

Targeted Next-Generation Sequencing-Based Multiple Gene Mutation Profiling of Patients with Rectal Adenocarcinoma Receiving or Not Receiving Neoadjuvant Chemoradiotherapy

 and
and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Methods and Materials
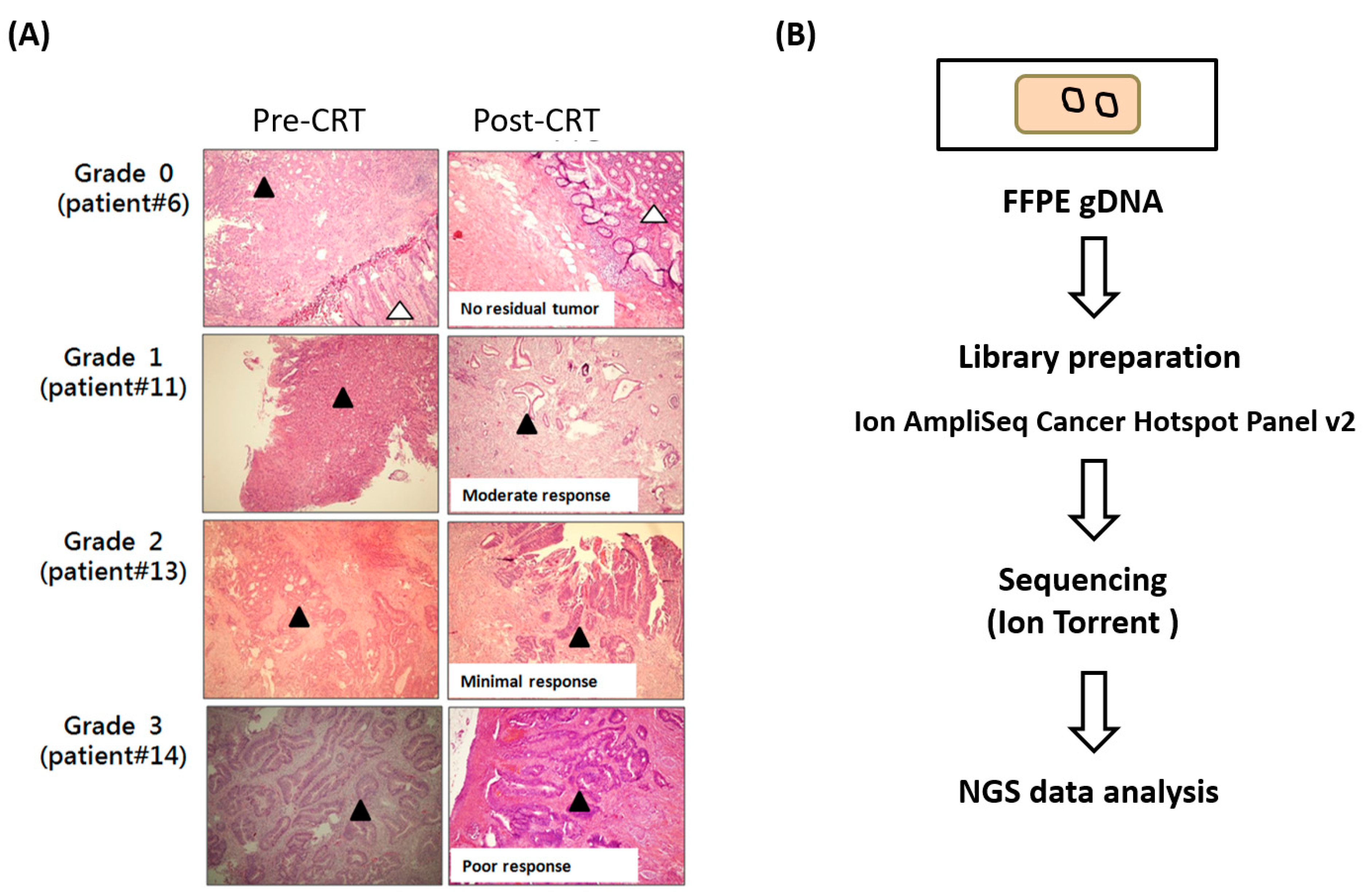
4.1. Clinical Samples
4.2. DNA Extraction
4.3. Cancer Hotspot Panel v2 Sequencing
4.4. Data Analysis
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- De Caluwe, L.; Van Nieuwenhove, Y.; Ceelen, W.P. Preoperative chemoradiation versus radiation alone for stage II and III resectable rectal cancer. Cochrane Database Syst. Rev. 2013, 28, CD006041. [Google Scholar] [CrossRef] [PubMed]
- Bosset, J.F.; Collette, L.; Calais, G.; Mineur, L.; Maingon, P.; Radosevic-Jelic, L.; Daban, A.; Bardet, E.; Beny, A.; Ollier, J.C.; et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N. Engl. J. Med. 2006, 355, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Nahas, S.C.; Rizkallah Nahas, C.S.; Sparapan Marques, C.F.; Ribeiro, U., Jr.; Cotti, G.C.; Imperiale, A.R.; Capareli, F.C.; Chih Chen, A.T.; Hoff, P.M.; Cecconello, I. Pathologic Complete Response in Rectal Cancer: Can We Detect It? Lessons Learned From a Proposed Randomized Trial of Watch-and-Wait Treatment of Rectal Cancer. Dis. Colon Rectum 2016, 59, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Glynne-Jones, R.; Grainger, J.; Harrison, M.; Ostler, P.; Makris, A. Neoadjuvant chemotherapy prior to preoperative chemoradiation or radiation in rectal cancer: Should we be more cautious? Br. J. Cancer 2006, 94, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Molinari, C.; Matteucci, F.; Caroli, P.; Passardi, A. Biomarkers and Molecular Imaging as Predictors of Response to Neoadjuvant Chemoradiotherapy in Patients With Locally Advanced Rectal Cancer. Clin. Colorectal Cancer 2015, 14, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.B.; Wu, X.Y.; Yu, R.; Li, C.; Wang, L.Q.; Shen, W.; Lu, P.H. P53 status as a predictive biomarker for patients receiving neoadjuvant radiation-based treatment: A meta-analysis in rectal cancer. PLoS ONE 2012, 7, e45388. [Google Scholar] [CrossRef]
