta, V.; Angelini, F.; Sluijter, J.P.; Barbetta, A.; Messina, E.; et al. Cardiospheres and tissue engineering for myocardial regeneration: Potential for clinical application. J. Cell Mol. Med. 2010, 14, 1071–1077. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.G.; Kwon, Y.W.; Lee, T.W.; Park, G.T.; Kim, J.H. Recent advances in stem cell therapeutics and tissue engineering strategies. Biomater. Res. 2018, 22, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, J.L.; Zhu, W.; Tang, Y.L.; Krishnamurthy, P.; Ge, Y.; Cooke, J.P.; Chen, Y.; Garry, D.J.; Yang, H.T.; Rajasekaran, N.S.; et al. Convergences of life sciences and engineering in understanding and treating heart failure. Circ. Res. 2019, 124, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Thomson, J.A.; Itskovitz-Eldor, J.; Shapiro, S.S.; Waknitz, M.A.; Swiergiel, J.J.; Marshall, V.S.; Jones, J.M. Embryonic stem cell lines derived from human blastocysts. Science 1998, 282, 1145–1147. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burridge, P.W.; Matsa, E.; Shukla, P.; Lin, Z.C.; Churko, J.M.; Ebert, A.D.; Lan, F.; Diecke, S.; Huber, B.; Mordwinkin, N.M.; et al. Chemically defined generation of human cardiomyocytes. Nat. Methods 2014, 11, 855–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, X.; Zhang, J.; Azarin, S.M.; Zhu, K.; Hazeltine, L.B.; Bao, X.; Hsiao, C.; Kamp, T.J.; Palecek, S.P. Directed cardiomyocyte differentiation from human pluripotent stem cells by modulating Wnt/β-catenin signaling under fully defined conditions. Nat. Protoc. 2013, 8, 162–175. [Google Scholar] [CrossRef] [Green Version]
- James, D.; Nam, H.S.; Seandel, M.; Nolan, D.; Janovitz, T.; Tomishima, M.; Studer, L.; Lee, G.; Lyden, D.; Benezra, R.; et al. Expansion and maintenance of human embryonic stem cell-derived endothelial cells by TGFbeta inhibition is Id1 dependent. Nat. Biotechnol. 2010, 28, 161–166. [Google Scholar] [CrossRef]
- Sahara, M.; Hansson, E.M.; Wernet, O.; Lui, K.O.; Später, D.; Chien, K.R. Manipulation of a VEGF-Notch signaling circuit drives formation of functional vascular endothelial progenitors from human pluripotent stem cells. Cell Res. 2014, 24, 820–841. [Google Scholar] [CrossRef] [Green Version]
- Patsch, C.; Challet-Meylan, L.; Thoma, E.C.; Urich, E.; Heckel, T.; O’Sullivan, J.F.; Grainger, S.J.; Kapp, F.G.; Sun, L.; Christensen, K.; et al. Generation of vascular endothelial and smooth muscle cells from human pluripotent stem cells. Nat. Cell Biol. 2015, 17, 994–1003. [Google Scholar] [CrossRef]
- Gong, J.; Zhou, D.; Jiang, L.; Qiu, P.; Milewicz, D.M.; Chen, Y.E.; Yang, B. In vitro lineage-specific differentiation of vascular smooth muscle cells in response to SMAD3 deficiency: Implications for SMAD3-related thoracic aortic aneurysm. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1651–1663. [Google Scholar] [CrossRef]
- Chen, I.Y.; Matsa, E.; Wu, J.C. Induced pluripotent stem cells: At the heart of cardiovascular precision medicine. Nat. Rev. Cardiol. 2016, 13, 333–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahara, M.; Santoro, F.; Chien, K.R. Programming and reprogramming a human heart cell. EMBO J. 2015, 34, 710–738. [Google Scholar] [CrossRef] [PubMed]
- Tenreiro, M.F.; Louro, A.F.; Alves, P.M.; Serra, M. Next generation of heart regenerative therapies: Progress and promise of cardiac tissue engineering. NPJ Regen. Med. 2021, 6, 30. [Google Scholar] [CrossRef] [PubMed]
- Palpant, N.J.; Pabon, L.; Friedman, C.E.; Roberts, M.; Hadland, B.; Zaunbrecher, R.J.; Bernstein, I.; Zheng, Y.; Murry, C.E. Generating high-purity cardiac and endothelial derivatives from patterned mesoderm using human pluripotent stem cells. Nat. Protoc. 2017, 12, 15–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, V.C.; Ye, J.; Shukla, P.; Hua, G.; Chen, D.; Lin, Z.; Liu, J.C.; Chai, J.; Gold, J.; Wu, J.; et al. Development of a scalable suspension culture for cardiac differentiation from human pluripotent stem cells. Stem Cell Res. 2015, 15, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Santoro, F.; Chien, K.R.; Sahara, M. Isolation of human ESC-derived cardiac derivatives and embryonic heart cells for population and single-cell RNA-seq analysis. STAR Protoc. 2021, 2, 100339. [Google Scholar] [CrossRef]
- Yang, X.; Pabon, L.; Murry, C.E. Engineering adolescence: Maturation of human pluripotent stem cell-derived cardiomyocytes. Circ. Res. 2014, 114, 511–523. [Google Scholar] [CrossRef] [Green Version]
- Veerman, C.C.; Kosmidis, G.; Mummery, C.L.; Casini, S.; Verkerk, A.O.; Bellin, M. Immaturity of human stem-cell-derived cardiomyocytes in culture: Fatal flaw or soluble problem? Stem Cells Dev. 2015, 24, 1035–1052. [Google Scholar] [CrossRef] [Green Version]
- Zuppinger, C.; Gibbons, G.; Dutta-Passecker, P.; Segiser, A.; Most, H.; Suter, T.M. Characterization of cytoskeleton features and maturation status of cultured human iPSC-derived cardiomyocytes. Eur. J. Histochem. 2017, 61, 2763. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.W.; Chen, B.; Yang, X.; Fugate, J.A.; Kalucki, F.A.; Futakuchi-Tsuchida, A.; Couture, L.; Vogel, K.W.; Astley, C.A.; Baldessari, A.; et al. Human embryonic stem cell-derived cardiomyocytes restore function in infarcted hearts of non-human primates. Nat. Biotechnol. 2018, 36, 597–605. [Google Scholar] [CrossRef]
- Romagnuolo, R.; Masoudpour, H.; Porta-Sánchez, A.; Qiang, B.; Barry, J.; Laskary, A.; Qi, X.; Massé, S.; Magtibay, K.; Kawajiri, H.; et al. Human embryonic stem cell-derived cardiomyocytes regenerate the infarcted pig heart but induce ventricular tachyarrhythmias. Stem Cell Rep. 2019, 12, 967–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karbassi, E.; Fenix, A.; Marchiano, S.; Muraoka, N.; Nakamura, K.; Yang, X.; Murry, C.E. Cardiomyocyte maturation: Advances in knowledge and implications for regenerative medicine. Nat. Rev. Cardiol. 2020, 17, 341–359. [Google Scholar] [CrossRef] [PubMed]
- Reinecke, H.; Zhang, M.; Bartosek, T.; Murry, C.E. Survival, integration, and differentiation of cardiomyocyte grafts: A study in normal and injured rat hearts. Circulation 1999, 100, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Soysa, T.Y.; Ranade, S.S.; Okawa, S.; Ravichandran, S.; Huang, Y.; Salunga, H.T.; Schricker, A.; Del Sol, A.; Gifford, C.A.; Srivastava, D. Single-cell analysis of cardiogenesis reveals basis for organ-level developmental defects. Nature 2019, 572, 120–124. [Google Scholar] [CrossRef]
- Cui, Y.; Zheng, Y.; Liu, X.; Yan, L.; Fan, X.; Yong, J.; Hu, Y.; Dong, J.; Li, Q.; Wu, X.; et al. Single-cell transcriptome analysis maps the developmental track of the human heart. Cell Rep. 2019, 26, 1934–1950.e5. [Google Scholar] [CrossRef] [Green Version]
- Litviňuková, M.; Talavera-López, C.; Maatz, H.; Reichart, D.; Worth, C.L.; Lindberg, E.L.; Kanda, M.; Polanski, K.; Heinig, M.; Lee, M.; et al. Cells of the adult human heart. Nature 2020, 588, 466–472. [Google Scholar] [CrossRef]
- Sahara, M.; Santoro, F.; Sohlmér, J.; Zhou, C.; Witman, N.; Leung, C.Y.; Mononen, M.; Bylund, K.; Gruber, P.; Chien, K.R. Population and single-cell analysis of human cardiogenesis reveals unique LGR5 ventricular progenitors in embryonic outflow tract. Dev. Cell 2019, 48, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Feric, N.T.; Radisic, M. Maturing human pluripotent stem cell-derived cardiomyocytes in human engineered cardiac tissues. Adv. Drug Deliv. Rev. 2016, 96, 110–134. [Google Scholar] [CrossRef] [Green Version]
- Lundy, S.D.; Zhu, W.Z.; Regnier, M.; Laflamme, M.A. Structural and functional maturation of cardiomyocytes derived from human pluripotent stem cells. Stem Cells Dev. 2013, 22, 1991–2002. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, W.H.; Schneiderbanger, K.; Schubert, P.; Didié, M.; Münzel, F.; Heubach, J.F.; Kostin, S.; Neuhuber, W.L.; Eschenhagen, T. Tissue engineering of a differentiated cardiac muscle construct. Circ. Res. 2002, 90, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.; Eder, A.; Bönstrup, M.; Flato, M.; Mewe, M.; Schaaf, S.; Aksehirlioglu, B.; Schwoerer, A.P.; Uebeler, J.; Eschenhagen, T. Development of a drug screening platform based on engineered heart tissue. Circ. Res. 2010, 107, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronaldson-Bouchard, K.; Ma, S.P.; Yeager, K.; Chen, T.; Song, L.; Sirabella, D.; Morikawa, K.; Teles, D.; Yazawa, M.; Vunjak-Novakovic, G. Advanced maturation of human cardiac tissue grown from pluripotent stem cells. Nature 2018, 556, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Jackman, C.P.; Carlson, A.L.; Bursac, N. Dynamic culture yields engineered myocardium with near-adult functional output. Biomaterials 2016, 111, 66–79. [Google Scholar] [CrossRef] [Green Version]
- Kroll, K.; Chabria, M.; Wang, K.; Häusermann, F.; Schuler, F.; Polonchuk, L. Electro-mechanical conditioning of human iPSC-derived cardiomyocytes for translational research. Prog. Biophys. Mol. Biol. 2017, 130, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Nunes, S.S.; Miklas, J.W.; Liu, J.; Aschar-Sobbi, R.; Xiao, Y.; Zhang, B.; Jiang, J.; Massé, S.; Gagliardi, M.; Hsieh, A.; et al. Biowire: A platform for maturation of human pluripotent stem cell-derived cardiomyocytes. Nat. Methods 2013, 10, 781–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Shadrin, I.Y.; Lam, J.; Xian, H.Q.; Snodgrass, H.R.; Bursac, N. Tissue-engineered cardiac patch for advanced functional maturation of human ESC-derived cardiomyocytes. Biomaterials 2013, 34, 5813–5820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirt, M.N.; Hansen, A.; Eschenhagen, T. Cardiac tissue engineering: State of the art. Circ. Res. 2014, 114, 354–367. [Google Scholar] [CrossRef] [Green Version]
