
Drug-Induced Enterocolitis Syndrome in Children
 ,
, 

Abstract
:1. Introduction
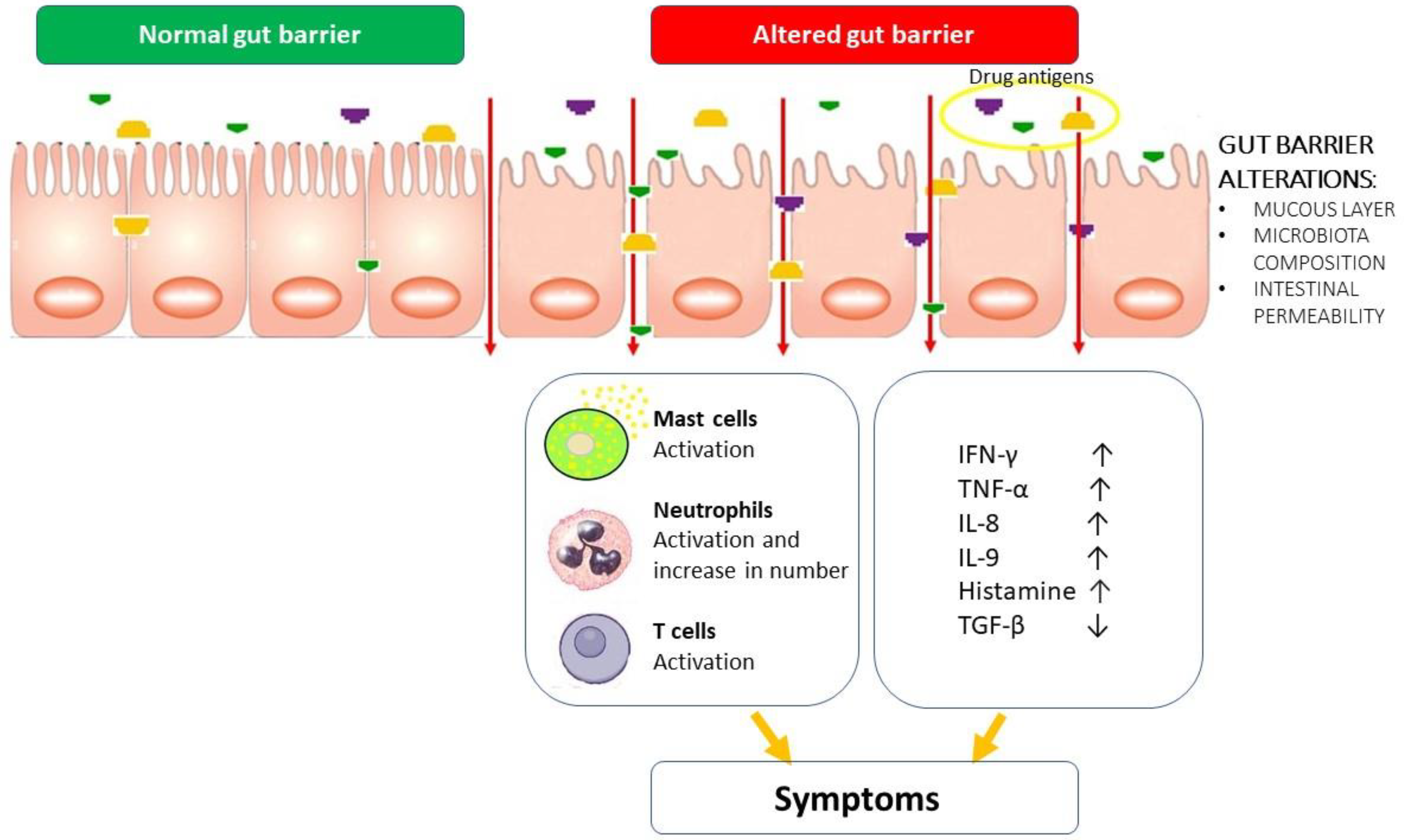
2. General Mechanisms of Gut Protection and Injury
3. Possible Pathogenetic Mechanisms of DIES and Similarities with FPIES
4. Clinical Manifestations of DIES
5. Laboratory Findings in Children with DIES
6. Diagnosis of DIES
7. Management of DIES in Children
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Elio, N.; Francesca, M.; Simona, B.; Pucci, N. Drug-Induced Enterocolitis Syndrome (DIES). Pediatr. Allergy Immunol. 2014, 25, 415–416. [Google Scholar]
- Infante, S.; Zapatero, L. Drug-Induced Enterocolitis Syndrome by Amoxicillin. Pediatr. Allergy Immunol. 2017, 28, 105–106. [Google Scholar] [CrossRef] [PubMed]
- Bouvette, G.; Verreault, N.; Gagnon, N.; Lavoie, A. Drug-Induced Enterocolitis Syndrome (DIES) with Pantoprazole in an Adult Patient. J. Allergy Clin. Immunol. Pract. 2020, 8, 3183–3184. [Google Scholar] [CrossRef] [PubMed]
- Van Thuijl, A.O.J.; Landzaat, L.J.; Liem, O.; Emons, J.A.M.; Arends, N.J.T. Drug-Induced Enterocolitis Syndrome (DIES): A Clinical Entity That Deserves More Awareness. Ann. Allergy Asthma Immunol. 2019, 122, 538–539. [Google Scholar] [CrossRef] [PubMed]
- Eyraud, C.; Biermé, P.; Adam, M.B. Drug-Induced Enterocolitis Syndrome: A Rare, Severe, Non-IgE-Mediated Immediate Drug Allergy. Arch. Pédiatrie 2023, 30, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Worcel, J.; Tarelho, M.; Baron, M.; Ponvert, C.; Bidat, E.; Benoist, G.; Lezmi, G. Drug-Induced Enterocolitis Syndrome (DIES) in a 10-Year-Old Girl. Arch. Pediatr. 2020, 27, 51–52. [Google Scholar] [CrossRef]
- Mori, F.; Liccioli, G.; Fuchs, O.; Barni, S.; Giovannini, M.; Sarti, L.; Novembre, E.; Caubet, J.C. Drug-Induced Enterocolitis Syndrome: Similarities and Differences Compared with Food Protein-Induced Enterocolitis Syndrome. Pediatr. Allergy Immunol. 2021, 32, 1165–1172. [Google Scholar] [CrossRef]
- Freundt Serpa, N.P.; Sánchez-Morillas, L.; Jaqueti Moreno, P.; González-Gutiérrez, M.L.; Cimarra, M.; Cerecedo, I.; Fernández-Rivas, M. Drug-Induced Enterocolitis Syndrome Due to Amoxicillin-Clavulanic Acid with Good Tolerance to Penicillin. J. Investig. Allergol. Clin. Immunol. 2020, 30, 301–302. [Google Scholar] [CrossRef]
- Pascal, B.; Evrard, B.; Merlin, E.; Egron, C.; Bonnet, B.; Michaud, E. Drug-Induced Enterocolitis Syndrome with Paracetamol (Acetaminophen) in a 12-Month-Old Boy. Pediatr. Allergy Immunol. 2022, 33, e13755. [Google Scholar] [CrossRef]
- Gillies, M.; Ranakusuma, A.; Hoffmann, T.; Thorning, S.; McGuire, T.; Glasziou, P.; Del, C. Common Harms from Amoxicillin: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials for Any Indication. CMAJ 2015, 187, E21–E31. [Google Scholar] [CrossRef]
- Grattagliano, I.; Ubaldi, E.; Portincasa, P. Drug-Induced Enterocolitis: Prevention and Management in Primary Care. J. Dig. Dis. 2018, 19, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Campbell, C.; Kandalgaonkar, M.R.; Golonka, R.M.; Yeoh, B.S.; Vijay-Kumar, M.; Saha, P. Crosstalk between Gut Microbiota and Host Immunity: Impact on Inflammation and Immunotherapy. Biomedicines 2023, 11, 294. [Google Scholar] [CrossRef] [PubMed]
