
Mitochondrial DNA Together with miR-142-3p in Plasma Can Predict Unfavorable Outcomes in Patients after Acute Myocardial Infarction

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Plasma Parameters of STEMI Patients; Variation at 6-Month Follow-Up
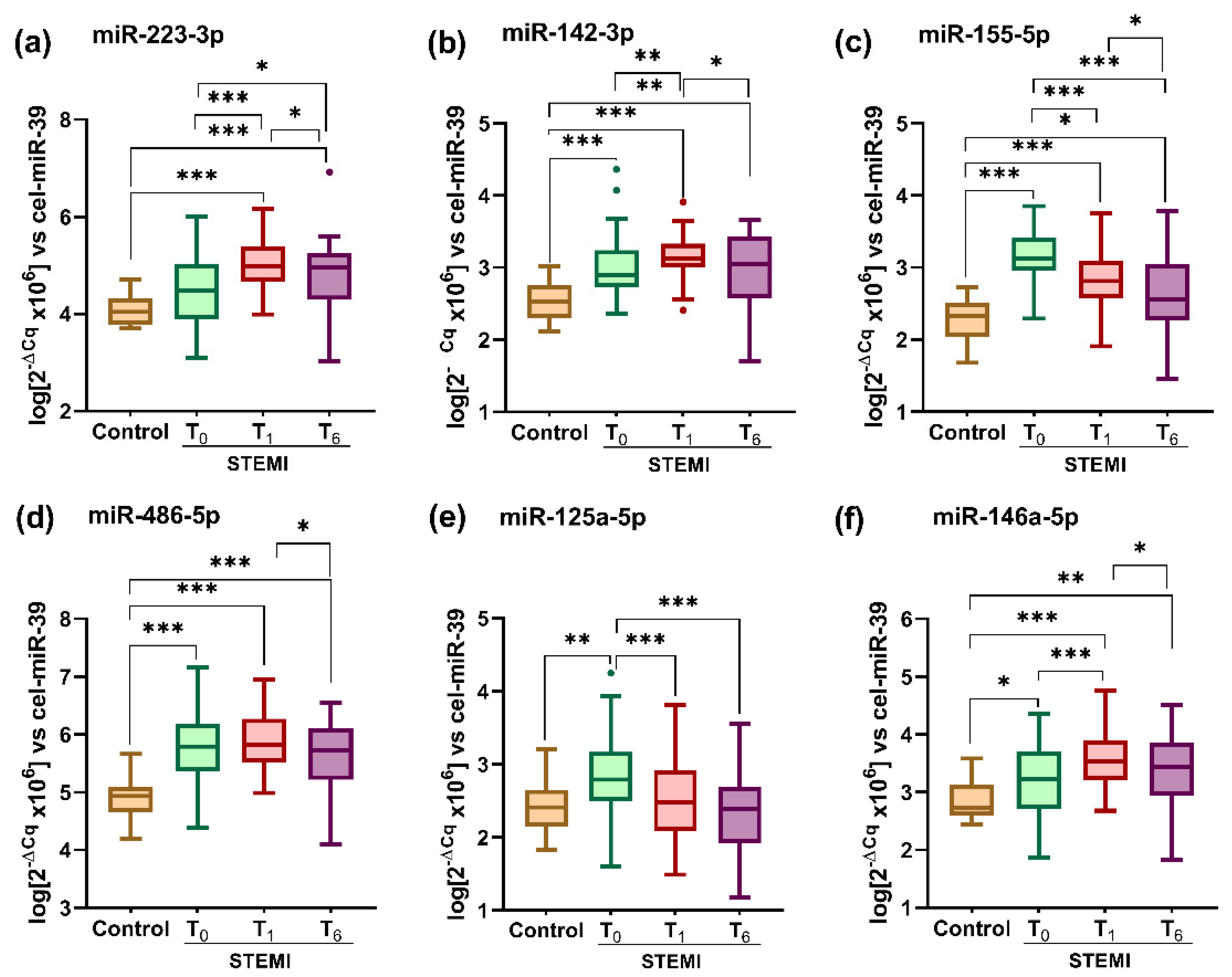
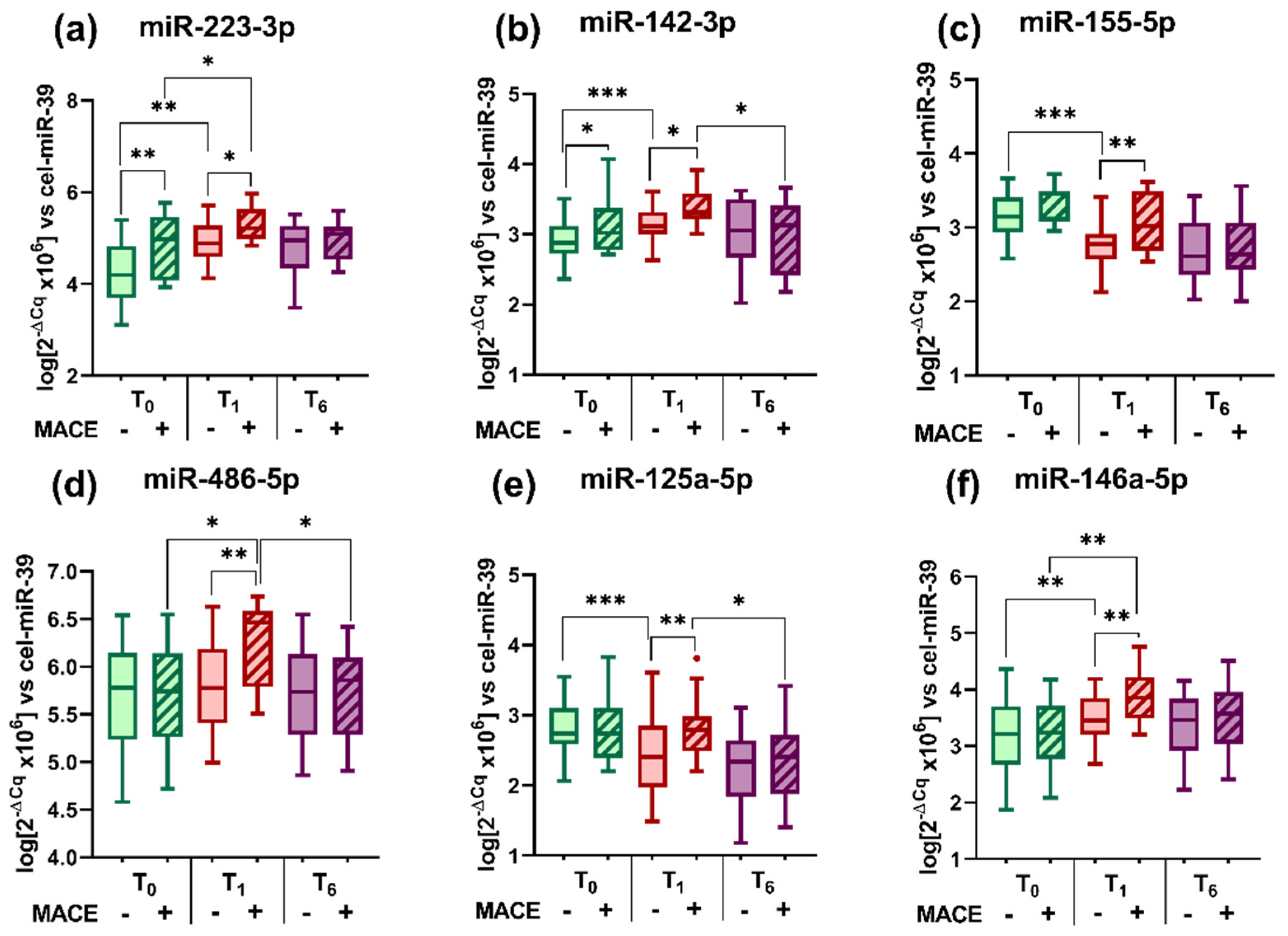
2.2. Plasma Levels of miRNAs in STEMI Patients; Variation at 6-Month Follow-Up
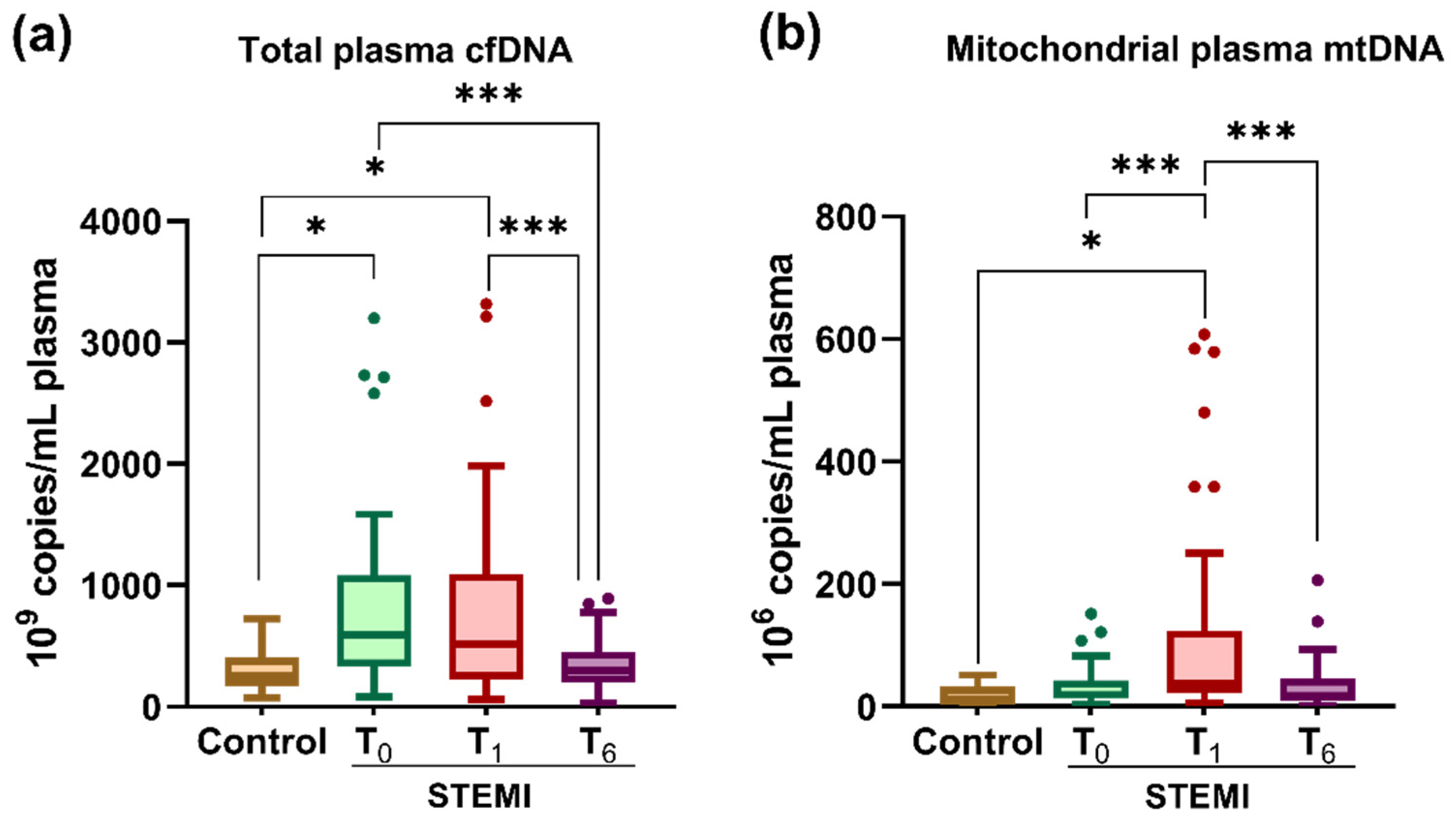
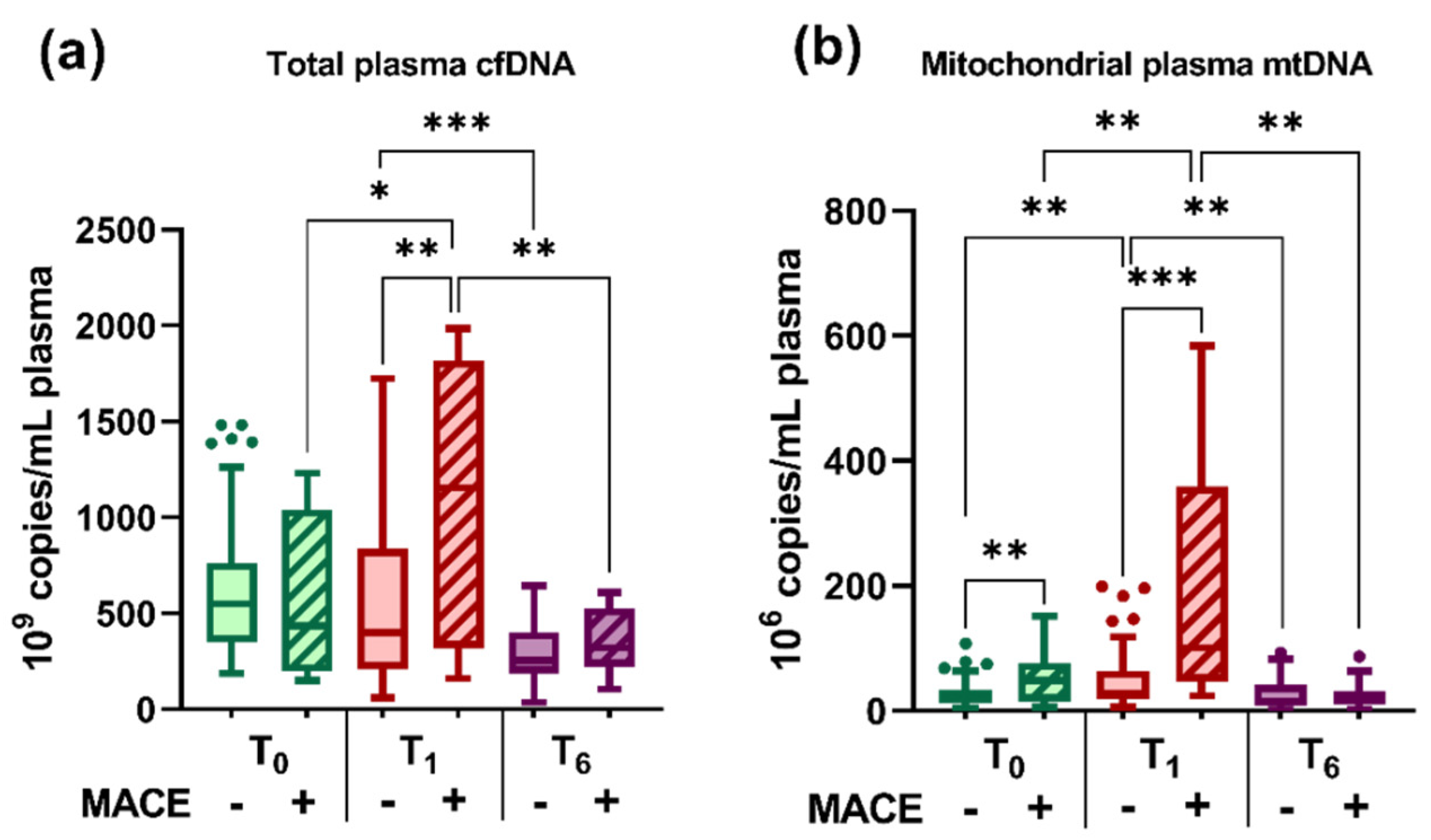
2.3. Plasma Levels of cfDNA and mtDNA in STEMI Patients; Variation at the 6-Month Follow-Up
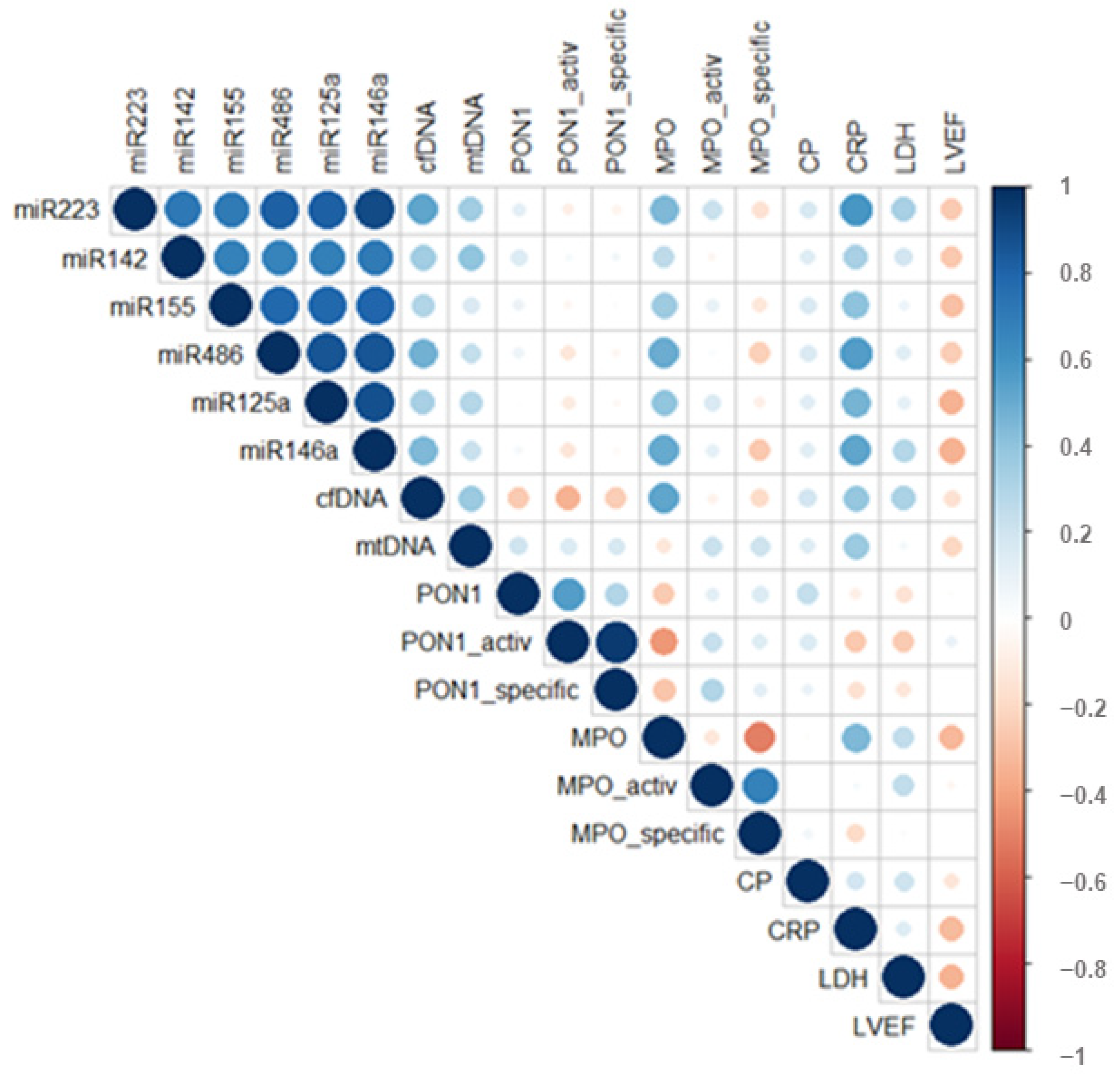
2.4. Correlations between Plasma Levels of miRNAs, cfDNA, mtDNA, and Main Plasma Parameters of STEMI Patients
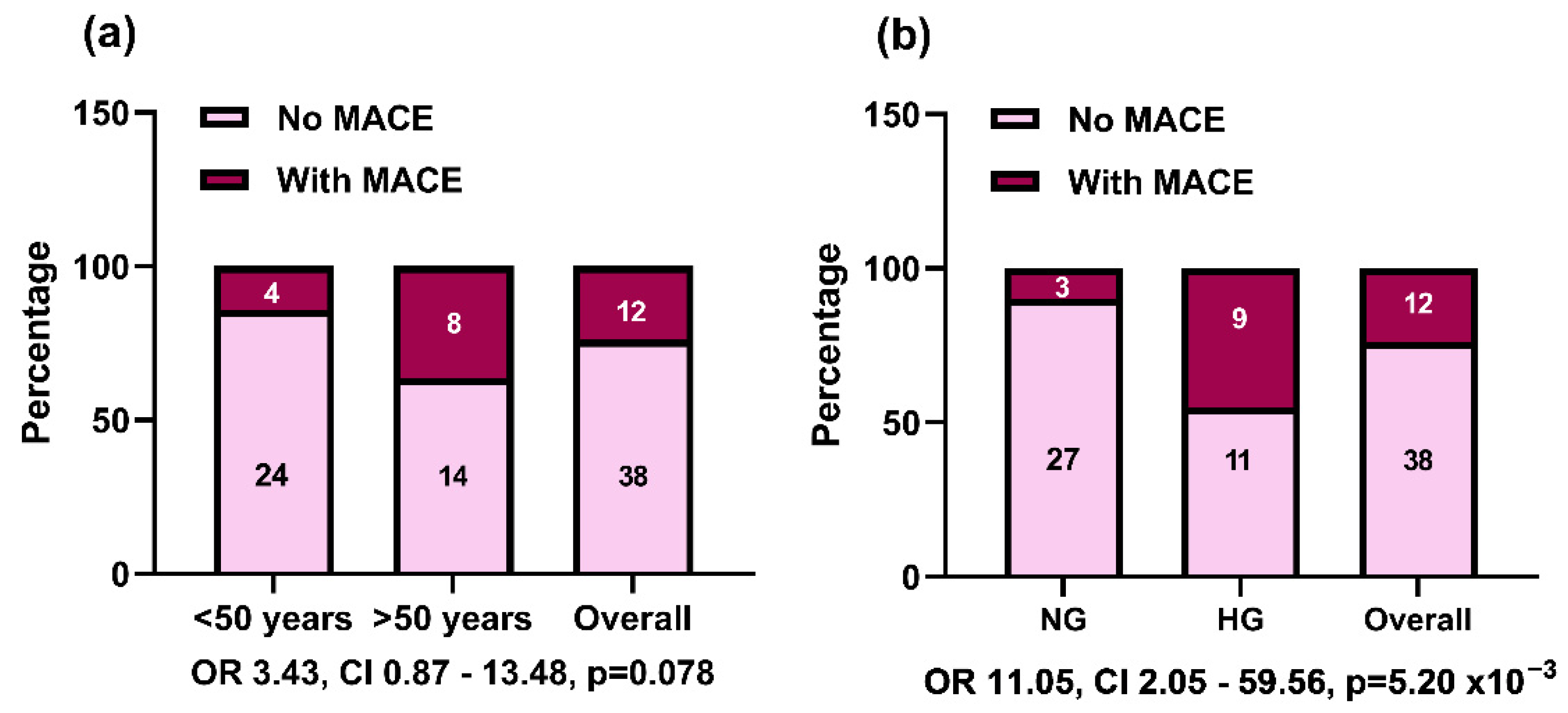
2.5. Clinical Parameters Associated with MACE at the 6-Month Follow-Up
2.6. Plasma Parameters Associated with MACE at the 6-Month Follow-Up
2.7. Association of Plasma miRNA Levels with MACE at the 6-Month Follow-Up
2.8. Association of Plasma cfDNA and mtDNA Levels with MACE at the 6-Month Follow-Up
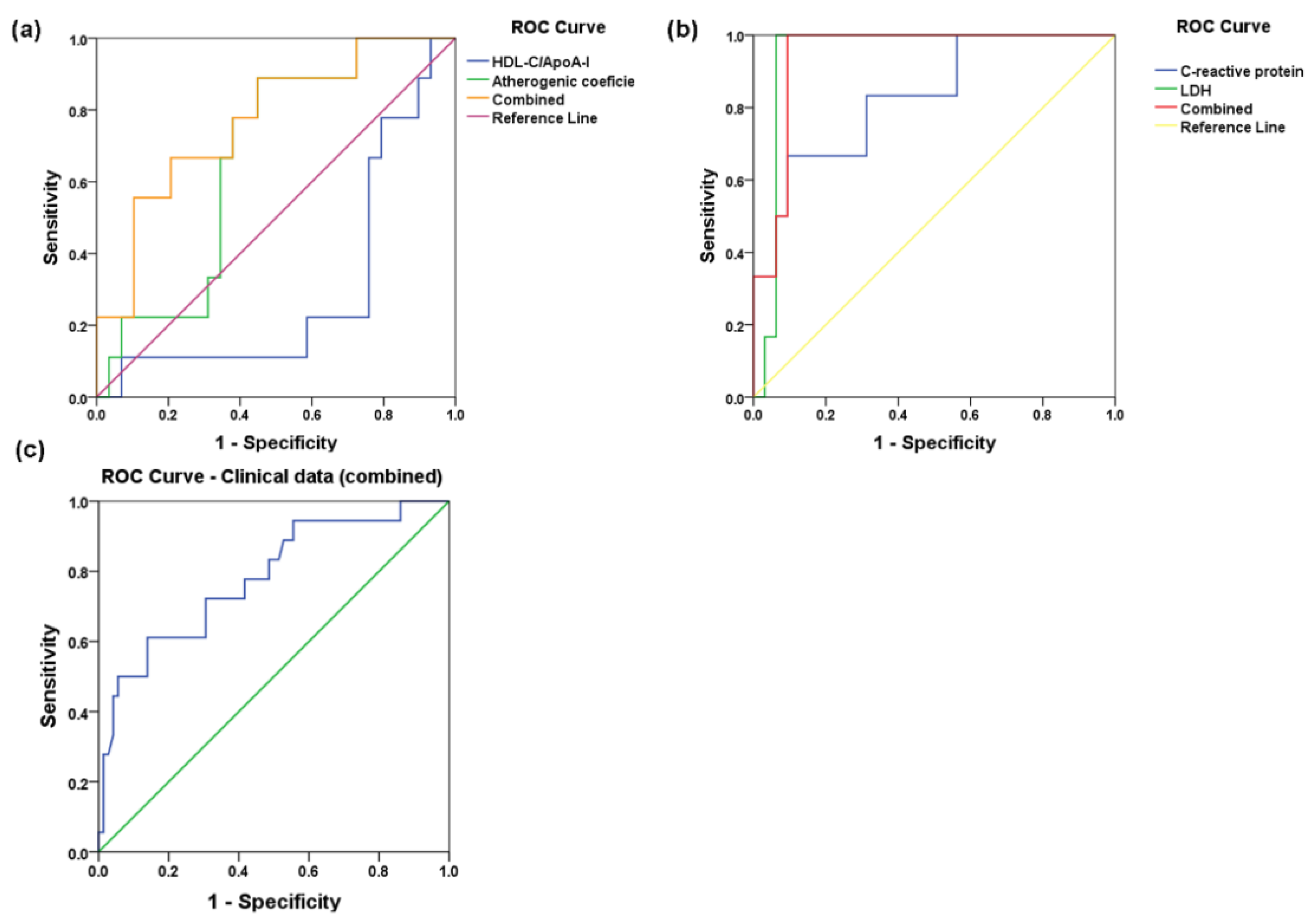
2.9. Statistical Associations of Plasma Biochemical and Cardiac Parameters with Subsequent MACE in STEMI Patients
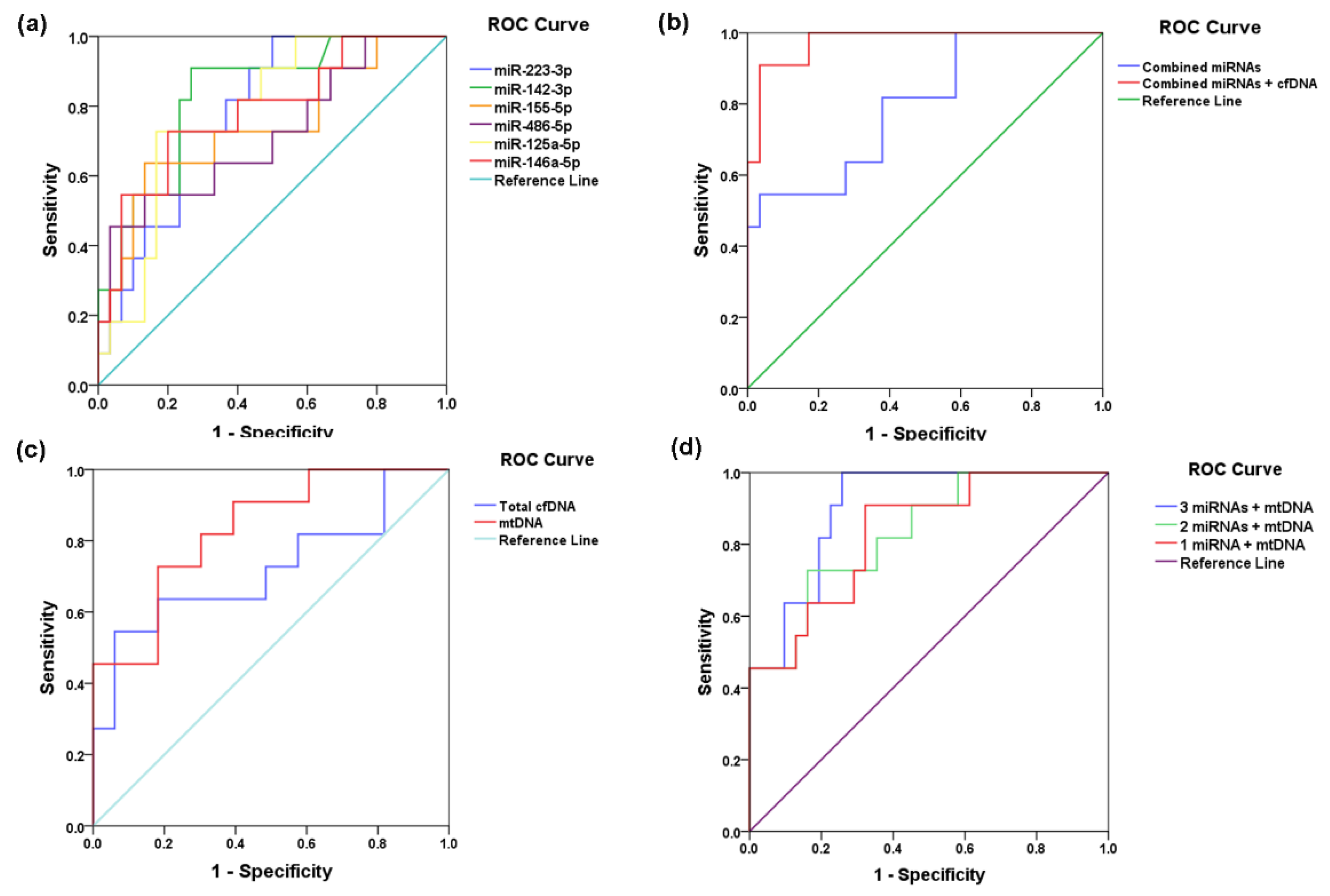
2.10. Plasma-Selected miRNA, cfDNA, and mtDNA Levels as Predictors for Subsequent MACE in STEMI Patients
3. Discussion
4. Materials and Methods
4.1. Study Design: STEMI Patients and Control Group
4.2. Determination of Plasma Parameters of STEMI Patients and Controls
4.3. Analysis of microRNAs in the Plasma of STEMI Patients and Controls
4.4. Analysis of cfDNA and mtDNA in the Plasma of STEMI Patients and Controls
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poudel, I.; Tejpal, C.; Rashid, H.; Jahan, N. Major Adverse Cardiovascular Events: An Inevitable Outcome of ST-elevation myocardial infarction? A Literature Review. Cureus 2019, 11, e5280. [Google Scholar] [CrossRef] [PubMed]
