
Bioaccumulation of Non-Essential Trace Elements Detected in Women’s Follicular Fluid, Urine, and Plasma Is Associated with Poor Reproductive Outcomes following Single Euploid Embryo Transfer: A Pilot Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Demographics and Reproductive Characteristics
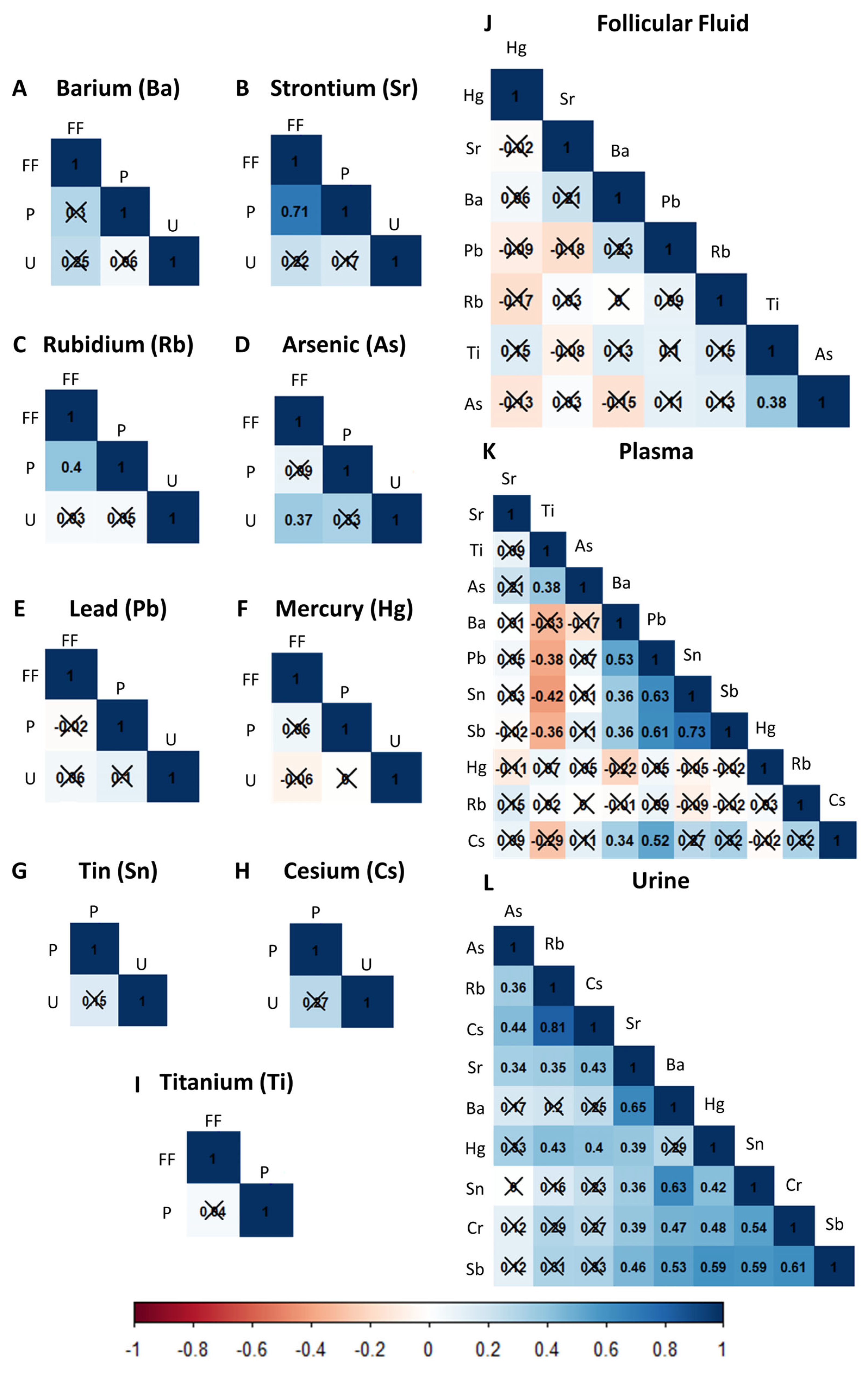
2.2. Correlations of Non-Essential Trace Elements between and within Biological Matrices
2.3. Non-Essential Trace Elements Are Inversely Correlated with Ovarian Response and Preimplantation IVF Outcomes
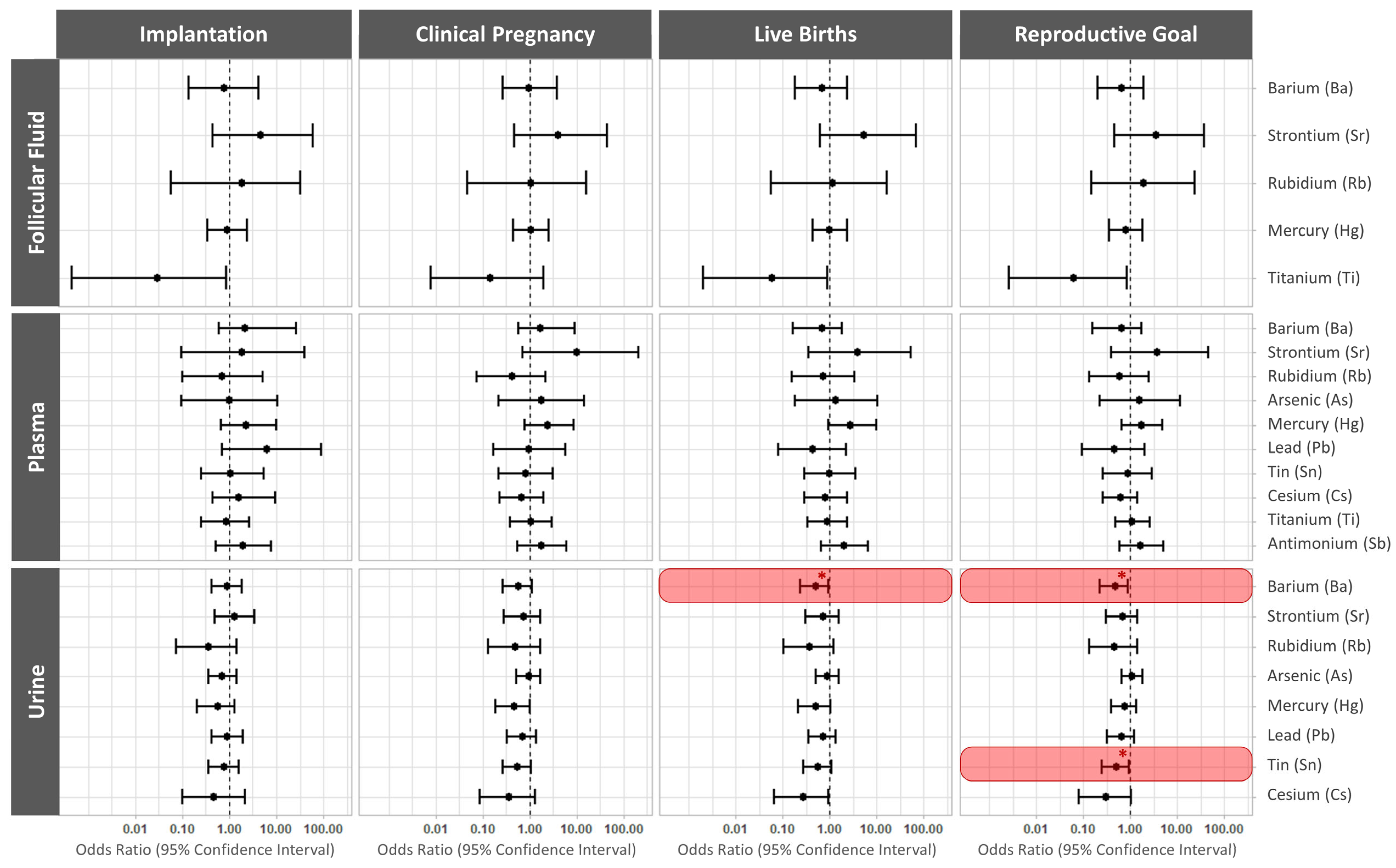
2.4. Elevated Urinary Barium and Tin Reduce the Odds of a Live Birth following Single Frozen Embryo Transfer
3. Discussion
4. Materials and Methods
4.1. Ethical Approval
4.2. Study Population
4.3. Collection of Urine, Blood, and Follicular Fluid Samples
4.4. Quantification of Non-Essential Trace Elements
4.5. Clinical Management and Reproductive Outcome Assessment
4.6. Statistical Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Engwa, G.A.; Ferdinand, P.U.; Nwalo, F.N.; Unachukwu, M.N. Mechanism and health effects of heavy metal toxicity in humans. In Poisoning in the Modern World—New Tricks for an Old Dog? Karcioglu, O., Arslan, B., Eds.; BoD–Books on Demand: Paris, France, 2019; ISBN 978-1-83880-786-3. [Google Scholar]
- Rehman, K.; Fatima, F.; Waheed, I.; Akash, M.S.H. Prevalence of Exposure of Heavy Metals and Their Impact on Health Consequences. J. Cell Biochem. 2018, 119, 157–184. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, V.Y.; Bloom, M.S. Role of environmental factors and Gonadotoxin exposure in unexplained female infertility. In Unexplained Infertility; Schattman, G., Esteves, S., Agarwal, A., Eds.; Springer LLC: New York, NY, USA, 2015; pp. 161–173. ISBN 9781493921409. [Google Scholar]