- Duldulao, M.P.; Lee, W.; Nelson, R.A.; Li, W.; Chen, Z.; Kim, J.; Garcia-Aguilar, J. Mutations in specific codons of the KRAS oncogene are associated with variable resistance to neoadjuvant chemoradiation therapy in patients with rectal adenocarcinoma. Ann. Surg. Oncol. 2013, 20, 2166–2171. [Google Scholar] [CrossRef]
- Aghagolzadeh, P.; Radpour, R. New trends in molecular and cellular biomarker discovery for colorectal cancer. World J. Gastroenterol. 2016, 22, 5678–5693. [Google Scholar] [CrossRef]
- Gonzalez-Pons, M.; Cruz-Correa, M. Colorectal Cancer Biomarkers: Where Are We Now? BioMed Res. Int. 2015, 2015, 149014. [Google Scholar] [CrossRef] [Green Version]
- Sveen, A.; Kopetz, S.; Lothe, R.A. Biomarker-guided therapy for colorectal cancer: Strength in complexity. Nat. Rev. Clin. Oncol. 2020, 17, 11–32. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lin, Y.; Huang, Y.; Jin, J.; Zou, S.; Zhang, X.; Li, H.; Feng, T.; Chen, J.; Zuo, Z.; et al. Genome landscapes of rectal cancer before and after preoperative chemoradiotherapy. Theranostics 2019, 9, 6856–6866. [Google Scholar] [CrossRef] [PubMed]
- Kamran, S.C.; Lennerz, J.K.; Margolis, C.A.; Liu, D.; Reardon, B.; Wankowicz, S.A.; Van Seventer, E.E.; Tracy, A.; Wo, J.Y.; Carter, S.L.; et al. Integrative Molecular Characterization of Resistance to Neoadjuvant Chemoradiation in Rectal Cancer. Clin Cancer Res. 2019, 25, 5561–5571. [Google Scholar] [CrossRef] [PubMed]
- Chow, O.S.; Kuk, D.; Keskin, M.; Smith, J.J.; Camacho, N.; Pelossof, R.; Chen, C.T.; Chen, Z.; Avila, K.; Weiser, M.R.; et al. KRAS and Combined KRAS/TP53 Mutations in Locally Advanced Rectal Cancer are Independently Associated with Decreased Response to Neoadjuvant Therapy. Ann. Surg. Oncol. 2016, 23, 2548–2555. [Google Scholar] [CrossRef]
- Sanger, F.; Nicklen, S.; Coulson, A.R. DNA sequencing with chain-terminating inhibitors. Proc. Natl. Acad. Sci. USA 1977, 74, 5463–5467. [Google Scholar] [CrossRef]
- Crumley, S.M.; Pepper, K.L.; Phan, A.T.; Olsen, R.J.; Schwartz, M.R.; Portier, B.P. Next-Generation Sequencing of Matched Primary and Metastatic Rectal Adenocarcinomas Demonstrates Minimal Mutation Gain and Concordance to Colonic Adenocarcinomas. Arch. Pathol. Lab. Med. 2015, 140, 529–535. [Google Scholar] [CrossRef]