- Tiburcy, M.; Hudson, J.E.; Balfanz, P.; Schlick, S.; Meyer, T.; Chang Liao, M.L.; Levent, E.; Raad, F.; Zeidler, S.; Wingender, E.; et al. Defined Engineered human myocardium with advanced maturation for applications in heart failure modeling and repair. Circulation 2017, 135, 1832–1847. [Google Scholar] [CrossRef]
- Ulmer, B.M.; Stoehr, A.; Schulze, M.L.; Patel, S.; Gucek, M.; Mannhardt, I.; Funcke, S.; Murphy, E.; Eschenhagen, T.; Hansen, A. Contractile work contributes to maturation of energy metabolism in hiPSC-derived cardiomyocytes. Stem Cell Rep. 2018, 10, 834–847. [Google Scholar] [CrossRef] [Green Version]
- Frey, O.; Misun, P.M.; Fluri, D.A.; Hengstler, J.G.; Hierlemann, A. Reconfigurable microfluidic hanging drop network for multi-tissue interaction and analysis. Nat. Commun. 2014, 5, 4250. [Google Scholar] [CrossRef] [Green Version]
- Correia, C.; Koshkin, A.; Duarte, P.; Hu, D.; Carido, M.; Sebastião, M.J.; Gomes-Alves, P.; Elliott, D.A.; Domian, I.J.; Teixeira, A.P.; et al. 3D aggregate culture improves metabolic maturation of human pluripotent stem cell derived cardiomyocytes. Biotechnol. Bioeng. 2018, 115, 630–644. [Google Scholar] [CrossRef] [PubMed]
- Abecasis, B.; Gomes-Alves, P.; Rosa, S.; Gouveia, P.J.; Ferreira, L.; Serra, M.; Alves, P.M. Unveiling the molecular crosstalk in a human induced pluripotent stem cell-derived cardiac model. Biotechnol. Bioeng. 2019, 116, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Dunn, K.K.; Reichardt, I.M.; Simmons, A.D.; Jin, G.; Floy, M.E.; Hoon, K.M.; Palecek, S.P. Coculture of endothelial cells with human pluripotent stem cell-derived cardiac progenitors reveals a differentiation stage-specific enhancement of cardiomyocyte maturation. Biotechnol. J. 2019, 14, e1800725. [Google Scholar] [CrossRef]
- Bargehr, J.; Ong, L.P.; Colzani, M.; Davaapil, H.; Hofsteen, P.; Bhandari, S.; Gambardella, L.; Le Novère, N.; Iyer, D.; Sampaziotis, F.; et al. Epicardial cells derived from human embryonic stem cells augment cardiomyocyte-driven heart regeneration. Nat. Biotechnol. 2019, 37, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Brutsaert, D.L. Cardiac endothelial-myocardial signaling: Its role in cardiac growth, contractile performance, and rhythmicity. Physiol. Rev. 2003, 83, 59–115. [Google Scholar] [CrossRef] [PubMed]
- Tirziu, D.; Giordano, F.J.; Simons, M. Cell communications in the heart. Circulation 2010, 122, 928–937. [Google Scholar] [CrossRef] [Green Version]
- Pinto, A.R.; Ilinykh, A.; Ivey, M.J.; Kuwabara, J.T.; D’Antoni, M.L.; Debuque, R.; Chandran, A.; Wang, L.; Arora, K.; Rosenthal, N.A.; et al. Revisiting cardiac cellular composition. Circ. Res. 2016, 118, 400–409. [Google Scholar] [CrossRef] [Green Version]
- Fountoulaki, K.; Dagres, N.; Iliodromitis, E.K. Cellular communications in the heart. Card. Fail. Rev. 2015, 1, 64–68. [Google Scholar] [CrossRef]
- Hu, D.; Linders, A.; Yamak, A.; Correia, C.; Kijlstra, J.D.; Garakani, A.; Xiao, L.; Milan, D.J.; van der Meer, P.; Serra, M.; et al. Metabolic maturation of human pluripotent stem cell-derived cardiomyocytes by inhibition of HIF1α and LDHA. Circ. Res. 2018, 123, 1066–1079. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Rodriguez, M.L.; Leonard, A.; Sun, L.; Fischer, K.A.; Wang, Y.; Ritterhoff, J.; Zhao, L.; Kolwicz, S.C., Jr.; Pabon, L.; et al. Fatty acids enhance the maturation of cardiomyocytes derived from human pluripotent stem cells. Stem Cell Rep. 2019, 13, 657–668. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Rodriguez, M.; Pabon, L.; Fischer, K.A.; Reinecke, H.; Regnier, M.; Sniadecki, N.J.; Ruohola-Baker, H.; Murry, C.E. Tri-iodo-l-thyronine promotes the maturation of human cardiomyocytes-derived from induced pluripotent stem cells. J. Mol. Cell Cardiol. 2014, 72, 296–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Iismaa, S.E.; Naqvi, N.; Nicks, A.; Husain, A.; Graham, R.M. Thyroid hormone action in postnatal heart development. Stem Cell Res. 2014, 13, 582–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rog-Zielinska, E.A.; Thomson, A.; Kenyon, C.J.; Brownstein, D.G.; Moran, C.M.; Szumska, D.; Michailidou, Z.; Richardson, J.; Owen, E.; Watt, A.; et al. Glucocorticoid receptor is required for foetal heart maturation. Hum. Mol. Genet. 2013, 22, 3269–3282. [Google Scholar] [CrossRef] [Green Version]
- Ferrini, A.; Stevens, M.M.; Sattler, S.; Rosenthal, N. Toward regeneration of the heart: Bioengineering strategies for immunomodulation. Front. Cardiovasc. Med. 2019, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Garcia, M.J.; Quesnel, E.; Al-Attar, R.; Laskary, A.R.; Laflamme, M.A. Maturation of human pluripotent stem cell derived cardiomyocytes in vitro and in vivo. Semin. Cell Dev. Biol. 2021, 118, 163–171. [Google Scholar] [CrossRef]
- Chung, S.; Dzeja, P.P.; Faustino, R.S.; Perez-Terzic, C.; Behfar, A.; Terzic, A. Mitochondrial oxidative metabolism is required for the cardiac differentiation of stem cells. Nat. Clin. Pract. Cardiovasc. Med. 2007, 4, S60–S67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, A.; Zamani, M.; Huang, N.F. Extracellular matrix-based biomaterials for cardiovascular tissue engineering. J. Cardiovasc. Dev. Dis. 2021, 8, 137. [Google Scholar] [CrossRef]
- Moroni, L.; Burdick, J.A.; Highley, C.; Lee, S.J.; Morimoto, Y.; Takeuchi, S.; Yoo, J.J. Biofabrication strategies for 3D in vitro models and regenerative medicine. Nat. Rev. Mater. 2018, 3, 21–37. [Google Scholar] [CrossRef]
- Tous, E.; Purcell, B.; Ifkovits, J.L.; Burdick, J.A. Injectable acellular hydrogels for cardiac repair. J. Cardiovasc. Transl. Res. 2011, 4, 528–542. [Google Scholar] [CrossRef]
- Hasan, A.; Khattab, A.; Islam, M.A.; Hweij, K.A.; Zeitouny, J.; Waters, R.; Sayegh, M.; Hossain, M.M.; Paul, A. Injectable hydrogels for cardiac tissue repair after myocardial infarction. Adv. Sci. 2015, 2, 1500122. [Google Scholar] [CrossRef]
- Ye, Z.; Zhou, Y.; Cai, H.; Tan, W. Myocardial regeneration: Roles of stem cells and hydrogels. Adv. Drug Deliv. Rev. 2011, 63, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.D.; Christman, K.L. Injectable hydrogel therapies and their delivery strategies for treating myocardial infarction. Expert Opin. Drug Deliv. 2013, 10, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, B.V.; Khurshid, S.S.; Fisher, O.Z.; Khademhosseini, A.; Peppas, N.A. Hydrogels in regenerative medicine. Adv. Mater. 2009, 21, 3307–3329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malda, J.; Visser, J.; Melchels, F.P.; Jüngst, T.; Hennink, W.E.; Dhert, W.J.; Groll, J.; Hutmacher, D.W. 25th anniversary article: Engineering hydrogels for biofabrication. Adv. Mater. 2013, 25, 5011–5028. [Google Scholar] [CrossRef]
- Lee, S.; Serpooshan, V.; Tong, X.; Venkatraman, S.; Lee, M.; Lee, J.; Chirikian, O.; Wu, J.C.; Wu, S.M.; Yang, F. Contractile force generation by 3D hiPSC-derived cardiac tissues is enhanced by rapid establishment of cellular interconnection in matrix with muscle-mimicking stiffness. Biomaterials 2017, 131, 111–120. [Google Scholar] [CrossRef]
- Huebsch, N.; Loskill, P.; Deveshwar, N.; Spencer, C.I.; Judge, L.M.; Mandegar, M.A.; Fox, C.B.; Mohamed, T.M.; Ma, Z.; Mathur, A.; et al. Miniaturized iPS-cell-derived cardiac muscles for physiologically relevant drug response analyses. Sci. Rep. 2016, 6, 24726. [Google Scholar] [CrossRef] [Green Version]
- Mannhardt, I.; Breckwoldt, K.; Letuffe-Brenière, D.; Schaaf, S.; Schulz, H.; Neuber, C.; Benzin, A.; Werner, T.; Eder, A.; Schulze, T.; et al. Human engineered heart tissue: Analysis of contractile force. Stem Cell Rep. 2016, 7, 29–42. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Jha, A.K.; Harrington, D.A.; Farach-Carson, M.C.; Jia, X. Hyaluronic acid-based hydrogels: From a natural polysaccharide to complex networks. Soft Matter. 2012, 8, 3280–3294. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Kupfer, M.E.; Jung, J.P.; Yang, L.; Zhang, P.; Da Sie, Y.; Tran, Q.; Ajeti, V.; Freeman, B.T.; Fast, V.G.; et al. Myocardial tissue engineering with cells derived from human-induced pluripotent stem cells and a native-like, high-resolution, 3-dimensionally printed scaffold. Circ. Res. 2017, 120, 1318–1325. [Google Scholar] [CrossRef] [Green Version]
- Neves, M.I.; Moroni, L.; Barrias, C.C. Modulating alginate hydrogels for improved biological performance as cellular 3D microenvironments. Front. Bioeng. Biotechnol. 2020, 8, 665. [Google Scholar] [CrossRef]
- Riegler, J.; Tiburcy, M.; Ebert, A.; Tzatzalos, E.; Raaz, U.; Abilez, O.J.; Shen, Q.; Kooreman, N.G.; Neofytou, E.; Chen, V.C.; et al. Human engineered heart muscles engraft and survive long term in a rodent myocardial infarction model. Circ. Res. 2015, 117, 720–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, L.; Chang, Y.H.; Xiong, Q.; Zhang, P.; Zhang, L.; Somasundaram, P.; Lepley, M.; Swingen, C.; Su, L.; Wendel, J.S.; et al. Cardiac repair in a porcine model of acute myocardial infarction with human induced pluripotent stem cell-derived cardiovascular cells. Cell Stem Cell 2014, 15, 750–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemenschneider, S.B.; Mattia, D.J.; Wendel, J.S.; Schaefer, J.A.; Ye, L.; Guzman, P.A.; Tranquillo, R.T. Inosculation and perfusion of pre-vascularized tissue patches containing aligned human microvessels after myocardial infarction. Biomaterials 2016, 97, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.; Tian, S.; Zhao, C.; Chen, X.; Lei, I.; Wang, Z.; Ma, P.X. Porous nanofibrous poly(L-lactic acid) scaffolds supporting cardiovascular progenitor cells for cardiac tissue engineering. Acta. Biomater. 2015, 26, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Chow, A.; Stuckey, D.J.; Kidher, E.; Rocco, M.; Jabbour, R.J.; Mansfield, C.A.; Darzi, A.; Harding, S.E.; Stevens, M.M.; Athanasiou, T. Human induced pluripotent stem cell-derived cardiomyocyte encapsulating bioactive hydrogels improve rat heart function post myocardial infarction. Stem Cell Rep. 2017, 9, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Song, S.Y.; Kim, H.; Yoo, J.; Kwon, S.P.; Park, B.W.; Kim, J.J.; Ban, K.; Char, K.; Park, H.J.; Kim, B.S. Prevascularized, multiple-layered cell sheets of direct cardiac reprogrammed cells for cardiac repair. Biomater. Sci. 2020, 8, 4508–4520. [Google Scholar] [CrossRef]