- Takiishi, T.; Fenero, C.I.M.; Câmara, N.O.S. Intestinal Barrier and Gut Microbiota: Shaping Our Immune Responses throughout Life. Tissue Barriers 2017, 5, e1373208. [Google Scholar] [CrossRef] [PubMed]
- Odenwald, M.A.; Turner, J.R. The Intestinal Epithelial Barrier: A Therapeutic Target? Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 9–21. [Google Scholar] [CrossRef]
- Pabst, R.; Russell, M.W.; Brandtzaeg, P. Tissue Distribution of Lymphocytes and Plasma Cells and the Role of the Gut. Trends Immunol. 2008, 29, 206–208. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Barbara, G.; Buurman, W.; Ockhuizen, T.; Schulzke, J.D.; Serino, M.; Tilg, H.; Watson, A.; Wells, J.M. Intestinal Permeability—A New Target for Disease Prevention and Therapy. BMC Gastroenterol. 2014, 14, 189. [Google Scholar] [CrossRef]
- Maldonado, R.A.; von Andrian, U.H. How Tolerogenic Dendritic Cells Induce Regulatory T Cells. Adv. Immunol. 2010, 108, 111–165. [Google Scholar]
- Varol, C.; Vallon-Eberhard, A.; Elinav, E.; Aychek, T.; Shapira, Y.; Luche, H.; Fehling, H.J.; Hardt, W.D.; Shakhar, G.; Jung, S. Intestinal Lamina Propria Dendritic Cell Subsets Have Different Origin and Functions. Immunity 2009, 31, 502–512. [Google Scholar] [CrossRef]
- Schulz, O.; Jaensson, E.; Persson, E.K.; Liu, X.; Worbs, T.; Agace, W.W.; Pabst, O. Intestinal CD103+, but Not CX3CR1+, Antigen Sampling Cells Migrate in Lymph and Serve Classical Dendritic Cell Functions. J. Exp. Med. 2009, 206, 3101–3114. [Google Scholar] [CrossRef]
- Coombes, J.L.; Siddiqui, K.R.R.; Arancibia-Cárcamo, C.V.; Hall, J.; Sun, C.M.; Belkaid, Y.; Powrie, F. A Functionally Specialized Population of Mucosal CD103+ DCs Induces Foxp3+ Regulatory T Cells via a TGF-β -and Retinoic Acid-Dependent Mechanism. J. Exp. Med. 2007, 204, 1757–1764. [Google Scholar] [CrossRef]
- Bogunovic, M.; Ginhoux, F.; Helft, J.; Shang, L.; Hashimoto, D.; Greter, M.; Liu, K.; Jakubzick, C.; Ingersoll, M.A.; Leboeuf, M.; et al. Origin of the Lamina Propria Dendritic Cell Network. Immunity 2009, 31, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Van der Sluis, M.; De Koning, B.A.E.; De Bruijn, A.C.J.M.; Velcich, A.; Meijerink, J.P.P.; Van Goudoever, J.B.; Büller, H.A.; Dekker, J.; Van Seuningen, I.; Renes, I.B.; et al. Muc2-Deficient Mice Spontaneously Develop Colitis, Indicating That MUC2 Is Critical for Colonic Protection. Gastroenterology 2006, 131, 117–129. [Google Scholar] [CrossRef]
- McDole, J.R.; Wheeler, L.W.; McDonald, K.G.; Wang, B.; Konjufca, V.; Knoop, K.A.; Newberry, R.D.; Miller, M.J. Goblet Cells Deliver Luminal Antigen to CD103 + Dendritic Cells in the Small Intestine. Nature 2012, 483, 345–349. [Google Scholar] [CrossRef]
- Robbe, C.; Capon, C.; Coddeville, B.; Michalski, J.C. Structural Diversity and Specific Distribution of O-Glycans in Normal Human Mucins along the Intestinal Tract. Biochem. J. 2004, 384, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, J.M.; Murphy, K.; Stanton, C.; Ross, R.P.; Kober, O.I.; Juge, N.; Avershina, E.; Rudi, K.; Narbad, A.; Jenmalm, M.C.; et al. The Composition of the Gut Microbiota throughout Life, with an Emphasis on Early Life. Microb. Ecol. Health Dis. 2015, 26, 26050. [Google Scholar] [CrossRef] [PubMed]
