
In Vitro Cytotoxicity, Colonisation by Fibroblasts and Antimicrobial Properties of Surgical Meshes Coated with Bacterial Cellulose

 , , , and
, , , and 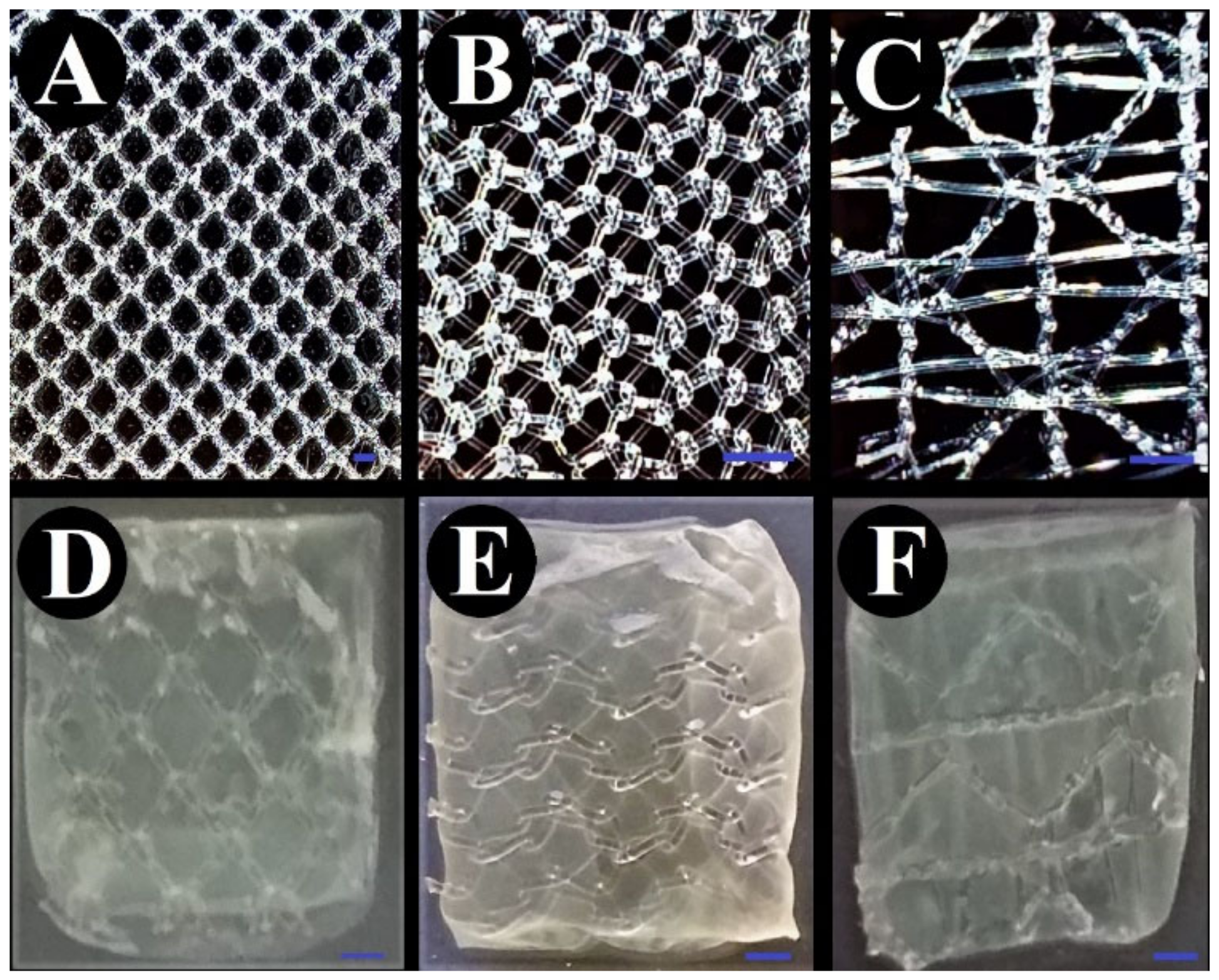{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Sample Preparation
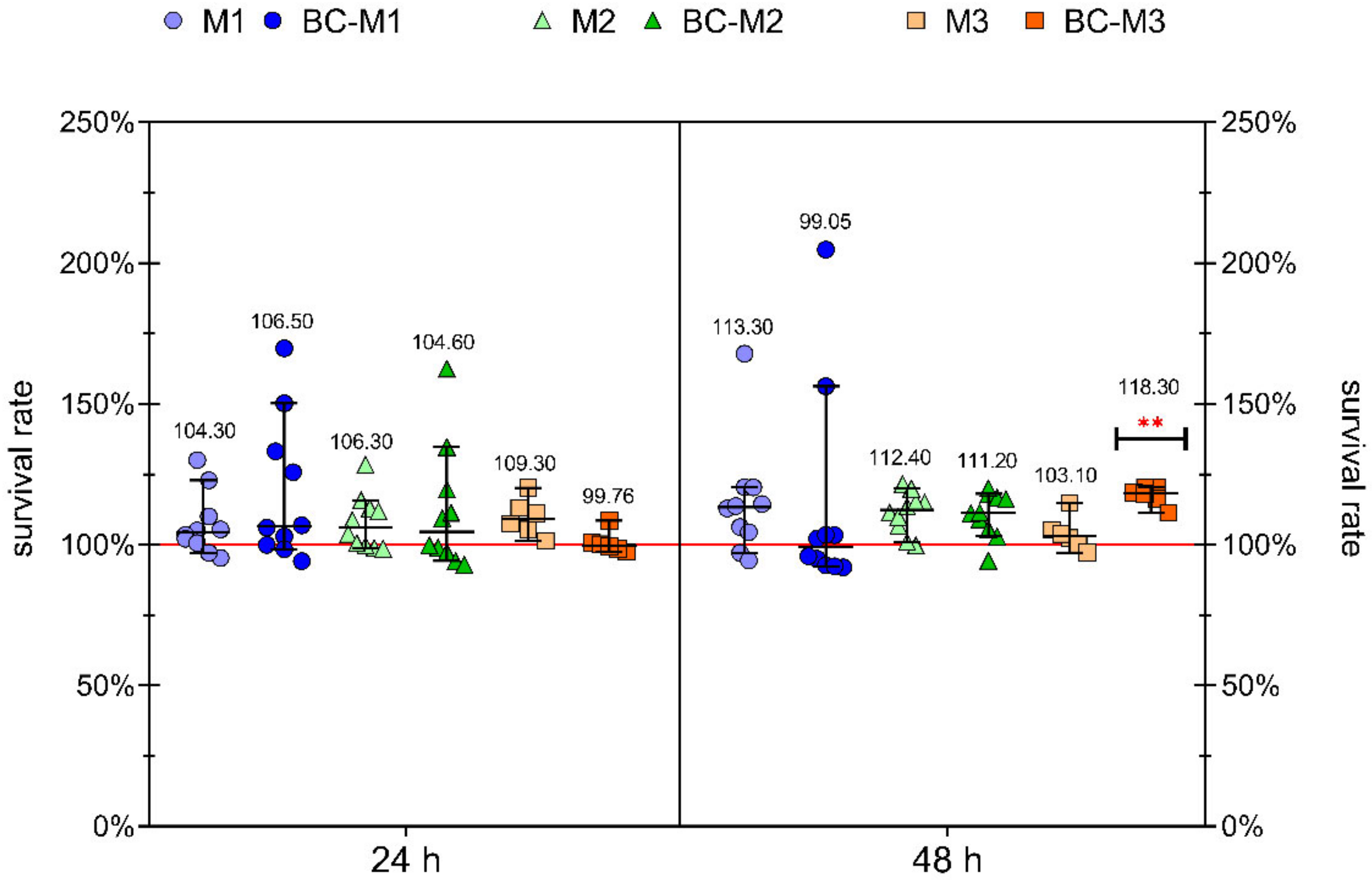
2.2. Cytotoxicity ASSAY
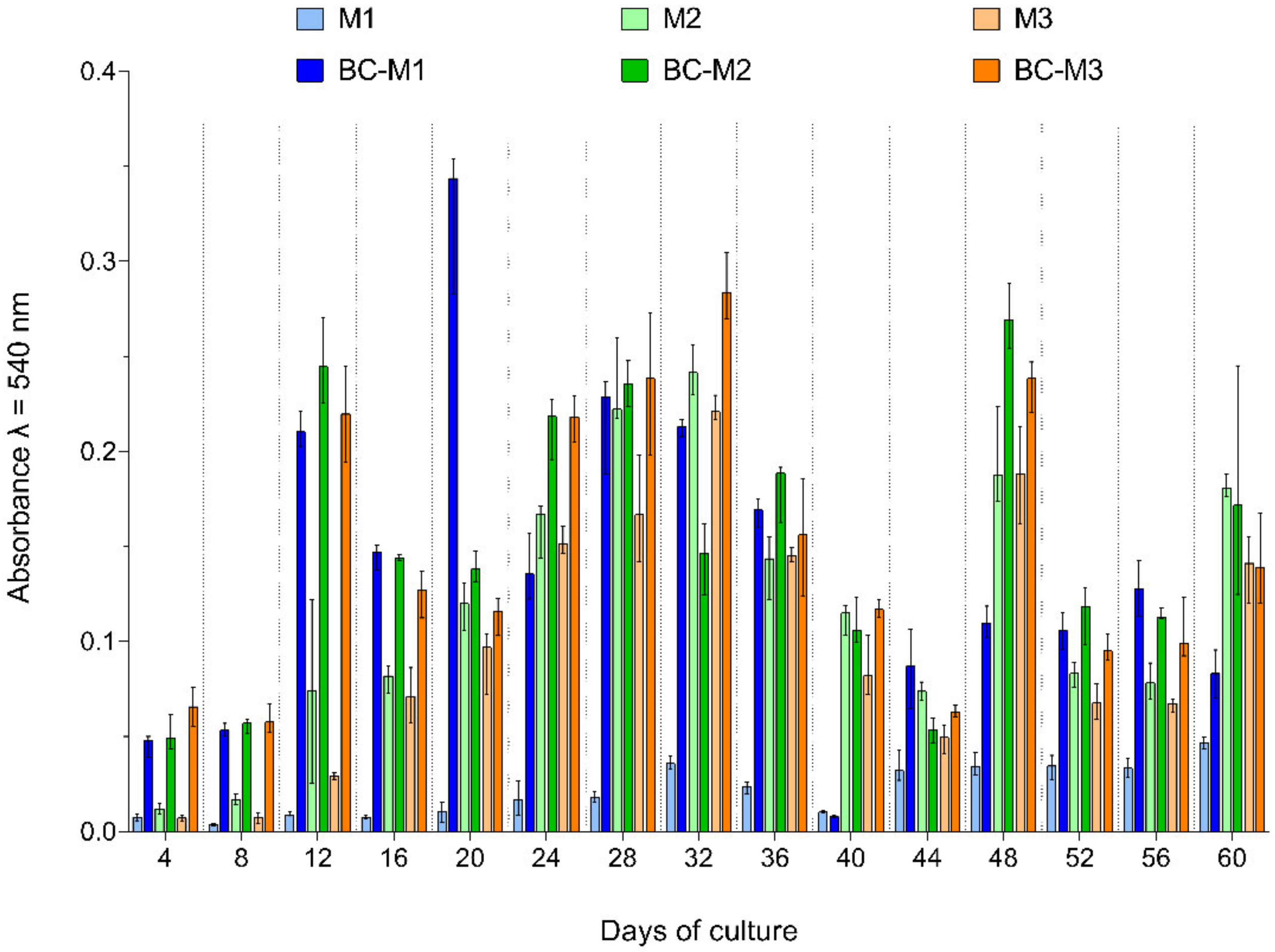
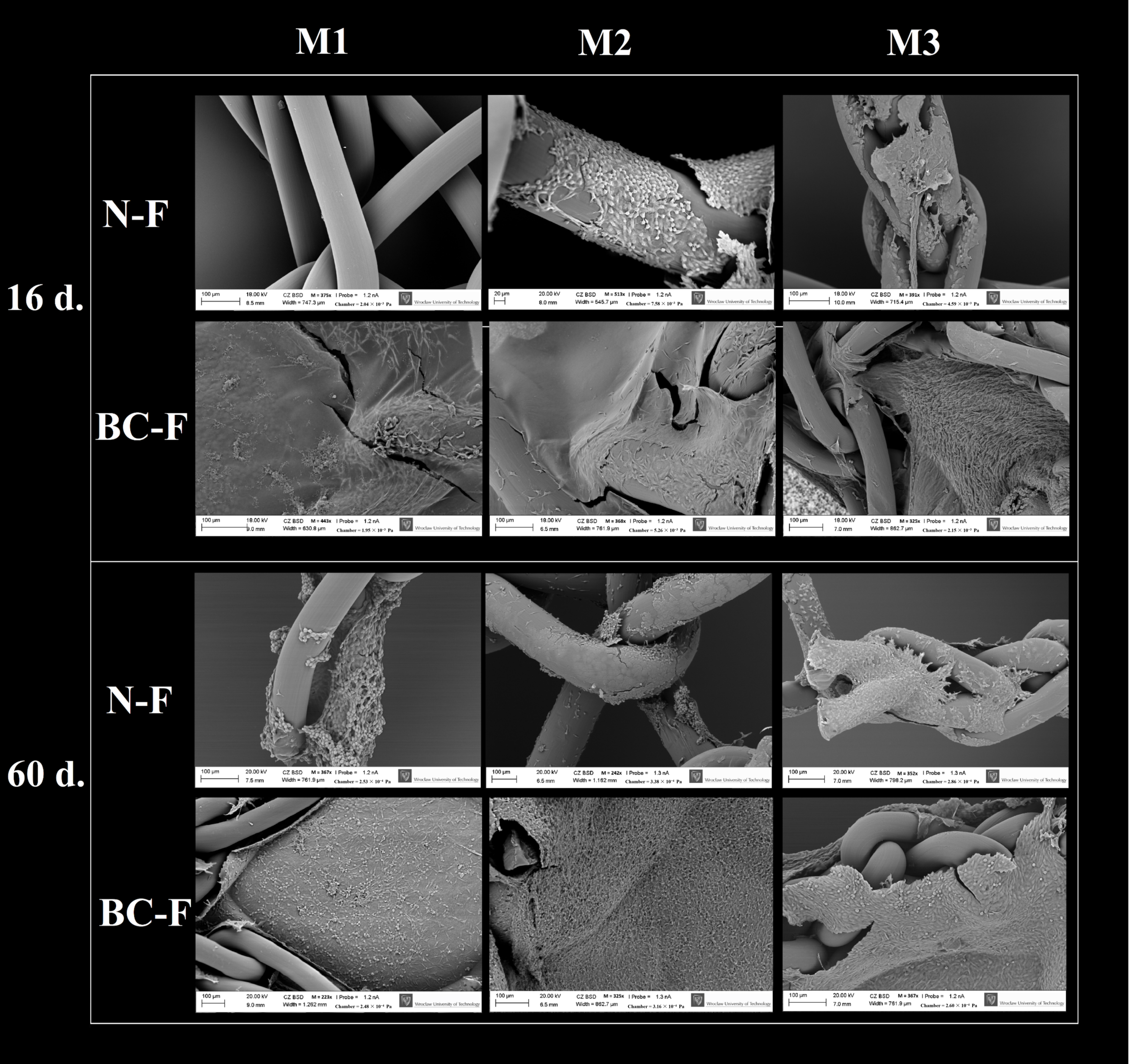
2.3. Cell Colonisation Measurement
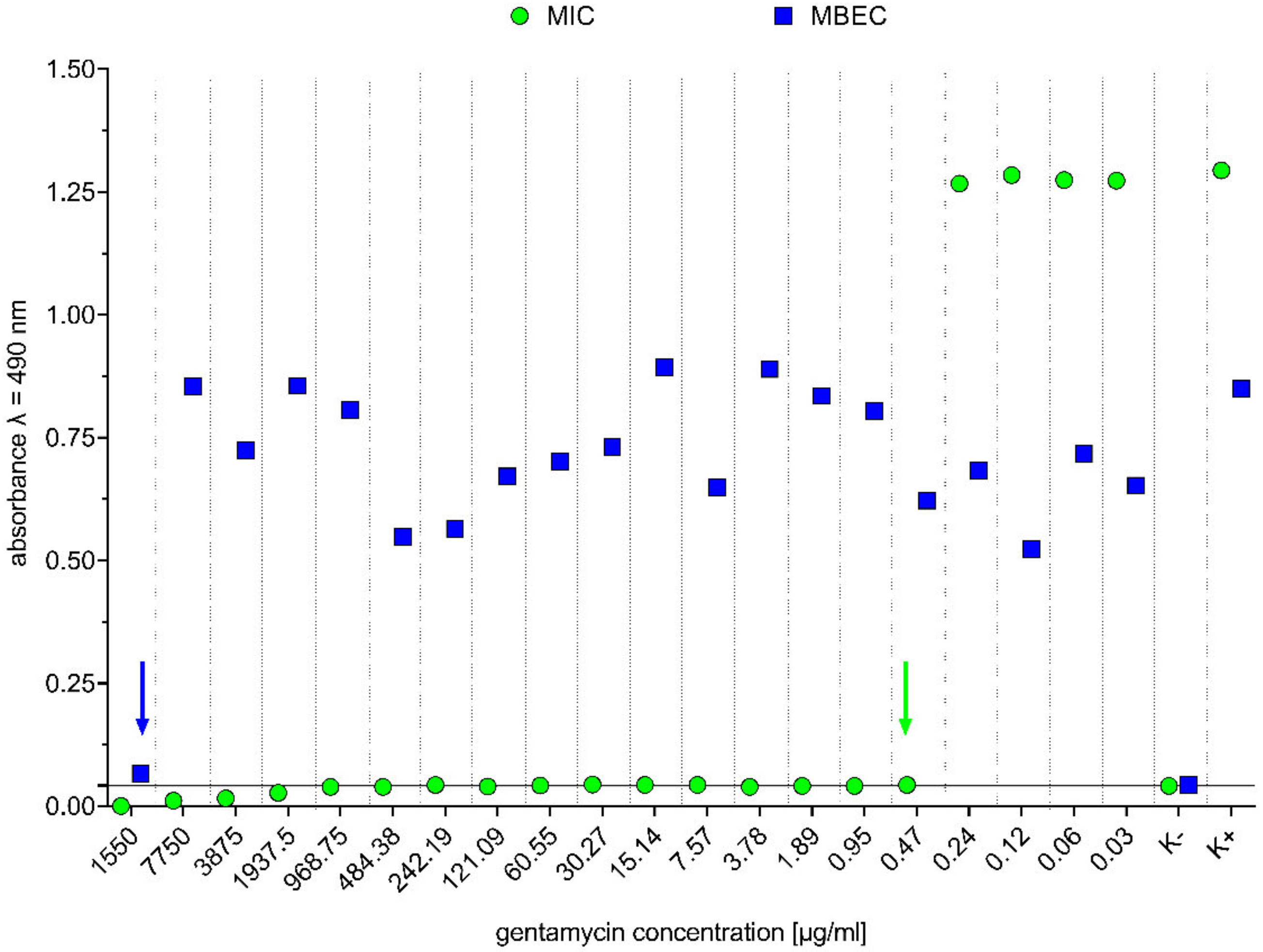
2.4. Determination of Minimal Inhibitory Concentration (MIC) and Minimal Biofilm Eradication Concentration (MBEC) of Gentamicin
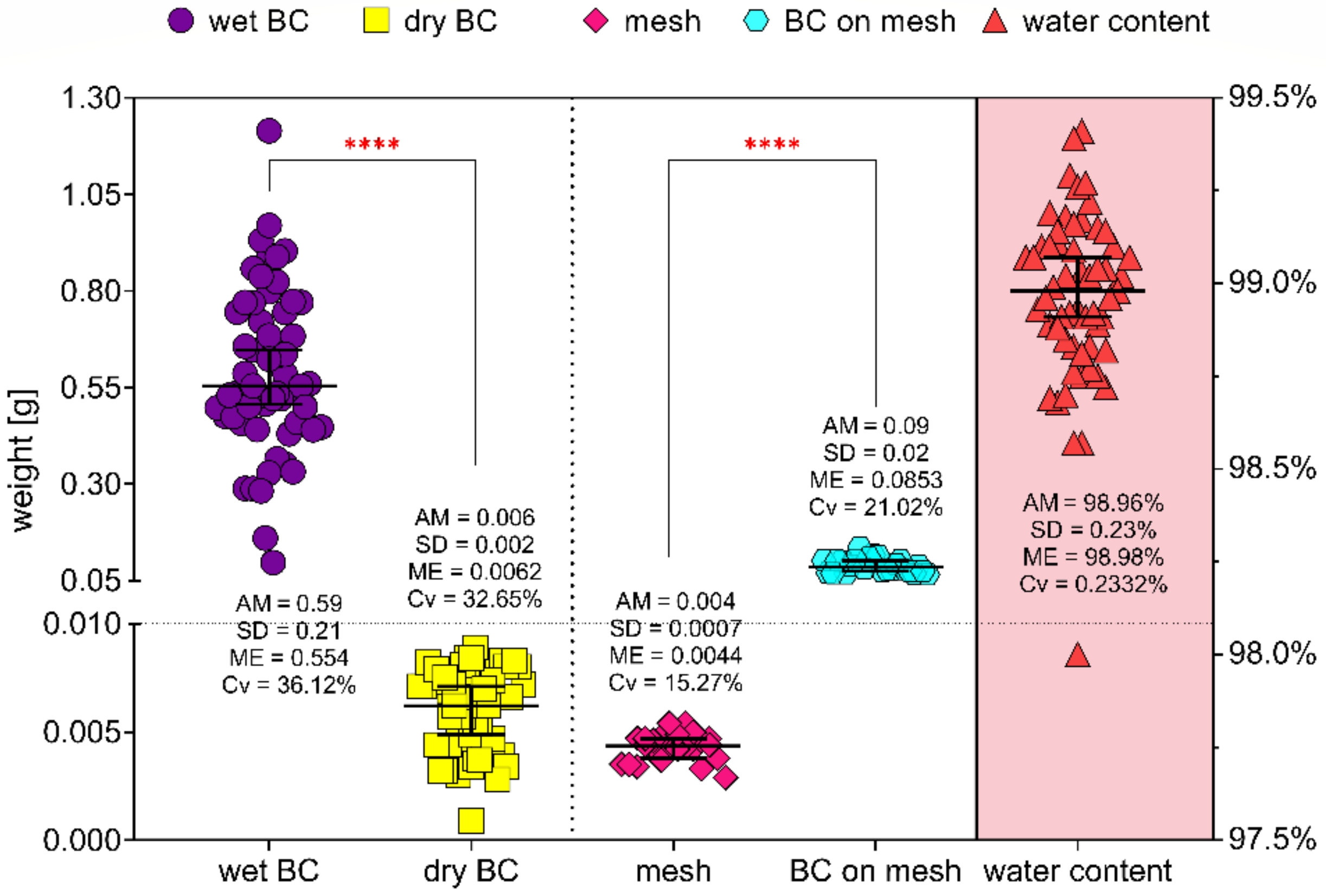
2.5. Bacterial Cellulose Water Content Determination
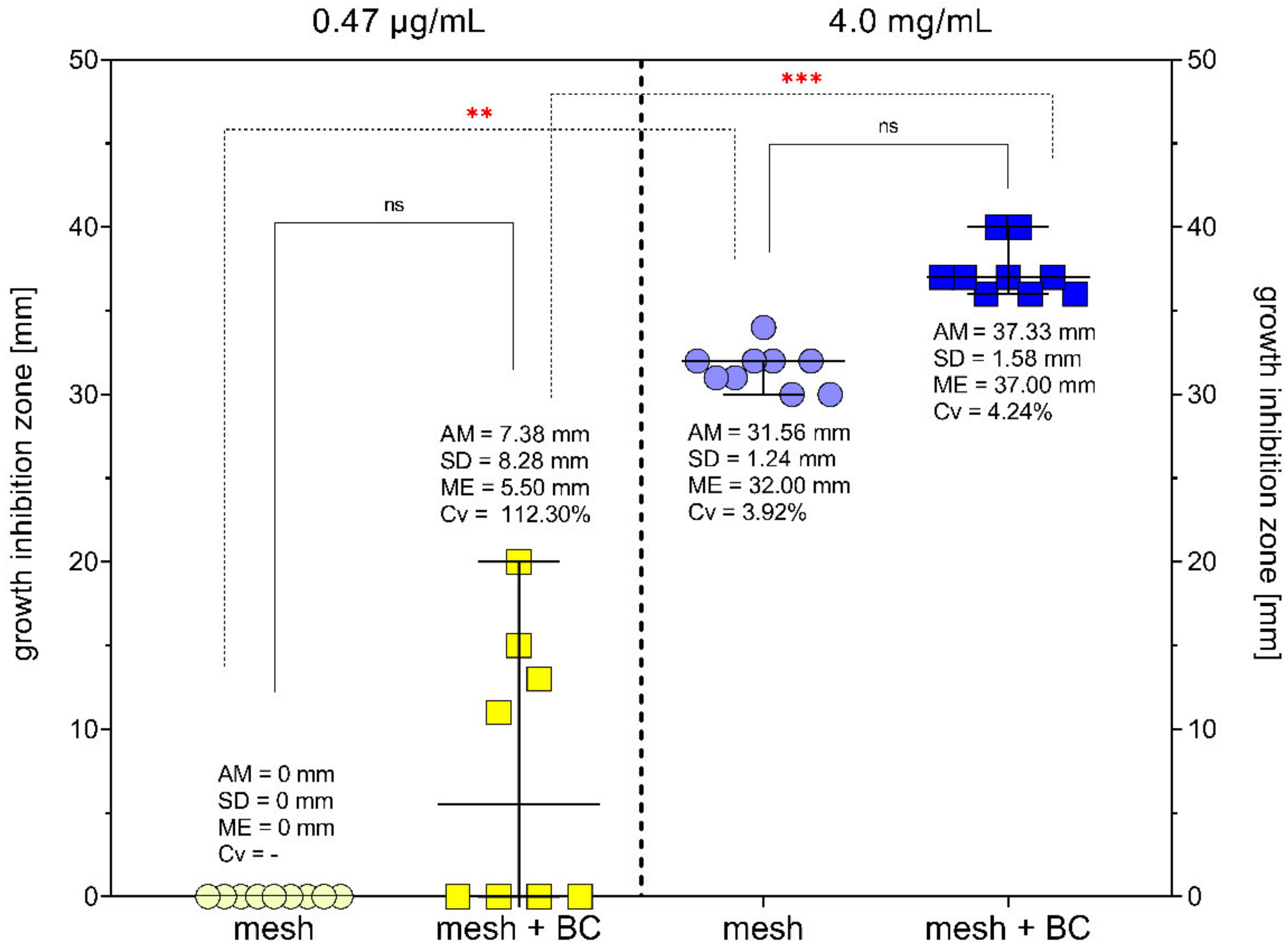
2.6. Modified Disc Diffusion Method
3. Discussion
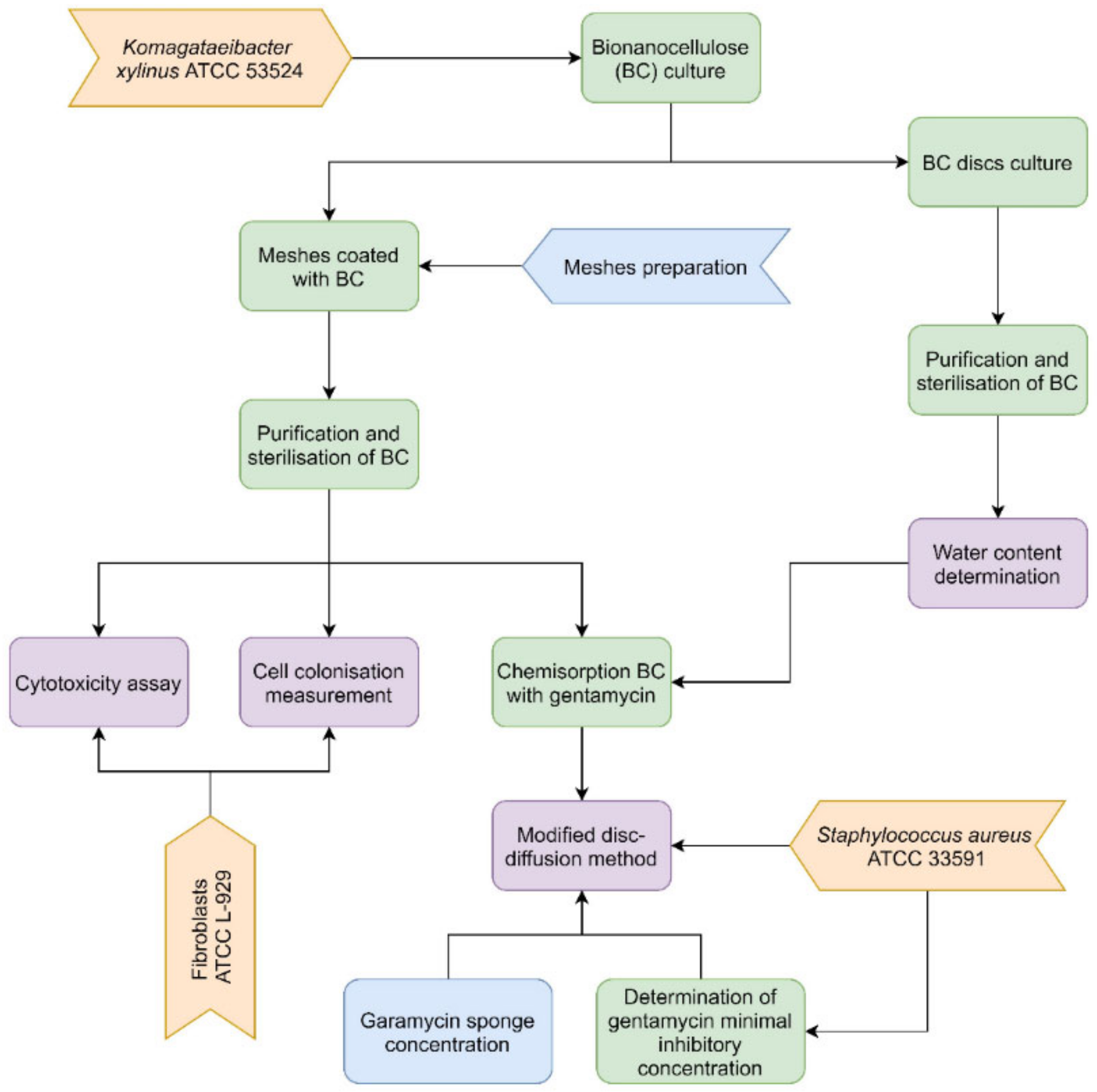
4. Materials and Methods
4.1. Sample Preparation
- non-absorbable mesh made from polypropylene-polyvinylpyrrolidone-polyethylene glycol with adhesive layer (Adhesix™, BARD, New Providence, NJ, USA), later referred to as the M1.
- non-absorbable macroporous mesh made from polypropylene microfilaments (Hermesh 4, Polhernia, Gdansk, Poland), later referred to as the M2.
- non-absorbable macroporous mesh made from polypropylene monofilaments, knitted with quadriaxial technology (Hermesh 8, Herniamesh® S.r.l. Chivasso, Turin, Italy), later referred to as the M3.
4.2. Cytotoxicity Assay
4.3. Cell Colonisation Measurement
4.4. Determination of Minimal Inhibitory Concentration (MIC) and Minimal Biofilm Eradication Concentration (MBEC) of Gentamicin
4.5. Bacterial Cellulose Water Content Determination
4.6. Chemisorption of BC-Coated Meshes with Gentamicin and Determination of Its Release Profile
4.7. Modified Disc Diffusion Method
4.8. Statistical Evaluation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, C.; Liu, D.; Li, F.; Watson, D.I.; Gao, X.; Koetje, J.H.; Luo, T.; Yan, C.; Du, X.; Wang, Z. Systematic review and meta-analysis of laparoscopic mesh versus suture repair of hiatus hernia: Objective and subjective outcomes. Surg. Endosc. 2017, 31, 4913–4922. [Google Scholar] [CrossRef] [Green Version]
- Spiro, C.; Quarmby, N.; Gananadha, S. Mesh-related complications in paraoesophageal repair: A systematic review. Surg. Endosc. 2020, 34, 4257–4280. [Google Scholar] [CrossRef] [PubMed]
- Liang, M.K.; Holihan, J.L.; Itani, K.; Alawadi, Z.M.; Gonzalez, J.R.F.; Askenasy, E.P.; Ballecer, C.; Chong, H.S.; Goldblatt, M.I.; Greenberg, J.A.; et al. Ventral hernia management: Expert consensus guided by systematic review. Ann. Surg. 2017, 265, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-T.; Weng, T.-Y.; Tam, K.-W. Effectiveness and Safety of Mesh Repair for Incarcerated or Strangulated Hernias: A Systematic Review and Meta-Analysis. World J. Surg. 2020, 44, 2176–2184. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Feussner, H. Classical (Open) Surgery. In Biomedical Engineering in Gastrointestinal Surgery; Academic Press: Cambridge, MA, USA, 2017; pp. 221–267. ISBN 9780128032305. [Google Scholar]