- Ren, S.; Jiang, X.; Li, Z.; Wen, Y.; Chen, D.; Li, X.; Zhang, X.; Zhuo, R.; Chu, H. Physical properties of poly(N-isopropylacrylamide) hydrogel promote its effects on cardiac protection after myocardial infarction. J. Int. Med. Res. 2012, 40, 2167–2182. [Google Scholar] [CrossRef]
- Vasile, C.; Pamfil, D.; Stoleru, E.; Baican, M. New developments in medical applications of hybrid hydrogels containing natural polymers. Molecules 2020, 25, 1539. [Google Scholar] [CrossRef] [Green Version]
- Navaei, A.; Truong, D.; Heffernan, J.; Cutts, J.; Brafman, D.; Sirianni, R.W.; Vernon, B.; Nikkhah, M. PNIPAAm-based biohybrid injectable hydrogel for cardiac tissue engineering. Acta Biomater. 2016, 32, 10–23. [Google Scholar] [CrossRef]
- Jiang, X.J.; Wang, T.; Li, X.Y.; Wu, D.Q.; Zheng, Z.B.; Zhang, J.F.; Chen, J.L.; Peng, B.; Jiang, H.; Huang, C.; et al. Injection of a novel synthetic hydrogel preserves left ventricle function after myocardial infarction. J. Biomed. Mater. Res. A 2009, 90, 472–477. [Google Scholar] [CrossRef]
- Lee, L.C.; Wall, S.T.; Klepach, D.; Ge, L.; Zhang, Z.; Lee, R.J.; Hinson, A.; Gorman, J.H., 3rd; Gorman, R.C.; Guccione, J.M. Algisyl-LVR™ with coronary artery bypass grafting reduces left ventricular wall stress and improves function in the failing human heart. Int. J. Cardiol. 2013, 168, 2022–2028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, L.C.; Zhihong, Z.; Hinson, A.; Guccione, J.M. Reduction in left ventricular wall stress and improvement in function in failing hearts using Algisyl-LVR. J. Vis. Exp. 2013, 74, 50096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, F.M.; Callanan, A.; Kavanagh, E.G.; Burke, P.E.; Grace, P.A.; McGloughlin, T.M. Fibrin: A natural biodegradable scaffold in vascular tissue engineering. Cells Tissues Organs 2008, 188, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Christman, K.L.; Vardanian, A.J.; Fang, Q.; Sievers, R.E.; Fok, H.H.; Lee, R.J. Injectable fibrin scaffold improves cell transplant survival, reduces infarct expansion, and induces neovasculature formation in ischemic myocardium. J. Am. Coll. Cardiol. 2004, 44, 654–660. [Google Scholar] [CrossRef] [Green Version]
- Wendel, J.S.; Ye, L.; Tao, R.; Zhang, J.; Zhang, J.; Kamp, T.J.; Tranquillo, R.T. Functional effects of a tissue-engineered cardiac patch from human induced pluripotent stem cell-derived cardiomyocytes in a rat infarct model. Stem Cells Transl. Med. 2015, 4, 1324–1332. [Google Scholar] [CrossRef]
- Christman, K.L.; Fok, H.H.; Sievers, R.E.; Fang, Q.; Lee, R.J. Fibrin glue alone and skeletal myoblasts in a fibrin scaffold preserve cardiac function after myocardial infarction. Tissue Eng. 2004, 10, 403–409. [Google Scholar] [CrossRef]
- Gao, L.; Gregorich, Z.R.; Zhu, W.; Mattapally, S.; Oduk, Y.; Lou, X.; Kannappan, R.; Borovjagin, A.V.; Walcott, G.P.; Pollard, A.E.; et al. Large cardiac muscle patches engineered from human induced-pluripotent stem cell-derived cardiac cells improve recovery from myocardial infarction in Swine. Circulation 2018, 137, 1712–1730. [Google Scholar] [CrossRef]
- Edalat, S.G.; Jang, Y.; Kim, J.; Park, Y. Collagen type I containing hybrid hydrogel enhances cardiomyocyte maturation in a 3D cardiac model. Polymers 2019, 11, 687. [Google Scholar] [CrossRef] [Green Version]
- Qin, X.; Riegler, J.; Tiburcy, M.; Zhao, X.; Chour, T.; Ndoye, B.; Nguyen, M.; Adams, J.; Ameen, M.; Denney, T.S., Jr.; et al. Magnetic resonance imaging of cardiac strain pattern following transplantation of human tissue engineered heart muscles. Circ. Cardiovasc. Imaging 2016, 9, e004731. [Google Scholar] [CrossRef] [Green Version]
- Rowley, J.A.; Madlambayan, G.; Mooney, D.J. Alginate hydrogels as synthetic extracellular matrix materials. Biomaterials 1999, 20, 45–53. [Google Scholar] [CrossRef]
- Burdick, J.A.; Mauck, R.L.; Gerecht, S. To serve and protect: Hydrogels to improve stem cell-based therapies. Cell Stem Cell 2016, 18, 13–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landa, N.; Miller, L.; Feinberg, M.S.; Holbova, R.; Shachar, M.; Freeman, I.; Cohen, S.; Leor, J. Effect of injectable alginate implant on cardiac remodeling and function after recent and old infarcts in rat. Circulation 2008, 117, 1388–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leor, J.; Tuvia, S.; Guetta, V.; Manczur, F.; Castel, D.; Willenz, U.; Petneházy, O.; Landa, N.; Feinberg, M.S.; Konen, E.; et al. Intracoronary injection of in situ forming alginate hydrogel reverses left ventricular remodeling after myocardial infarction in Swine. J. Am. Coll. Cardiol. 2009, 54, 1014–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Rodrigues, J.; Tomás, H. Injectable and biodegradable hydrogels: Gelation, biodegradation and biomedical applications. Chem. Soc. Rev. 2012, 41, 2193–2221. [Google Scholar] [CrossRef] [PubMed]
- Deng, C.; Zhang, P.; Vulesevic, B.; Kuraitis, D.; Li, F.; Yang, A.F.; Griffith, M.; Ruel, M.; Suuronen, E.J. A collagen–chitosan hydrogel for endothelial differentiation and angiogenesis. Tissue Eng. Part A 2010, 16, 3099–3109. [Google Scholar] [CrossRef]
- Henning, R.J.; Khan, A.; Jimenez, E. Chitosan hydrogels significantly limit left ventricular infarction and remodeling and preserve myocardial contractility. J. Surg. Res. 2016, 201, 490–497. [Google Scholar] [CrossRef]
- Wang, T.; Wu, D.Q.; Jiang, X.J.; Zhang, X.Z.; Li, X.Y.; Zhang, J.F.; Zheng, Z.B.; Zhuo, R.; Jiang, H.; Huang, C. Novel thermosensitive hydrogel injection inhibits post-infarct ventricle remodelling. Eur. J. Heart Fail. 2009, 11, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Dobner, S.; Bezuidenhout, D.; Govender, P.; Zilla, P.; Davies, N. A synthetic non-degradable polyethylene glycol hydrogel retards adverse post-infarct left ventricular remodeling. J. Card. Fail. 2009, 15, 629–636. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, J.; Shen, B.; Chan, C.W.; Wang, C.; Zhao, Y.; Chan, H.N.; Tian, Q.; Chen, Y.; Yao, C.; et al. Engineering a freestanding biomimetic cardiac patch using biodegradable poly(lactic-co-glycolic acid) (PLGA) and human embryonic stem cell-derived ventricular cardiomyocytes (hESC-VCMs). Macromol. Biosci. 2015, 15, 426–436. [Google Scholar] [CrossRef]
- Li, J.; Minami, I.; Shiozaki, M.; Yu, L.; Yajima, S.; Miyagawa, S.; Shiba, Y.; Morone, N.; Fukushima, S.; Yoshioka, M.; et al. Human pluripotent stem cell-derived cardiac tissue-like constructs for repairing the infarcted myocardium. Stem Cell Rep. 2017, 9, 1546–1559. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Liu, Y.; Fu, W.; Yao, M.; Ding, Z.; Xuan, J.; Li, D.; Wang, S.; Xia, Y.; Cao, M. Poly(N-isopropylacrylamide)-Based thermoresponsive composite hydrogels for biomedical applications. Polymers 2020, 12, 580. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, K.L.; Ma, Z.; Nelson, D.M.; Hashizume, R.; Guan, J.; Tobita, K.; Wagner, W.R. Synthesis, characterization and therapeutic efficacy of a biodegradable, thermoresponsive hydrogel designed for application in chronic infarcted myocardium. Biomaterials 2009, 30, 4357–4368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebouças, J.S.; Santos-Magalhães, N.S.; Formiga, F.R. Cardiac regeneration using growth factors: Advances and challenges. Arq. Bras. Cardiol. 2016, 107, 271–275. [Google Scholar] [CrossRef]
- Shachar, M.; Tsur-Gang, O.; Dvir, T.; Leor, J.; Cohen, S. The effect of immobilized RGD peptide in alginate scaffolds on cardiac tissue engineering. Acta. Biomater. 2011, 7, 152–162. [Google Scholar] [CrossRef]
- Sondermeijer, H.P.; Witkowski, P.; Seki, T.; van der Laarse, A.; Itescu, S.; Hardy, M.A. RGDfK-peptide modified alginate scaffold for cell transplantation and cardiac neovascularization. Tissue Eng. Part A 2018, 24, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Boateng, S.Y.; Lateef, S.S.; Mosley, W.; Hartman, T.J.; Hanley, L.; Russell, B. RGD and YIGSR synthetic peptides facilitate cellular adhesion identical to that of laminin and fibronectin but alter the physiology of neonatal cardiac myocytes. Am. J. Physiol. Cell Physiol. 2005, 288, C30–C38. [Google Scholar] [CrossRef] [PubMed]
- Schussler, O.; Coirault, C.; Louis-Tisserand, M.; Al-Chare, W.; Oliviero, P.; Menard, C.; Michelot, R.; Bochet, P.; Salomon, D.R.; Chachques, J.C.; et al. Use of arginine-glycine-aspartic acid adhesion peptides coupled with a new collagen scaffold to engineer a myocardium-like tissue graft. Nat. Clin. Pract. Cardiovasc. Med. 2009, 6, 240–249. [Google Scholar] [CrossRef]
- Kuraitis, D.; Hosoyama, K.; Blackburn, N.J.R.; Deng, C.; Zhong, Z.; Suuronen, E.J. Functionalization of soft materials for cardiac repair and regeneration. Crit. Rev. Biotechnol. 2019, 39, 451–468. [Google Scholar] [CrossRef]