- Shadel, G.S.; Horvath, T.L. Mitochondrial ROS signaling in organismal homeostasis. Cell 2015, 163, 560–569. [Google Scholar] [CrossRef] [PubMed]
- West, A.P.; Shadel, G.S. Mitochondrial DNA in innate immune responses and inflammatory pathology. Nat. Rev. Immunol. 2017, 17, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Oka, T.; Hikoso, S.; Yamaguchi, O.; Taneike, M.; Takeda, T.; Tamai, T.; Oyabu, J.; Murakawa, T.; Nakayama, H.; Nishida, K.; et al. Mitochondrial DNA that escapes from autophagy causes inflammation and heart failure. Nature 2012, 485, 251–255. [Google Scholar] [CrossRef]
- Borissoff, J.I.; Joosen, I.A.; Versteylen, M.O.; Brill, A.; Fuchs, T.A.; Savchenko, A.S.; Gallant, M.; Martinod, K.; Ten Cate, H.; Hofstra, L.; et al. Elevated levels of circulating DNA and chromatin are independently associated with severe coronary atherosclerosis and a prothrombotic state. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2032–2040. [Google Scholar] [CrossRef]
- Liu, L.P.; Cheng, K.; Ning, M.A.; Li, H.H.; Wang, H.C.; Li, F.; Chen, S.Y.; Qu, F.L.; Guo, W.Y. Association between peripheral blood cells mitochondrial DNA content and severity of coronary heart disease. Atherosclerosis 2017, 261, 105–110. [Google Scholar] [CrossRef]
- Xie, J.; Yang, J.; Hu, P. Correlations of Circulating Cell-Free DNA With Clinical Manifestations in Acute Myocardial Infarction. Am. J. Med. Sci. 2018, 356, 121–129. [Google Scholar] [CrossRef]
- Vecoli, C.; Borghini, A.; Pulignani, S.; Mercuri, A.; Turchi, S.; Carpeggiani, C.; Picano, E.; Andreassi, M.G. Prognostic value of mitochondrial DNA(4977) deletion and mitochondrial DNA copy number in patients with stable coronary artery disease. Atherosclerosis 2018, 276, 91–97. [Google Scholar] [CrossRef]