- Rokhsefat, S.; Lin, A.; Comelli, E.M. Mucin–Microbiota Interaction During Postnatal Maturation of the Intestinal Ecosystem: Clinical Implications. Dig. Dis. Sci. 2016, 61, 1473–1486. [Google Scholar] [CrossRef] [PubMed]
- Biol-N’garagba, M.C.; Niepceron, E.; Mathian, B.; Louisot, P. Glucocorticoid-Induced Maturation of Glycoprotein Galactosylation and Fucosylation Processes in the Rat Small Intestine. J. Steroid Biochem. Mol. Biol. 2003, 84, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Nanthakumar, N.N.; Dai, D.; Meng, D.; Chaudry, N.; Newburg, D.S.; Walker, W.A. Regulation of Intestinal Ontogeny: Effect of Glucocorticoids and Luminal Microbes on Galactosyltransferase and Trehalase Induction in Mice. Glycobiology 2005, 15, 221–232. [Google Scholar] [CrossRef]
- Jakobsson, H.E.; Rodríguez-Piñeiro, A.M.; Schütte, A.; Ermund, A.; Boysen, P.; Bemark, M.; Sommer, F.; Bäckhed, F.; Hansson, G.C.; Johansson, M.E. The Composition of the Gut Microbiota Shapes the Colon Mucus Barrier. EMBO Rep. 2015, 16, 164–177. [Google Scholar] [CrossRef]
- Schwerbrock, N.M.J.; Makkink, M.K.; van der Sluis, M.; Büller, H.A.; Einerhand, A.W.C.; Sartor, R.B.; Dekker, J. Interleukin 10-Deficient Mice Exhibit Defective Colonic Muc2 Synthesis before and after Induction of Colitis by Commensal Bacteria. Inflamm. Bowel Dis. 2004, 10, 811–823. [Google Scholar] [CrossRef]
- Kandori, H.; Hirayama, K.; Takeda, M.; Doi, K. Histochemical, Lectin-Histochemical and Morphometrical Characteristics of Intestinal Goblet Cells of Germfree and Conventional Mice. Exp. Anim. 1996, 45, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.E.V.; Jakobsson, H.E.; Holmén-Larsson, J.; Schütte, A.; Ermund, A.; Rodríguez-Piñeiro, A.M.; Arike, L.; Wising, C.; Svensson, F.; Bäckhed, F.; et al. Normalization of Host Intestinal Mucus Layers Requires Long-Term Microbial Colonization. Cell Host Microbe 2015, 18, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Milosevic, I.; Vujovic, A.; Barac, A.; Djelic, M.; Korac, M.; Spurnic, A.R.; Gmizic, I.; Stevanovic, O.; Djordjevic, V.; Lekic, N.; et al. Gut-Liver Axis, Gut Microbiota, and Its Modulation in the Management of Liver Diseases: A Review of the Literature. Int. J. Mol. Sci. 2019, 20, 395. [Google Scholar] [CrossRef]
- Michaudel, C.; Sokol, H. The Gut Microbiota at the Service of Immunometabolism. Cell Metab. 2020, 32, 514–523. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, A.M.; Shanahan, F. The Gut Flora as a Forgotten Organ. EMBO Rep. 2006, 7, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Amoroso, C.; Perillo, F.; Strati, F.; Fantini, M.C.; Caprioli, F.; Facciotti, F. The Role of Gut Microbiota Biomodulators on Mucosal Immunity and Intestinal Inflammation. Cells 2020, 9, 1234. [Google Scholar] [CrossRef]
- Shi, N.; Li, N.; Duan, X.; Niu, H. Interaction between the Gut Microbiome and Mucosal Immune System. Mil. Med. Res. 2017, 4, 14. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Bittinger, K.; Xuanwen, L.; Abernethy, D.R.; Bushman, F.D.; Fitzgerald, G.A. Bidirectional Interactions between Indomethacin and the Murine Intestinal Microbiota. eLife 2015, 4, e08973. [Google Scholar] [CrossRef]