- Lutolf, M.P.; Gilbert, P.M.; Blau, H.M. Designing materials to direct stem-cell fate. Nature 2009, 462, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.C.; Lee, B.G.; Park, D.W.; Kim, K.; Chu, H.; Kim, K.; Huard, J.; Wang, Y. Controlled dual delivery of fibroblast growth factor-2 and Interleukin-10 by heparin-based coacervate synergistically enhances ischemic heart repair. Biomaterials 2015, 72, 138–151. [Google Scholar] [CrossRef] [Green Version]
- Turner, N.A.; Porter, K.E. Function and fate of myofibroblasts after myocardial infarction. Fibrogenesis Tissue Repair 2013, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julier, Z.; Park, A.J.; Briquez, P.S.; Martino, M.M. Promoting tissue regeneration by modulating the immune system. Acta. Biomater. 2017, 53, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Suarez, S.L.; Rane, A.A.; Muñoz, A.; Wright, A.T.; Zhang, S.X.; Braden, R.L.; Almutairi, A.; McCulloch, A.D.; Christman, K.L. Intramyocardial injection of hydrogel with high interstitial spread does not impact action potential propagation. Acta. Biomater. 2015, 26, 13–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.; Matsumura, Y.; Wagner, W.R. Ventricular wall biomaterial injection therapy after myocardial infarction: Advances in material design, mechanistic insight and early clinical experiences. Biomaterials 2017, 129, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Das, D.; Noh, I. Overviews of biomimetic medical materials. Adv. Exp. Med. Biol. 2018, 1064, 3–24. [Google Scholar]
- Perea-Gil, I.; Prat-Vidal, C.; Bayes-Genis, A. In vivo experience with natural scaffolds for myocardial infarction: The times they are a-changin. Stem Cell Res. Ther. 2015, 6, 248. [Google Scholar] [CrossRef] [Green Version]
- Ott, H.C.; Matthiesen, T.S.; Goh, S.K.; Black, L.D.; Kren, S.M.; Netoff, T.I.; Taylor, D.A. Perfusion-decellularized matrix: Using nature’s platform to engineer a bioartificial heart. Nat. Med. 2008, 14, 213–221. [Google Scholar] [CrossRef]
- Lee, P.F.; Chau, E.; Cabello, R.; Yeh, A.T.; Sampaio, L.C.; Gobin, A.S.; Taylor, D.A. Inverted orientation improves decellularization of whole porcine hearts. Acta. Biomater. 2017, 49, 181–191. [Google Scholar] [CrossRef]
- Gilbert, T.W.; Sellaro, T.L.; Badylak, S.F. Decellularization of tissues and organs. Biomaterials 2006, 27, 3675–3683. [Google Scholar] [CrossRef]
- Crapo, P.M.; Gilbert, T.W.; Badylak, S.F. An overview of tissue and whole organ decellularization processes. Biomaterials 2011, 32, 3233–3243. [Google Scholar] [CrossRef] [Green Version]
- Singelyn, J.M.; Sundaramurthy, P.; Johnson, T.D.; Schup-Magoffin, P.J.; Hu, D.P.; Faulk, D.M.; Wang, J.; Mayle, K.M.; Bartels, K.; Salvatore, M.; et al. Catheter-deliverable hydrogel derived from decellularized ventricular extracellular matrix increases endogenous cardiomyocytes and preserves cardiac function post-myocardial infarction. J. Am. Coll. Cardiol. 2012, 59, 751–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seif-Naraghi, S.B.; Singelyn, J.M.; Salvatore, M.A.; Osborn, K.G.; Wang, J.J.; Sampat, U.; Kwan, O.L.; Strachan, G.M.; Wong, J.; Schup-Magoffin, P.J.; et al. Safety and efficacy of an injectable extracellular matrix hydrogel for treating myocardial infarction. Sci. Transl. Med. 2013, 5, 173ra25. [Google Scholar] [CrossRef] [Green Version]
- D’Amore, A.; Yoshizumi, T.; Luketich, S.K.; Wolf, M.T.; Gu, X.; Cammarata, M.; Hoff, R.; Badylak, S.F.; Wagner, W.R. Bi-layered polyurethane—Extracellular matrix cardiac patch improves ischemic ventricular wall remodeling in a rat model. Biomaterials 2016, 107, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Ozpinar, E.W.; Su, T.; Tang, J.; Shen, D.; Qiao, L.; Hu, S.; Li, Z.; Liang, H.; Mathews, K.; et al. An off-the-shelf artificial cardiac patch improves cardiac repair after myocardial infarction in rats and pigs. Sci. Transl. Med. 2020, 12, eaat9683. [Google Scholar] [CrossRef] [PubMed]
- Guyette, J.P.; Charest, J.M.; Mills, R.W.; Jank, B.J.; Moser, P.T.; Gilpin, S.E.; Gershlak, J.R.; Okamoto, T.; Gonzalez, G.; Milan, D.J.; et al. Bioengineering human myocardium on native extracellular matrix. Circ. Res. 2016, 118, 56–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, T.; Yamato, M.; Isoi, Y.; Akutsu, T.; Setomaru, T.; Abe, K.; Kikuchi, A.; Umezu, M.; Okano, T. Fabrication of pulsatile cardiac tissue grafts using a novel 3-dimensional cell sheet manipulation technique and temperature-responsive cell culture surfaces. Circ. Res. 2002, 90, e40. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, M.; Miyagawa, S.; Miki, K.; Saito, A.; Fukushima, S.; Higuchi, T.; Kawamura, T.; Kuratani, T.; Daimon, T.; Shimizu, T.; et al. Feasibility, safety, and therapeutic efficacy of human induced pluripotent stem cell-derived cardiomyocyte sheets in a porcine ischemic cardiomyopathy model. Circulation 2012, 126, S29–S37. [Google Scholar] [CrossRef] [Green Version]
- Goldfracht, I.; Efraim, Y.; Shinnawi, R.; Kovalev, E.; Huber, I.; Gepstein, A.; Arbel, G.; Shaheen, N.; Tiburcy, M.; Zimmermann, W.H.; et al. Engineered heart tissue models from hiPSC-derived cardiomyocytes and cardiac ECM for disease modeling and drug testing applications. Acta Biomater. 2019, 92, 145–159. [Google Scholar] [CrossRef]
- Weinberger, F.; Breckwoldt, K.; Pecha, S.; Kelly, A.; Geertz, B.; Starbatty, J.; Yorgan, T.; Cheng, K.H.; Lessmann, K.; Stolen, T.; et al. Cardiac repair in guinea pigs with human engineered heart tissue from induced pluripotent stem cells. Sci. Transl. Med. 2016, 8, 363ra148. [Google Scholar] [CrossRef]
- Bian, W.; Badie, N.; Himel, H.D., 4th; Bursac, N. Robust T-tubulation and maturation of cardiomyocytes using tissue-engineered epicardial mimetics. Biomaterials 2014, 35, 3819–3828. [Google Scholar] [CrossRef] [Green Version]
- Shadrin, I.Y.; Allen, B.W.; Qian, Y.; Jackman, C.P.; Carlson, A.L.; Juhas, M.E.; Bursac, N. Cardiopatch platform enables maturation and scale-up of human pluripotent stem cell-derived engineered heart tissues. Nat. Commun. 2017, 8, 1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Z.; Wang, J.; Loskill, P.; Huebsch, N.; Koo, S.; Svedlund, F.L.; Marks, N.C.; Hua, E.W.; Grigoropoulos, C.P.; Conklin, B.R.; et al. Self-organizing human cardiac microchambers mediated by geometric confinement. Nat. Commun. 2015, 6, 7413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drakhlis, L.; Biswanath, S.; Farr, C.M.; Lupanow, V.; Teske, J.; Ritzenhoff, K.; Franke, A.; Manstein, F.; Bolesani, E.; Kempf, H.; et al. Human heart-forming organoids recapitulate early heart and foregut development. Nat. Biotechnol. 2021, 39, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Hofbauer, P.; Jahnel, S.M.; Papai, N.; Giesshammer, M.; Deyett, A.; Schmidt, C.; Penc, M.; Tavernini, K.; Grdseloff, N.; Meledeth, C.; et al. Cardioids reveal self-organizing principles of human cardiogenesis. Cell 2021, 184, 3299–3317. [Google Scholar] [CrossRef]
- MacQueen, L.A.; Sheehy, S.P.; Chantre, C.O.; Zimmerman, J.F.; Pasqualini, F.S.; Liu, X.; Goss, J.A.; Campbell, P.H.; Gonzalez, G.M.; Park, S.J.; et al. A tissue-engineered scale model of the heart ventricle. Nat. Biomed. Eng. 2018, 2, 930–941. [Google Scholar] [CrossRef]
- Gouveia, P.J.; Rosa, S.; Ricotti, L.; Abecasis, B.; Almeida, H.V.; Monteiro, L.; Nunes, J.; Carvalho, F.S.; Serra, M.; Luchkin, S.; et al. Flexible nanofilms coated with aligned piezoelectric microfibers preserve the contractility of cardiomyocytes. Biomaterials 2017, 139, 213–228. [Google Scholar] [CrossRef]
- Feiner, R.; Engel, L.; Fleischer, S.; Malki, M.; Gal, I.; Shapira, A.; Shacham-Diamand, Y.; Dvir, T. Engineered hybrid cardiac patches with multifunctional electronics for online monitoring and regulation of tissue function. Nat. Mater. 2016, 15, 679–685. [Google Scholar] [CrossRef] [Green Version]
- Feinberg, A.W.; Feigel, A.; Shevkoplyas, S.S.; Sheehy, S.; Whitesides, G.M.; Parker, K.K. Muscular thin films for building actuators and powering devices. Science 2007, 317, 1366–1370. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Montgomery, M.; Chamberlain, M.D.; Ogawa, S.; Korolj, A.; Pahnke, A.; Wells, L.A.; Massé, S.; Kim, J.; Reis, L.; et al. Biodegradable scaffold with built-in vasculature for organ-on-a-chip engineering and direct surgical anastomosis. Nat. Mater. 2016, 15, 669–678. [Google Scholar] [CrossRef] [Green Version]
- Bian, W.; Jackman, C.P.; Bursac, N. Controlling the structural and functional anisotropy of engineered cardiac tissues. Biofabrication 2014, 6, 024109. [Google Scholar] [CrossRef]
- Vunjak-Novakovic, G.; Ronaldson-Bouchard, K.; Radisic, M. Organs-on-a-chip models for biological research. Cell 2021, 184, 4597–4611. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Rafatian, N.; Feric, N.T.; Cox, B.J.; Aschar-Sobbi, R.; Wang, E.Y.; Aggarwal, P.; Zhang, B.; Conant, G.; Ronaldson-Bouchard, K.; et al. A platform for generation of chamber-specific cardiac tissues and disease modeling. Cell 2019, 176, 913–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lind, J.U.; Busbee, T.A.; Valentine, A.D.; Pasqualini, F.S.; Yuan, H.; Yadid, M.; Park, S.J.; Kotikian, A.; Nesmith, A.P.; Campbell, P.H.; et al. Instrumented cardiac microphysiological devices via multimaterial three-dimensional printing. Nat. Mater. 2017, 16, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Hudson, A.R.; Shiwarski, D.J.; Tashman, J.W.; Hinton, T.J.; Yerneni, S.; Bliley, J.M.; Campbell, P.G.; Feinberg, A.W. 3D bioprinting of collagen to rebuild components of the human heart. Science 2019, 365, 482–487. [Google Scholar] [CrossRef]