- Gleeson, F.C.; Kipp, B.R.; Voss, J.S.; Campion, M.B.; Minot, D.M.; Tu, Z.J.; Klee, E.W.; Sciallis, A.P.; Graham, R.P.; Lazaridis, K.N.; et al. Endoscopic ultrasound fine-needle aspiration cytology mutation profiling using targeted next-generation sequencing: Personalized care for rectal cancer. Am. J. Clin. Pathol. 2015, 143, 879–888. [Google Scholar] [CrossRef]
- McCourt, C.M.; McArt, D.G.; Mills, K.; Catherwood, M.A.; Maxwell, P.; Waugh, D.J.; Hamilton, P.; O’Sullivan, J.M.; Salto-Tellez, M. Validation of next generation sequencing technologies in comparison to current diagnostic gold standards for BRAF, EGFR and KRAS mutational analysis. PLoS ONE 2013, 8, e69604. [Google Scholar] [CrossRef]
- Choi, M.; Scholl, U.I.; Ji, W.; Liu, T.; Tikhonova, I.R.; Zumbo, P.; Nayir, A.; Bakkaloglu, A.; Ozen, S.; Sanjad, S.; et al. Genetic diagnosis by whole exome capture and massively parallel DNA sequencing. Proc. Natl. Acad. Sci. USA 2009, 106, 19096–19101. [Google Scholar] [CrossRef]
- D’Haene, N.; Le Mercier, M.; De Neve, N.; Blanchard, O.; Delaunoy, M.; El Housni, H.; Dessars, B.; Heimann, P.; Remmelink, M.; Demetter, P.; et al. Clinical Validation of Targeted Next Generation Sequencing for Colon and Lung Cancers. PLoS ONE 2015, 10, e0138245. [Google Scholar] [CrossRef]
- Shitara, M.; Okuda, K.; Suzuki, A.; Tatematsu, T.; Hikosaka, Y.; Moriyama, S.; Sasaki, H.; Fujii, Y.; Yano, M. Genetic profiling of thymic carcinoma using targeted next-generation sequencing. Lung Cancer 2014, 86, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Chen, L.; Sah, S.; Latham, G.J.; Patel, R.; Song, Q.; Koeppen, H.; Tam, R.; Schleifman, E.; Mashhedi, H.; et al. Profiling cancer gene mutations in clinical formalin-fixed, paraffin-embedded colorectal tumor specimens using targeted next-generation sequencing. Oncologist 2014, 19, 336–343. [Google Scholar] [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci. Signal. 2013, 6, pl1. [Google Scholar] [CrossRef] [PubMed]
- Giannakis, M.; Mu, X.J.; Shukla, S.A.; Qian, Z.R.; Cohen, O.; Nishihara, R.; Bahl, S.; Cao, Y.; Amin-Mansour, A.; Yamauchi, M.; et al. Genomic Correlates of Immune-Cell Infiltrates in Colorectal Carcinoma. Cell Rep. 2016, 15, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Hoadley, K.A.; Yau, C.; Hinoue, T.; Wolf, D.M.; Lazar, A.J.; Drill, E.; Shen, R.; Taylor, A.M.; Cherniack, A.D.; Thorsson, V.; et al. Cell-of-Origin Patterns Dominate the Molecular Classification of 10,000 Tumors from 33 Types of Cancer. Cell 2018, 173, 291–304.e6. [Google Scholar] [CrossRef] [PubMed]