- Center for Devices and Radiological Health—FDA. Hernia Surgical Mesh Implants; U.S. Food and Drug Administration: Hampton, VA, USA, 2018; pp. 1–4.
- Mohsina, A.; Kumar, N.; Sharma, A.; Shrivastava, S.; Mathew, D.D.; Remya, V.; Sonal; Maiti, S.; Singh, K. Polypropylene mesh seeded with fibroblasts: A new approach for the repair of abdominal wall defects in rats. Tissue Cell 2017, 49, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Köhler, B.; Benito-Martínez, S.; Rodríguez, M.; García-Moreno, F.; Pascual, G.; Bellón, J.M. Experimental study on the use of a chlorhexidine-loaded carboxymethylcellulose gel as antibacterial coating for hernia repair meshes. Hernia 2019, 23, 789–800. [Google Scholar] [CrossRef]
- Blatnik, J.A.; Thatiparti, T.R.; Krpata, D.M.; Zuckerman, S.T.; Rosen, M.J.; von Recum, H.A. Infection prevention using affinity polymer-coated, synthetic meshes in a pig hernia model. J. Surg. Res. 2017, 219, 5–10. [Google Scholar] [CrossRef]
- Guillaume, O.; Pérez-Tanoira, R.; Fortelny, R.; Redl, H.; Moriarty, T.F.; Richards, R.G.; Eglin, D.; Puchner, A.P. Infections associated with mesh repairs of abdominal wall hernias: Are antimicrobial biomaterials the longed-for solution? Biomaterials 2018, 167, 15–31. [Google Scholar] [CrossRef] [Green Version]
- Kao, A.M.; Arnold, M.R.; Augenstein, V.A.; Heniford, B.T. Prevention and Treatment Strategies for Mesh Infection in Abdominal Wall Reconstruction. Plast. Reconstr. Surg. 2018, 142, 149S–155S. [Google Scholar] [CrossRef]
- Shubinets, V.; Carney, M.J.; Colen, D.L.; Mirzabeigi, M.N.; Weissler, J.M.; Lanni, M.A.; Braslow, B.M.; Fischer, J.P.; Kovach, S.J. Management of Infected Mesh After Abdominal Hernia Repair: Systematic Review and Single-Institution Experience. Ann. Plast. Surg. 2018, 80, 145–153. [Google Scholar] [CrossRef]
- Langbach, O.; Kristoffersen, A.K.; Abesha-Belay, E.; Enersen, M.; Røkke, O.; Olsen, I. Oral, intestinal, and skin bacteria in ventral hernia mesh implants. J. Oral Microbiol. 2016, 8, 31854. [Google Scholar] [CrossRef] [PubMed]
- Ober, I.; Nickerson, D.; Caragea, M.; Ball, C.G.; Kirkpatrick, A.W. Invasive Candida albicans fungal infection requiring explantation of a noncrosslinked porcine derived biologic mesh: A rare but catastrophic complication in abdominal wall reconstruction. Can. J. Surg. 2020, 63, E533–E536. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Xiong, Y.; Chen, J.; Shen, Y. Study of mesh infection management following inguinal hernioplasty with an analysis of risk factors: A 10-year experience. Hernia 2020, 24, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Pande, T.; Naidu, C.S. Mesh infection in cases of polypropylene mesh hernioplasty. Hernia 2020, 24, 849–856. [Google Scholar] [CrossRef]