- Butts, C.D.; Bloom, M.S.; McGough, A.; Lenhart, N.; Wong, R.; Mok-Lin, E.; Parsons, P.J.; Galusha, A.L.; Yucel, R.M.; Feingold, B.J.; et al. Seafood consumption is associated with higher follicular fluid arsenic (As) and mercury (Hg) concentrations in women undergoing in vitro fertilization (IVF). Environ. Res. 2020, 188, 109753. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Bloom, M.S.; Parsons, P.J.; Fitzgerald, E.F.; Bell, E.M.; Steuerwald, A.J.; Fujimoto, V.Y. A Pilot Study of Seafood Consumption and Exposure to Mercury, Lead, Cadmium and Arsenic among Infertile Couples Undergoing in Vitro Fertilization (IVF). Environ. Toxicol. Pharmacol. 2013, 36, 30–34. [Google Scholar] [CrossRef]
- Chatterjee, A.; Chatterji, U. Arsenic abrogates the estrogen-signaling pathway in the rat uterus. Reprod. Biol. Endocrinol. 2010, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, S.; Ghosh, D. The Involvement of Hypophyseal-Gonadal and Hypophyseal-Adrenal Axes in Arsenic-Mediated Ovarian and Uterine Toxicity: Modulation by HCG. J. Biochem. Mol. Toxicol. 2010, 24, 29–41. [Google Scholar] [CrossRef]
- Pillai, A.; Laxmi Priya, P.N.; Gupta, S. Effects of Combined Exposure to Lead and Cadmium on Pituitary Membrane of Female Rats. Arch. Toxicol. 2002, 76, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Butts, C.D.; Bloom, M.S.; McGough, A.; Lenhart, N.; Wong, R.; Mok-Lin, E.; Parsons, P.J.; Galusha, A.L.; Yucel, R.M.; Feingold, B.J.; et al. Variability of essential and non-essential trace elements in the follicular fluid of women undergoing in vitro fertilization (IVF). Ecotoxicol. Environ. Saf. 2021, 209, 111733. [Google Scholar] [CrossRef]
- Rodríguez-Díaz, R.; Blanes-Zamora, R.; Paz-Montelongo, S.; Gómez-Rodríguez, J.; Fiestas, S.R.; González-Weller, D.; Gutiérrez, J.; Rubio, C.; Hardisson, A.; Niebla-Canelo, D.; et al. The Influence of Follicular Fluid Metals on Assisted Reproduction Outcome. Biol. Trace Elem. Res. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Schmalbrock, L.J.; Weiss, G.; Rijntjes, E.; Reinschissler, N.; Sun, Q.; Schenk, M.; Schomburg, L. Pronounced Trace Element Variation in Follicular Fluids of Subfertile Women Undergoing Assisted Reproduction. Nutrients 2021, 13, 4134. [Google Scholar] [CrossRef]