- Yaeger, R.; Chatila, W.K.; Lipsyc, M.D.; Hechtman, J.F.; Cercek, A.; Sanchez-Vega, F.; Jayakumaran, G.; Middha, S.; Zehir, A.; Donoghue, M.T.A.; et al. Clinical Sequencing Defines the Genomic Landscape of Metastatic Colorectal Cancer. Cancer Cell 2018, 33, 125–136.e3. [Google Scholar] [CrossRef]
- Mondaca, S.; Walch, H.; Nandakumar, S.; Chatila, W.K.; Schultz, N.; Yaeger, R. Specific Mutations in APC, but Not Alterations in DNA Damage Response, Associate with Outcomes of Patients with Metastatic Colorectal Cancer. Gastroenterology 2020, 159, 1975–1978.e4. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef]
- Garcia-Aguilar, J.; Chen, Z.; Smith, D.D.; Li, W.; Madoff, R.D.; Cataldo, P.; Marcet, J.; Pastor, C. Identification of a biomarker profile associated with resistance to neoadjuvant chemoradiation therapy in rectal cancer. Ann. Surg. 2011, 254, 486–492, discussion 492–483. [Google Scholar] [CrossRef] [Green Version]
- Erben, P.; Strobel, P.; Horisberger, K.; Popa, J.; Bohn, B.; Hanfstein, B.; Kahler, G.; Kienle, P.; Post, S.; Wenz, F.; et al. KRAS and BRAF mutations and PTEN expression do not predict efficacy of cetuximab-based chemoradiotherapy in locally advanced rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 1032–1038. [Google Scholar] [CrossRef]
- Davies, J.M.; Trembath, D.; Deal, A.M.; Funkhouser, W.K.; Calvo, B.F.; Finnegan, T.; Weck, K.E.; Tepper, J.E.; O’Neil, B.H. Phospho-ERK and AKT status, but not KRAS mutation status, are associated with outcomes in rectal cancer treated with chemoradiotherapy. Radiat. Oncol. 2011, 6, 114. [Google Scholar] [CrossRef]
- Russo, A.L.; Ryan, D.P.; Borger, D.R.; Wo, J.Y.; Szymonifka, J.; Liang, W.Y.; Kwak, E.L.; Blaszkowsky, L.S.; Clark, J.W.; Allen, J.N.; et al. Mutational and clinical predictors of pathologic complete response in the treatment of locally advanced rectal cancer. J. Gastrointest. Cancer 2014, 45, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas, N. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012, 487, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.; Lambert, A.W.; Ozturk, S.; Papageorgis, P.; Lopez, D.; Shen, N.; Sen, Z.; Abdolmaleky, H.M.; Gyorffy, B.; Feng, H.; et al. Targeting RICTOR Sensitizes SMAD4-Negative Colon Cancer to Irinotecan. Mol. Cancer Res. 2020, 18, 414–423. [Google Scholar] [CrossRef]