- Devaux, Y.; Vausort, M.; Goretti, E.; Nazarov, P.V.; Azuaje, F.; Gilson, G.; Corsten, M.F.; Schroen, B.; Lair, M.L.; Heymans, S.; et al. Use of circulating microRNAs to diagnose acute myocardial infarction. Clin. Chem. 2012, 58, 559–567. [Google Scholar] [CrossRef]
- de Gonzalo-Calvo, D.; Perez-Boza, J.; Curado, J.; Devaux, Y.; EU-CardioRNA COST Action CA17129. Challenges of microRNA-based biomarkers in clinical application for cardiovascular diseases. Clin. Transl. Med. 2022, 12, e585. [Google Scholar] [CrossRef]
- Barbalata, T.; Moraru, O.E.; Stancu, C.S.; Sima, A.V.; Niculescu, L.S. MiR-223-3p levels in the plasma and atherosclerotic plaques are increased in aged patients with carotid artery stenosis; association with HDL-related proteins. Mol. Biol Rep. 2021, 49, 6779–6788. [Google Scholar] [CrossRef] [PubMed]
- Barbalata, T.; Moraru, O.E.; Stancu, C.S.; Devaux, Y.; Simionescu, M.; Sima, A.V.; Niculescu, L.S. Increased miR-142 Levels in Plasma and Atherosclerotic Plaques from Peripheral Artery Disease Patients with Post-Surgery Cardiovascular Events. Int. J. Mol. Sci. 2020, 21, 9600. [Google Scholar] [CrossRef] [PubMed]
- Niculescu, L.S.; Simionescu, N.; Sanda, G.M.; Carnuta, M.G.; Stancu, C.S.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; Simionescu, M.; et al. MiR-486 and miR-92a Identified in Circulating HDL Discriminate between Stable and Vulnerable Coronary Artery Disease Patients. PLoS ONE 2015, 10, e0140958. [Google Scholar] [CrossRef] [PubMed]
- Simionescu, N.; Niculescu, L.S.; Carnuta, M.G.; Sanda, G.M.; Stancu, C.S.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; Simionescu, M.; et al. Hyperglycemia Determines Increased Specific MicroRNAs Levels in Sera and HDL of Acute Coronary Syndrome Patients and Stimulates MicroRNAs Production in Human Macrophages. PLoS ONE 2016, 11, e0161201. [Google Scholar] [CrossRef]