- Bueno-Lledó, J.; Torregrosa-Gallud, A.; Carreño-Saénz, O.; García-Pastor, P.; Carbonell-Tatay, F.; Bonafé-Diana, S.; Iserte-Hernández, J. Partial versus complete removal of the infected mesh after abdominal wall hernia repair. Am. J. Surg. 2017, 214, 47–52. [Google Scholar] [CrossRef]
- Sharma, R.; Fadaee, N.; Zarrinkhoo, E.; Towfigh, S. Why we remove mesh. Hernia 2018, 22, 953–959. [Google Scholar] [CrossRef]
- Wang, D.; Fu, Y.; Liu, Q.; Chen, J. Maximal Infected Mesh Removal with Methylene Blue Injection for Mesh Infection after Inguinal Hernia Repair. Surg. Infect. 2021, 22, 347–352. [Google Scholar] [CrossRef]
- Pérez-Köhler, B.; Benito-Martínez, S.; Nisa, F.G.-M.; Rodríguez, M.; Pascual, G.; Bellón, J.M. Preclinical bioassay of a novel antibacterial mesh for the repair of abdominal hernia defects. Surgery 2020, 167, 598–608. [Google Scholar] [CrossRef]
- Augimeri, R.V.; Varley, A.J.; Strap, J.L. Establishing a Role for Bacterial Cellulose in Environmental Interactions: Lessons Learned from Diverse Biofilm-Producing Proteobacteria. Front. Microbiol. 2015, 6, 1282. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Walker, K.T.; Ledesma-Amaro, R.; Ellis, T. Engineering Bacterial Cellulose by Synthetic Biology. Int. J. Mol. Sci. 2020, 21, 9185. [Google Scholar] [CrossRef]
- Gorgieva, S.; Trček, J. Bacterial Cellulose: Production, Modification and Perspectives in Biomedical Applications. Nanomaterials 2019, 9, 1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troncoso, O.P.; Torres, F.G. Bacterial Cellulose—Graphene Based Nanocomposites. Int. J. Mol. Sci. 2020, 21, 6532. [Google Scholar] [CrossRef] [PubMed]
- Sulaeva, I.; Henniges, U.; Rosenau, T.; Potthast, A. Bacterial cellulose as a material for wound treatment: Properties and modifications. A review. Biotechnol. Adv. 2015, 33, 1547–1571. [Google Scholar] [CrossRef] [PubMed]
- Pértile, R.A.; Moreira, S.; Gil da Costa, R.M.; Correia, A.; Guãrdao, L.; Gartner, F.; Vilanova, M.; Gama, M. Bacterial Cellulose: Long-Term Biocompatibility Studies. J. Biomater. Sci. Polym. Ed. 2012, 23, 1339–1354. [Google Scholar] [CrossRef] [Green Version]
- Kwak, M.H.; Kim, J.E.; Go, J.; Koh, E.K.; Song, S.H.; Son, H.J.; Kim, H.S.; Yun, Y.H.; Jung, Y.J.; Hwang, D.Y. Bacterial cellulose membrane produced by Acetobacter sp. A10 for burn wound dressing applications. Carbohydr. Polym. 2015, 122, 387–398. [Google Scholar] [CrossRef]
- Jeong, S.I.; Lee, S.E.; Yang, H.; Jin, Y.-H.; Park, C.-S.; Park, Y.S. Toxicologic evaluation of bacterial synthesized cellulose in endothelial cells and animals. Mol. Cell. Toxicol. 2010, 6, 370–377. [Google Scholar] [CrossRef]