- Boulay, J.L.; Mild, G.; Lowy, A.; Reuter, J.; Lagrange, M.; Terracciano, L.; Laffer, U.; Herrmann, R.; Rochlitz, C. SMAD4 is a.a predictive marker for 5-fluorouracil-based chemotherapy in patients with colorectal cancer. Br. J. Cancer 2002, 87, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Alhopuro, P.; Alazzouzi, H.; Sammalkorpi, H.; Davalos, V.; Salovaara, R.; Hemminki, A.; Jarvinen, H.; Mecklin, J.P.; Schwartz, S., Jr.; Aaltonen, L.A.; et al. SMAD4 levels and response to 5-fluorouracil in colorectal cancer. Clin. Cancer Res. 2005, 11, 6311–6316. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Xia, X.; Yang, C.; Shen, J.; Mai, J.; Kim, H.C.; Kirui, D.; Kang, Y.; Fleming, J.B.; Koay, E.J.; et al. SMAD4 Gene Mutation Renders Pancreatic Cancer Resistance to Radiotherapy through Promotion of Autophagy. Clin. Cancer Res. 2018, 24, 3176–3185. [Google Scholar] [CrossRef]
- Fang, T.; Liang, T.; Wang, Y.; Wu, H.; Liu, S.; Xie, L.; Liang, J.; Wang, C.; Tan, Y. Prognostic role and clinicopathological features of SMAD4 gene mutation in colorectal cancer: A systematic review and meta-analysis. BMC Gastroenterol. 2021, 21, 297. [Google Scholar] [CrossRef]
- Park, J.W.; Seo, M.J.; Cho, K.S.; Kook, M.C.; Jeong, J.M.; Roh, S.G.; Cho, S.Y.; Cheon, J.H.; Kim, H.K. Smad4 and p53 synergize in suppressing autochthonous intestinal cancer. Cancer Med. 2022, 11, 1925–1936. [Google Scholar] [CrossRef]
- Sakamoto, N.; Feng, Y.; Stolfi, C.; Kurosu, Y.; Green, M.; Lin, J.; Green, M.E.; Sentani, K.; Yasui, W.; McMahon, M.; et al. BRAF(V600E) cooperates with CDX2 inactivation to promote serrated colorectal tumorigenesis. Elife 2017, 6, e20331. [Google Scholar] [CrossRef] [PubMed]
- Tong, K.; Pellon-Cardenas, O.; Sirihorachai, V.R.; Warder, B.N.; Kothari, O.A.; Perekatt, A.O.; Fokas, E.E.; Fullem, R.L.; Zhou, A.; Thackray, J.K.; et al. Degree of Tissue Differentiation Dictates Susceptibility to BRAF-Driven Colorectal Cancer. Cell Rep. 2017, 21, 3833–3845. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor Regression | |||||||