- Hinton, T.J.; Jallerat, Q.; Palchesko, R.N.; Park, J.H.; Grodzicki, M.S.; Shue, H.J.; Ramadan, M.H.; Hudson, A.R.; Feinberg, A.W. Three-dimensional printing of complex biological structures by freeform reversible embedding of suspended hydrogels. Sci. Adv. 2015, 1, e1500758. [Google Scholar] [CrossRef] [Green Version]
- Grigoryan, B.; Paulsen, S.J.; Corbett, D.C.; Sazer, D.W.; Fortin, C.L.; Zaita, A.J.; Greenfield, P.T.; Calafat, N.J.; Gounley, J.P.; Ta, A.H.; et al. Multivascular networks and functional intravascular topologies within biocompatible hydrogels. Science 2019, 364, 458–464. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Arneri, A.; Bersini, S.; Shin, S.R.; Zhu, K.; Goli-Malekabadi, Z.; Aleman, J.; Colosi, C.; Busignani, F.; Dell’Erba, V.; et al. Bioprinting 3D microfibrous scaffolds for engineering endothelialized myocardium and heart-on-a-chip. Biomaterials 2016, 110, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Skylar-Scott, M.A.; Uzel, S.G.M.; Nam, L.L.; Ahrens, J.H.; Truby, R.L.; Damaraju, S.; Lewis, J.A. Biomanufacturing of organ-specific tissues with high cellular density and embedded vascular channels. Sci. Adv. 2019, 5, eaaw2459. [Google Scholar] [CrossRef] [Green Version]
- Eschenhagen, T.; Fink, C.; Remmers, U.; Scholz, H.; Wattchow, J.; Weil, J.; Zimmermann, W.; Dohmen, H.H.; Schäfer, H.; Bishopric, N.; et al. Three-dimensional reconstitution of embryonic cardiomyocytes in a collagen matrix: A new heart muscle model system. FASEB J. 1997, 11, 683–694. [Google Scholar] [CrossRef]
- Boudou, T.; Legant, W.R.; Mu, A.; Borochin, M.A.; Thavandiran, N.; Radisic, M.; Zandstra, P.W.; Epstein, J.A.; Margulies, K.B.; Chen, C.S. A microfabricated platform to measure and manipulate the mechanics of engineered cardiac microtissues. Tissue Eng. Part A 2012, 18, 910–919. [Google Scholar] [CrossRef]
- Takasato, M.; Er, P.X.; Chiu, H.S.; Maier, B.; Baillie, G.J.; Ferguson, C.; Parton, R.G.; Wolvetang, E.J.; Roost, M.S.; Chuva de Sousa Lopes, S.M.; et al. Kidney organoids from human iPS cells contain multiple lineages and model human nephrogenesis. Nature 2015, 526, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Serra, D.; Mayr, U.; Boni, A.; Lukonin, I.; Rempfler, M.; Challet Meylan, L.; Stadler, M.B.; Strnad, P.; Papasaikas, P.; Vischi, D.; et al. Self-organization and symmetry breaking in intestinal organoid development. Nature 2019, 569, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Mansour, A.A.; Gonçalves, J.T.; Bloyd, C.W.; Li, H.; Fernandes, S.; Quang, D.; Johnston, S.; Parylak, S.L.; Jin, X.; Gage, F.H. An in vivo model of functional and vascularized human brain organoids. Nat. Biotechnol. 2018, 36, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.T.; Walsh, K. The future of cardiovascular regenerative medicine. Circulation 2016, 133, 2618–2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, D.J.; Coyle, R.C.; Tan, Y.; Jia, J.; Wong, K.; Toomer, K.; Menick, D.R.; Mei, Y. Inspiration from heart development: Biomimetic development of functional human cardiac organoids. Biomaterials 2017, 142, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Richards, D.J.; Li, Y.; Kerr, C.M.; Yao, J.; Beeson, G.C.; Coyle, R.C.; Chen, X.; Jia, J.; Damon, B.; Wilson, R.; et al. Human cardiac organoids for the modelling of myocardial infarction and drug cardiotoxicity. Nat. Biomed. Eng. 2020, 4, 446–462. [Google Scholar] [CrossRef]
- Ogle, B.M.; Bursac, N.; Domian, I.; Huang, N.F.; Menasché, P.; Murry, C.E.; Pruitt, B.; Radisic, M.; Wu, J.C.; Wu, S.M.; et al. Distilling complexity to advance cardiac tissue engineering. Sci. Transl. Med. 2016, 8, 342ps13. [Google Scholar] [CrossRef] [Green Version]
- Borovjagin, A.V.; Ogle, B.M.; Berry, J.L.; Zhang, J. From microscale devices to 3D printing: Advances in fabrication of 3D cardiovascular tissues. Circ. Res. 2017, 120, 150–165. [Google Scholar] [CrossRef]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Lee, S.J.; Cheng, H.J.; Yoo, J.J.; Atala, A. 3D bioprinted functional and contractile cardiac tissue constructs. Acta. Biomater. 2018, 70, 48–56. [Google Scholar] [CrossRef]
- Qasim, M.; Haq, F.; Kang, M.H.; Kim, J.H. 3D printing approaches for cardiac tissue engineering and role of immune modulation in tissue regeneration. Int. J. Nanomed. 2019, 14, 1311–1333. [Google Scholar] [CrossRef] [Green Version]
- Maiullari, F.; Costantini, M.; Milan, M.; Pace, V.; Chirivì, M.; Maiullari, S.; Rainer, A.; Baci, D.; Marei, H.E.; Seliktar, D.; et al. A multi-cellular 3D bioprinting approach for vascularized heart tissue engineering based on HUVECs and iPSC-derived cardiomyocytes. Sci. Rep. 2018, 8, 13532. [Google Scholar] [CrossRef] [PubMed]
- Pati, F.; Jang, J.; Ha, D.H.; Won Kim, S.; Rhie, J.W.; Shim, J.H.; Kim, D.H.; Cho, D.W. Printing three-dimensional tissue analogues with decellularized extracellular matrix bioink. Nat. Commun. 2014, 5, 3935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badylak, S.F.; Taylor, D.; Uygun, K. Whole-organ tissue engineering: Decellularization and recellularization of three-dimensional matrix scaffolds. Annu. Rev. Biomed. Eng. 2011, 13, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Kupfer, M.E.; Lin, W.H.; Ravikumar, V.; Qiu, K.; Wang, L.; Gao, L.; Bhuiyan, D.B.; Lenz, M.; Ai, J.; Mahutga, R.R.; et al. In situ expansion, differentiation, and electromechanical coupling of human cardiac muscle in a 3D bioprinted, chambered organoid. Circ. Res. 2020, 127, 207–224. [Google Scholar] [CrossRef]
- Vegas, A.J.; Veiseh, O.; Doloff, J.C.; Ma, M.; Tam, H.H.; Bratlie, K.; Li, J.; Bader, A.R.; Langan, E.; Olejnik, K.; et al. Combinatorial hydrogel library enables identification of materials that mitigate the foreign body response in primates. Nat. Biotechnol. 2016, 34, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Dondossola, E.; Holzapfel, B.M.; Alexander, S.; Filippini, S.; Hutmacher, D.W.; Friedl, P. Examination of the foreign body response to biomaterials by nonlinear intravital microscopy. Nat. Biomed. Eng. 2016, 1, 0007. [Google Scholar] [CrossRef] [Green Version]
- Doloff, J.C.; Veiseh, O.; Vegas, A.J.; Tam, H.H.; Farah, S.; Ma, M.; Li, J.; Bader, A.; Chiu, A.; Sadraei, A.; et al. Colony stimulating factor-1 receptor is a central component of the foreign body response to biomaterial implants in rodents and non-human primates. Nat. Mater. 2017, 16, 671–680. [Google Scholar] [CrossRef]
- Kolesky, D.B.; Homan, K.A.; Skylar-Scott, M.A.; Lewis, J.A. Three-dimensional bioprinting of thick vascularized tissues. Proc. Natl. Acad. Sci. USA 2016, 113, 3179–3184. [Google Scholar] [CrossRef] [Green Version]
- Zhu, W.; Qu, X.; Zhu, J.; Ma, X.; Patel, S.; Liu, J.; Wang, P.; Lai, C.S.; Gou, M.; Xu, Y.; et al. Direct 3D bioprinting of prevascularized tissue constructs with complex microarchitecture. Biomaterials 2017, 124, 106–115. [Google Scholar] [CrossRef] [Green Version]
- Bernal, P.N.; Delrot, P.; Loterie, D.; Li, Y.; Malda, J.; Moser, C.; Levato, R. Volumetric bioprinting of complex living-tissue constructs within seconds. Adv. Mater. 2019, 31, e1904209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Wang, L.; Li, T.; Liu, S.; Guo, B.; Huang, W.; Wu, Y. 3D bioprinting in cardiac tissue engineering. Theranostics 2021, 11, 7948–7969. [Google Scholar] [CrossRef] [PubMed]
- Kozaniti, F.K.; Metsiou, D.N.; Manara, A.E.; Athanassiou, G.; Deligianni, D.D. Recent advancements in 3D printing and bioprinting methods for cardiovascular tissue engineering. Bioengineering 2021, 8, 133. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, N.L.; Muskheli, V.; Razumova, M.V.; Korte, F.S.; Regnier, M.; Hauch, K.D.; Pabon, L.; Reinecke, H.; Murry, C.E. Growth of engineered human myocardium with mechanical loading and vascular coculture. Circ. Res. 2011, 109, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Feric, N.T.; Pallotta, I.; Singh, R.; Bogdanowicz, D.R.; Gustilo, M.; Chaudhary, K.; Willette, R.N.; Chendrimada, T.; Xu, X.; Graziano, M.P.; et al. Engineered cardiac tissues generated in the Biowire™ II: A platform for human-based drug discovery. Toxicol. Sci. 2019, 172, 89–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braam, S.R.; Passier, R.; Mummery, C.L. Cardiomyocytes from human pluripotent stem cells in regenerative medicine and drug discovery. Trends Pharmacol. Sci. 2009, 30, 536–545. [Google Scholar] [CrossRef] [PubMed]
- Magdy, T.; Schuldt, A.J.T.; Wu, J.C.; Bernstein, D.; Burridge, P.W. Human induced pluripotent stem cell (hiPSC)-derived cells to assess drug cardiotoxicity: Opportunities and problems. Annu. Rev. Pharmacol. Toxicol. 2018, 58, 83–103. [Google Scholar] [CrossRef]
- Marsano, A.; Conficconi, C.; Lemme, M.; Occhetta, P.; Gaudiello, E.; Votta, E.; Cerino, G.; Redaelli, A.; Rasponi, M. Beating heart on a chip: A novel microfluidic platform to generate functional 3D cardiac microtissues. Lab Chip 2016, 16, 599–610. [Google Scholar] [CrossRef]
- Kensah, G.; Roa Lara, A.; Dahlmann, J.; Zweigerdt, R.; Schwanke, K.; Hegermann, J.; Skvorc, D.; Gawol, A.; Azizian, A.; Wagner, S.; et al. Murine and human pluripotent stem cell-derived cardiac bodies form contractile myocardial tissue in vitro. Eur. Heart J. 2013, 34, 1134–1146. [Google Scholar] [CrossRef] [Green Version]
- Bristow, M.R.; Ginsburg, R.; Strosberg, A.; Montgomery, W.; Minobe, W. Pharmacology and inotropic potential of forskolin in the human heart. J. Clin. Investig. 1984, 74, 212–223. [Google Scholar] [CrossRef]