- Żywicka, A.; Peitler, D.; Rakoczy, R.; Junka, A.F.; Fijałkowski, K. Wet and Dry Forms of Bacterial Cellulose Synthetized by Different Strains of Gluconacetobacter xylinus as Carriers for Yeast Immobilization. Appl. Biochem. Biotechnol. 2016, 180, 805–816. [Google Scholar] [CrossRef]
- Pacheco, G.; De Mello, C.V.; Chiari-Andréo, B.G.; Isaac, V.L.B.; Ribeiro, S.J.L.; Pecoraro, É.; Trovatti, E. Bacterial cellulose skin masks-Properties and sensory tests. J. Cosmet. Dermatol. 2018, 17, 840–847. [Google Scholar] [CrossRef]
- Wang, X.; Tang, J.; Huang, J.; Hui, M. Production and characterization of bacterial cellulose membranes with hyaluronic acid and silk sericin. Colloids Surfaces B Biointerfaces 2020, 195, 111273. [Google Scholar] [CrossRef]
- Mautner, A.; Bismarck, A. Bacterial nanocellulose papers with high porosity for optimized permeance and rejection of nm-sized pollutants. Carbohydr. Polym. 2021, 251, 117130. [Google Scholar] [CrossRef]
- Ghorbani, M.; Samanian, K.; Afsharpuor, M. Mechanical properties of Bacterial cellulose Nanofibers bio-composite as a long-lasting coating on the paper works. Int. J. Conserv. Sci. 2018, 9, 389–400. [Google Scholar]
- Chan, C.K.; Shin, J.; Jiang, S. Development of Tailor-Shaped Bacterial Cellulose Textile Cultivation Techniques for Zero-Waste Design. Cloth. Text. Res. J. 2018, 36, 33–44. [Google Scholar] [CrossRef]
- Fernandes, M.; Gama, M.; Dourado, F.; Souto, A.P. Development of novel bacterial cellulose composites for the textile and shoe industry. Microb. Biotechnol. 2019, 12, 650–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.; Zhu, J.; Zhang, Q.; Zhan, X.; Chen, F. A Shape Recovery Zwitterionic Bacterial Cellulose Aerogel with Superior Performances for Water Remediation. Langmuir 2019, 35, 11959–11967. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, F.; Sun, Y.; Xu, X.; Chen, X.; Pan, B.; Sun, D.; Qian, J. Bacterial cellulose derived paper-like purifier with multifunctionality for water decontamination. Chem. Eng. J. 2019, 371, 730–737. [Google Scholar] [CrossRef]
- Wang, J.L.; Guo, Y.J.; Li, D.J.; Long, G.D.; Tang, Q.B.; Zu, X.T.; Ma, J.Y.; Du, B.; Tang, Y.L.; Torun, H.; et al. Bacterial cellulose coated ST-cut quartz surface acoustic wave humidity sensor with high sensitivity, fast response and recovery. Smart Mater. Struct. 2020, 29, 045037. [Google Scholar] [CrossRef]
- Wang, J.L.; Guo, Y.J.; Long, G.D.; Tang, Y.L.; Tang, Q.B.; Zu, X.T.; Ma, J.Y.; Du, B.; Torun, H.; Fu, Y.Q. Integrated sensing layer of bacterial cellulose and polyethyleneimine to achieve high sensitivity of ST-cut quartz surface acoustic wave formaldehyde gas sensor. J. Hazard. Mater. 2019, 388, 121743. [Google Scholar] [CrossRef] [PubMed]
- Legnani, C.; Barud, H.S.; Caiut, J.M.A.; Calil, V.L.; Maciel, I.O.; Quirino, W.G.; Ribeiro, S.J.L.; Cremona, M. Transparent bacterial cellulose nanocomposites used as substrate for organic light-emitting diodes. J. Mater. Sci. Mater. Electron. 2019, 30, 16718–16723. [Google Scholar] [CrossRef]