- Bloom, M.S.; Fujimoto, V.Y.; Steuerwald, A.J.; Cheng, G.; Browne, R.W.; Parsons, P.J. Background Exposure to Toxic Metals in Women Adversely Influences Pregnancy during in Vitro Fertilization (IVF). Reprod. Toxicol. 2012, 34, 471–481. [Google Scholar] [CrossRef]
- Bloom, M.S.; Parsons, P.J.; Kim, D.; Steuerwald, A.J.; Vaccari, S.; Cheng, G.; Fujimoto, V.Y. Toxic Trace Metals and Embryo Quality Indicators during in Vitro Fertilization (IVF). Reprod. Toxicol. 2011, 31, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Bloom, M.S.; Kim, K.; Kruger, P.C.; Parsons, P.J.; Arnason, J.G.; Steuerwald, A.J.; Fujimoto, V.Y. Associations between Toxic Metals in Follicular Fluid and in Vitro Fertilization (IVF) Outcomes. J. Assist. Reprod. Genet. 2012, 29, 1369–1379. [Google Scholar] [CrossRef] [PubMed]
- Jomova, K.; Valko, M. Advances in Metal-Induced Oxidative Stress and Human Disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef]
- Jaishankar, M.; Tseten, T.; Anbalagan, N.; Mathew, B.B.; Beeregowda, K.N. Toxicity, Mechanism and Health Effects of Some Heavy Metals. Interdiscip. Toxicol. 2014, 7, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Choy, C.M.Y.; Lam, C.W.K.; Cheung, L.T.F.; Briton-Jones, C.M.; Cheung, L.P.; Haines, C.J. Infertility, Blood Mercury Concentrations and Dietary Seafood Consumption: A Case-Control Study. BJOG 2002, 109, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Maeda, E.; Murata, K.; Kumazawa, Y.; Sato, W.; Shirasawa, H.; Iwasawa, T.; Izumo, K.; Tatsuta, N.; Sakamoto, M.; Terada, Y. Associations of Environmental Exposures to Methylmercury and Selenium with Female Infertility: A Case–Control Study. Environ. Res. 2019, 168, 357–363. [Google Scholar] [CrossRef]
- Dickerson, E.H.; Sathyapalan, T.; Knight, R.; Maguiness, S.M.; Killick, S.R.; Robinson, J.; Atkin, S.L. Endocrine Disruptor & Nutritional Effects of Heavy Metals in Ovarian Hyperstimulation. J. Assist. Reprod. Genet. 2011, 28, 1223–1228. [Google Scholar] [CrossRef]