- Molenaar, P.; Christ, T.; Hussain, R.I.; Engel, A.; Berk, E.; Gillette, K.T.; Chen, L.; Galindo-Tovar, A.; Krobert, K.A.; Ravens, U.; et al. PDE3, but not PDE4, reduces β1- and β2;-adrenoceptor-mediated inotropic and lusitropic effects in failing ventricle from metoprolol-treated patients. Br. J. Pharmacol. 2013, 169, 528–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuppinger, C. 3D cardiac cell culture: A critical review of current technologies and applications. Front. Cardiovasc. Med. 2019, 6, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lind, J.U.; Yadid, M.; Perkins, I.; O’Connor, B.B.; Eweje, F.; Chantre, C.O.; Hemphill, M.A.; Yuan, H.; Campbell, P.H.; Vlassak, J.J.; et al. Cardiac microphysiological devices with flexible thin-film sensors for higher-throughput drug screening. Lab Chip 2017, 17, 3692–3703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Radisic, M. Organ-on-a-chip devices advance to market. Lab Chip 2017, 17, 2395–2420. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.G.W.; Owen, T.; Bhagwan, J.R.; Mosqueira, D.; Scott, E.; Mannhardt, I.; Patel, A.; Barriales-Villa, R.; Monserrat, L.; Hansen, A.; et al. Isogenic pairs of hiPSC-CMs with hypertrophic cardiomyopathy/LVNC-associated ACTC1 E99K mutation unveil differential functional deficits. Stem Cell Rep. 2018, 11, 1226–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de la Roche, J.; Angsutararux, P.; Kempf, H.; Janan, M.; Bolesani, E.; Thiemann, S.; Wojciechowski, D.; Coffee, M.; Franke, A.; Schwanke, K.; et al. Comparing human iPSC-cardiomyocytes versus HEK293T cells unveils disease-causing effects of Brugada mutation A735V of NaV1.5 sodium channels. Sci. Rep. 2019, 9, 11173. [Google Scholar] [CrossRef] [Green Version]
- Bellin, M.; Casini, S.; Davis, R.P.; D’Aniello, C.; Haas, J.; Ward-van Oostwaard, D.; Tertoolen, L.G.; Jung, C.B.; Elliott, D.A.; Welling, A.; et al. Isogenic human pluripotent stem cell pairs reveal the role of a KCNH2 mutation in long-QT syndrome. EMBO J. 2013, 32, 3161–3175. [Google Scholar] [CrossRef]
- Wang, G.; McCain, M.L.; Yang, L.; He, A.; Pasqualini, F.S.; Agarwal, A.; Yuan, H.; Jiang, D.; Zhang, D.; Zangi, L.; et al. Modeling the mitochondrial cardiomyopathy of Barth syndrome with induced pluripotent stem cell and heart-on-chip technologies. Nat. Med. 2014, 20, 616–623. [Google Scholar] [CrossRef]
- Mosqueira, D.; Mannhardt, I.; Bhagwan, J.R.; Lis-Slimak, K.; Katili, P.; Scott, E.; Hassan, M.; Prondzynski, M.; Harmer, S.C.; Tinker, A.; et al. CRISPR/Cas9 editing in human pluripotent stem cell-cardiomyocytes highlights arrhythmias, hypocontractility, and energy depletion as potential therapeutic targets for hypertrophic cardiomyopathy. Eur. Heart J. 2018, 39, 3879–3892. [Google Scholar] [CrossRef]
- Hinson, J.T.; Chopra, A.; Nafissi, N.; Polacheck, W.J.; Benson, C.C.; Swist, S.; Gorham, J.; Yang, L.; Schafer, S.; Sheng, C.C.; et al. HEART DISEASE. Titin mutations in iPS cells define sarcomere insufficiency as a cause of dilated cardiomyopathy. Science 2015, 349, 982–986. [Google Scholar] [CrossRef] [Green Version]
- Prondzynski, M.; Lemoine, M.D.; Zech, A.T.; Horváth, A.; Di Mauro, V.; Koivumäki, J.T.; Kresin, N.; Busch, J.; Krause, T.; Krämer, E.; et al. Disease modeling of a mutation in α-actinin 2 guides clinical therapy in hypertrophic cardiomyopathy. EMBO Mol. Med. 2019, 11, e11115. [Google Scholar] [CrossRef] [PubMed]
- Gangadhar, T.C.; Von der Lohe, E.; Sawada, S.G.; Helft, P.R. Takotsubo cardiomyopathy in a patient with esophageal cancer: A case report. J. Med. Case Rep. 2008, 2, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, M.R.; Myerburg, R.J.; Francis, D.P.; Cole, G.D.; Marbán, E. Translating stem cell research to cardiac disease therapies: Pitfalls and prospects for improvement. J. Am. Coll. Cardiol. 2014, 64, 922–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerbin, K.A.; Murry, C.E. The winding road to regenerating the human heart. Cardiovasc. Pathol. 2015, 24, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschenhagen, T.; Bolli, R.; Braun, T.; Field, L.J.; Fleischmann, B.K.; Frisén, J.; Giacca, M.; Hare, J.M.; Houser, S.; Lee, R.T.; et al. Cardiomyocyte regeneration: A consensus statement. Circulation 2017, 136, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Terrovitis, J.; Lautamäki, R.; Bonios, M.; Fox, J.; Engles, J.M.; Yu, J.; Leppo, M.K.; Pomper, M.G.; Wahl, R.L.; Seidel, J.; et al. Noninvasive quantification and optimization of acute cell retention by in vivo positron emission tomography after intramyocardial cardiac-derived stem cell delivery. J. Am. Coll. Cardiol. 2009, 54, 1619–1626. [Google Scholar] [CrossRef] [Green Version]
- Chong, J.J.; Yang, X.; Don, C.W.; Minami, E.; Liu, Y.W.; Weyers, J.J.; Mahoney, W.M.; Van Biber, B.; Cook, S.M.; Palpant, N.J.; et al. Human embryonic-stem-cell-derived cardiomyocytes regenerate non-human primate hearts. Nature 2014, 510, 273–277. [Google Scholar] [CrossRef]
- Shiba, Y.; Gomibuchi, T.; Seto, T.; Wada, Y.; Ichimura, H.; Tanaka, Y.; Ogasawara, T.; Okada, K.; Shiba, N.; Sakamoto, K.; et al. Allogeneic transplantation of iPS cell-derived cardiomyocytes regenerates primate hearts. Nature 2016, 538, 388–391. [Google Scholar] [CrossRef]
- Galdos, F.X.; Guo, Y.; Paige, S.L.; VanDusen, N.J.; Wu, S.M.; Pu, W.T. Cardiac Regeneration: Lessons From Development. Circ. Res. 2017, 120, 941–959. [Google Scholar] [CrossRef] [Green Version]
- Madonna, R.; Van Laake, L.W.; Botker, H.E.; Davidson, S.M.; De Caterina, R.; Engel, F.B.; Eschenhagen, T.; Fernandez-Aviles, F.; Hausenloy, D.J.; Hulot, J.S.; et al. ESC working group on cellular biology of the heart: Position paper for cardiovascular research: Tissue engineering strategies combined with cell therapies for cardiac repair in ischaemic heart disease and heart failure. Cardiovasc. Res. 2019, 115, 488–500. [Google Scholar] [CrossRef] [Green Version]
- Silver, S.E.; Barrs, R.W.; Mei, Y. Transplantation of human pluripotent stem cell-derived cardiomyocytes for cardiac regenerative therapy. Front. Cardiovasc. Med. 2021, 8, 707890. [Google Scholar] [CrossRef] [PubMed]
- Mirotsou, M.; Jayawardena, T.M.; Schmeckpeper, J.; Gnecchi, M.; Dzau, V.J. Paracrine mechanisms of stem cell reparative and regenerative actions in the heart. J. Mol. Cell Cardiol. 2011, 50, 280–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pecha, S.; Yorgan, K.; Röhl, M.; Geertz, B.; Hansen, A.; Weinberger, F.; Sehner, S.; Ehmke, H.; Reichenspurner, H.; Eschenhagen, T.; et al. Human iPS cell-derived engineered heart tissue does not affect ventricular arrhythmias in a guinea pig cryo-injury model. Sci. Rep. 2019, 9, 9831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, X.; Liu, Y.; Bai, A.; Cai, H.; Bai, Y.; Jiang, W.; Yang, H.; Wang, X.; Yang, L.; Sun, N.; et al. A viscoelastic adhesive epicardial patch for treating myocardial infarction. Nat. Biomed. Eng. 2019, 3, 632–643. [Google Scholar] [CrossRef]
- Zimmermann, W.H.; Melnychenko, I.; Wasmeier, G.; Didié, M.; Naito, H.; Nixdorff, U.; Hess, A.; Budinsky, L.; Brune, K.; Michaelis, B.; et al. Engineered heart tissue grafts improve systolic and diastolic function in infarcted rat hearts. Nat. Med. 2006, 12, 452–458. [Google Scholar] [CrossRef]
- Querdel, E.; Reinsch, M.; Castro, L.; Köse, D.; Bähr, A.; Reich, S.; Geertz, B.; Ulmer, B.; Schulze, M.; Lemoine, M.D.; et al. Human engineered heart tissue patches remuscularize the injured heart in a dose-dependent manner. Circulation 2021, 143, 1991–2006. [Google Scholar] [CrossRef]
- Kawamura, T.; Miyagawa, S.; Fukushima, S.; Maeda, A.; Kashiyama, N.; Kawamura, A.; Miki, K.; Okita, K.; Yoshida, Y.; Shiina, T.; et al. Cardiomyocytes derived from MHC-Homozygous induced pluripotent stem cells exhibit reduced allogeneic immunogenicity in MHC-matched non-human primates. Stem Cell Rep. 2016, 6, 312–320. [Google Scholar] [CrossRef] [Green Version]
- Madonna, R. Human-induced pluripotent stem cells: In quest of clinical applications. Mol. Biotechnol. 2012, 52, 193–203. [Google Scholar] [CrossRef]
- Almeida, S.O.; Skelton, R.J.; Adigopula, S.; Ardehali, R. Arrhythmia in stem cell transplantation. Card. Electrophysiol. Clin. 2015, 7, 357–370. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.K.; Neofytou, E.; Rhee, J.W.; Wu, J.C. Potential strategies to address the major clinical barriers facing stem cell regenerative therapy for cardiovascular disease: A review. JAMA Cardiol. 2016, 1, 953–962. [Google Scholar] [CrossRef] [Green Version]
- Frey, N.; Linke, A.; Süselbeck, T.; Müller-Ehmsen, J.; Vermeersch, P.; Schoors, D.; Rosenberg, M.; Bea, F.; Tuvia, S.; Leor, J. Intracoronary delivery of injectable bioabsorbable scaffold (IK-5001) to treat left ventricular remodeling after ST-elevation myocardial infarction: A first-in-man study. Circ. Cardiovasc. Interv. 2014, 7, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.V.; Zeymer, U.; Douglas, P.S.; Al-Khalidi, H.; Liu, J.; Gibson, C.M.; Harrison, R.W.; Joseph, D.S.; Heyrman, R.; Krucoff, M.W. A randomized, double-blind, placebo-controlled trial to evaluate the safety and effectiveness of intracoronary application of a novel bioabsorbable cardiac matrix for the prevention of ventricular remodeling after large ST-segment elevation myocardial infarction: Rationale and design of the PRESERVATION I trial. Am. Heart J. 2015, 170, 929–937. [Google Scholar] [PubMed]
- Rao, S.V.; Zeymer, U.; Douglas, P.S.; Al-Khalidi, H.; White, J.A.; Liu, J.; Levy, H.; Guetta, V.; Gibson, C.M.; Tanguay, J.F.; et al. Bioabsorbable intracoronary matrix for prevention of ventricular remodeling after myocardial infarction. J. Am. Coll. Cardiol. 2016, 68, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Coats, A.J.; Cristian, G.; Dragomir, D.; Pusineri, E.; Piredda, M.; Bettari, L.; Dowling, R.; Volterrani, M.; Kirwan, B.A.; et al. A prospective comparison of alginate-hydrogel with standard medical therapy to determine impact on functional capacity and clinical outcomes in patients with advanced heart failure (AUGMENT-HF trial). Eur. Heart J. 2015, 36, 2297–2309. [Google Scholar] [CrossRef] [Green Version]