- Barbalata, T.; Zhang, L.; Dulceanu, M.D.; Stancu, C.S.; Devaux, Y.; Sima, A.V.; Niculescu, L.S.; EU-CardioRNA COST Action CA17129. Regulation of microRNAs in high-fat diet induced hyperlipidemic hamsters. Sci. Rep. 2020, 10, 20549. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.J.; Lei, H.P.; Wu, H.; Chen, J.Y.; Deng, C.Y.; Sheng, W.S.; Fu, Y.H.; Li, X.H.; Lin, Y.B.; Han, Y.L.; et al. Plasma miR-142 predicts major adverse cardiovascular events as an intermediate biomarker of dual antiplatelet therapy. Acta Pharmacol. Sin. 2019, 40, 208–215. [Google Scholar] [CrossRef]
- Pan, C.H.; Chien, S.C.; Chen, C.J.; Shih, C.M.; Hsieh, M.H.; Huang, C.Y.; Bi, W.F.; Chan, C.S.; Kao, Y.T.; Hsiao, C.Y.; et al. Circulating level of microRNA-142-5p is a potential biomarker for predicting in-stent restenosis: A case-control study. BMC Cardiovasc. Disord. 2021, 21, 77. [Google Scholar] [CrossRef]
- Wang, Y.; Ouyang, M.; Wang, Q.; Jian, Z. MicroRNA-142-3p inhibits hypoxia/reoxygenationinduced apoptosis and fibrosis of cardiomyocytes by targeting high mobility group box 1. Int. J. Mol. Med. 2016, 38, 1377–1386. [Google Scholar] [CrossRef]
- Jylhava, J.; Lehtimaki, T.; Jula, A.; Moilanen, L.; Kesaniemi, Y.A.; Nieminen, M.S.; Kahonen, M.; Hurme, M. Circulating cell-free DNA is associated with cardiometabolic risk factors: The Health 2000 Survey. Atherosclerosis 2014, 233, 268–271. [Google Scholar] [CrossRef]
- Gornik, I.; Wagner, J.; Gasparovic, V.; Milicic, D.; Degoricija, V.; Skoric, B.; Gornik, O.; Lauc, G. Prognostic value of cell-free DNA in plasma of out-of-hospital cardiac arrest survivors at ICU admission and 24h post-admission. Resuscitation 2014, 85, 233–237. [Google Scholar] [CrossRef] [Green Version]