- Su, K.; Cetinbas, M.; Martin, V.; Virkud, Y.; Seay, H.; Ndahayo, R.; Rosow, R.; Elkort, M.; Gupta, B.; Kramer, E.; et al. Early Infancy Dysbiosis in Food Protein-Induced Enterocolitis Syndrome: A Prospective Cohort Study. Allergy 2023. [Google Scholar] [CrossRef]
- Niccolai, E.; Baldi, S.; Ricci, F.; Russo, E.; Nannini, G.; Menicatti, M.; Poli, G.; Taddei, A.; Bartolucci, G.; Calabrò, A.S.; et al. Evaluation and Comparison of Short Chain Fatty Acids Composition in Gut Diseases. World J. Gastroenterol. 2019, 25, 5543. [Google Scholar] [CrossRef]
- Wang, H.B.; Wang, P.Y.; Wang, X.; Wan, Y.L.; Liu, Y.C. Butyrate Enhances Intestinal Epithelial Barrier Function via Up-Regulation of Tight Junction Protein Claudin-1 Transcription. Dig. Dis. Sci. 2012, 57, 3126–3135. [Google Scholar] [CrossRef]
- Sun, Y.; O’Riordan, M.X.D. Regulation of Bacterial Pathogenesis by Intestinal Short-Chain Fatty Acids. Adv. Appl. Microbiol. 2013, 85, 93–118. [Google Scholar] [PubMed]
- Bhaskaran, N.; Quigley, C.; Paw, C.; Butala, S.; Schneider, E.; Pandiyan, P. Role of Short Chain Fatty Acids in Controlling Tregs and Immunopathology during Mucosal Infection. Front. Microbiol. 2018, 9. [Google Scholar] [CrossRef]
- Schulthess, J.; Pandey, S.; Capitani, M.; Rue-Albrecht, K.C.; Arnold, I.; Franchini, F.; Chomka, A.; Ilott, N.E.; Johnston, D.G.W.; Pires, E.; et al. The Short Chain Fatty Acid Butyrate Imprints an Antimicrobial Program in Macrophages. Immunity 2019, 50, 432–445. [Google Scholar] [CrossRef] [PubMed]
- Pichler, W.J.; Adam, J.; Watkins, S.; Wuillemin, N.; Yun, J.; Yerly, D. Drug Hypersensitivity: How Drugs Stimulate T Cells via Pharmacological Interaction with Immune Receptors. Int. Arch. Allergy Immunol. 2015, 168, 13–24. [Google Scholar] [CrossRef]
- Pichler, W.J.; Beeler, A.; Keller, M.; Lerch, M.; Posadas, S.; Schmid, D.; Spanou, Z.; Zawodniak, A.; Gerber, B. Pharmacological Interaction of Drugs with Immune Receptors: The p-i Concept. Allergol. Int. 2006, 55, 17–25. [Google Scholar] [CrossRef]
- Pichler, W.J. Pharmacological Interaction of Drugs with Antigen-Specific Immune Receptors: The p-i Concept. Curr. Opin. Allergy Clin. Immunol. 2002, 2, 301–305. [Google Scholar] [CrossRef]
- Schnyder, B.; Mauri-Hellweg, D.; Zanni, M.; Bettens, F.; Pichler, W.J. Direct, MHC-Dependent Presentation of the Drug Sulfamethoxazole to Human Aβ T Cell Clones. J. Clin. Investig. 1997, 100, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Zanni, M.P.; Von Greyerz, S.; Schnyder, B.; Brander, K.A.; Frutig, K.; Hari, Y.; Valitutti, S.; Pichler, W.J. HLA-Restricted, Processing- and Metabolism-Independent Pathway of Drug Recognition by Human Aβ T Lymphocytes. J. Clin. Investig. 1998, 102, 1591–1598. [Google Scholar] [CrossRef]
- Demoly, P.; Adkinson, N.F.; Brockow, K.; Castells, M.; Chiriac, A.M.; Greenberger, P.A.; Khan, D.A.; Lang, D.M.; Park, H.S.; Pichler, W.; et al. International Consensus on Drug Allergy. Allergy Eur. J. Allergy Clin. Immunol. 2014, 69, 420–437. [Google Scholar] [CrossRef]
- Schrijvers, R.; Gilissen, L.; Chiriac, A.M.; Demoly, P. Pathogenesis and Diagnosis of Delayed-Type Drug Hypersensitivity Reactions, from Bedside to Bench and Back. Clin. Transl. Allergy 2015, 5, 31. [Google Scholar] [CrossRef]
