
The Crossroads of the Coagulation System and the Immune System: Interactions and Connections
 , , , and
, , , and
Abstract
:1. Introduction
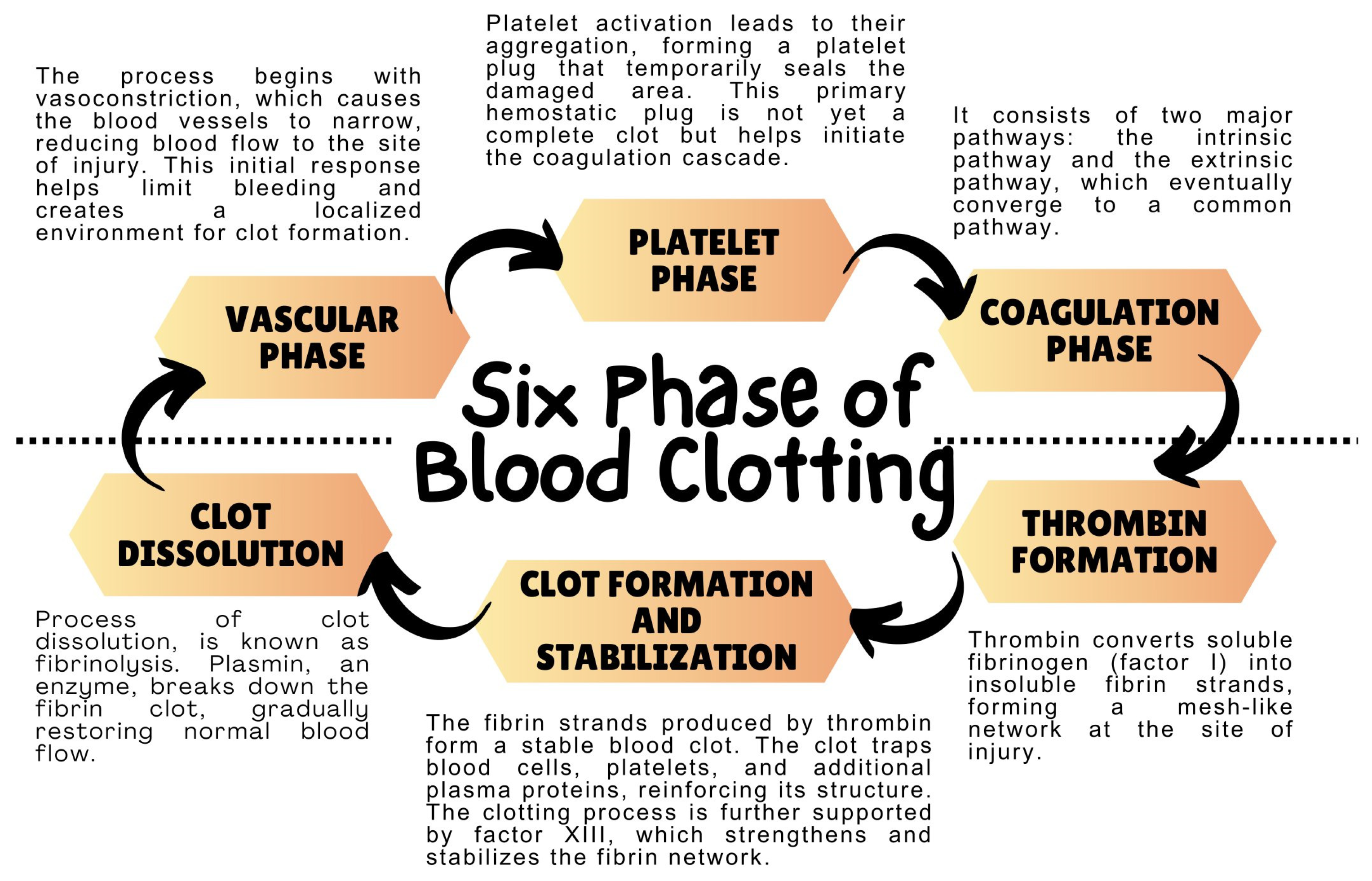
2. Coagulation System—Mechanism of Action
3. Blood Coagulation Process and the Role of Immune System Cells
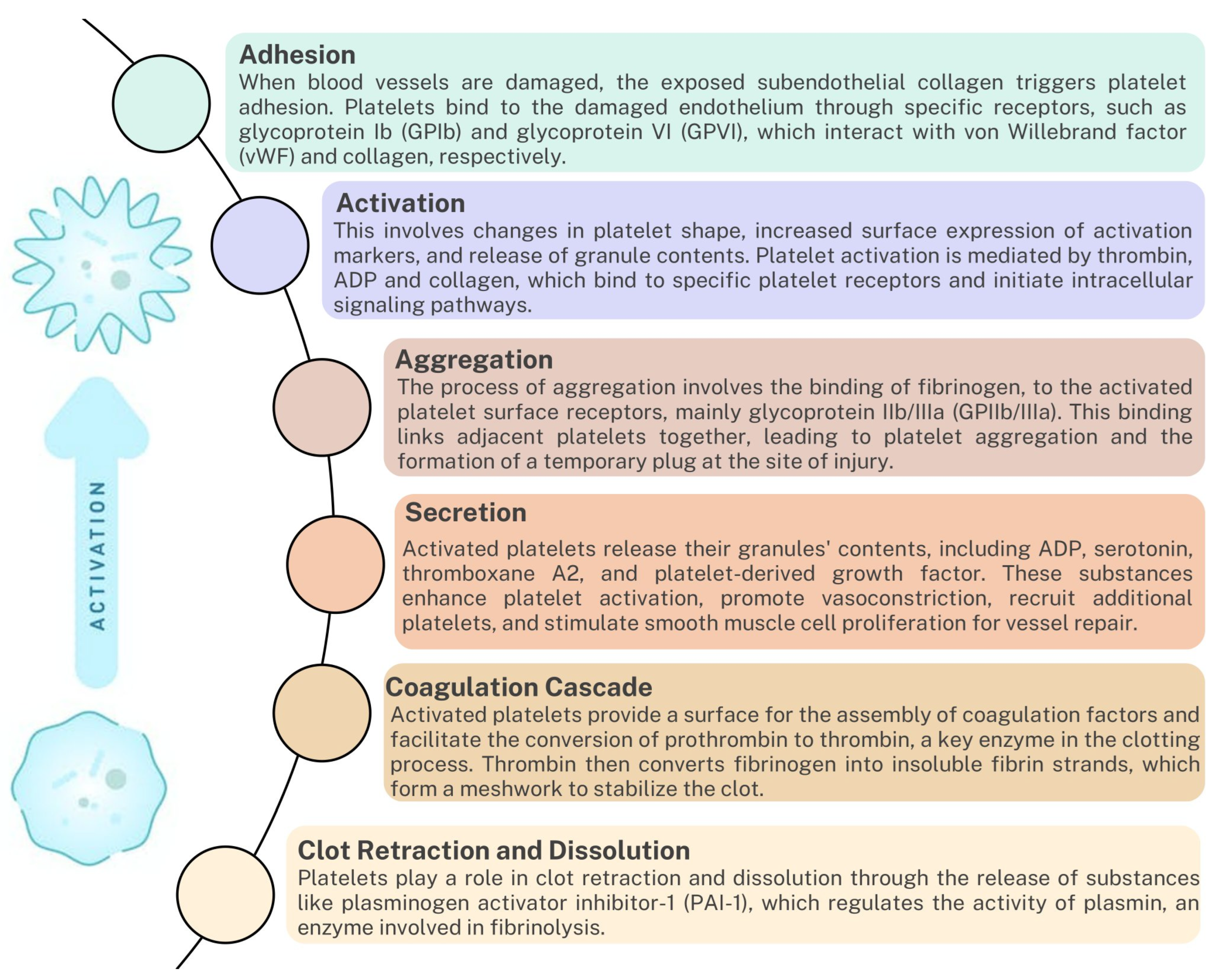
3.1. Platelets
3.2. Tissue Factor (TF)
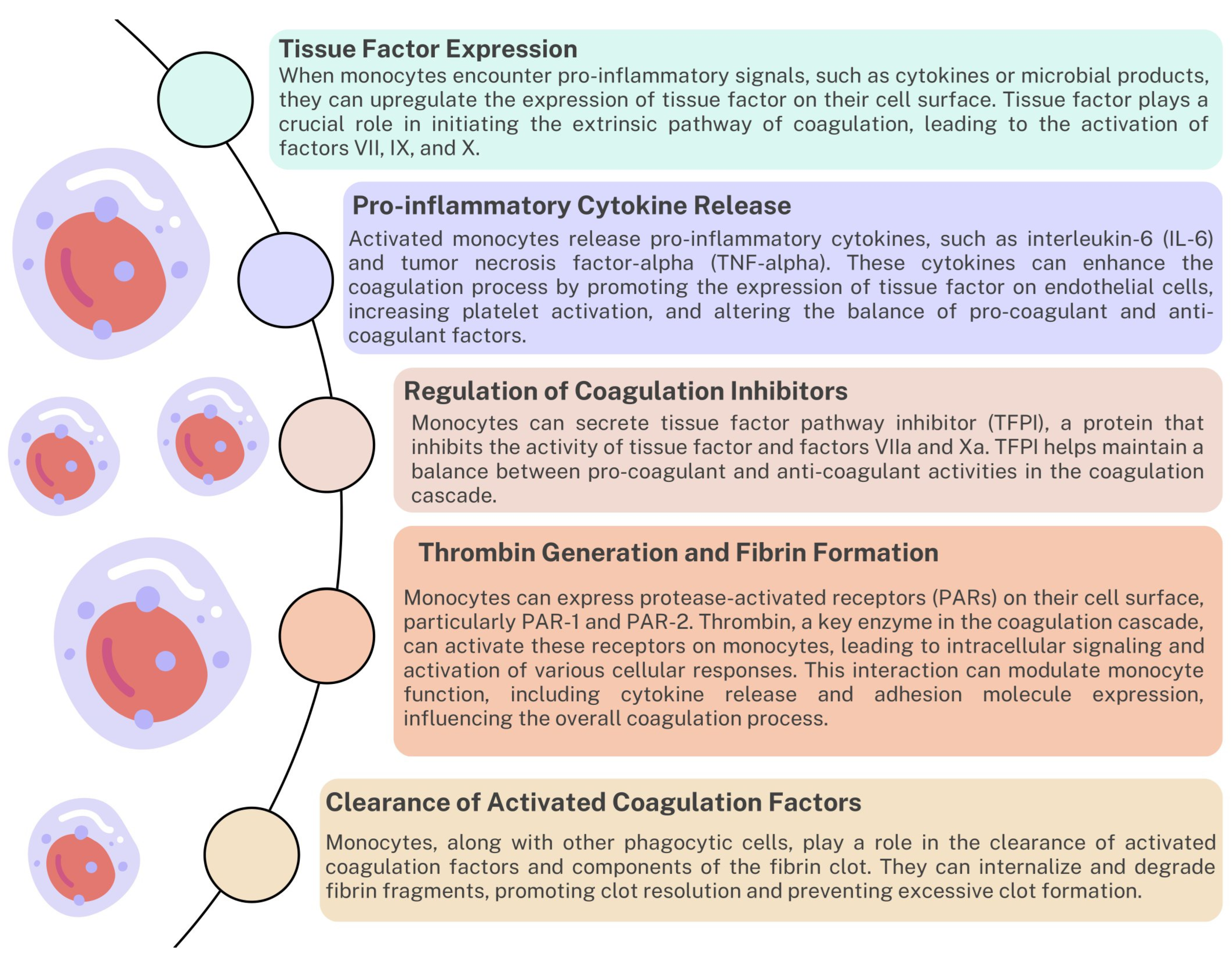
3.3. Monocytes/Macrophages
3.4. Neutrophils
3.5. Dendritic Cells
3.6. Lymphocytes
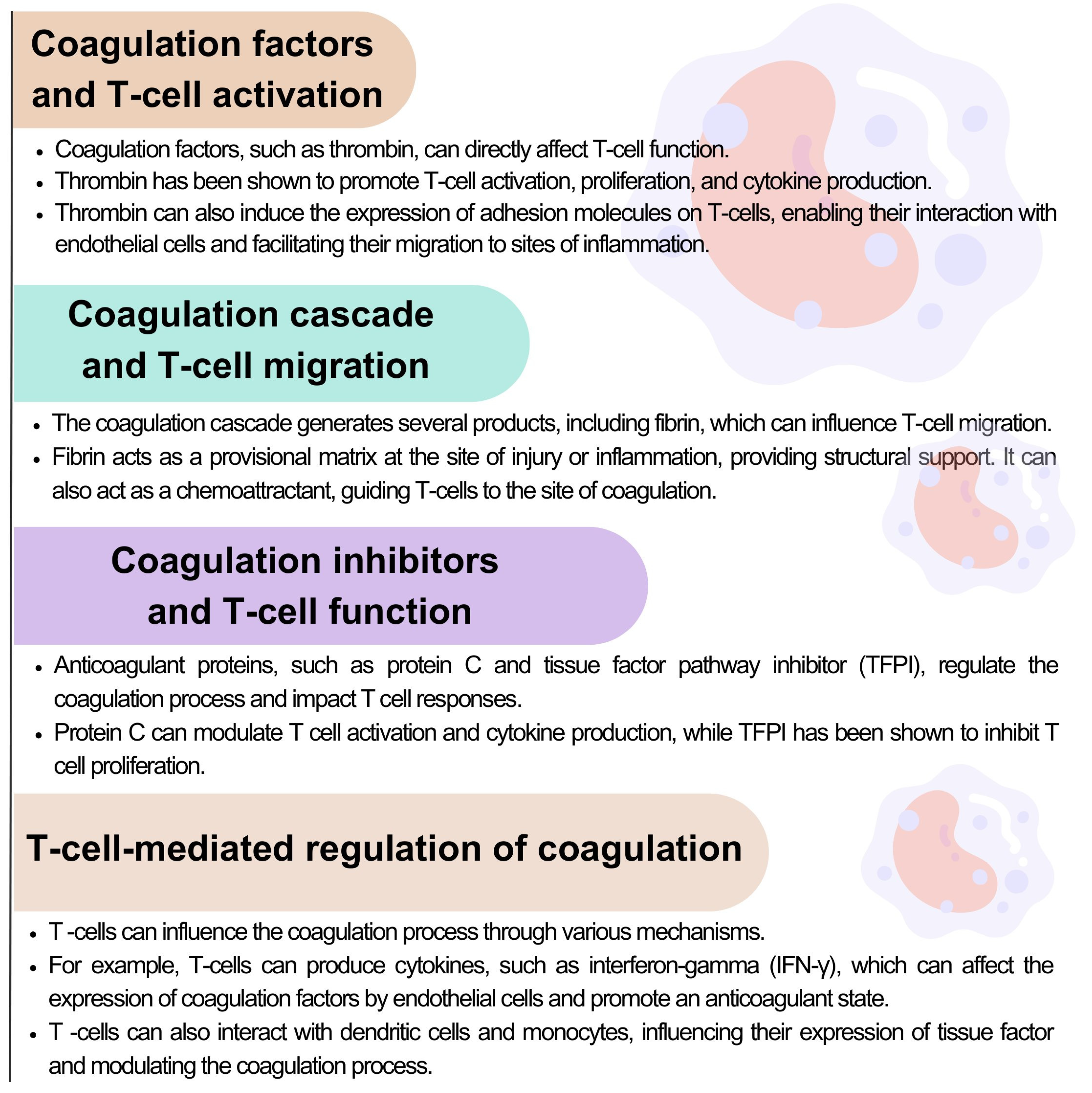
3.6.1. The Role of T Lymphocytes in the Coagulation Process

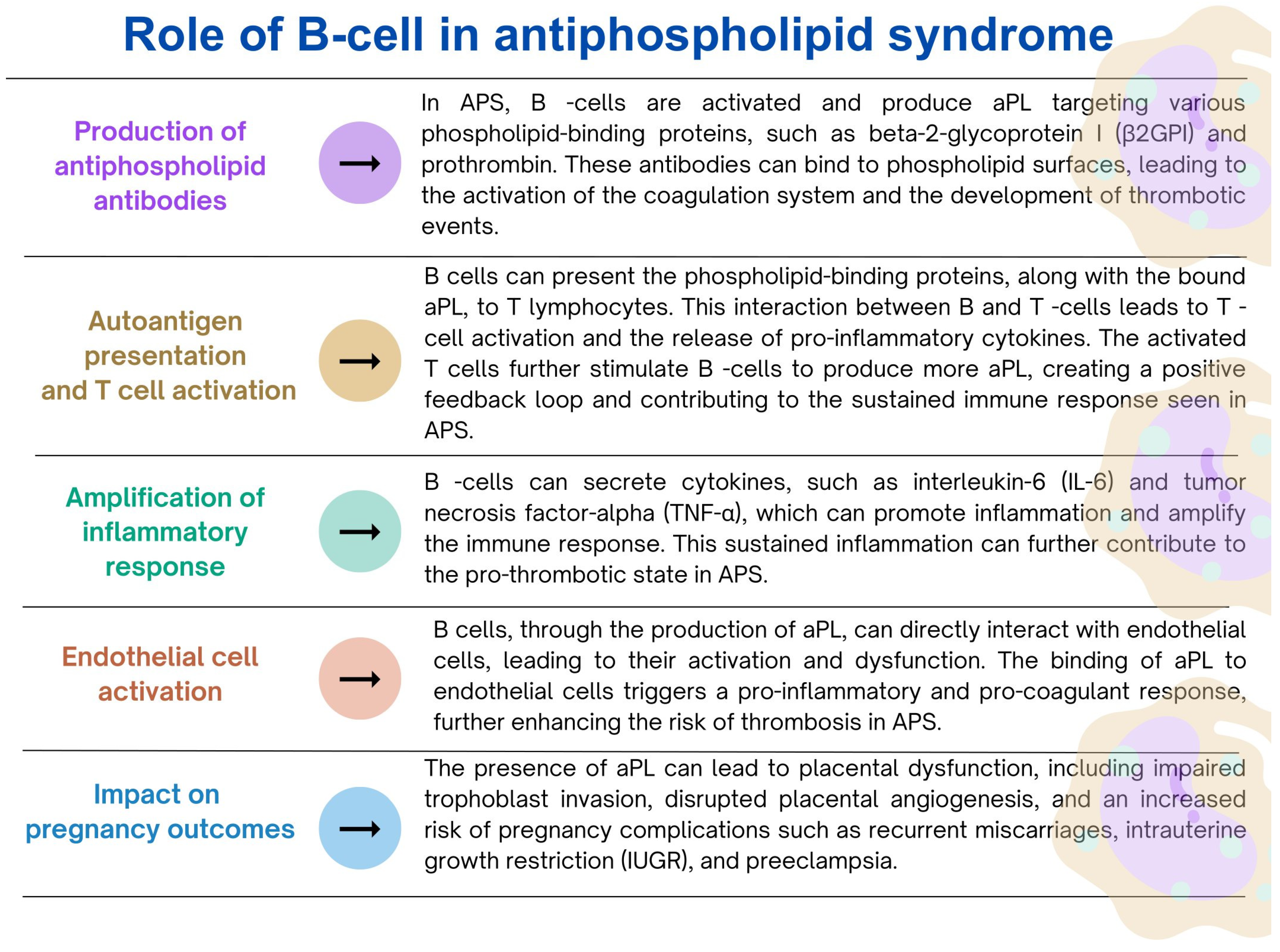
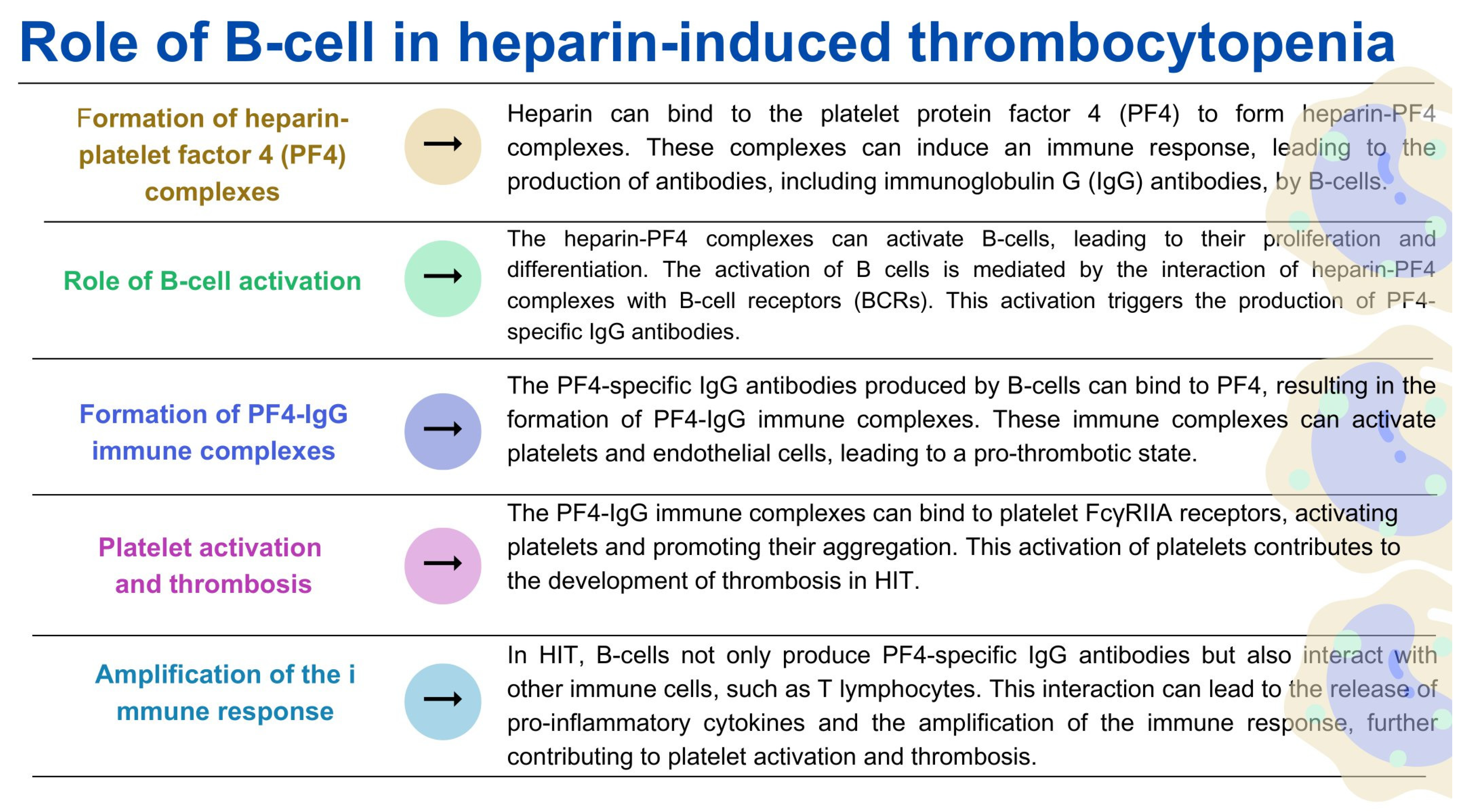
3.6.2. The role of B Lymphocytes in the Coagulation Process
4. The Role of the Coagulation System in Selected Disorders of the Immune System
4.1. Role of Immunotrombosis
4.2. Interrelations between Complement and Hemostasis
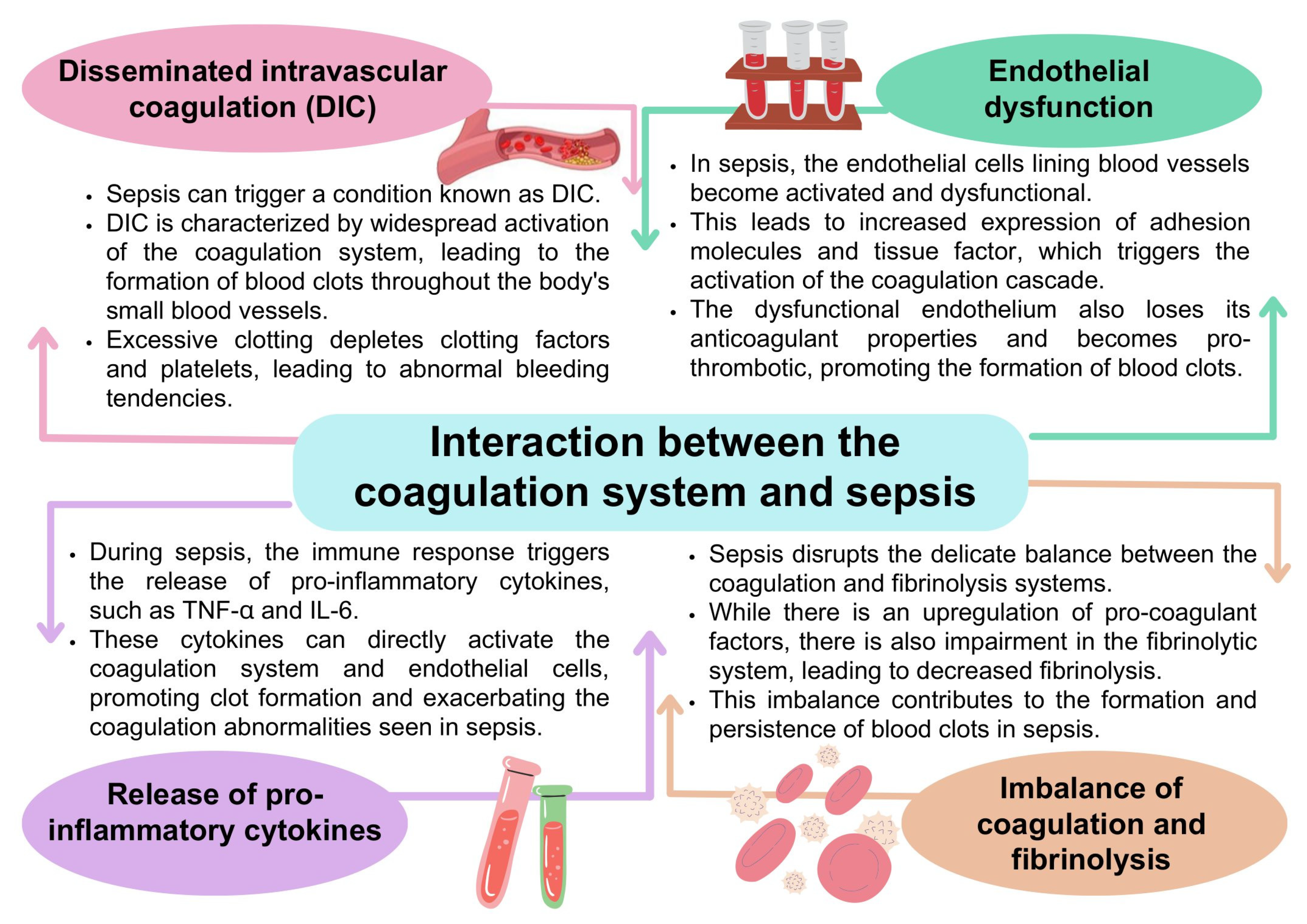
4.3. Coagulation Disorders and Sepsis
4.4. The Role of Coagulation Disorders in Autoimmune Diseases
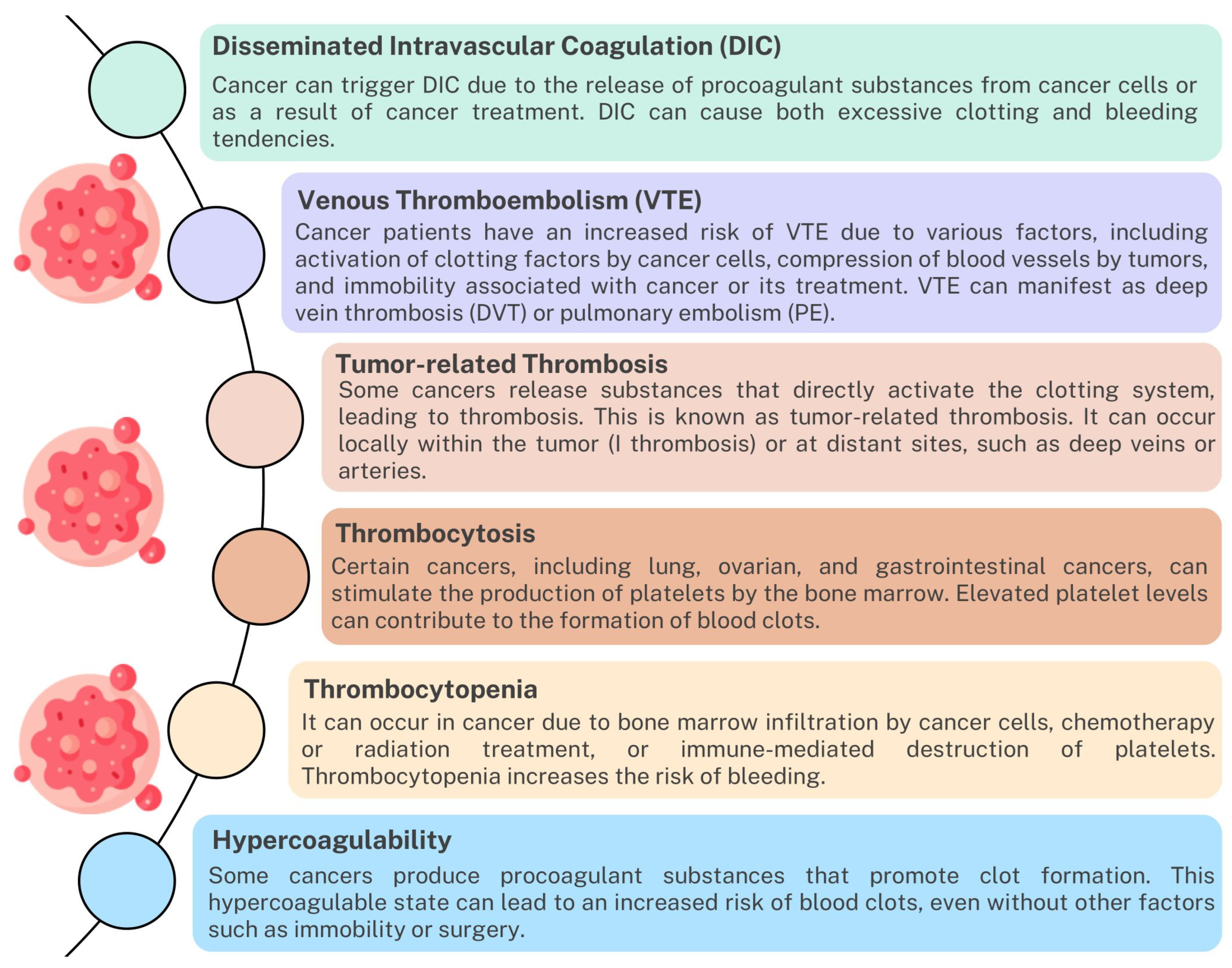
4.5. Disturbances of the Coagulation System in Neoplastic Diseases

4.5.1. Development of Inflammation
4.5.2. Angiogenesis
4.5.3. Coagulation Mediated by Immune Cells
4.6. Immunotherapy and Coagulation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Introduction to the Immune Response. In Primer Immune Response; Elsevier: Amsterdam, The Netherlands, 2014; pp. 3–20. [CrossRef]
- Mogensen, T.H. Pathogen Recognition and Inflammatory Signaling in Innate Immune Defenses. Clin. Microbiol. Rev. 2009, 22, 240–273. [Google Scholar] [CrossRef] [Green Version]
- Netea, M.G.; Domínguez-Andrés, J.; Barreiro, L.B.; Chavakis, T.; Divangahi, M.; Fuchs, E.; Joosten, L.A.B.; van der Meer, J.W.M.; Mhlanga, M.M.; Mulder, W.J.M.; et al. Defining trained immunity and its role in health and disease. Nat. Rev. Immunol. 2020, 20, 375–388. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Wu, L.; Yan, G.; Chen, Y.; Zhou, M.; Wu, Y.; Li, Y. Inflammation and tumor progression: Signaling pathways and targeted intervention. Signal Transduct. Target. Ther. 2021, 6, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.; Kawai, T.; Akira, S. Pathogen Recognition by the Innate Immune System. Int. Rev. Immunol. 2011, 30, 16–34. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Wu, M. Pattern recognition receptors in health and diseases. Signal Transduct. Target. Ther. 2021, 6, 291. [Google Scholar] [CrossRef] [PubMed]
- Palta, S.; Saroa, R.; Palta, A. Overview of the coagulation system. Indian J. Anaesth. 2014, 58, 515–523. [Google Scholar] [CrossRef]
- LaPelusa, A.; Dave, H.D. Physiology, Hemostasis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Golebiewska, E.M.; Poole, A.W. Platelet secretion: From haemostasis to wound healing and beyond. Blood Rev. 2015, 29, 153–162. [Google Scholar] [CrossRef]
- Chapin, J.C.; Hajjar, K.A. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015, 29, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Delvaeye, M.; Conway, E.M. Coagulation and innate immune responses: Can we view them separately? Blood 2009, 114, 2367–2374. [Google Scholar] [CrossRef]
- Dahlbäck, B.; Villoutreix, B.O. Regulation of Blood Coagulation by the Protein C Anticoagulant Pathway. Arter. Thromb. Vasc. Biol. 2005, 25, 1311–1320. [Google Scholar] [CrossRef] [Green Version]
- Popescu, N.I.; Lupu, C.; Lupu, F. Disseminated intravascular coagulation and its immune mechanisms. Blood 2022, 139, 1973–1986. [Google Scholar] [CrossRef] [PubMed]
- Tsantes, A.G.; Parastatidou, S.; Tsantes, E.A.; Bonova, E.; Tsante, K.A.; Mantzios, P.G.; Vaiopoulos, A.G.; Tsalas, S.; Konstantinidi, A.; Houhoula, D.; et al. Sepsis-Induced Coagulopathy: An Update on Pathophysiology, Biomarkers, and Current Guidelines. Life 2023, 13, 350. [Google Scholar] [CrossRef] [PubMed]
- Cantrell, R.; Palumbo, J.S. Hemostasis and tumor immunity. Res. Pract. Thromb. Haemost. 2022, 6, e12728. [Google Scholar] [CrossRef] [PubMed]
- Klavina, P.A.; Leon, G.; Curtis, A.M.; Preston, R.J. Dysregulated haemostasis in thrombo-inflammatory disease. Clin. Sci. 2022, 136, 1809–1829. [Google Scholar] [CrossRef]
- Foley, J.H.; Conway, E.M. Cross Talk Pathways Between Coagulation and Inflammation. Circ. Res. 2016, 118, 1392–1408. [Google Scholar] [CrossRef]
- Levi, M.; van der Poll, T.; Büller, H.R. Bidirectional Relation Between Inflammation and Coagulation. Circulation 2004, 109, 2698–2704. [Google Scholar] [CrossRef] [Green Version]
- Mackman, N. Role of Tissue Factor in Hemostasis, Thrombosis, and Vascular Development. Arter. Thromb. Vasc. Biol. 2004, 24, 1015–1022. [Google Scholar] [CrossRef] [Green Version]
- Neubauer, K.; Zieger, B. Endothelial cells and coagulation. Cell Tissue Res. 2022, 387, 391–398. [Google Scholar] [CrossRef]
- Adams, R.L.C.; Bird, R.J. Review article: Coagulation cascade and therapeutics update: Relevance to nephrology. Part 1: Overview of coagulation, thrombophilias and history of anticoagulants. Nephrology 2009, 14, 462–470. [Google Scholar] [CrossRef]
- Grover, S.P.; Mackman, N. Intrinsic Pathway of Coagulation and Thrombosis. Arter. Thromb. Vasc. Biol. 2019, 39, 331–338. [Google Scholar] [CrossRef]
- Chaudhry, R.; Usama, S.M.; Babiker, H.M. Physiology, Coagulation Pathways. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Göbel, K.; Eichler, S.; Wiendl, H.; Chavakis, T.; Kleinschnitz, C.; Meuth, S.G. The Coagulation Factors Fibrinogen, Thrombin, and Factor XII in Inflammatory Disorders—A Systematic Review. Front. Immunol. 2018, 9, 1731. [Google Scholar] [CrossRef] [Green Version]
- Al-Koussa, H.; AlZaim, I.; El-Sabban, M.E. Pathophysiology of Coagulation and Emerging Roles for Extracellular Vesicles in Coagulation Cascades and Disorders. J. Clin. Med. 2022, 11, 4932. [Google Scholar] [CrossRef] [PubMed]
- Esmon, C.T.; Xu, J.; Lupu, F. Innate immunity and coagulation. J. Thromb. Haemost. 2011, 9, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Antoniak, S. The coagulation system in host defense. Res. Pract. Thromb. Haemost. 2018, 2, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Keragala, C.B.; Draxler, D.F.; McQuilten, Z.K.; Medcalf, R.L. Haemostasis and innate immunity—A complementary relationship. Br. J. Haematol. 2018, 180, 782–798. [Google Scholar] [CrossRef] [Green Version]