- Ashar, F.N.; Zhang, Y.; Longchamps, R.J.; Lane, J.; Moes, A.; Grove, M.L.; Mychaleckyj, J.C.; Taylor, K.D.; Coresh, J.; Rotter, J.I.; et al. Association of Mitochondrial DNA Copy Number With Cardiovascular Disease. JAMA Cardiol. 2017, 2, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.; Ni, Y.; Bazeley, P.; Grandhi, S.; Wang, J.; Li, S.T.; Hazen, S.L.; Wilson Tang, W.H.; LaFramboise, T. Mitochondrial DNA Content Is Linked to Cardiovascular Disease Patient Phenotypes. J. Am. Heart Assoc. 2021, 10, e018776. [Google Scholar] [CrossRef]
- Cosentino, N.; Campodonico, J.; Moltrasio, M.; Lucci, C.; Milazzo, V.; Rubino, M.; De Metrio, M.; Marana, I.; Grazi, M.; Bonomi, A.; et al. Mitochondrial Biomarkers in Patients with ST-Elevation Myocardial Infarction and Their Potential Prognostic Implications: A Prospective Observational Study. J. Clin. Med. 2021, 10, 275. [Google Scholar] [CrossRef] [PubMed]
- Sudakov, N.P.; Apartsin, K.A.; Lepekhova, S.A.; Nikiforov, S.B.; Katyshev, A.I.; Lifshits, G.I.; Vybivantseva, A.V.; Konstantinov, Y.M. The level of free circulating mitochondrial DNA in blood as predictor of death in case of acute coronary syndrome. Eur. J. Med. Res. 2017, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Herbers, E.; Kekalainen, N.J.; Hangas, A.; Pohjoismaki, J.L.; Goffart, S. Tissue specific differences in mitochondrial DNA maintenance and expression. Mitochondrion 2019, 44, 85–92. [Google Scholar] [CrossRef]
- Bliksoen, M.; Mariero, L.H.; Torp, M.K.; Baysa, A.; Ytrehus, K.; Haugen, F.; Seljeflot, I.; Vaage, J.; Valen, G.; Stenslokken, K.O. Extracellular mtDNA activates NF-kappaB via toll-like receptor 9 and induces cell death in cardiomyocytes. Basic Res. Cardiol. 2016, 111, 42. [Google Scholar] [CrossRef]
- Salminen, A.; Ojala, J.; Kaarniranta, K.; Kauppinen, A. Mitochondrial dysfunction and oxidative stress activate inflammasomes: Impact on the aging process and age-related diseases. Cell Mol. Life Sci. 2012, 69, 2999–3013. [Google Scholar] [CrossRef]