- Cebrian, A.V.S.; Carvalho, R.S.; Barreto, A.R.J.; Maturi, F.E.; Barud, H.S.; Silva, R.R.; Legnani, C.; Cremona, M.; Ribeiro, S.J.L. Development of Conformable Substrates for OLEDs Using Highly Transparent Bacterial Cellulose Modified with Recycled Polystyrene. Adv. Sustain. Syst. 2021, 6, 2000258. [Google Scholar] [CrossRef]
- Padrão, J.; Gonçalves, S.; Silva, J.P.; Sencadas, V.; Lanceros-Mendez, S.; Pinheiro, A.C.; Vicente, A.A.; Rodrigues, L.; Dourado, F. Bacterial cellulose-lactoferrin as an antimicrobial edible packaging. Food Hydrocoll. 2016, 58, 126–140. [Google Scholar] [CrossRef] [Green Version]
- Viana, R.M.; Sá, N.M.; Barros, M.O.; Borges, M.; Azeredo, H.M. Nanofibrillated bacterial cellulose and pectin edible films added with fruit purees. Carbohydr. Polym. 2018, 196, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popa, L.; Ghica, M.V.; Tudoroiu, E.-E.; Ionescu, D.-G.; Dinu-Pîrvu, C.-E. Bacterial Cellulose—A Remarkable Polymer as a Source for Biomaterials Tailoring. Materials 2022, 15, 1054. [Google Scholar] [CrossRef] [PubMed]
- Singhania, R.R.; Patel, A.K.; Tsai, M.-L.; Chen, C.-W.; Di Dong, C. Genetic modification for enhancing bacterial cellulose production and its applications. Bioengineered 2021, 12, 6793–6807. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Jin, J.N.; Kan, E.; Kim, K.J.; Lee, S.H. Bacterial cellulose-chitosan composite hydrogel beads for enzyme immobilization. Biotechnol. Bioprocess Eng. 2017, 22, 89–94. [Google Scholar] [CrossRef]
- Drozd, R.; Rakoczy, R.; Wasak, A.; Junka, A.; Fijałkowski, K. The application of magnetically modified bacterial cellulose for immobilization of laccase. Int. J. Biol. Macromol. 2018, 108, 462–470. [Google Scholar] [CrossRef]
- Picheth, G.F.; Pirich, C.; Sierakowski, M.R.; Woehl, M.A.; Sakakibara, C.N.; de Souza, C.F.; Martin, A.A.; da Silva, R.; de Freitas, R.A. Bacterial cellulose in biomedical applications: A review. Int. J. Biol. Macromol. 2017, 104, 97–106. [Google Scholar] [CrossRef]
- Wang, J.; Tavakoli, J.; Tang, Y. Bacterial cellulose production, properties and applications with different culture methods—A review. Carbohydr. Polym. 2019, 219, 63–76. [Google Scholar] [CrossRef] [Green Version]
- Aditya, T.; Allain, J.P.; Jaramillo, C.; Restrepo, A.M. Surface Modification of Bacterial Cellulose for Biomedical Applications. Int. J. Mol. Sci. 2022, 23, 610. [Google Scholar] [CrossRef]
- Wahid, F.; Huang, L.-H.; Zhao, X.-Q.; Li, W.-C.; Wang, Y.-Y.; Jia, S.-R.; Zhong, C. Bacterial cellulose and its potential for biomedical applications. Biotechnol. Adv. 2021, 53, 107856. [Google Scholar] [CrossRef]
- Oz, Y.E.; Keskin-Erdogan, Z.; Safa, N.; Tuna, E.E.H. A review of functionalised bacterial cellulose for targeted biomedical fields. J. Biomater. Appl. 2021, 36, 648–681. [Google Scholar] [CrossRef]