- Burzynski, L.C.; Humphry, M.; Pyrillou, K.; Wiggins, K.A.; Chan, J.N.; Figg, N.; Kitt, L.L.; Summers, C.; Tatham, K.C.; Martin, P.B.; et al. The Coagulation and Immune Systems Are Directly Linked through the Activation of Interleukin-1α by Thrombin. Immunity 2019, 50, 1033–1042.e6. [Google Scholar] [CrossRef] [Green Version]
- Vilar, R.; Fish, R.J.; Casini, A.; Neerman-Arbez, M. Fibrin(ogen) in human disease: Both friend and foe. Haematologica 2020, 105, 284–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasconcelos, D.M.; Gonçalves, R.M.; Almeida, C.R.; Pereira, I.O.; Oliveira, M.I.; Neves, N.; Silva, A.M.; Ribeiro, A.C.; Cunha, C.; Almeida, A.R.; et al. Fibrinogen scaffolds with immunomodulatory properties promote in vivo bone regeneration. Biomaterials 2016, 111, 163–178. [Google Scholar] [CrossRef] [Green Version]
- Monroe, D.M.; Hoffman, M.; Roberts, H.R. Platelets and Thrombin Generation. Arter. Thromb. Vasc. Biol. 2002, 22, 1381–1389. [Google Scholar] [CrossRef] [Green Version]
- Hanby, H.A.; Bao, J.; Noh, J.-Y.; Jarocha, D.; Poncz, M.; Weiss, M.J.; Marks, M.S. Platelet dense granules begin to selectively accumulate mepacrine during proplatelet formation. Blood Adv. 2017, 1, 1478–1490. [Google Scholar] [CrossRef] [Green Version]
- Sharda, A.; Flaumenhaft, R. The life cycle of platelet granules. F1000Research 2018, 7, 236. [Google Scholar] [CrossRef]
- Blair, P.; Flaumenhaft, R. Platelet α-granules: Basic biology and clinical correlates. Blood Rev. 2009, 23, 177–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiteheart, S.W. Platelet granules: Surprise packages. Blood 2011, 118, 1190–1191. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.A.; Ashworth, K.J.; Di Paola, J.; Ku, D.N. Platelet α-granules are required for occlusive high-shear-rate thrombosis. Blood Adv. 2020, 4, 3258–3267. [Google Scholar] [CrossRef] [PubMed]
- Koenen, R.R.; Weber, C. Chemokines: Established and novel targets in atherosclerosis. EMBO Mol. Med. 2011, 3, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Morán, G.A.G.; Parra-Medina, R.; Cardona, A.G.; Quintero-Ronderos, P.; Rodríguez, É.G. Cytokines, Chemokines and Growth Factors. In Autoimmunity: From Bench to Bedside; El Rosario University Press: Bogota, Colombia, 2013. [Google Scholar]
- Rumbaut, R.E.; Thiagarajan, P. Platelet Aggregation. In Platelet-Vessel Wall Interactions in Hemostasis and Thrombosis; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2010. [Google Scholar]
- Amelirad, A.; Shamsasenjan, K.; Akbarzadehlaleh, P.; Sarvar, D.P. Signaling Pathways of Receptors Involved in Platelet Activation andShedding of These Receptors in Stored Platelets. Adv. Pharm. Bull. 2019, 9, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Scridon, A. Platelets and Their Role in Hemostasis and Thrombosis—From Physiology to Pathophysiology and Therapeutic Implications. Int. J. Mol. Sci. 2022, 23, 12772. [Google Scholar] [CrossRef]
- Heuberger, D.M.; Schuepbach, R.A. Protease-activated receptors (PARs): Mechanisms of action and potential therapeutic modulators in PAR-driven inflammatory diseases. Thromb. J. 2019, 17, 4. [Google Scholar] [CrossRef] [Green Version]
- Han, X.; Nieman, M.T.; Kerlin, B.A. Protease-activated receptors: An illustrated review. Res. Pract. Thromb. Haemost. 2020, 5, 17–26. [Google Scholar] [CrossRef]
- Renna, S.A.; McKenzie, S.E.; Michael, J.V. Species Differences in Platelet Protease-Activated Receptors. Int. J. Mol. Sci. 2023, 24, 8298. [Google Scholar] [CrossRef]
- Peng, Q.; Ratnasothy, K.; Boardman, D.A.; Jacob, J.; Tung, S.L.; McCluskey, D.; Smyth, L.A.; Lechler, R.I.; Dorling, A.; Lombardi, G. Protease Activated Receptor 4 as a Novel Modulator of Regulatory T Cell Function. Front. Immunol. 2019, 10, 1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadowski, P.P.; Weikert, C.; Pultar, J.; Lee, S.; Eichelberger, B.; Koppensteiner, R.; Lang, I.M.; Panzer, S.; Gremmel, T. Ticagrelor Inhibits Toll-Like and Protease-Activated Receptor Mediated Platelet Activation in Acute Coronary Syndromes. Cardiovasc. Drugs Ther. 2020, 34, 53–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhuo, X.; Wu, Y.; Fu, X.; Liang, X.; Xiang, Y.; Li, J.; Mao, C.; Jiang, Y. The Yin-Yang roles of protease-activated receptors in inflammatory signalling and diseases. FEBS J. 2022, 289, 4000–4020. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, S.; Ruf, W.; Bosmann, M. Advocacy of targeting protease-activated receptors in severe coronavirus disease 2019. Br. J. Pharmacol. 2022, 179, 2086–2099. [Google Scholar] [CrossRef]
- GP9—Platelet Glycoprotein IX—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P14770/entry#sequences (accessed on 15 June 2023).
- GP1BA—Platelet Glycoprotein Ib Alpha Chain—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P07359/entry (accessed on 15 June 2023).
- GP5—Platelet Glycoprotein V—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P40197/entry (accessed on 15 June 2023).
- GP6—Platelet Glycoprotein VI—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/Q9HCN6/entry (accessed on 15 June 2023).
- ITGA2—Integrin Alpha-2—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P17301/entry (accessed on 15 June 2023).
- ITGA6—Integrin Alpha-6—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P23229/entry (accessed on 15 June 2023).
- ITGAV—Integrin Alpha-V—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P06756/entry (accessed on 15 June 2023).
- ITGA2B—Integrin Alpha-IIb—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P08514/entry (accessed on 15 June 2023).
- F2R—Proteinase-Activated Receptor 1—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P25116/entry (accessed on 15 June 2023).
- F2RL3—Proteinase-Activated Receptor 4—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/Q96RI0/entry (accessed on 17 July 2023).
- P2RY1—P2Y Purinoceptor 1—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P47900/entry (accessed on 15 June 2023).
- P2RY12—P2Y Purinoceptor 12—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/Q9H244/entry (accessed on 15 June 2023).
- HTR2A—5-Hydroxytryptamine Receptor 2A—Homo Sapiens (Human)|UniProtKB|UniProt. Available online: https://www.uniprot.org/uniprotkb/P28223/entry (accessed on 15 June 2023).
- Rangaswamy, C.; Englert, H.; Deppermann, C.; Renné, T. Polyanions in Coagulation and Thrombosis: Focus on Polyphosphate and Neutrophils Extracellular Traps. Thromb. Haemost. 2021, 121, 1021–1030. [Google Scholar] [CrossRef]