- Adair, K.; Meng, X.; Naisbitt, D.J. Drug Hapten-Specific T-Cell Activation: Current Status and Unanswered Questions. Proteomics 2021, 21, 2000267. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Yerly, D.; Naisbitt, D.J. Mechanisms Leading to T-Cell Activation in Drug Hypersensitivity. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 317–324. [Google Scholar] [CrossRef]
- Whitaker, P.; Meng, X.; Lavergne, S.N.; El-Ghaiesh, S.; Monshi, M.; Earnshaw, C.; Peckham, D.; Gooi, J.; Conway, S.; Pirmohamed, M.; et al. Mass Spectrometric Characterization of Circulating and Functional Antigens Derived from Piperacillin in Patients with Cystic Fibrosis. J. Immunol. 2011, 187, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Aiba, S. Maturation of Dendritic Cells Induced by Cytokines and Haptens. Tohoku J. Exp. Med. 1998, 184, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.F. Contact Dermatitis: From Pathomechanisms to Immunotoxicology. Exp. Dermatol. 2012, 21, 382–389. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Zagursky, R. Penicillin and Cephalosporin Allergy. Ann. Allergy Asthma Immunol. 2014, 112, 404–412. [Google Scholar] [CrossRef]
- Pichler, W.J.; Watkins, S.; Yerly, D. Risk Assessment in Drug Hypersensitivity: Detecting Small Molecules Which Outsmart the Immune System. Front. Allergy 2022, 3, 827893. [Google Scholar] [CrossRef]
- Caubet, J.C.; Bencharitiwong, R.; Ross, A.; Sampson, H.A.; Berin, M.C.; Nowak-Węgrzyn, A. Humoral and Cellular Responses to Casein in Patients with Food Protein–Induced Enterocolitis to Cow’s Milk. J. Allergy Clin. Immunol. 2017, 139, 572–583. [Google Scholar] [CrossRef]
- Shek, L.P.C.; Bardina, L.; Castro, R.; Sampson, H.A.; Beyer, K. Humoral and Cellular Responses to Cow Milk Proteins in Patients with Milk-Induced IgE-Mediated and Non-IgE-Mediated Disorders. Allergy Eur. J. Allergy Clin. Immunol. 2005, 60, 912–919. [Google Scholar] [CrossRef]
- Van Sickle, G.J.; Powell, G.K.; McDonald, P.J.; Goldblum, R.M. Milk- and Soy Protein-Induced Enterocolitis: Evidence for Lymphocyte Sensitization to Specific Food Proteins. Gastroenterology 1985, 88, 1915–1921. [Google Scholar] [CrossRef]
- Benlounes, N.; Dupont, C.; Candalh, C.; Blaton, M.A.; Darmon, N.; Desjeux, J.F.; Heyman, M. The Threshold for Immune Cell Reactivity to Milk Antigens Decreases in Cow’s Milk Allergy with Intestinal Symptoms. J. Allergy Clin. Immunol. 1996, 98, 781–789. [Google Scholar] [CrossRef]
- Heyman, M.; Darmon, N.; Dupont, C.; Dugas, B.; Hirribaren, A.; Blaton, M.A.; Desjeux, J.F. Mononuclear Cells from Infants Allergic to Cow’s Milk Secrete Tumor Necrosis Factor α, Altering Intestinal Function. Gastroenterology 1994, 106, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.R.; Rugtveit, J.; Brandtzaeg, P. Allergen-Responsive CD4+CD25+ Regulatory T Cells in Children Who Have Outgrown Cow’s Milk Allergy. J. Exp. Med. 2004, 199, 1679–1688. [Google Scholar] [CrossRef]