- Piasecka-Zelga, J.; Zelga, P.; Szulc, J.; Wietecha, J.; Ciechańska, D. An in vivo biocompatibility study of surgical meshes made from bacterial cellulose modified with chitosan. Int. J. Biol. Macromol. 2018, 116, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Ludwicka, K.; Kolodziejczyk, M.; Gendaszewska-Darmach, E.; Chrzanowski, M.; Jędrzejczak-Krzepkowska, M.; Rytczak, P.; Bielecki, S. Stable composite of bacterial nanocellulose and perforated polypropylene mesh for biomedical applications. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 107, 978–987. [Google Scholar] [CrossRef] [PubMed]
- The Surgical Disaster of the Mesh Infection—Global Alliance for Infections in Surgery. Available online: https://infectionsinsurgery.org/the-surgical-disaster-of-the-mesh-infection/?fbclid=IwAR26mrtxbm8MOR_rChMhr0Mu10XbwXV4ETvq1Otc (accessed on 17 January 2022).
- Dydak, K.; Junka, A.; Szymczyk, P.; Chodaczek, G.; Toporkiewicz, M.; Fijałkowski, K.; Dudek, B.; Bartoszewicz, M. Development and biological evaluation of Ti6Al7Nb scaffold implants coated with gentamycin-saturated bacterial cellulose biomaterial. PLoS ONE 2018, 13, e0205205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Junka, A.; Bartoszewicz, M.; Dziadas, M.; Szymczyk, P.; Dydak, K.; Żywicka, A.; Owczarek, A.; Bil-Lula, I.; Czajkowska, J.; Fijałkowski, K. Application of bacterial cellulose experimental dressings saturated with gentamycin for management of bone biofilm in vitro and ex vivo. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Krasowski, G.; Junka, A.; Paleczny, J.; Czajkowska, J.; Makomaska-Szaroszyk, E.; Chodaczek, G.; Majkowski, M.; Migdał, P.; Fijałkowski, K.; Kowalska-Krochmal, B.; et al. In Vitro Evaluation of Polihexanide, Octenidine and NaClO/HClO-Based Antiseptics against Biofilm Formed by Wound Pathogens. Membranes 2021, 11, 62. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.-D.; Yang, H.; Park, H.R.; Park, C.-S.; Park, Y.S.; Lee, S.E. Evaluation of immunoreactivity of in vitro and in vivo models against bacterial synthesized cellulose to be used as a prosthetic biomaterial. BioChip J. 2013, 7, 201–209. [Google Scholar] [CrossRef]
- Volova, T.G.; Prudnikova, S.V.; Sukovatyi, A.G.; Shishatskaya, E.I. Production and properties of bacterial cellulose by the strain Komagataeibacter xylinus B-12068. Appl. Microbiol. Biotechnol. 2018, 102, 7417–7428. [Google Scholar] [CrossRef] [Green Version]
- Goldschmidt, E.; Cacicedo, M.; Kornfeld, S.; Valinoti, M.; Ielpi, M.; Ajler, P.M.; Yampolsky, C.; Rasmussen, J.; Castro, G.R.; Argibay, P. Construction andin vitrotesting of a cellulose dura mater graft. Neurol. Res. 2016, 38, 25–31. [Google Scholar] [CrossRef]
- Lai, C.; Hu, K.S.; Wang, Q.L.; Sheng, L.Y.; Zhang, S.J.; Zhang, Y. Anti-Adhesion Mesh for Hernia Repair Based on Modified Bacterial Cellulose. Starch/Staerke 2018, 70, 1700319. [Google Scholar] [CrossRef]