- Periayah, M.H.; Halim, A.S.; Mat Saad, A.Z. Mechanism Action of Platelets and Crucial Blood Coagulation Pathways in Hemostasis. Int. J. Hematol. Oncol. Stem Cell Res. 2017, 11, 319–327. [Google Scholar]
- Sang, Y.; Roest, M.; de Laat, B.; de Groot, P.G.; Huskens, D. Interplay between platelets and coagulation. Blood Rev. 2021, 46, 100733. [Google Scholar] [CrossRef]
- Swieringa, F.; Spronk, H.M.; Heemskerk, J.W.; van der Meijden, P.E. Integrating platelet and coagulation activation in fibrin clot formation. Res. Pract. Thromb. Haemost. 2018, 2, 450–460. [Google Scholar] [CrossRef]
- Ahmadi, S.E.; Shabannezhad, A.; Kahrizi, A.; Akbar, A.; Safdari, S.M.; Hoseinnezhad, T.; Zahedi, M.; Sadeghi, S.; Mojarrad, M.G.; Safa, M. Tissue factor (coagulation factor III): A potential double-edge molecule to be targeted and re-targeted toward cancer. Biomark. Res. 2023, 11, 60. [Google Scholar] [CrossRef]
- Unruh, D.; Horbinski, C. Beyond thrombosis: The impact of tissue factor signaling in cancer. J. Hematol. Oncol. 2020, 13, 93. [Google Scholar] [CrossRef]
- Chu, A.J. Tissue Factor, Blood Coagulation, and Beyond: An Overview. Int. J. Inflamm. 2011, 2011, e367284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, S.A.; Pendurthi, U.R.; Sen, P.; Rao, L.V.M. The Role of Putative Phosphatidylserine-Interactive Residues of Tissue Factor on Its Coagulant Activity at the Cell Surface. PLoS ONE 2016, 11, e0158377. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Zhang, L.; Yu, C.; Yang, X.-F.; Wang, H. Monocyte and macrophage differentiation: Circulation inflammatory monocyte as biomarker for inflammatory diseases. Biomark. Res. 2014, 2, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shantsila, E.; Lip, G.Y.H. The role of monocytes in thrombotic disorders. Insights from Tissue Factor, Monocyte-Platelet Aggregates and Novel Mechanisms. Thromb. Haemost. 2009, 102, 916–924. [Google Scholar] [CrossRef]
- Peshkova, A.D.; Le Minh, G.; Tutwiler, V.; Andrianova, I.A.; Weisel, J.W.; Litvinov, R.I. Activated Monocytes Enhance Platelet-Driven Contraction of Blood Clots via Tissue Factor Expression. Sci. Rep. 2017, 7, 5149. [Google Scholar] [CrossRef] [Green Version]
- Shahneh, F.; Christian Probst, H.; Wiesmann, S.C.; A-Gonzalez, N.; Ruf, W.; Steinbrink, K.; Raker, V.K.; Becker, C. Inflammatory Monocyte Counts Determine Venous Blood Clot Formation and Resolution. Arter. Thromb. Vasc. Biol. 2022, 42, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Braun, O.; Zhang, S.; Norström, E.; Thorlacius, H.; Bader, J.E.; Enos, R.T.; Velázquez, K.T.; Carson, M.S.; Nagarkatti, M.; et al. Monocytes regulate systemic coagulation and inflammation in abdominal sepsis. Am. J. Physiol. Circ. Physiol. 2015, 308, H540–H547. [Google Scholar] [CrossRef]
- Bode, M.; Mackman, N. Regulation of tissue factor gene expression in monocytes and endothelial cells: Thromboxane A2 as a new player. Vasc. Pharmacol. 2014, 62, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Gerhardt, T.; Ley, K. Monocyte trafficking across the vessel wall. Cardiovasc. Res. 2015, 107, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Granger, D.N.; Senchenkova, E. Leukocyte–Endothelial Cell Adhesion. In Inflammation and the Microcirculation; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2010. [Google Scholar]
- Čejková, S.; Králová-Lesná, I.; Poledne, R. Monocyte adhesion to the endothelium is an initial stage of atherosclerosis development. Cor Vasa 2016, 58, e419–e425. [Google Scholar] [CrossRef]
- Hirayama, D.; Iida, T.; Nakase, H. The Phagocytic Function of Macrophage-Enforcing Innate Immunity and Tissue Homeostasis. Int. J. Mol. Sci. 2017, 19, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, P.J.; Wynn, T.A. Protective and pathogenic functions of macrophage subsets. Nat. Rev. Immunol. 2011, 11, 723–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duque, G.A.; Descoteaux, A. Macrophage Cytokines: Involvement in Immunity and Infectious Diseases. Front. Immunol. 2014, 5, 491. [Google Scholar] [CrossRef] [Green Version]
- Kerr, R.; Stirling, D.; Ludlam, C.A. Interleukin 6 and Haemostasis. Br. J. Haematol. 2001, 115, 3–12. [Google Scholar] [CrossRef]
- Montes-Worboys, A.; Rodriguez-Portal, J.A.; Arellano-Orden, E.; Digon-Pereiras, J.; Rodriguez-Panadero, F. Interleukin-8 activates coagulation and correlates with survival after talc pleurodesis. Eur. Respir. J. 2010, 35, 160–166. [Google Scholar] [CrossRef] [Green Version]
- Jovinge, S.; Ares, M.P.; Kallin, B.; Nilsson, J. Human Monocytes/Macrophages Release TNF-α in Response to Ox-LDL. Arter. Thromb. Vasc. Biol. 1996, 16, 1573–1579. [Google Scholar] [CrossRef]
- Poitevin, S.; Cochery-Nouvellon, E.; Dupont, A.; Nguyen, P. Monocyte IL-10 produced in response to lipopolysaccharide modulates thrombin generation by inhibiting tissue factor expression and release of active tissue factor-bound microparticles. Thromb. Haemost. 2007, 97, 598–607. [Google Scholar] [CrossRef]
- Alshehri, F.S.M.; Whyte, C.S.; Tuncay, A.; Williams, M.-L.; Wilson, H.M.; Mutch, N.J. Monocytes Expose Factor XIII-A and Stabilize Thrombi against Fibrinolytic Degradation. Int. J. Mol. Sci. 2021, 22, 6591. [Google Scholar] [CrossRef]
- Calafat, J.; Janssen, H.; Ståhle-Bäckdahl, M.S.; Zuurbier, A.E.; Knol, E.F.; Egesten, A. Human Monocytes and Neutrophils Store Transforming Growth Factor-α in a Subpopulation of Cytoplasmic Granules. Blood 1997, 90, 1255–1266. [Google Scholar] [CrossRef]
- Wang, Z.; Zhou, Q.; Liu, H.; Zhang, J.; Zhu, Z.; Wu, J.; Chen, X.; Liu, Y. Association Between Monocyte Count and Preoperative Deep Venous Thrombosis in Older Patients with hip Fracture: A Retrospective Study. Clin. Appl. Thromb. 2022, 28. [Google Scholar] [CrossRef]
- Karahan, S.; Okuyan, E. Role of Systemic Inflammatory Markers in Pulmonary Embolism Severity and Mortality. Exp. Appl. Med. Sci. 2021, 2, 189–196. [Google Scholar] [CrossRef]
- Białas, A.J.; Kornicki, K.; Ciebiada, M.; Antczak, A.; Sitarek, P.; Miłkowska-Dymanowska, J.; Piotrowski, W.J.; Górski, P. Monocyte to large platelet ratio as a diagnostic tool of pulmonary embolism in patients with acute exacerbation of COPD. Pol. Arch. Med. Wewnętrznej 2017, 128, 906–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Z.; Liu, Q.; Li, H.; Zhang, M.; You, L.; Lin, Y.; Wang, K.; Gou, Q.; Wang, Z.; Zhou, S.; et al. The role of monocytes in thrombotic diseases: A review. Front. Cardiovasc. Med. 2023, 10, 1113827. [Google Scholar] [CrossRef]