- Bliksoen, M.; Mariero, L.H.; Ohm, I.K.; Haugen, F.; Yndestad, A.; Solheim, S.; Seljeflot, I.; Ranheim, T.; Andersen, G.O.; Aukrust, P.; et al. Increased circulating mitochondrial DNA after myocardial infarction. Int. J. Cardiol. 2012, 158, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthelemy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology/American College of Cardiology /American Heart Association/World Heart Federation Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Rev. Esp. Cardiol. (Engl. Ed.) 2017, 70, 1082. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Carnuta, M.G.; Stancu, C.S.; Toma, L.; Sanda, G.M.; Niculescu, L.S.; Deleanu, M.; Popescu, A.C.; Popescu, M.R.; Vlad, A.; Dimulescu, D.R.; et al. Dysfunctional high-density lipoproteins have distinct composition, diminished anti-inflammatory potential and discriminate acute coronary syndrome from stable coronary artery disease patients. Sci. Rep. 2017, 7, 7295. [Google Scholar] [CrossRef]
- Yu, J.; Miller, R.; Zhang, W.; Sharma, M.; Holtschlag, V.; Watson, M.A.; McLeod, H.L. Copy-number analysis of topoisomerase and thymidylate synthase genes in frozen and FFPE DNAs of colorectal cancers. Pharmacogenomics 2008, 9, 1459–1466. [Google Scholar] [CrossRef]
- Lindqvist, D.; Fernstrom, J.; Grudet, C.; Ljunggren, L.; Traskman-Bendz, L.; Ohlsson, L.; Westrin, A. Increased plasma levels of circulating cell-free mitochondrial DNA in suicide attempters: Associations with HPA-axis hyperactivity. Transl. Psychiatry 2016, 6, e971. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All STEMI with Follow-Up (n = 50) | No MACE (n = 38) | With MACE (n = 12) | p-Value |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Age (years) | 49.36 ± 1.27 | 49.34 ± 1.61 | 49.42 ± 1.49 | 0.641 |
| Aged group (>50 years old), n (%) | 22 (44.0) | 14 (36.8) | 8 (66.7) | 0.070 |
| Gender (male), n (%) | 45 (90.0) | 34 (89.5) | 11 (91.7) | 0.825 |
| LVEF (%) | 37.96 ± 1.32 | 39.38 ± 1.27 | 32.70 ± 3.78 | 0.037 |