- Hoffman, K.M.; Ho, D.G.; Sampson, H.A. Evaluation of the Usefulness of Lymphocyte Proliferation Assays in the Diagnosis of Allergy to Cow’s Milk. J. Allergy Clin. Immunol. 1997, 99, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, K.M.; Caubet, J.C.; Sickles, L.; Ford, L.S.; Sampson, H.A.; Nowak-Wgrzyn, A. Poor Utility of Atopy Patch Test in Predicting Tolerance Development in Food Protein-Induced Enterocolitis Syndrome. Ann. Allergy Asthma Immunol. 2012, 109, 221–222. [Google Scholar] [CrossRef]
- Ruffner, M.A.; Ruymann, K.; Barni, S.; Cianferoni, A.; Brown-Whitehorn, T.; Spergel, J.M. Food Protein-Induced Enterocolitis Syndrome: Insights from Review of a Large Referral Population. J. Allergy Clin. Immunol. Pract. 2013, 1, 343–349. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, J.B.; Hart, J.P.; Pizzo, S.V.; Shelburne, C.P.; Staats, H.F.; Gunn, M.D.; Abraham, S.N. Mast Cell-Derived Tumor Necrosis Factor Induces Hypertrophy of Draining Lymph Nodes during Infection. Nat. Immunol. 2003, 4, 1199–1205. [Google Scholar] [CrossRef]
- Shin, T.Y.; Kim, S.H.; Choi, C.H.; Shin, H.Y.; Kim, H.M. Isodon Japonicus Decreases Immediate-Type Allergic Reaction and Tumor Necrosis Factor-α Production. Int. Arch. Allergy Immunol. 2004, 135, 17–23. [Google Scholar] [CrossRef]
- Zhang, Y.; Ramos, B.F.; Jakschik, B.A. Neutrophil Recruitment by Tumor Necrosis Factor from Mast Cells in Immune Complex Peritonitis. Science 1992, 258, 1957–1959. [Google Scholar] [CrossRef]
- Rijnierse, A.; Koster, A.S.; Nijkamp, F.P.; Kraneveld, A.D. TNF-α Is Crucial for the Development of Mast Cell-Dependent Colitis in Mice. Am. J. Physiol.-Gastrointest. Liver Physiol. 2006, 291, G969–G976. [Google Scholar] [CrossRef] [PubMed]
- Baert, F.J.; Rutgeerts, P.R. Anti-TNF Strategies in Crohn’s Disease: Mechanisms, Clinical Effects, Indications. Int. J. Color. Dis. 1999, 14, 47–51. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Lorentz, A.; Schwengberg, S.; Weier, G.; Raab, R.; Manns, M.P. Mast Cells Are an Important Cellular Source of Tumour Necrosis Factor in Human Intestinal Tissue. Gut 1999, 44, 643–652. [Google Scholar] [CrossRef]
- Suryaprasad, A.G.; Prindiville, T. The Biology of TNF Blockade. Autoimmun. Rev. 2003, 2, 346–357. [Google Scholar] [CrossRef]
- Biedermann, T.; Kneilling, M.; Mailhammer, R.; Maier, K.; Sander, C.A.; Kollias, G.; Kunkel, S.L.; Hültner, L.; Röcken, M. Mast Cells Control Neutrophil Recruitment during T Cell-Mediated Delayed-Type Hypersensitivity Reactions through Tumor Necrosis Factor and Macrophage Inflammatory Protein 2. J. Exp. Med. 2000, 192, 1441–1452. [Google Scholar] [CrossRef]
- Granger, D.N.; Kubes, P. The Microcirculation and Inflammation: Modulation of Leukocyte-Endothelial Cell Adhesion. J. Leukoc. Biol. 1994, 55, 662–675. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.L.; Hwang, J.B.; Kwon, Y.D.; Park, M.H.; Shin, W.J.; Park, J.B. Deposition of Eosinophil-Granule Major Basic Protein and Expression of Intercellular Adhesion Molecule-1 and Vascular Cell Adhesion Molecule-1 in the Mucosa of the Small Intestine in Infants with Cow’s Milk-Sensitive Enteropathy. J. Allergy Clin. Immunol. 1999, 103, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Benlounes, N.; Candalh, C.; Matarazzo, P.; Dupont, C.; Heyman, M. The Time-Course of Milk Antigen-Induced TNF-α Secretion Differs According to the Clinical Symptoms in Children with Cow’s Milk Allergy. J. Allergy Clin. Immunol. 1999, 104, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Lee, J.B.; Liu, B.; Ohta, S.; Wang, P.Y.; Kartashov, A.V.; Mugge, L.; Abonia, J.P.; Barski, A.; Izuhara, K.; et al. Induction of Interleukin-9-Producing Mucosal Mast Cells Promotes Susceptibility to IgE-Mediated Experimental Food Allergy. Immunity 2015, 43, 788–802. [Google Scholar] [CrossRef]