- Jang, H.J.; Schellingerhout, D.; Kim, J.; Chung, J.; Kim, D.-E. Towards a biomarker for acute arterial thrombosis using complete blood count and white blood cell differential parameters in mice. Sci. Rep. 2023, 13, 4043. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.; Kim, J.-E.; Park, S.; Han, K.-S.; Kim, H.K. Neutrophil and monocyte activation markers have prognostic impact in disseminated intravascular coagulation: In vitro effect of thrombin on monocyte CD163 shedding. Thromb. Res. 2011, 127, 450–456. [Google Scholar] [CrossRef]
- Blbulyan, A.; Martirosyan, A.; Petrek, M.; Navratilova, Z.; Manukyan, G. Antiphospholipid syndrome and monocytes: New aspects. Georgian Med. News 2017, 12–17. [Google Scholar]
- Štok, U.; Štucin, N.; Blokar, E.; Ambrožič, A.; Sodin-Šemrl, S.; Čučnik, S.; Žigon, P. Antiphospholipid Antibody Syndrome-Associated Increased Surface Expression of VLA4 Integrin on Human Monocytes. Biomedicines 2022, 10, 2341. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.L.; Sadler, J.E. Pathogenesis of Thrombotic Microangiopathies. Annu. Rev. Pathol. Mech. Dis. 2008, 3, 249–277. [Google Scholar] [CrossRef] [PubMed]
- Copelovitch, L.; Kaplan, B.S. The thrombotic microangiopathies. Pediatr. Nephrol. 2008, 23, 1761–1767. [Google Scholar] [CrossRef] [Green Version]
- Maldonado-Peña, J.; Rivera, K.; Ortega, C.; Betancourt, M.; Lugo, J.E.; Camargo, E. Can monocytosis act as an independent variable for predicting deep vein thrombosis? Int. J. Cardiol. 2016, 219, 282–284. [Google Scholar] [CrossRef]
- Rosales, C. Neutrophil: A Cell with Many Roles in Inflammation or Several Cell Types? Front. Physiol. 2018, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, S.; Opneja, A.; Nayak, L. The role of neutrophils in thrombosis. Thromb. Res. 2018, 170, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Rizo, V.; Martínez-Guzmán, M.A.; Iñiguez-Gutierrez, L.; García-Orozco, A.; Alvarado-Navarro, A.; Fafutis-Morris, M. Neutrophil Extracellular Traps and Its Implications in Inflammation: An Overview. Front. Immunol. 2017, 8, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirakawa, K.; Sano, M. Neutrophils and Neutrophil Extracellular Traps in Cardiovascular Disease: An Overview and Potential Therapeutic Approaches. Biomedicines 2022, 10, 1850. [Google Scholar] [CrossRef]
- Li, T.; Zhang, Z.; Li, X.; Dong, G.; Zhang, M.; Xu, Z.; Yang, J. Neutrophil Extracellular Traps: Signaling Properties and Disease Relevance. Mediat. Inflamm. 2020, 2020, 9254087. [Google Scholar] [CrossRef]
- Noubouossie, D.F.; Whelihan, M.F.; Yu, Y.-B.; Sparkenbaugh, E.; Pawlinski, R.; Monroe, D.M.; Key, N.S. In vitro activation of coagulation by human neutrophil DNA and histone proteins but not neutrophil extracellular traps. Blood 2017, 129, 1021–1029. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Brill, A.; Duerschmied, D.; Schatzberg, D.; Monestier, M.; Myers, D.D.; Wrobleski, S.K.; Wakefield, T.W.; Hartwig, J.H.; Wagner, D.D. Extracellular DNA traps promote thrombosis. Proc. Natl. Acad. Sci. USA 2010, 107, 15880–15885. [Google Scholar] [CrossRef]
- Carestia, A.; Kaufman, T.; Schattner, M. Platelets: New Bricks in the Building of Neutrophil Extracellular Traps. Front. Immunol. 2016, 7, 271. [Google Scholar] [CrossRef] [Green Version]
- Pitchford, S.; Pan, D.; Welch, H.C. Platelets in neutrophil recruitment to sites of inflammation. Curr. Opin. Hematol. 2017, 24, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Lam, F.W.; Vijayan, K.V.; Rumbaut, R.E. Platelets and Their Interactions with Other Immune Cells. Compr. Physiol. 2015, 5, 1265–1280. [Google Scholar] [CrossRef]
- Rossaint, J.; Margraf, A.; Zarbock, A. Role of Platelets in Leukocyte Recruitment and Resolution of Inflammation. Front. Immunol. 2018, 9, 2712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Futosi, K.; Fodor, S.; Mócsai, A. Neutrophil cell surface receptors and their intracellular signal transduction pathways. Int. Immunopharmacol. 2013, 17, 638–650. [Google Scholar] [CrossRef] [Green Version]
- Zarbock, A.; Ley, K. Neutrophil Adhesion and Activation under Flow. Microcirculation 2009, 16, 31–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noubouossie, D.F.; Reeves, B.N.; Strahl, B.D.; Key, N.S. Neutrophils: Back in the thrombosis spotlight. Blood 2019, 133, 2186–2197. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Xin, L.; Xiao, X.; Huang, Y.; Lin, C.; Liu, X.; Wei, H.; Xu, R.; Chen, Y. Neutrophils: As a Key Bridge between Inflammation and Thrombosis. Evid.-Based Complement. Altern. Med. 2022, 2022, e1151910. [Google Scholar] [CrossRef] [PubMed]
- Wang, J. Neutrophils in tissue injury and repair. Cell Tissue Res. 2018, 371, 531–539. [Google Scholar] [CrossRef] [Green Version]
- Wilgus, T.A.; Roy, S.; McDaniel, J.C.; Sweere, J.M.; Ishak, H.; Sunkari, V.; Bach, M.S.; Manasherob, R.; Yadava, K.; Ruppert, S.M.; et al. Neutrophils and Wound Repair: Positive Actions and Negative Reactions. Adv. Wound Care 2013, 2, 379–388. [Google Scholar] [CrossRef] [Green Version]
- Flaumenhaft, R. Dendritic Cells Inflamed by Coagulation. Hematologist 2008, 5. [Google Scholar] [CrossRef]
- Niessen, F.; Schaffner, F.; Furlan-Freguia, C.; Pawlinski, R.; Bhattacharjee, G.; Chun, J.; Derian, C.K.; Andrade-Gordon, P.; Rosen, H.; Ruf, W. Dendritic cell PAR1–S1P3 signalling couples coagulation and inflammation. Nature 2008, 452, 654–658. [Google Scholar] [CrossRef] [Green Version]
- Ruf, W.; Furlan-Freguia, C.; Niessen, F. Vascular and dendritic cell coagulation signaling in sepsis progression. J. Thromb. Haemost. 2009, 7, 118–121. [Google Scholar] [CrossRef] [Green Version]
- Summerfield, A.; McCullough, K.C. Dendritic Cells in Innate and Adaptive Immune Responses against Influenza Virus. Viruses 2009, 1, 1022–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mellman, I. Dendritic Cells: Master Regulators of the Immune Response. Cancer Immunol. Res. 2013, 1, 145–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrivastava, S.; Ma, L.; Tham, E.-L.; McVey, J.H.; Chen, D.; Dorling, A. Protease-activated receptor-2 signalling by tissue factor on dendritic cells suppresses antigen-specific CD4+T-cell priming. Immunology 2013, 139, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Toda, M.; D’Alessandro-Gabazza, C.N.; Takagi, T.; Chelakkot-Govindalayathila, A.-L.; Taguchi, O.; Roeen, Z.; Munesue, S.; Yamamoto, Y.; Yamamoto, H.; Gabazza, E.C.; et al. Thrombomodulin Modulates Dendritic Cells via Both Antagonism of High Mobility Group Protein B1 and an Independent Mechanism. Allergol. Int. 2014, 63, 57–66. [Google Scholar] [CrossRef]