- Zharikov, A.N.; Lubyansky, V.G.; Gladysheva, E.K.; Skiba, E.A.; Budaeva, V.V.; Semyonova, E.N.; Sakovich, G.V. Early morphological changes in tissues when replacing abdominal wall defects by bacterial nanocellulose in experimental trials. J. Mater. Sci. Mater. Med. 2018, 29, 95. [Google Scholar] [CrossRef]
- Helenius, G.; Bäckdahl, H.; Bodin, A.; Nannmark, U.; Gatenholm, P.; Risberg, B. In vivo biocompatibility of bacterial cellulose. J. Biomed. Mater. Res. Part A 2006, 76, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.; Zhang, S.-J.; Chen, X.-C.; Sheng, L.-Y.; Qi, T.-W.; Yan, L.-P. Development of a cellulose-based prosthetic mesh for pelvic organ prolapse treatment: In vivo long-term evaluation in an ewe vagina model. Mater. Today Bio 2021, 12, 100172. [Google Scholar] [CrossRef] [PubMed]
- Ai, F.-F.; Mao, M.; Zhang, Y.; Kang, J.; Zhu, L. Experimental study of a new original mesh developed for pelvic floor reconstructive surgery. Int. Urogynecol. J. 2020, 31, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Żywicka, A.; Wenelska, K.; Junka, A.; Chodaczek, G.; Szymczyk, P.; Fijałkowski, K. Immobilization pattern of morphologically different microorganisms on bacterial cellulose membranes. World J. Microbiol. Biotechnol. 2019, 35, 11. [Google Scholar] [CrossRef]
- Maczynska, B.; Secewicz, A.; Smutnicka, D.; Szymczyk-Ziółkowska, P.; Dudek-Wicher, R.; Junka, A.; Bartoszewicz, M. In vitro efficacy of gentamicin released from collagen sponge in eradication of bacterial biofilm preformed on hydroxyapatite surface. PLoS ONE 2019, 14, e0217769. [Google Scholar] [CrossRef]
- Rebelo, A.R.; Archer, A.J.; Chen, X.; Liu, C.; Yang, G.; Liu, Y. Dehydration of bacterial cellulose and the water content effects on its viscoelastic and electrochemical properties. Sci. Technol. Adv. Mater. 2018, 19, 203–211. [Google Scholar] [CrossRef]
- Zhong, C. Industrial-Scale Production and Applications of Bacterial Cellulose. Front. Bioeng. Biotechnol. 2020, 8, 605374. [Google Scholar] [CrossRef]
- Dugan, J.M.; E Gough, J.; Eichhorn, S.J. Bacterial cellulose scaffolds and cellulose nanowhiskers for tissue engineering. Nanomedicine 2013, 8, 287–298. [Google Scholar] [CrossRef]
- Stevanović, M.; Đošić, M.; Janković, A.; Kojić, V.; Vukašinović-Sekulić, M.; Stojanović, J.; Odović, J.; Sakač, M.C.; Rhee, K.Y.; Mišković-Stanković, V. Gentamicin-Loaded Bioactive Hydroxyapatite/Chitosan Composite Coating Electrodeposited on Titanium. ACS Biomater. Sci. Eng. 2018, 4, 3994–4007. [Google Scholar] [CrossRef]
- Kılınç, S.; Tunç, T.; Pazarcı, Ö.; Sümer, Z. Research into biocompatibility and cytotoxicity of daptomycin, gentamicin, vancomycin and teicoplanin antibiotics at common doses added to bone cement. Jt. Dis. Relat. Surg. 2020, 31, 328–334. [Google Scholar] [CrossRef]