- Lozano-Ojalvo, D.; Chen, X.; Dunkin, D.; Agashe, C.; Baker, M.; Bird, J.A.; Molina, E.; Nowak-Wegrzyn, A.; Berin, M.C. Untargeted Serum Metabolomic Analysis Reveals a Role for Purinergic Signaling in FPIES. J. Allergy Clin. Immunol. 2023, 151, 797–802. [Google Scholar] [CrossRef]
- Demoly, P.; Hillaire-Buys, D. Classification and Epidemiology of Hypersensitivity Drug Reactions. Immunol. Allergy Clin. North Am. 2004, 24, 345–356. [Google Scholar] [CrossRef]
- Barni, S.; Mori, F.; Bianchi, A.; Pucci, N.; Novembre, E. Shift from IgE-Mediated Cow’s Milk Allergy to Food Protein-Induced Enterocolitis Syndrome in 2 Infants. Pediatr. Allergy Immunol. 2018, 29, 446–447. [Google Scholar] [CrossRef] [PubMed]
- Caubet, J.C.; Cianferoni, A.G.M. Food Protein-Induced Enterocolitis Syndrome. Clin. Exp. Allergy 2019, 49, 1178–1190. [Google Scholar] [CrossRef] [PubMed]
- Shimomura, M.; Ito, Y.; Tanaka, H.; Meguro, T.; Kimura, M. Increased Serum Cortisol on Oral Food Challenge in Infants with Food Protein-Induced Enterocolitis Syndrome. Pediatr. Int. 2018, 60, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Yaytokgil, S.B.; Güvenir, H.; Celík, I.K.; Topal, Ö.Y.; Karaatmaca, B.; Civelek, E.; Toyran, M.; Misirlioglu, E.D. Evaluation of Drug Patch Tests in Children. Allergy Asthma Proc. 2021, 42, 167. [Google Scholar] [CrossRef]
- Nowak-Węgrzyn, A.; Chehade, M.; Groetch, M.E.; Spergel, J.M.; Wood, R.A.; Allen, K.; Atkins, D.; Bahna, S.; Barad, A.V.; Berin, C.; et al. International Consensus Guidelines for the Diagnosis and Management of Food Protein–Induced Enterocolitis Syndrome: Executive Summary—Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2017, 139, 1111–1126. [Google Scholar] [CrossRef]
- Hoffmann, N.V.; Ahmed, A.; Fortunato, J.E. Food Protein–Induced Enterocolitis Syndrome: Dynamic Relationship among Gastrointestinal Symptoms, Immune Response, and the Autonomic Nervous System. Ann. Allergy Asthma Immunol. 2021, 126, 498–505. [Google Scholar] [CrossRef]
- Wu, H.; Denna, T.H.; Storkersen, J.N.; Gerriets, V.A. Beyond a Neurotransmitter: The Role of Serotonin in Inflammation and Immunity. Pharmacol. Res. 2019, 140, 100–114. [Google Scholar] [CrossRef]
- Moeller, J.R.; Gummin, D.D.; Nelson, T.J.; Drendel, A.L.; Shah, B.K.; Berger, S. Risk of Ventricular Arrhythmias and Association with Ondansetron. J. Pediatr. 2016, 179, 118–123. [Google Scholar] [CrossRef]
- Fernandes, F.M.; da Silva Paulino, A.M.; Sedda, B.C.; da Silva, E.P.; Martins, R.R.; Oliveira, A.G. Assessment of the Risk of QT-Interval Prolongation Associated with Potential Drug-Drug Interactions in Patients Admitted to Intensive Care Units. Saudi Pharm. J. 2019, 27, 229–234. [Google Scholar] [CrossRef]