- Yanagita, M.; Kobayashi, R.; Kashiwagi, Y.; Shimabukuro, Y.; Murakami, S. Thrombin regulates the function of human blood dendritic cells. Biochem. Biophys. Res. Commun. 2007, 364, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Syrovets, T.; Paskas, S.; Laumonnier, Y.; Simmet, T. Mature Dendritic Cells Express Functional Thrombin Receptors Triggering Chemotaxis and CCL18/Pulmonary and Activation-Regulated Chemokine Induction. J. Immunol. 2008, 181, 1215–1223. [Google Scholar] [CrossRef] [Green Version]
- Larosa, D.; Orange, J. 1. Lymphocytes. J. Allergy Clin. Immunol. 2008, 121, S364–S369, quiz S412. [Google Scholar] [CrossRef]
- Appay, V.; van Lier, R.A.W.; Sallusto, F.; Roederer, M. Phenotype and function of human T lymphocyte subsets: Consensus and issues. Cytom. Part A 2008, 73, 975–983. [Google Scholar] [CrossRef]
- Hohlstein, P.; Gussen, H.; Bartneck, M.; Warzecha, K.T.; Roderburg, C.; Buendgens, L.; Trautwein, C.; Koch, A.; Tacke, F. Prognostic Relevance of Altered Lymphocyte Subpopulations in Critical Illness and Sepsis. J. Clin. Med. 2019, 8, 353. [Google Scholar] [CrossRef] [Green Version]
- LeBien, T.W.; Tedder, T.F. B lymphocytes: How they develop and function. Blood 2008, 112, 1570–1580. [Google Scholar] [CrossRef] [Green Version]
- Tobón, G.J.; Izquierdo, J.H.; Cañas, C.A. B Lymphocytes: Development, Tolerance, and Their Role in Autoimmunity—Focus on Systemic Lupus Erythematosus. Autoimmune Dis. 2013, 2013, e827254. [Google Scholar] [CrossRef] [Green Version]
- Bouchard, B.A.; Tracy, P.B. The participation of leukocytes in coagulant reactions. J. Thromb. Haemost. 2003, 1, 464–469. [Google Scholar] [CrossRef] [Green Version]
- Cao, O.; Loduca, P.A.; Herzog, R.W. Role of regulatory T cells in tolerance to coagulation factors. J. Thromb. Haemost. 2009, 7, 88–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinha, A.; Ma, Y.; Scherzer, R.; Hur, S.; Li, D.; Ganz, P.; Deeks, S.G.; Hsue, P.Y. Role of T-Cell Dysfunction, Inflammation, and Coagulation in Microvascular Disease in HIV. J. Am. Heart Assoc. 2016, 5, e004243. [Google Scholar] [CrossRef]
- Shen, N.L.; Fan, S.T.; Pyati, J.; Graff, R.; LaPolla, R.J.; Edgington, T.S. The serine protease cofactor factor V is synthesized by lymphocytes. J. Immunol. 1993, 150, 2992–3001. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Song, H.; Xu, W.; Xu, J.; Jiang, J.; Gong, Z.; Liu, Y.; Yan, W.; Wang, L. Immune function of peripheral T cells in patients with venous thromboembolism or coronary artery atherosclerosis. Rev. Port. Cardiol. 2014, 33, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S.; Gabre, J.; Chabasse, C.; Bromberg, J.S.; Antalis, T.M.; Sarkar, R. Depletion of CD4 and CD8 Positive T Cells Impairs Venous Thrombus Resolution in Mice. Int. J. Mol. Sci. 2020, 21, 1650. [Google Scholar] [CrossRef] [Green Version]
- Luther, N.; Shahneh, F.; Brähler, M.; Krebs, F.; Jäckel, S.; Subramaniam, S.; Stanger, C.; Schönfelder, T.; Kleis-Fischer, B.; Reinhardt, C.; et al. Innate Effector-Memory T-Cell Activation Regulates Post-Thrombotic Vein Wall Inflammation and Thrombus Resolution. Circ. Res. 2016, 119, 1286–1295. [Google Scholar] [CrossRef]
- Budnik, I.; Brill, A. Immune Factors in Deep Vein Thrombosis Initiation. Trends Immunol. 2018, 39, 610–623. [Google Scholar] [CrossRef]
- Prochaska, J.H.; Luther, N.; Brähler, M.; Schulz, A.; Hermanns, M.I.; Lackner, K.J.; Espinola-Klein, C.; Münzel, T.; Wild, P.S.; Becker, C. Acute deep vein thrombosis suppresses peripheral T cell effector function. Br. J. Haematol. 2019, 184, 847–850. [Google Scholar] [CrossRef]
- Lei, H.; Schmidt-Bleek, K.; Dienelt, A.; Reinke, P.; Volk, H.-D. Regulatory T cell-mediated anti-inflammatory effects promote successful tissue repair in both indirect and direct manners. Front. Pharmacol. 2015, 6, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahneh, F.; Grill, A.; Klein, M.; Frauhammer, F.; Bopp, T.; Schäfer, K.; Raker, V.K.; Becker, C. Specialized regulatory T cells control venous blood clot resolution through SPARC. Blood 2021, 137, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Bayati, F.; Mohammadi, M.; Valadi, M.; Jamshidi, S.; Foma, A.M.; Sharif-Paghaleh, E. The Therapeutic Potential of Regulatory T Cells: Challenges and Opportunities. Front. Immunol. 2021, 11, 585819. [Google Scholar] [CrossRef]
- Zouggari, Y.; Ait-Oufella, H.; Waeckel, L.; Vilar, J.; Loinard, C.; Cochain, C.; Récalde, A.; Duriez, M.; Levy, B.I.; Lutgens, E.; et al. Regulatory T Cells Modulate Postischemic Neovascularization. Circulation 2009, 120, 1415–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maga, P.; Mikolajczyk, T.P.; Partyka, L.; Siedlinski, M.; Maga, M.; Krzanowski, M.; Malinowski, K.; Luc, K.; Nizankowski, R.; Bhatt, D.L.; et al. Involvement of CD8+ T cell subsets in early response to vascular injury in patients with peripheral artery disease in vivo. Clin. Immunol. 2018, 194, 26–33. [Google Scholar] [CrossRef]
- Weyand, C.M.; Younge, B.R.; Goronzy, J.J. T cells in arteritis and atherosclerosis. Curr. Opin. Infect. Dis. 2008, 19, 469–477. [Google Scholar] [CrossRef] [Green Version]
- Tabas, I.; Lichtman, A.H. Monocyte-Macrophages and T Cells in Atherosclerosis. Immunity 2017, 47, 621–634. [Google Scholar] [CrossRef] [Green Version]
- Senchenkova, E.Y.; Russell, J.; Yildirim, A.; Granger, D.N.; Gavins, F.N. Novel Role of T Cells and IL-6 (Interleukin-6) in Angiotensin II–Induced Microvascular Dysfunction. Hypertension 2019, 73, 829–838. [Google Scholar] [CrossRef]
- Cano, R.L.E.; Lopera, H.D.E. Introduction to T and B Lymphocytes. In Autoimmunity: From Bench to Bedside; El Rosario University Press: Bogota, Colombia, 2013. [Google Scholar]
- Alberts, B.; Johnson, A.; Lewis, J.; Raff, M.; Roberts, K.; Walter, P. B Cells and Antibodies. In Molecular Biology of the Cell, 4th ed.; Garland Science: New York, NY, USA, 2002. [Google Scholar]
- Galli, M.; Barbui, T. Antiprothrombin Antibodies: Detection and Clinical Significance in the Antiphospholipid Syndrome. Blood 1999, 93, 2149–2157. [Google Scholar] [CrossRef]
- Chan, J.P.; Merlini, M.; Gao, H.-X.; Mendiola, A.S.; Akassoglou, K.; Rubenstein, J.L.; Ryu, J.K. Blood Coagulation Factor Fibrinogen in Tumor Pathogenesis of Central Nervous System B-Cell Lymphoma. Am. J. Pathol. 2021, 191, 575–583. [Google Scholar] [CrossRef]