| Cardiovascular risk factors | ||||
| Hyperglycemia, n (%) | 20 (40.0) | 11 (28.9) | 9 (75.0) | 1.68 × 10−3 |
| Hypertension, n (%) | 28 (56.0) | 19 (50.0) | 9 (75.0) | 0.128 |
| Dyslipidemia, n (%) | 44 (88.0) | 32 (84.2) | 12 (100.0) | 0.142 |
| Obesity, n (%) | 12 (24.0) | 10 (26.3) | 2 (16.7) | 0.495 |
| Smoking, n (%) | 45 (90.0) | 35 (92.1) | 10 (83.3) | 0.377 |
| Angiographic characteristics | ||||
| LAD, n (%) | 21 (42.0) | 17 (44.7) | 4 (33.3) | 0.341 |
| RCA, n (%) | 20 (40.0) | 13 (34.2) | 7 (58.3) | |
| LCX, n (%) | 9 (18.0) | 8 (21.1) | 1 (8.3) | |
| Area under the Curve | |||||
|---|---|---|---|---|---|
| Test Result Variable(s) * | Area | Standard Error a | p-Value b | Asymptotic 95% Confidence Interval | |
| Lower Bound | Upper Bound | ||||
| Univariate models | |||||
| HDL-C/apoA-I ratio | 0.299 | 0.101 | 0.071 | 0.102 | 0.496 |
| Atherogenic coefficient (AC) | 0.667 | 0.092 | 0.135 | 0.486 | 0.848 |
| CRP | 0.860 | 0.076 | 1.77 × 10−3 | 0.711 | 1.000 |
| LDH | 0.943 | 0.040 | 6.67 × 10−4 | 0.864 | 1.000 |
| Multivariate model 1 (HDL/ApoA-I ratio and AC) | 0.770 | 0.089 | 0.015 | 0.595 | 0.945 |
| Multivariate model 2 (CRP and LDH) | 0.953 | 0.038 | 6.67 × 10−4 | 0.869 | 1.000 |
| Multivariate model 3 (dyslipidemia, hyperglycemia, hypertension, obesity, smoking and LVEF) | 0.780 | 0.065 | 2.46 × 10−4 | 0.653 | 0.908 |
| Area under the Curve | |||||
|---|---|---|---|---|---|
| Test Result Variable(s) * | Area | Standard Error a | p-Value b | Asymptotic 95% Confidence Interval | |
| Lower Bound | Upper Bound | ||||
| Univariate models | |||||
| miR-223-3p | 0.788 | 0.071 | 5.18 × 10−3 | 0.648 | 0.927 |
| miR-142-3p | 0.832 | 0.069 | 1.27 × 10−3 | 0.696 | 0.968 |
| miR-155-5p | 0.742 | 0.094 | 0.019 | 0.558 | 0.927 |
| miR-486-5p | 0.718 | 0.096 | 0.034 | 0.530 | 0.906 |
| miR-125a-5p | 0.782 | 0.074 | 6.21 × 10−3 | 0.636 | 0.928 |