- Wójcik, M.; Wilczyńska, A.; Vivcharenko, V.; Kazimierczak, P.; Adaszek, Ł.; Przekora, A. Bioactive curdlan/agarose dressing enriched with gentamicin for infected wounds—Pilot studies. Eng. Biomater. 2021, 2021, 2–7. [Google Scholar] [CrossRef]
- Portela, R.; Leal, C.R.; Almeida, P.L.; Sobral, R.G. Bacterial cellulose: A versatile biopolymer for wound dressing applications. Microb. Biotechnol. 2019, 12, 586–610. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Wu, J.; Xu, J.; Mosselhy, D.A.; Zheng, Y.; Yang, S. Bacterial Cellulose: Functional Modification and Wound Healing Applications. Adv. Wound Care 2021, 10, 623–640. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, T.; Guedes, G.; Sousa, F.L.; Freire, C.S.R.; Santos, H.A. Latest Advances on Bacterial Cellulose-Based Materials for Wound Healing, Delivery Systems, and Tissue Engineering. Biotechnol. J. 2019, 14, e1900059. [Google Scholar] [CrossRef]
- Dydak, K.; Junka, A.; Dydak, A.; Brożyna, M.; Paleczny, J.; Fijalkowski, K.; Kubielas, G.; Aniołek, O.; Bartoszewicz, M. In Vitro Efficacy of Bacterial Cellulose Dressings Chemisorbed with Antiseptics against Biofilm Formed by Pathogens Isolated from Chronic Wounds. Int. J. Mol. Sci. 2021, 22, 3996. [Google Scholar] [CrossRef]
- Liu, S.; Chu, M.; Zhu, Y.; Li, L.; Wang, L.; Gao, H.; Ren, L. A novel antibacterial cellulose based biomaterial for hernia mesh applications. RSC Adv. 2017, 7, 11601–11607. [Google Scholar] [CrossRef] [Green Version]
- ISO 10993-5:2009; Biological Evaluation of Medical Devices—Part 5: Tests for in Vitro Cytotoxicity. International Organization for Standardization (ISO): Geneva, Switzerland, 2009. Available online: https://www.iso.org/standard/36406.html (accessed on 12 May 2021).








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dydak, K.; Junka, A.; Nowacki, G.; Paleczny, J.; Szymczyk-Ziółkowska, P.; Górzyńska, A.; Aniołek, O.; Bartoszewicz, M. In Vitro Cytotoxicity, Colonisation by Fibroblasts and Antimicrobial Properties of Surgical Meshes Coated with Bacterial Cellulose. Int. J. Mol. Sci. 2022, 23, 4835. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23094835
Dydak K, Junka A, Nowacki G, Paleczny J, Szymczyk-Ziółkowska P, Górzyńska A, Aniołek O, Bartoszewicz M. In Vitro Cytotoxicity, Colonisation by Fibroblasts and Antimicrobial Properties of Surgical Meshes Coated with Bacterial Cellulose. International Journal of Molecular Sciences. 2022; 23(9):4835. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23094835
Chicago/Turabian StyleDydak, Karolina, Adam Junka, Grzegorz Nowacki, Justyna Paleczny, Patrycja Szymczyk-Ziółkowska, Aleksandra Górzyńska, Olga Aniołek, and Marzenna Bartoszewicz. 2022. "In Vitro Cytotoxicity, Colonisation by Fibroblasts and Antimicrobial Properties of Surgical Meshes Coated with Bacterial Cellulose" International Journal of Molecular Sciences 23, no. 9: 4835. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23094835