- Skupsky, J.; Zhang, A.-H.; Su, Y.; Scott, D.W. A role for thrombin in the initiation of the immune response to therapeutic factor VIII. Blood 2009, 114, 4741–4748. [Google Scholar] [CrossRef] [Green Version]
- Hansson, G.K. The B Cell. Arter. Thromb. Vasc. Biol. 2002, 22, 523–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasselwander, S.; Xia, N.; Mimmler, M.; Ascher, S.; Knopp, T.; Reifenberg, G.; Karbach, S.; Ruf, W.; Reinhardt, C.; Li, H. B lymphocyte-deficiency in mice promotes venous thrombosis. Heliyon 2022, 8, e11740. [Google Scholar] [CrossRef] [PubMed]
- Youinou, P.; Renaudineau, Y. The antiphospholipid syndrome as a model for B cell-induced autoimmune diseases. Thromb. Res. 2004, 114, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Dieudonné, Y.; Guffroy, A.; Poindron, V.; Sprauel, P.S.; Martin, T.; Korganow, A.-S.; Gies, V. B cells in primary antiphospholipid syndrome: Review and remaining challenges. Autoimmun. Rev. 2021, 20, 102798. [Google Scholar] [CrossRef]
- Hoogen, L.L.v.D.; Bisoendial, R.J. B-Cells and BAFF in Primary Antiphospholipid Syndrome, Targets for Therapy? J. Clin. Med. 2023, 12, 18. [Google Scholar] [CrossRef]
- Zheng, Y.; Wang, A.W.; Yu, M.; Padmanabhan, A.; Tourdot, B.E.; Newman, D.K.; White, G.C.; Aster, R.H.; Wen, R.; Wang, D. B-cell tolerance regulates production of antibodies causing heparin-induced thrombocytopenia. Blood 2014, 123, 931–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandelwal, S.; Lee, G.M.; Hester, C.G.; Poncz, M.; McKenzie, S.E.; Sachais, B.S.; Rauova, L.; Kelsoe, G.; Cines, D.B.; Frank, M.; et al. The antigenic complex in HIT binds to B cells via complement and complement receptor 2 (CD21). Blood 2016, 128, 1789–1799. [Google Scholar] [CrossRef] [Green Version]
- Staibano, P.; Arnold, D.M.; Bowdish, D.M.E.; Nazy, I. The unique immunological features of heparin-induced thrombocytopenia. Br. J. Haematol. 2017, 177, 198–207. [Google Scholar] [CrossRef] [Green Version]
- Warkentin, T.E. B cells, PF4/heparin complexes, and complement. Blood 2016, 128, 1781–1782. [Google Scholar] [CrossRef] [Green Version]
- Cosmi, B. Heparin-induced thrombocytopenia: New insights into the immune response. Transl. Cancer Res. 2017, 6, S145–S148. [Google Scholar] [CrossRef]
- Bakchoul, T.; Greinacher, A. Recent advances in the diagnosis and treatment of heparin-induced thrombocytopenia. Ther. Adv. Hematol. 2012, 3, 237–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelmann, B.; Massberg, S. Thrombosis as an intravascular effector of innate immunity. Nat. Rev. Immunol. 2013, 13, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.A.J.; O’Neill, L.A.J. Innate immune signaling and immunothrombosis: New insights and therapeutic opportunities. Eur. J. Immunol. 2022, 52, 1024–1034. [Google Scholar] [CrossRef]
- Marcos-Jubilar, M.; Lecumberri, R.; Páramo, J.A. Immunothrombosis: Molecular Aspects and New Therapeutic Perspectives. J. Clin. Med. 2023, 12, 1399. [Google Scholar] [CrossRef]
- Middleton, E.A.; He, X.-Y.; Denorme, F.; Campbell, R.A.; Ng, D.; Salvatore, S.P.; Mostyka, M.; Baxter-Stoltzfus, A.; Borczuk, A.C.; Loda, M.; et al. Neutrophil extracellular traps contribute to immunothrombosis in COVID-19 acute respiratory distress syndrome. Blood 2020, 136, 1169–1179. [Google Scholar] [CrossRef]
- Thierry, A.R.; Roch, B. Neutrophil Extracellular Traps and By-Products Play a Key Role in COVID-19: Pathogenesis, Risk Factors, and Therapy. J. Clin. Med. 2020, 9, 2942. [Google Scholar] [CrossRef]
- Zaid, Y.; Merhi, Y. Implication of Platelets in Immuno-Thrombosis and Thrombo-Inflammation. Front. Cardiovasc. Med. 2022, 9, 863846. [Google Scholar] [CrossRef]
- Ebermeyer, T.; Cognasse, F.; Berthelot, P.; Mismetti, P.; Garraud, O.; Hamzeh-Cognasse, H. Platelet Innate Immune Receptors and TLRs: A Double-Edged Sword. Int. J. Mol. Sci. 2021, 22, 7894. [Google Scholar] [CrossRef]
- Pryzdial, E.L.G.; Leatherdale, A.; Conway, E.M. Coagulation and complement: Key innate defense participants in a seamless web. Front. Immunol. 2022, 13, 918775. [Google Scholar] [CrossRef]
- Conway, E.M. Complement-coagulation connections. Blood Coagul. Fibrinolysis 2018, 29, 243–251. [Google Scholar] [CrossRef]
- Kenawy, H.I.; Boral, I.; Bevington, A. Complement-Coagulation Cross-Talk: A Potential Mediator of the Physiological Activation of Complement by Low pH. Front. Immunol. 2015, 6, 215. [Google Scholar] [CrossRef] [Green Version]
- Oikonomopoulou, K.; Ricklin, D.; Ward, P.A.; Lambris, J.D. Interactions between coagulation and complement—Their role in inflammation. Semin. Immunopathol. 2012, 34, 151–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simmons, J.; Pittet, J.-F. The coagulopathy of acute sepsis. Curr. Opin. Anaesthesiol. 2015, 28, 227–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellinger, R.P. Inflammation and Coagulation: Implications for the Septic Patient. Clin. Infect. Dis. 2003, 36, 1259–1265. [Google Scholar] [CrossRef]
- Fiusa, M.M.L.; Carvalho-Filho, M.A.; Annichino-Bizzacchi, J.M.; De Paula, E.V. Causes and consequences of coagulation activation in sepsis: An evolutionary medicine perspective. BMC Med. 2015, 13, 105. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- van der Poll, T.; Shankar-Hari, M.; Wiersinga, W.J. The immunology of sepsis. Immunity 2021, 54, 2450–2464. [Google Scholar] [CrossRef]
- Scarlatescu, E.; Tomescu, D.; Arama, S.S. Sepsis-Associated Coagulopathy. J. Crit. Care Med. 2016, 2, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Levi, M.; van der Poll, T. Coagulation and sepsis. Thromb. Res. 2017, 149, 38–44. [Google Scholar] [CrossRef]
- Maneta, E.; Aivalioti, E.; Tual-Chalot, S.; Veseli, B.E.; Gatsiou, A.; Stamatelopoulos, K.; Stellos, K. Endothelial dysfunction and immunothrombosis in sepsis. Front. Immunol. 2023, 14, 1144229. [Google Scholar] [CrossRef]
- Tsao, C.-M.; Ho, S.-T.; Wu, C.-C. Coagulation abnormalities in sepsis. Acta Anaesthesiol. Taiwanica 2015, 53, 16–22. [Google Scholar] [CrossRef]
- Shannon, O. The role of platelets in sepsis. Res. Pract. Thromb. Haemost. 2021, 5, 27–37. [Google Scholar] [CrossRef]
- Dixon, B. The Role of Microvascular Thrombosis in Sepsis. Anaesth. Intensiv. Care 2004, 32, 619–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinhart, K.; Bauer, M.; Riedemann, N.C.; Hartog, C.S. New Approaches to Sepsis: Molecular Diagnostics and Biomarkers. Clin. Microbiol. Rev. 2012, 25, 609–634. [Google Scholar] [CrossRef] [Green Version]