| miR-146a-5p | 0.785 | 0.083 | 5.67 × 10−3 | 0.622 | 0.948 |
| cfDNA | 0.722 | 0.102 | 0.029 | 0.523 | 0.921 |
| mtDNA | 0.832 | 0.069 | 1.09 × 10−3 | 0.698 | 0.966 |
| Multivariate model 1 (all 6 miRNAs) | 0.796 | 0.081 | 4.20 × 10−3 | 0.638 | 0.954 |
| Multivariate model 2 (all 6 miRNAs, cfDNA, and mtDNA) | 0.975 | 0.021 | 4.45 × 10−6 | 0.934 | 1.000 |
| Multivariate model 3 (mtDNA and miR-142-3p) | 0.833 | 0.069 | 1.17 × 10−3 | 0.697 | 0.968 |
| Multivariate model 4 (mtDNA, miR-142-3p, and miR-223-3p) | 0.833 | 0.070 | 1.17 × 10−3 | 0.696 | 0.970 |
| Multivariate model 5 (mtDNA, miR-142-3p, miR-223-3p, and miR-146a-5p) | 0.903 | 0.046 | 8.37 × 10−5 | 0.813 | 0.993 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbalata, T.; Scarlatescu, A.I.; Sanda, G.M.; Toma, L.; Stancu, C.S.; Dorobantu, M.; Micheu, M.M.; Sima, A.V.; Niculescu, L.S. Mitochondrial DNA Together with miR-142-3p in Plasma Can Predict Unfavorable Outcomes in Patients after Acute Myocardial Infarction. Int. J. Mol. Sci. 2022, 23, 9947. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23179947
Barbalata T, Scarlatescu AI, Sanda GM, Toma L, Stancu CS, Dorobantu M, Micheu MM, Sima AV, Niculescu LS. Mitochondrial DNA Together with miR-142-3p in Plasma Can Predict Unfavorable Outcomes in Patients after Acute Myocardial Infarction. International Journal of Molecular Sciences. 2022; 23(17):9947. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23179947
Chicago/Turabian StyleBarbalata, Teodora, Alina I. Scarlatescu, Gabriela M. Sanda, Laura Toma, Camelia S. Stancu, Maria Dorobantu, Miruna M. Micheu, Anca V. Sima, and Loredan S. Niculescu. 2022. "Mitochondrial DNA Together with miR-142-3p in Plasma Can Predict Unfavorable Outcomes in Patients after Acute Myocardial Infarction" International Journal of Molecular Sciences 23, no. 17: 9947. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23179947