- García-Fortea, P.; Cohen-Corcia, I.; Córdoba-Doña, J.A.; Reche-Rosado, A.; González-Mesa, E. Toxic Elements in Hair and in Vitro Fertilization Outcomes: A Prospective Cohort Study. Reprod. Toxicol. 2018, 77, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Hu, Y.; He, S.; Jiang, R.; Yao, Y.; Jin, Z.; Shen, J.; Tao, F.; Ji, Y.; Liang, C. Exposure to multiple toxic metals and the risk of early embryonic arrest among women undergoing assisted reproductive techniques. Environ. Res. 2022, 211, 113072. [Google Scholar] [CrossRef]
- Tolunay, H.E.; Şükür, Y.E.; Ozkavukcu, S.; Seval, M.M.; Ateş, C.; Türksoy, V.A.; Ecemiş, T.; Atabekoʇlu, C.S.; Özmen, B.; Berker, B.; et al. Heavy Metal and Trace Element Concentrations in Blood and Follicular Fluid Affect ART Outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 198, 73–77. [Google Scholar] [CrossRef]
- Wu, S.; Wang, M.; Deng, Y.; Qiu, J.; Zhang, X.; Tan, J. Associations of toxic and essential trace elements in serum, follicular fluid, and seminal plasma with In vitro fertilization outcomes. Ecotoxicol. Environ. Saf. 2020, 204, 110965. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Liang, K.; Li, M.; Rong, C.; Zheng, J.; Li, J. Metal elements associate with in vitro fertilization (IVF) outcomes in 195 couples. J. Trace Elements Med. Biol. 2021, 68, 126810. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Liang, C.; Cao, Y.; Zhu, D.; Shen, L.; Zhang, Z.; Jiang, T.; Zhang, Z.; Zong, K.; Liu, Y.; et al. The associations of serum metals concentrations with the intermediate and pregnancy outcomes in women undergoing in vitro fertilization (IVF). Ecotoxicol. Environ. Saf. 2022, 233, 113309. [Google Scholar] [CrossRef]
- Butts, C.D.; Bloom, M.S.; McGough, A.; Lenhart, N.; Wong, R.; Mok-Lin, E.; Parsons, P.J.; Galusha, A.L.; Browne, R.W.; Yucel, R.M.; et al. Toxic elements in follicular fluid adversely influence the likelihood of pregnancy and live birth in women undergoing IVF. Hum. Reprod. Open 2021, 2021, hoab023. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, I.; Coskun, S.; Mashhour, A.; Shinwari, N.; El-Doush, I.; Billedo, G.; Jaroudi, K.; Al-Shahrani, A.; Al-Kabra, M.; El Din Mohamed, G. Exposure to Heavy Metals (Lead, Cadmium and Mercury) and Its Effect on the Outcome of in-Vitro Fertilization Treatment. Int. J. Hyg. Environ. Health 2008, 211, 560–579. [Google Scholar] [CrossRef] [PubMed]