- Coates, R.W.; Weaver, K.R.; Lloyd, R.; Ceccacci, N.; Greenberg, M.R. Food Protein-Induced Enterocolitis Syndrome as a Cause for Infant Hypotension. West. J. Emerg. Med. 2011, 12, 512. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Age (years) | Triggering Drug | Clinical Manifestations after Drug Intake | Clinical Manifestations after DPT | Time between Drug Administration and Symptoms | Laboratory Findings | Treatment |
|---|---|---|---|---|---|---|---|
| Novembre, 2014 [1] | 6 | AMX | Vomiting and a morbilliform rash the next day | Vomiting, diarrhea, pallor, lethargy | 2 h | Leukocytosis with neutrophilia (WBC 20,480/mm3, N 82.2%) MethHb 1.1% | Saline solution infusion, IV hydrocortisone |
| Infante, 2017 [2] | 3 | AMX | Acute urticaria (2 y) | Vomiting, diarrhea, moderate abdominal pain | 4 h | Leukocytosis with neutrophilia (WBC 17,800/mm3, N 73.6%) | Saline solution infusion, antiemetics, hydrocortisone |
| Van Thuijl, 2019 [4] | 4 | AMX | Repetitive vomiting and lethargy | Severe abdominal pain, vomiting, pallor, lethargy | 1.5 h | Leukocytosis with neutrophilia (WBC 24,000/mm3; N 82.5%) | IM adrenalina, antihistaminic, IV hydrocortisone and ondansetron |
| Worcel, 2020 [6] | 10 | AMX | Repetitive vomiting, pallor, watery diarrhea 10 h later | Repetitive vomiting, pallor, lethargy, abdominal pain, watery diarrhea 8 h later | 2 h | N/A | Desloratadine, prednisolone, oral rehydration |
| Mori, 2021 [7] | 6 | AMX/CLV | Vomiting, pallor, lethargy | 2.5 h | Leukocytosis with neutrophilia (WBC 15,350/mm3, N 85.8%) MethHb 0.7% | Saline solution infusion | |
| Mori, 2021 [7] | 14 | AMX/CLV | Persistent vomiting with streaks of blood and lethargy | Vomiting, pallor, lethargy, abdominal pain, dehydration | 2.5 h | Leukocytosis with neutrophilia (WBC 10,730/mm3, N 86.3%) MethHb 0.7% | Saline solution infusion and IV ondansetron |
| Mori, 2021 [7] | 9 | AMX | Maculopapular exanthema | Vomiting, pallor, lethargy | 3 h | N/A | Saline solution infusion and IV ondansetron |
| Pascal, 2022 [9] | 0.8 | PAR | Vomiting, asthenia, pallor, tachycardia | Vomiting, pallor, lethargy | 4 h | Leukocytosis with neutrophilia (N 11,080/mm3) MethHb 1.3% | Saline solution infusion, steroid therapy |
| Eyraud, 2023 [5] | 4 | AMX | Erythematous rash and eyelid edema on the 7th day of treatment (2 y) | Vomiting, abdominal pain, intense pallor, and tachycardia | 2 h | N/A | Saline solution infusion, IV ondansetron, IM adrenaline |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Filippo, P.; Venanzi, A.; Ciarelli, F.; Panetti, B.; Di Pillo, S.; Chiarelli, F.; Attanasi, M. Drug-Induced Enterocolitis Syndrome in Children. Int. J. Mol. Sci. 2023, 24, 7880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24097880
Di Filippo P, Venanzi A, Ciarelli F, Panetti B, Di Pillo S, Chiarelli F, Attanasi M. Drug-Induced Enterocolitis Syndrome in Children. International Journal of Molecular Sciences. 2023; 24(9):7880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24097880
Chicago/Turabian StyleDi Filippo, Paola, Annamaria Venanzi, Francesca Ciarelli, Beatrice Panetti, Sabrina Di Pillo, Francesco Chiarelli, and Marina Attanasi. 2023. "Drug-Induced Enterocolitis Syndrome in Children" International Journal of Molecular Sciences 24, no. 9: 7880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24097880