- Schenz, J.; Weigand, M.A.; Uhle, F. Molecular and biomarker-based diagnostics in early sepsis: Current challenges and future perspectives. Expert Rev. Mol. Diagn. 2019, 19, 1069–1078. [Google Scholar] [CrossRef] [PubMed]
- Barichello, T.; Generoso, J.S.; Singer, M.; Dal-Pizzol, F. Biomarkers for sepsis: More than just fever and leukocytosis—A narrative review. Crit. Care 2022, 26, 14. [Google Scholar] [CrossRef] [PubMed]
- Agnello, L.; Ciaccio, M. Biomarkers of Sepsis. Diagnostics 2023, 13, 435. [Google Scholar] [CrossRef]
- Li, X.; Ma, X. The role of heparin in sepsis: Much more than just an anticoagulant. Br. J. Haematol. 2017, 179, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Fu, S.; Yu, S.; Wang, L.; Ma, X.; Li, X. Unfractionated heparin improves the clinical efficacy in adult sepsis patients: A systematic review and meta-analysis. BMC Anesthesiol. 2022, 22, 28. [Google Scholar] [CrossRef]
- Czempik, P.F.; Wiórek, A. Management Strategies in Septic Coagulopathy: A Review of the Current Literature. Healthcare 2023, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.-H.; Chiang, B.-L. The diagnosis and classification of autoimmune coagulopathy: An updated review. Autoimmun. Rev. 2014, 13, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Ichinose, A.; Osaki, T.; Souri, M. A Review of Coagulation Abnormalities of Autoimmune Acquired Factor V Deficiency with a Focus on Japan. Semin. Thromb. Hemost. 2022, 48, 206–218. [Google Scholar] [CrossRef]
- Cugno, M.; Borghi, A.; Garcovich, S.; Marzano, A.V. Coagulation and Skin Autoimmunity. Front. Immunol. 2019, 10, 1407. [Google Scholar] [CrossRef] [PubMed]
- Favaloro, E.J.; Pasalic, L.; Lippi, G. Autoimmune Diseases Affecting Hemostasis: A Narrative Review. Int. J. Mol. Sci. 2022, 23, 14715. [Google Scholar] [CrossRef] [PubMed]
- Saraya, A.K.; Rai, R.; Saxena, R.; Singh, R.R.; Padmakumar, K.; Malaviya, A.N. Coagulation abnormalities in systemic lupus erythematosus. Indian J. Med. Res. 1989, 90, 335–340. [Google Scholar]
- Byron, M.A. The Clotting Defect in SLE. Clin. Rheum. Dis. 1982, 8, 137–151. [Google Scholar] [CrossRef]
- Rick, M.E.; Hoyer, L.W. Haemostatic Disorders in Systemic Lupus Erythematosus. Clin. Rheum. Dis. 1975, 1, 583–596. [Google Scholar] [CrossRef]
- Li, Z.; Xiao, J.; Song, H.; Chen, Q.; Han, H.; Li, J.; Zhang, L.; He, Y.; Wei, M. Evaluation of coagulation disorders by thromboelastography in children with systemic lupus erythematosus. Lupus 2019, 28, 181–188. [Google Scholar] [CrossRef]
- Maia, G.A. Systemic Lupus Erythematosus-induced Coagulopathy: A Case Report [abstract]. Res. Pract. Thromb. Haemost. 2021, 5 (Suppl. 2). [Google Scholar]
- Jiménez, E.O.; Fragoso, S.L.; Gabayet, M.R. Acquired Inhibitors of Coagulation in a Patient With Systemic Lupus Erythematosus and Antiphospholipid Antibodies: Response to Rituximab. Reumatol. Clin. 2008, 4, 74–76. [Google Scholar] [CrossRef]
- Conn, D.L.; McDuffie, F.C.; Kazmier, F.J.; Schroeter, A.L.; Sun, N.C.J. Coagulation abnormalities in rheumatoid disease. Arthritis Rheum. 1976, 19, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Dimitroulas, T.; Douglas, K.M.J.; Panoulas, V.F.; Toms, T.; Smith, J.P.; Treharne, G.J.; Nightingale, P.; Hodson, J.; Kitas, G.D. Derangement of hemostasis in rheumatoid arthritis: Association with demographic, inflammatory and metabolic factors. Clin. Rheumatol. 2013, 32, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P. Hypercoagulation in Patients with Rheumatoid Arthritis Correlates with Activation of Act1/NF-κb Signaling Pathway. J. Rheum. Dis. Treat. 2015, 1. [Google Scholar] [CrossRef]
- Onuora, S. Blood coagulation factor drives arthritis pathogenesis. Nat. Rev. Rheumatol. 2014, 10, 700. [Google Scholar] [CrossRef]
- Mackworth-Young, C.G. Antiphospholipid syndrome: Multiple mechanisms. Clin. Exp. Immunol. 2004, 136, 393–401. [Google Scholar] [CrossRef]
- Anglés-Cano, E.; Guillin, M.-C. Antiphospholipid antibodies and the coagulation cascade. Rheum. Dis. Clin. N. Am. 2001, 27, 573–586. [Google Scholar] [CrossRef] [PubMed]
- Arreola-Diaz, R.; Majluf-Cruz, A.; Sanchez-Torres, L.; Hernandez-Juarez, J. The Pathophysiology of The Antiphospholipid Syndrome: A Perspective From The Blood Coagulation System. Clin. Appl. Thromb. 2022, 28. [Google Scholar] [CrossRef]
- Lee, P.; Norman, C.S.; Sukenik, S.; Alderdice, C.A. The clinical significance of coagulation abnormalities in systemic sclerosis (scleroderma). J. Rheumatol. 1985, 12, 514–517. [Google Scholar]
- Ames, P.R.; Lupoli, S.; Alves, J.; Atsumi, T.; Edwards, C.; Iannaccone, L.; Khamashta, M.A.; Hughes, G.R.; Brancaccio, V. The coagulation/fibrinolysis balance in systemic sclerosis: Evidence for a haematological stress syndrome. Rheumatology 1997, 36, 1045–1050. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Volpe, A.; Caramaschi, P.; Salvagno, G.L.; Montagnana, M.; Guidi, G.C. Plasma D-dimer concentration in patients with systemic sclerosis. Thromb. J. 2006, 4, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pattanaik, D.; Brown, M.; Postlethwaite, B.C.; Postlethwaite, A.E. Pathogenesis of Systemic Sclerosis. Front. Immunol. 2015, 6, 272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez, G.A.; Franchini, S.; Rovere-Querini, P.; Sabbadini, M.G.; Manfredi, A.A.; Maugeri, N. The role of platelets in the pathogenesis of systemic sclerosis. Front. Immunol. 2012, 3, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danese, S.; Papa, A.; Saibeni, S.; Repici, A.; Malesci, A.; Vecchi, M. Inflammation and Coagulation in Inflammatory Bowel Disease: The Clot Thickens. Am. J. Gastroenterol. 2007, 102, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Dolapcioglu, C.; Soylu, A.; Kendir, T.; Ince, A.T.; Dolapcioglu, H.; Purisa, S.; Bolukbas, C.; Sokmen, H.M.; Dalay, R.; Ovunc, O. Coagulation parameters in inflammatory bowel disease. Int. J. Clin. Exp. Med. 2014, 7, 1442–1448. [Google Scholar] [PubMed]
- Giannotta, M.; Tapete, G.; Emmi, G.; Silvestri, E.; Milla, M. Thrombosis in inflammatory bowel diseases: What’s the link? Thromb. J. 2015, 13, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chosamata, B. Teaching Corner: The management of immune thrombocytopenic purpura. Malawi Med. J. 2015, 27, 109–112. [Google Scholar] [CrossRef] [Green Version]
- Platelet Disorders—Immune Thrombocytopenia (ITP)|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health/immune-thrombocytopenia (accessed on 15 June 2023).