- Mann, D.L.; Lee, R.J.; Coats, A.J.; Neagoe, G.; Dragomir, D.; Pusineri, E.; Piredda, M.; Bettari, L.; Kirwan, B.A.; Dowling, R.; et al. One-year follow-up results from AUGMENT-HF: A multicentre randomized controlled clinical trial of the efficacy of left ventricular augmentation with Algisyl in the treatment of heart failure. Eur. J. Heart Fail. 2016, 18, 314–325. [Google Scholar] [CrossRef]
- Lee, R.J.; Hinson, A.; Bauernschmitt, R.; Matschke, K.; Fang, Q.; Mann, D.L.; Dowling, R.; Schiller, N.; Sabbah, H.N. The feasibility and safety of Algisyl-LVR™ as a method of left ventricular augmentation in patients with dilated cardiomyopathy: Initial first in man clinical results. Int. J. Cardiol. 2015, 199, 18–24. [Google Scholar] [CrossRef]
- Yanagawa, B.; Rao, V.; Yau, T.M.; Cusimano, R.J. Potential myocardial regeneration with CorMatrix ECM: A case report. J. Thorac. Cardiovasc. Surg. 2014, 147, e41–e43. [Google Scholar] [CrossRef] [Green Version]
- Mewhort, H.E.; Turnbull, J.D.; Meijndert, H.C.; Ngu, J.M.; Fedak, P.W. Epicardial infarct repair with basic fibroblast growth factor-enhanced CorMatrix-ECM biomaterial attenuates postischemic cardiac remodeling. J. Thorac. Cardiovasc. Surg. 2014, 147, 1650–1659. [Google Scholar] [CrossRef] [Green Version]
- Mewhort, H.E.; Turnbull, J.D.; Satriano, A.; Chow, K.; Flewitt, J.A.; Andrei, A.C.; Guzzardi, D.G.; Svystonyuk, D.A.; White, J.A.; Fedak, P.W. Epicardial infarct repair with bioinductive extracellular matrix promotes vasculogenesis and myocardial recovery. J. Heart Lung Transplant. 2016, 35, 661–670. [Google Scholar] [CrossRef] [Green Version]
- Traverse, J.H.; Henry, T.D.; Dib, N.; Patel, A.N.; Pepine, C.; Schaer, G.L.; DeQuach, J.A.; Kinsey, A.M.; Chamberlin, P.; Christman, K.L. First-in-man study of a cardiac extracellular matrix hydrogel in early and late myocardial infarction patients. JACC Basic Transl. Sci. 2019, 4, 659–669. [Google Scholar] [CrossRef]
- Menasché, P.; Vanneaux, V.; Hagège, A.; Bel, A.; Cholley, B.; Cacciapuoti, I.; Parouchev, A.; Benhamouda, N.; Tachdjian, G.; Tosca, L.; et al. Human embryonic stem cell-derived cardiac progenitors for severe heart failure treatment: First clinical case report. Eur. Heart J. 2015, 36, 2011–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menasché, P.; Vanneaux, V.; Hagège, A.; Bel, A.; Cholley, B.; Parouchev, A.; Cacciapuoti, I.; Al-Daccak, R.; Benhamouda, N.; Blons, H.; et al. Transplantation of human embryonic stem cell-derived cardiovascular progenitors for severe ischemic left ventricular dysfunction. J. Am. Coll. Cardiol. 2018, 71, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Kashiyama, N.; Miyagawa, S.; Fukushima, S.; Kawamura, T.; Kawamura, A.; Yoshida, S.; Eiraku, S.; Harada, A.; Matsunaga, K.; Watabe, T.; et al. MHC-mismatched allotransplantation of induced pluripotent stem cell-derived cardiomyocyte sheets to improve cardiac function in a primate ischemic cardiomyopathy model. Transplantation 2019, 103, 1582–1590. [Google Scholar] [CrossRef] [PubMed]
- Gyöngyösi, M.; Dib, N. Diagnostic and prognostic value of 3D NOGA mapping in ischemic heart disease. Nat. Rev. Cardiol. 2011, 8, 393–404. [Google Scholar] [CrossRef]
- Schmauss, D.; Haeberle, S.; Hagl, C.; Sodian, R. Three-dimensional printing in cardiac surgery and interventional cardiology: A single-centre experience. Eur. J. Cardiothorac. Surg. 2015, 47, 1044–1052. [Google Scholar] [CrossRef] [Green Version]
- Vukicevic, M.; Mosadegh, B.; Min, J.K.; Little, S.H. Cardiac 3D printing and its future directions. JACC Cardiovasc. Imaging 2017, 10, 171–184. [Google Scholar] [CrossRef]
- Hendrickson, T.; Mancino, C.; Whitney, L.; Tsao, C.; Rahimi, M.; Taraballi, F. Mimicking cardiac tissue complexity through physical cues: A review on cardiac tissue engineering approaches. Nanomedicine 2021, 33, 102367. [Google Scholar] [CrossRef]
- Chien, K.R.; Zangi, L.; Lui, K.O. Synthetic chemically modified mRNA (modRNA): Toward a new technology platform for cardiovascular biology and medicine. Cold Spring Harb. Perspect. Med. 2014, 5, a014035. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, L.; Clarke, J.C.; Yen, C.; Gregoire, F.; Albery, T.; Billger, M.; Egnell, A.C.; Gan, L.M.; Jennbacken, K.; Johansson, E.; et al. Biocompatible, purified VEGF-A mRNA improves cardiac function after intracardiac injection 1 week post-myocardial infarction in Swine. Mol. Ther. Methods Clin. Dev. 2018, 9, 330–346. [Google Scholar] [CrossRef] [Green Version]
- Gan, L.M.; Lagerström-Fermér, M.; Carlsson, L.G.; Arfvidsson, C.; Egnell, A.C.; Rudvik, A.; Kjaer, M.; Collén, A.; Thompson, J.D.; Joyal, J.; et al. Intradermal delivery of modified mRNA encoding VEGF-A in patients with type 2 diabetes. Nat. Commun. 2019, 10, 871. [Google Scholar] [CrossRef]
- Sluijter, J.P.; Verhage, V.; Deddens, J.C.; van den Akker, F.; Doevendans, P.A. Microvesicles and exosomes for intracardiac communication. Cardiovasc. Res. 2014, 102, 302–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamiak, M.; Sahoo, S. Exosomes in myocardial repair: Advances and challenges in the development of next-generation therapeutics. Mol. Ther. 2018, 26, 1635–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arslan, F.; Lai, R.C.; Smeets, M.B.; Akeroyd, L.; Choo, A.; Aguor, E.N.; Timmers, L.; van Rijen, H.V.; Doevendans, P.A.; Pasterkamp, G.; et al. Mesenchymal stem cell-derived exosomes increase ATP levels, decrease oxidative stress and activate PI3K/Akt pathway to enhance myocardial viability and prevent adverse remodeling after myocardial ischemia/reperfusion injury. Stem Cell Res. 2013, 10, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Schema of the latest biomaterials and biofabrication technologies for the generation of engineered heart muscles. 3D, three-dimensional; BP, bioprinting; EC, endothelial cell; ECM, extracellular matrix; EHT, engineered heart tissue; FRESH, freeform reversible embedding of suspended hydrogels; PDMS, polydimethylsiloxane; SWIFT, sacrificial writing into functional tissue. 1. Hydrogels: In situ gelling [82,97], Epicardial patch [83,95], Cell/biomolecule encapsulation [64,75], Casting molds [40,76]; 2. Deculllarized Bioscaffolds: ECM bioscaffolds [134,135]; 3. Microfabrication Technologies: Electronic cardiac patch [147], Patterning (on PDMS) [148], Angiochip [149], Anisotropic cardiac patch [140,150], Self-organizing patterned michrochamber [142], Electrospinning [145,146], Microfluidic chip [151], Muscle strip (ring shaped EHT) [40], Dynamic culture (cardiobundles) [137], Micro heart muscle arrays [76], BiowireTM [45,152]; 4. Organoids: Cardiac organoids [143,144]; 5. Bioprinting: Extrusion based multimaterial BP [153], FRESH BP [154,155], Stereolitography based BP of vasculature [156], Multiphoton-excited 3D BP [79], BP of microfibrous scaffold & ECs [157], SWIFT BP [158].
Figure 1.
Schema of the latest biomaterials and biofabrication technologies for the generation of engineered heart muscles. 3D, three-dimensional; BP, bioprinting; EC, endothelial cell; ECM, extracellular matrix; EHT, engineered heart tissue; FRESH, freeform reversible embedding of suspended hydrogels; PDMS, polydimethylsiloxane; SWIFT, sacrificial writing into functional tissue. 1. Hydrogels: In situ gelling [82,97], Epicardial patch [83,95], Cell/biomolecule encapsulation [64,75], Casting molds [40,76]; 2. Deculllarized Bioscaffolds: ECM bioscaffolds [134,135]; 3. Microfabrication Technologies: Electronic cardiac patch [147], Patterning (on PDMS) [148], Angiochip [149], Anisotropic cardiac patch [140,150], Self-organizing patterned michrochamber [142], Electrospinning [145,146], Microfluidic chip [151], Muscle strip (ring shaped EHT) [40], Dynamic culture (cardiobundles) [137], Micro heart muscle arrays [76], BiowireTM [45,152]; 4. Organoids: Cardiac organoids [143,144]; 5. Bioprinting: Extrusion based multimaterial BP [153], FRESH BP [154,155], Stereolitography based BP of vasculature [156], Multiphoton-excited 3D BP [79], BP of microfibrous scaffold & ECs [157], SWIFT BP [158].

Figure 2.
Modeling of cardiac tissue engineering-based personalized medicine for genetic heart disease. The panel highlights the hPSC-CM and 3D engineered heart tissue-combined platforms for the personalized treatment to genetic heart disease, as Prondzynski et al. have demonstrated such a proof-of-concept successfully to the inherited HCM-affected family, harboring a rare c.740C>T mutation in the ACTN2 gene [201]. The image of catheterization was obtained from a previous report [202]. CM, cardiomyocyte; HCM, hypertrophic cardiomyopathy; hiPSC, human inducible pluripotent stem cell.
Figure 2.
Modeling of cardiac tissue engineering-based personalized medicine for genetic heart disease. The panel highlights the hPSC-CM and 3D engineered heart tissue-combined platforms for the personalized treatment to genetic heart disease, as Prondzynski et al. have demonstrated such a proof-of-concept successfully to the inherited HCM-affected family, harboring a rare c.740C>T mutation in the ACTN2 gene [201]. The image of catheterization was obtained from a previous report [202]. CM, cardiomyocyte; HCM, hypertrophic cardiomyopathy; hiPSC, human inducible pluripotent stem cell.