|---|---|---|---|---|---|---|---|
| Grade 0 (n = 9) | Grade 1 (n = 11) | Grade 2–3 (n = 9) | |||||
| n | (%) | n | (%) | n | (%) | p Value | |
| Age | 0.870 | ||||||
| <65 years | 4 | (44.4) | 6 | (54.5) | 5 | (55.6) | |
| ≥65 years | 5 | (55.6) | 5 | (45.5) | 4 | (44.4) | |
| Sex | 0.568 | ||||||
| Female | 4 | (44.4) | 3 | (27.3) | 2 | (22.2) | |
| Male | 5 | (55.6) | 8 | (72.7) | 7 | (77.8) | |
| Clinical stage | 0.402 | ||||||
| I-II | 2 | (22.2) | 4 | (36.4) | 1 | (11.1) | |
| III-IV | 7 | (77.8) | 7 | (63.6) | 8 | (88.9) | |
| pT stage | 0.192 | ||||||
| I-II | 0 | (0.0) | 2 | (18.2) | 2 | (22.2) | |
| III-IV | 9 | (100.0) | 9 | (81.8) | 7 | (77.8) | |
| pN stage | 0.367 | ||||||
| N0 | 3 | (33.3) | 4 | (36.4) | 1 | (11.1) | |
| >N1 | 6 | (66.7) | 7 | (63.6) | 8 | (88.9) | |
| pM stage | 0.081 | ||||||
| M0 | 7 | (77.8) | 11 | (100.0) | 9 | (100.0) | |
| M1 | 2 | (22.2) | 0 | (0.0) | 0 | (0.0) | |
| Lymph node metastasis | 0.096 | ||||||
| No | 8 | (88.9) | 5 | (45.5) | 5 | (55.6) | |
| Yes | 1 | (11.1) | 6 | (54.5) | 4 | (44.4) | |
| Total | Grade 0 | Grade 1–3 | ||||
|---|---|---|---|---|---|---|
| Gene | n = 29 | % | n = 9 | % | n = 20 | % |
| ALK | 2 | 6.9 | 1 | 11.1 | 1 | 5.0 |
| APC | 19 | 65.5 | 7 | 77.8 | 12 | 60.0 |
| ATM | 5 | 17.2 | 1 | 11.1 | 4 | 20.0 |
| BRAF | 6 | 20.7 | 1 | 11.1 | 5 | 25.0 |
| CDKN2A | 9 | 31.0 | 2 | 22.2 | 7 | 35.0 |
| CTNNB1 | 3 | 10.3 | 1 | 11.1 | 2 | 10.0 |
| EGFR | 7 | 24.1 | 2 | 22.2 | 5 | 25.0 |
| ERBB4 | 3 | 10.3 | 1 | 11.1 | 2 | 10.0 |
| FBXW7 | 6 | 20.7 | 3 | 33.3 | 3 | 15.0 |
| FGFR1 | 5 | 17.2 | 2 | 22.2 | 3 | 15.0 |
| FLT3 | 4 | 13.8 | 1 | 11.1 | 3 | 15.0 |
| GNA11 | 2 | 6.9 | 0 | 0.0 | 2 | 10.0 |
| GNAQ | 1 | 3.4 | 1 | 11.1 | 0 | 0.0 |
| KDR | 4 | 13.8 | 1 | 11.1 | 3 | 15.0 |
| KIT | 5 | 17.2 | 1 | 11.1 | 4 | 20.0 |
| KRAS | 14 | 48.3 | 6 | 66.7 | 8 | 40.0 |
| MET | 3 | 10.3 | 2 | 22.2 | 1 | 5.0 |
| PIK3CA | 6 | 20.7 | 1 | 11.1 | 5 | 25.0 |
| PTEN | 6 | 20.7 | 1 | 11.1 | 5 | 25.0 |
| PTPN11 | 4 | 13.8 | 0 | 0.0 | 4 | 20.0 |
| RB1 | 3 | 10.3 | 1 | 11.1 | 2 | 10.0 |
| RET | 4 | 13.8 | 1 | 11.1 | 3 | 15.0 |
| SMAD4 | 6 | 20.7 | 1 | 11.1 | 5 | 25.0 |
| STK11 | 3 | 10.3 | 1 | 11.1 | 2 | 10.0 |