- Álvarez-Román, M.T.; Fernández-Bello, I.; Jiménez-Yuste, V.; Martín-Salces, M.; Arias-Salgado, E.G.; Pollmar, M.I.R.; Sanz, R.J.; Butta, N.V. Procoagulant profile in patients with immune thrombocytopenia. Br. J. Haematol. 2016, 175, 925–934. [Google Scholar] [CrossRef]
- Valade, S.; Mariotte, E.; Azoulay, E. Coagulation Disorders in Hemophagocytic Lymphohistiocytosis/Macrophage Activation Syndrome. Crit. Care Clin. 2020, 36, 415–426. [Google Scholar] [CrossRef]
- Valade, S.; Joly, B.S.; Veyradier, A.; Fadlallah, J.; Zafrani, L.; Lemiale, V.; Launois, A.; Stepanian, A.; Galicier, L.; Fieschi, C.; et al. Coagulation disorders in patients with severe hemophagocytic lymphohistiocytosis. PLoS ONE 2021, 16, e0251216. [Google Scholar] [CrossRef]
- Ling, L.; Huang, X.; Liu, C.; Liao, J.; Zhou, J. Monitoring coagulation-fibrinolysis activation prompted timely diagnosis of hemophagocytic lymphohistiocytosis-related disseminated intravascular coagulation. Thromb. J. 2021, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.T.; Gorzelanny, C.; Gebhardt, C.; Pantel, K.; Schneider, S.W. Interplay between coagulation and inflammation in cancer: Limitations and therapeutic opportunities. Cancer Treat. Rev. 2022, 102, 102322. [Google Scholar] [CrossRef] [PubMed]
- Lima, L.G.; Monteiro, R.Q. Activation of blood coagulation in cancer: Implications for tumour progression. Biosci. Rep. 2013, 33, e00064. [Google Scholar] [CrossRef] [PubMed]
- Loreto, M.F.; De Martinis, M.; Corsi, M.P.; Modesti, M.; Ginaldi, L. Coagulation and cancer: Implications for diagnosis and management. Pathol. Oncol. Res. 2000, 6, 301–312. [Google Scholar] [CrossRef] [Green Version]
- Kitchens, C.S. Thrombocytopenia and thrombosis in disseminated intravascular coagulation (DIC). Hematol. Am. Soc. Hematol. Educ. Program 2009, 2009, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Razak, N.B.A.; Jones, G.; Bhandari, M.; Berndt, M.C.; Metharom, P. Cancer-Associated Thrombosis: An Overview of Mechanisms, Risk Factors, and Treatment. Cancers 2018, 10, 380. [Google Scholar] [CrossRef] [Green Version]
- Gouin-Thibault, I.; Achkar, A.; Samama, M. The Thrombophilic State in Cancer Patients. Acta Haematol. 2001, 106, 33–42. [Google Scholar] [CrossRef]
- Kvolik, S.; Jukic, M.; Matijevic, M.; Marjanovic, K.; Glavas-Obrovac, L. An overview of coagulation disorders in cancer patients. Surg. Oncol. 2010, 19, e33–e46. [Google Scholar] [CrossRef]
- Mantha, S. Bleeding Disorders Associated with Cancer. Cancer Treat Res. 2019, 179, 191–203. [Google Scholar] [CrossRef]
- Falanga, A.; Marchetti, M.; Vignoli, A. Coagulation and cancer: Biological and clinical aspects. J. Thromb. Haemost. 2013, 11, 223–233. [Google Scholar] [CrossRef]
- Palacios-Acedo, A.L.; Mège, D.; Crescence, L.; Dignat-George, F.; Dubois, C.; Panicot-Dubois, L. Platelets, Thrombo-Inflammation, and Cancer: Collaborating With the Enemy. Front. Immunol. 2019, 10, 1805. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.K.; Malviya, R. Coagulation and inflammation in cancer: Limitations and prospects for treatment. Biochim. Biophys. Acta BBA—Rev. Cancer 2022, 1877, 188727. [Google Scholar] [CrossRef] [PubMed]
- Setiawan, B.; Budianto, W.; Sukarnowati, T.W.; Rizky, D.; Pangarsa, E.A.; Santosa, D.; Setiabudy, R.D.; Suharti, C. Correlation of Inflammation and Coagulation Markers with the Incidence of Deep Vein Thrombosis in Cancer Patients with High Risk of Thrombosis. Int. J. Gen. Med. 2022, 15, 6215–6226. [Google Scholar] [CrossRef]
- Panova-Noeva, M.; Schulz, A.; Arnold, N.; Hermanns, M.I.; Prochaska, J.H.; Laubert-Reh, D.; Spronk, H.M.; Blettner, M.; Beutel, M.; Pfeiffer, N.; et al. Coagulation and inflammation in long-term cancer survivors: Results from the adult population. J. Thromb. Haemost. 2018, 16, 699–708. [Google Scholar] [CrossRef] [Green Version]
- Galmiche, A.; Rak, J.; Roumenina, L.T.; Saidak, Z. Coagulome and the tumor microenvironment: An actionable interplay. Trends Cancer 2022, 8, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Shoji, M.; Hancock, W.W.; Abe, K.; Micko, C.; Casper, K.A.; Baine, R.M.; Wilcox, J.N.; Danave, I.; Dillehay, D.L.; Matthews, E.; et al. Activation of coagulation and angiogenesis in cancer: Immunohistochemical localization in situ of clotting proteins and vascular endothelial growth factor in human cancer. Am. J. Pathol. 1998, 152, 399–411. [Google Scholar] [PubMed]
- Belting, M.; Ahamed, J.; Ruf, W. Signaling of the Tissue Factor Coagulation Pathway in Angiogenesis and Cancer. Arter. Thromb. Vasc. Biol. 2005, 25, 1545–1550. [Google Scholar] [CrossRef] [Green Version]
- Bluff, J.E.; Brown, N.J.; Reed, M.W.; Staton, C.A. Tissue factor, angiogenesis and tumour progression. Breast Cancer Res. 2008, 10, 204. [Google Scholar] [CrossRef]
- Nash, G.; Walsh, D.; Kakkar, A. The role of the coagulation system in tumour angiogenesis. Lancet Oncol. 2001, 2, 608–613. [Google Scholar] [CrossRef]
- Ward, M.P.; Kane, L.E.; Norris, L.A.; Mohamed, B.M.; Kelly, T.; Bates, M.; Clarke, A.; Brady, N.; Martin, C.M.; Brooks, R.D.; et al. Platelets, immune cells and the coagulation cascade; friend or foe of the circulating tumour cell? Mol. Cancer 2021, 20, 59. [Google Scholar] [CrossRef]
- Schmied, L.; Höglund, P.; Meinke, S. Platelet-Mediated Protection of Cancer Cells From Immune Surveillance—Possible Implications for Cancer Immunotherapy. Front. Immunol. 2021, 12, 640578. [Google Scholar] [CrossRef]
- Kasthuri, R.S.; Taubman, M.B.; Mackman, N. Role of Tissue Factor in Cancer. J. Clin. Oncol. 2009, 27, 4834–4838. [Google Scholar] [CrossRef] [Green Version]
- Hisada, Y.; Mackman, N. Tissue Factor and Cancer: Regulation, Tumor Growth, and Metastasis. Semin. Thromb. Hemost. 2019, 45, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Cao, D.; Zheng, X.; Wang, G.; Liu, M. Tissue factor as a new target for tumor therapy—Killing two birds with one stone: A narrative review. Ann. Transl. Med. 2022, 10, 1250. [Google Scholar] [CrossRef]
- Ruf, W.; Graf, C. Coagulation signaling and cancer immunotherapy. Thromb. Res. 2020, 191 (Suppl. S1), S106–S111. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Lee, S.Y. Clinical Characteristics and Treatment of Immune-Related Adverse Events of Immune Checkpoint Inhibitors. Immune Netw. 2020, 20, e9. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, L.C.; Shah, A.A.; Bingham, C.O. Immune-Related Adverse Effects of Cancer Immunotherapy—Implications for Rheumatology. Rheum. Dis. Clin. N. Am. 2017, 43, 65–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, C.B.B.; Zawislak, M.C.; Wong, P.-C.V. Management of Hematologic Adverse Events Associated With Immune Checkpoint Inhibitors. J. Adv. Pract. Oncol. 2021, 12, 392–404. [Google Scholar] [CrossRef]
- Hu, W.; Wang, G.; Huang, D.; Sui, M.; Xu, Y. Cancer Immunotherapy Based on Natural Killer Cells: Current Progress and New Opportunities. Front. Immunol. 2019, 10, 1205. [Google Scholar] [CrossRef]
- Yu, Y. The Function of NK Cells in Tumor Metastasis and NK Cell-Based Immunotherapy. Cancers 2023, 15, 2323. [Google Scholar] [CrossRef]
- Toffoli, E.C.; Sheikhi, A.; Höppner, Y.D.; de Kok, P.; Yazdanpanah-Samani, M.; Spanholtz, J.; Verheul, H.M.W.; van der Vliet, H.J.; de Gruijl, T.D. Natural Killer Cells and Anti-Cancer Therapies: Reciprocal Effects on Immune Function and Therapeutic Response. Cancers 2021, 13, 711. [Google Scholar] [CrossRef] [PubMed]
- Gockel, L.M.; Nekipelov, K.; Ferro, V.; Bendas, G.; Schlesinger, M. Tumour cell-activated platelets modulate the immunological activity of CD4+, CD8+, and NK cells, which is efficiently antagonized by heparin. Cancer Immunol. Immunother. 2022, 71, 2523–2533. [Google Scholar] [CrossRef] [PubMed]
- Terwoord, J.D.; Beyer, A.M.; Gutterman, D.D. Endothelial dysfunction as a complication of anti-cancer therapy. Pharmacol. Ther. 2022, 237, 108116. [Google Scholar] [CrossRef]
- Toya, T.; Sara, J.D.; Corban, M.T.; Taher, R.; Godo, S.; Herrmann, J.; Lerman, L.O.; Lerman, A. Assessment of peripheral endothelial function predicts future risk of solid-tumor cancer. Eur. J. Prev. Cardiol. 2020, 27, 608–618. [Google Scholar] [CrossRef]
- Van Hinsbergh, V.W.M. Endothelium—Role in regulation of coagulation and inflammation. Semin. Immunopathol. 2012, 34, 93–106. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Receptor Name | Gene | Protein ID | Molecular Weight [kDa] | Amino Acid Length | Ligands | Ref. |
|---|---|---|---|---|---|---|
| Platelet glycoprotein IX | GP9 | P14770 | 19.046 | 177 |
| [50] |
| Platelet glycoprotein Ib alpha chain | GP1BA | P07359 | 71.540 | 652 | [51] | |
| Platelet glycoprotein V | GP5 | P40197 | 60.959 | 560 | [52] | |
| Platelet glycoprotein VI | GP6 | Q9HCN6 | 36.866 | 339 |
| [53] |
| Integrin alpha-2/beta-1 | ITGA2 | P17301 | 129.296 | 1181 |
| [54] |
| Integrin alpha-6/beta-1 | ITGA6 | P23229 | 126.606 | 1130 |
| [55] |
| Integrin alpha-V/ | ITGAV | P06756 | 116.038 | 1048 |
| [56] |
| Integrin alpha-IIb/beta-3 | ITGA2B | P08514 | 113.377 | 1039 |
| [57] |
| Proteinase-activated receptor 1 (PAR1) | F2R | P25116 | 47.441 | 425 |
| [58] |
| Proteinase-activated receptor 4 (PAR4) | F2RL3 | Q96RI0 | 41.133 | 385 | [59] | |
| P2Y purinoceptor 1 | P2RY1 | P47900 | 42.072 | 373 |
| [60] |
| P2Y purinoceptor 12 | P2RY12 | Q9H244 | 39.439 | 342 |
| [61] |
| 5-hydroxytryptamine receptor 2A | HTR2A | P28223 | 52.603 | 471 |
| [62] |
| Disease | Description of the Disorder | Ref. |
|---|---|---|
| Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) |
| [74,89,90,91,99] |
| Arterial Thrombosis |
| [92,93] |
| Disseminated Intravascular Coagulation (DIC) |
| [94] |
| Antiphospholipid Syndrome (APS) |
| [95,96] |
| Thrombotic Microangiopathies |
| [97,98] |
| Disease | Description of the Disorder | Ref. |
|---|---|---|
| Systemic lupus erythematosus (SLE) |
| [197,198,199,200,201,202] |
| Rheumatoid arthritis (RA) |
| [203,204,205,206] |
| Antiphospholipid syndrome (APS) |
| [207,208,209] |
| Systemic sclerosis (SSc) |
| [210,211,212,213,214] |
| Inflammatory bowel disease (IBD) |
| [215,216,217] |
| Immune thrombocytopenic purpura (ITP) |
| [218,219,220] |
| Limfohistiocytoza hemofagocytarna (HLH) |
| [221,222,223] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilhelm, G.; Mertowska, P.; Mertowski, S.; Przysucha, A.; Strużyna, J.; Grywalska, E.; Torres, K. The Crossroads of the Coagulation System and the Immune System: Interactions and Connections. Int. J. Mol. Sci. 2023, 24, 12563. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241612563
Wilhelm G, Mertowska P, Mertowski S, Przysucha A, Strużyna J, Grywalska E, Torres K. The Crossroads of the Coagulation System and the Immune System: Interactions and Connections. International Journal of Molecular Sciences. 2023; 24(16):12563. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241612563
Chicago/Turabian StyleWilhelm, Grzegorz, Paulina Mertowska, Sebastian Mertowski, Anna Przysucha, Jerzy Strużyna, Ewelina Grywalska, and Kamil Torres. 2023. "The Crossroads of the Coagulation System and the Immune System: Interactions and Connections" International Journal of Molecular Sciences 24, no. 16: 12563. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241612563