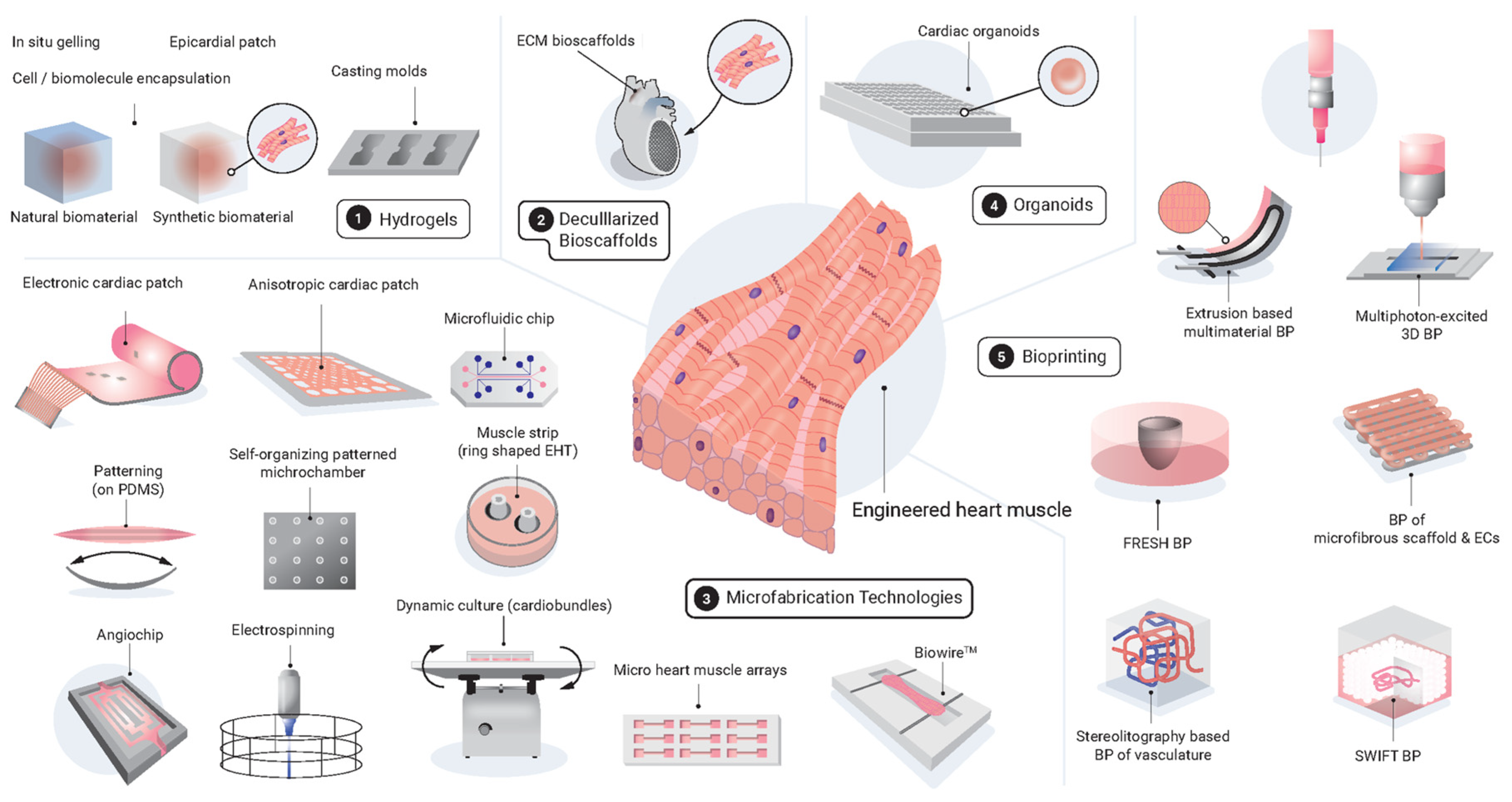{kind=link}
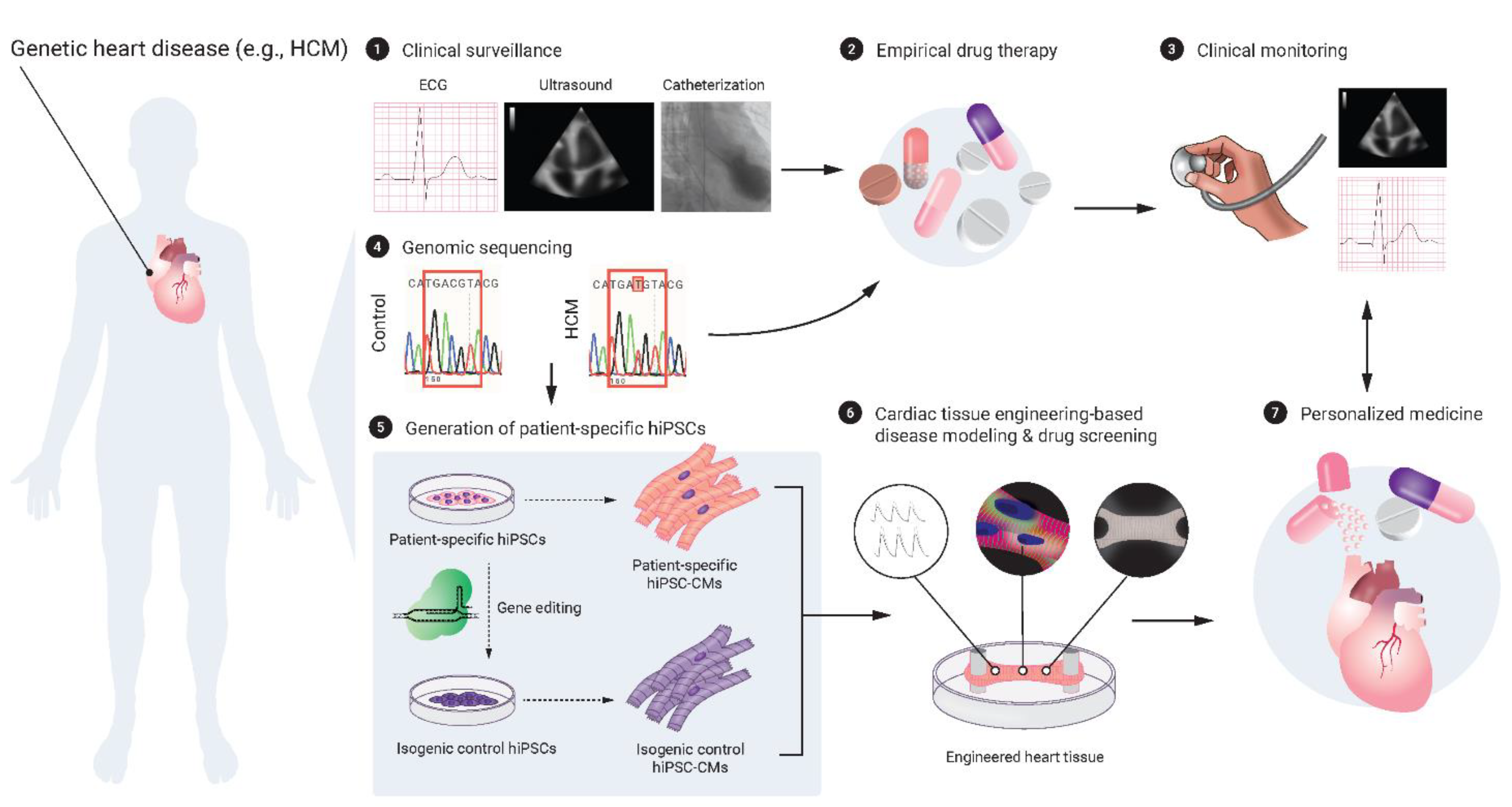{kind=link}
Table 1.
Tissue-engineering strategies for promoting maturation in hPSC-CMs. 3D, three-dimensional; EC, endothelial cell; EHT, engineered heart tissue; FB, fibroblast; SMC, smooth muscle cell.
Table 1.
Tissue-engineering strategies for promoting maturation in hPSC-CMs. 3D, three-dimensional; EC, endothelial cell; EHT, engineered heart tissue; FB, fibroblast; SMC, smooth muscle cell.
| Major Classification | Type of Strategies | Subtype | References |
|---|---|---|---|
| Physiological stimulation | Mechanical stress loading | [40,41,42,43] | |
| Electrical stimulation/pacing | [42,44,45] | ||
| Advanced culture | 3D cultures | EHTs with a scaffold protein | [46,47,48,49] |
| Cardiac spheroids without scaffold proteins | [47,50,51] | ||
| Intercellular crosstalk | Co-culture/administration with ECs | [52,53] | |
| Co-culture/administration with FBs | [48] | ||
| Co-culture/administration with epicardial cells | [54] | ||
| Co-culture/administration with SMCs/ECs and FBs | [55,56,57,58] | ||
| Biochemical intervention | Metabolic intervention | High fatty acid/low glucose diet | [59,60] |
| Hormone intervention | Tri-iodothyronine (T3) | [61,62] | |
| Glucocorticoid | [63] | ||
| Paracrine signals | Growth factors | [23,64] | |
| Genetic regulation | Overexpression of maturation-inducing genes | Ion channels (e.g., KCNJ2), etc. | [23,32] |
| Induction of cell cycle arrest | [23,32] | ||
| In vivo transplantation | Transplantation into a normal or injured heart | [32,65] |
Table 2.
The selected in vivo preclinical studies and human clinical trials of cardiac tissue engineering-based therapies for heart regeneration and repair. CABG, coronary artery bypass grafting; CM, cardiomyocyte; EC, endothelial cell; ECM, extracellular matrix; EF, ejection fraction; EHM, engineered heart muscle; hESC, human embryonic stem cell; hiPSC, human inducible pluripotent stem cell; HF, heart failure; IGF, insulin-like growth factor; IJ, injection; IR, ischemia reperfusion injury; MI, myocardial infarction; PLGA, poly(lactic-co-glycolic acid); PNIPAAm, poly(N-isopropylacrylamide); SMC, smooth muscle cell.
Table 2.
The selected in vivo preclinical studies and human clinical trials of cardiac tissue engineering-based therapies for heart regeneration and repair. CABG, coronary artery bypass grafting; CM, cardiomyocyte; EC, endothelial cell; ECM, extracellular matrix; EF, ejection fraction; EHM, engineered heart muscle; hESC, human embryonic stem cell; hiPSC, human inducible pluripotent stem cell; HF, heart failure; IGF, insulin-like growth factor; IJ, injection; IR, ischemia reperfusion injury; MI, myocardial infarction; PLGA, poly(lactic-co-glycolic acid); PNIPAAm, poly(N-isopropylacrylamide); SMC, smooth muscle cell.
| In Vivo Preclinical Studies | |||||||
| Tissue Engineering Strategy | Biomaterial | Cell Source | Animal | Disease Model | Route of Administration | References | |
| Cardiac patch | Fibrin | hiPSC-CM, pericytes | Rat | MI | Epicardium | [95] | |
| Cardiac patch | Fibrin (IGF-loaded) | hiPSC-CM, -EC, and -SMC | Pig | MI | Epicardium | [97] | |
| Muscle strip/EHM | Fibrin | hiPSC-CM, -EC | Guinea pig | Cryoinjury | Epicardium | [139,213] | |
| EHM | Collagen | hESC-CM | Rat | MI/IR | Epicardium | [99] | |
| EHM | Collagen | hESC-CM | Rat | Chronic MI/IR | Epicardium | [81] | |
| In situ gelling system | Alginate | Acellular | Rat/Pig | MI | Intramyocardial/ Intracoronary IJ | [102,103] | |
| In situ gelling system | Chitosan | Acellular | Rat | MI | Intramyocardial IJ | [106] | |
| Nanofibers/EHM | PLGA | hiPSC-CM | Rat | MI | Epicardium | [110] | |
| In situ gelling system | PNIPAAm-based | Acellular | Rat | Chronic MI | Intramyocardial IJ | [112] | |
| In situ gelling system | Decellularized cardiac ECM hydrogel | Acellular | Pig | MI | Trans-endocardial IJ | [132] | |
| 3D-printing-based cardiac patch | ECM scaffold | hiPSC-CM, -EC, and -SMC | Mouse | MI | Epicardium | [79] | |
| Cell sheet | Scaffold-free | hiPSC-CM | Pig | MI | Epicardium | [137] | |
| Human Clinical Trials | |||||||
| Trial Name (Trial Identifier) | Patient Population | Phase | Tissue Engineering Strategy | Biomaterial | Cell Source | Route of Administration | References |
| PRESERVATION I (NCT01226563) | Acute MI; Congestive HF; ST elevation MI | Phase 1 completed | In situ gelling system | Alginate-based hydrogel | acellular | Intracoronary IJ | [221,222,223] |
| AUGMENT-HF (NCT01311791) | Severe chronic HF (EF ≤ 35%) [57% ischemic and 43% nonischemic] | Phase 2 completed | In situ gelling system | Alginate-based hydrogel | acellular | Intramyocardial IJ | [224,225,226] |
| Epicardial infarct repair using CorMatrixTM-ECM (NCT02887768) | Acute~subacute MI (within 6 weeks); CABG scheduled | Phase 1 completed | Cardiac patch | Porcine small intestine-derived ECM epicardial patch | acellular | Epicardium | [227,228,229] |
| VentriGel in post-MI patients (NCT02305602) | Recent ~ late MI (60 days to 3 yrs); Ischemic HF (EF ≥ 25%; ≤45%) | Phase 1 completed | In situ gelling system | Porcine myocardium-derived ECM hydrogel | acellular | Trans-endocardial IJ | [230] |
| ESCORT (NCT02057900) | Severe chronic ischemic HF (EF ≤3 5%) | Phase 1 completed | Cardiac patch | Fibrin patch | hESC-derived CD15+Isl1+ progenitors | Epicardium | [231,232] |
| BioVAT-HF (NCT04396899) | Severe HF (EF ≤ 35%) | Phase 1 & 2 recruiting | EHM | Collagen type I hydrogel | hiPSC-CM, -stromal cell | Epicardium | |
| Human (allogenic) iPSC-CM sheet for ischemic cardiomyopathy (NCT04696328) | Severe chronic ischemic HF (EF ≤ 35%) | Phase 1 recruiting | Cell sheet | Scaffold-free cell sheet | hiPSC-CM | Epicardium | [217,233] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Häneke, T.; Sahara, M. Progress in Bioengineering Strategies for Heart Regenerative Medicine. Int. J. Mol. Sci. 2022, 23, 3482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23073482
AMA Style
Häneke T, Sahara M. Progress in Bioengineering Strategies for Heart Regenerative Medicine. International Journal of Molecular Sciences. 2022; 23(7):3482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23073482
Chicago/Turabian StyleHäneke, Timm, and Makoto Sahara. 2022. "Progress in Bioengineering Strategies for Heart Regenerative Medicine" International Journal of Molecular Sciences 23, no. 7: 3482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23073482
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.