| TP53 | 27 | 93.1 | 8 | 88.9 | 19 | 95.0 |
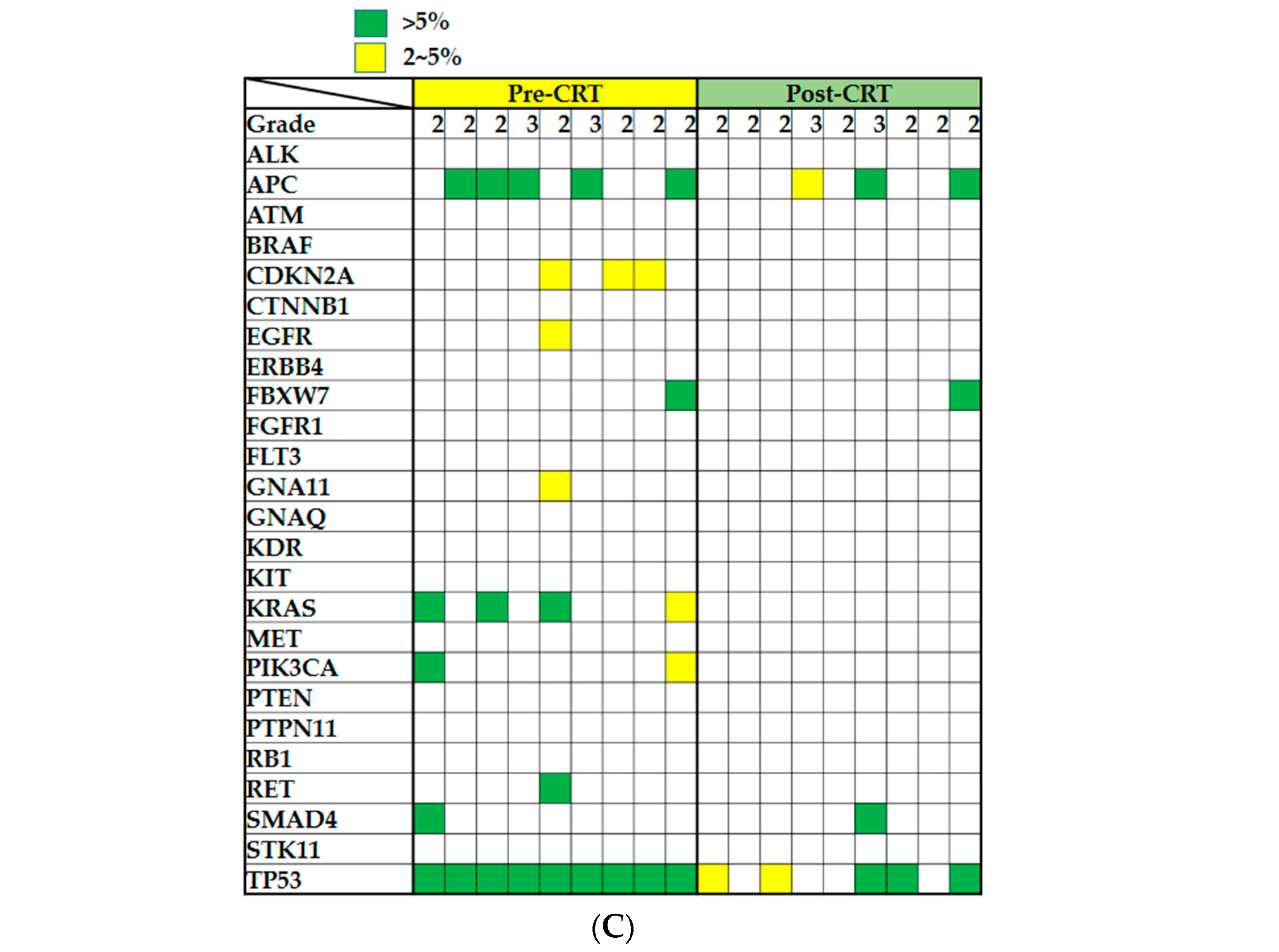
| Patients No. | Genes | Protein Change | Mutation Type | Nucleotide Change | Pre-CRT% | Post-CRT% |
|---|---|---|---|---|---|---|
| 23 | APC | p.M1383fs | Frameshift | c.4146_4147insA | 38.3 | 8.1 |
| 29 | APC | p.L1488fs | Frameshift | c.4461delT | 11.7 | 8.0 |
| 18 | APC | p.E1309 * | Stop gained | c.3925G > T | 16.6 | 6.6 |
| 18 | APC | p.E1353 * | Stop gained | c.4057G > T | 19.2 | 6.4 |
| 25 | BRAF | p.V600E | Missense | c.1799T > A | 15.1 | 11.9 |
| 7 | FBXW7 | p.G459E | Missense | c.1376G > A | 0.0 | 5.2 |
| 29 | FBXW7 | p.R505C | Missense | c.1513C > T | 12.2 | 9.6 |
| 23 | KRAS | p.A146T | Missense | c.436G > A | 21.7 | 5.1 |
| 18 | SMAD4 | p.A118V | Missense | c.353C > T | 0.0 | 6.1 |
| 23 | TP53 | p.M237I | Missense | c.711G > A | 37.6 | 6.9 |
| 25 | TP53 | p.R342 * | Stop gained | c.1024C > T | 39.7 | 22.7 |
| 20 | TP53 | p.R213fs | Frameshift | c.636dupT | 15.6 | 7.1 |
| 29 | TP53 | p.Q104 * | Stop gained | c.310C > T | 23.6 | 12.0 |
| 18 | TP53 | p.V173M | Missense | c.517G > A | 26.3 | 7.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.-K.; Tseng, H.-H.; Leung, C.-M.; Lu, K.-C.; Tsai, K.-W. Targeted Next-Generation Sequencing-Based Multiple Gene Mutation Profiling of Patients with Rectal Adenocarcinoma Receiving or Not Receiving Neoadjuvant Chemoradiotherapy. Int. J. Mol. Sci. 2022, 23, 10353. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231810353
Chang Y-K, Tseng H-H, Leung C-M, Lu K-C, Tsai K-W. Targeted Next-Generation Sequencing-Based Multiple Gene Mutation Profiling of Patients with Rectal Adenocarcinoma Receiving or Not Receiving Neoadjuvant Chemoradiotherapy. International Journal of Molecular Sciences. 2022; 23(18):10353. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231810353
Chicago/Turabian StyleChang, You-Kang, Hui-Hwa Tseng, Chung-Man Leung, Kuo-Cheng Lu, and Kuo-Wang Tsai. 2022. "Targeted Next-Generation Sequencing-Based Multiple Gene Mutation Profiling of Patients with Rectal Adenocarcinoma Receiving or Not Receiving Neoadjuvant Chemoradiotherapy" International Journal of Molecular Sciences 23, no. 18: 10353. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms231810353