- Henriques, M.C.; Loureiro, S.; Fardilha, M.; Herdeiro, M.T. Exposure to Mercury and Human Reproductive Health: A Systematic Review. Reprod. Toxicol. 2019, 85, 93–103. [Google Scholar] [CrossRef]
- Peana, M.; Medici, S.; Dadar, M.; Zoroddu, M.A.; Pelucelli, A.; Chasapis, C.T.; Bjørklund, G. Environmental Barium: Potential Exposure and Health-Hazards. Arch. Toxicol. 2021, 95, 2605–2612. [Google Scholar] [CrossRef]
- Kravchenko, J.; Darrah, T.H.; Miller, R.K.; Lyerly, H.K.; Vengosh, A. A Review of the Health Impacts of Barium from Natural and Anthropogenic Exposure. Environ. Geochem. Health 2014, 36, 797–814. [Google Scholar] [CrossRef]
- Wang, C.; Pi, X.; Chen, Y.; Wang, D.; Yin, S.; Jin, L.; Li, Z.; Ren, A.; Wang, L.; Yin, C. Prenatal Exposure to Barium and the Occurrence of Neural Tube Defects in Offspring. Sci. Total Environ. 2021, 764, 144245. [Google Scholar] [CrossRef]
- Cohen-Solal, M. Strontium Overload and Toxicity: Impact on Renal Osteodystrophy. Nephrol. Dial. Transplant. 2002, 17, 30–34. [Google Scholar] [CrossRef]
- Kaufman, M.H. Parthenogenetic Activation of Oocytes. Cold Spring Harb. Protoc. 2018, 2018, 20–23. [Google Scholar] [CrossRef]
- Anifandis, G.; Michopoulos, A.; Daponte, A.; Chatzimeletiou, K.; Simopoulou, M.; Messini, C.I.; Polyzos, N.P.; Vassiou, K.; Dafopoulos, K.; Goulis, D.G. Artificial oocyte activation: Physiological, pathophysiological and ethical aspects. Syst. Biol. Reprod. Med. 2018, 65, 3–11. [Google Scholar] [CrossRef]
- Priya, K.; Setty, M.; Babu, U.V.; Pai, K.S.R. Implications of environmental toxicants on ovarian follicles: How it can adversely affect the female fertility? Environ. Sci. Pollut. Res. 2021, 28, 67925–67939. [Google Scholar] [CrossRef] [PubMed]
- Tulić, L.; Vidaković, S.; Tulić, I.; Ćurčić, M.; Bulat, Z. Toxic Metal and Trace Element Concentrations in Blood and Outcome of In Vitro Fertilization in Women. Biol. Trace Elem. Res. 2019, 188, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Domingo-Relloso, A.; Bozack, A.; Kiihl, S.; Rodriguez-Hernandez, Z.; Rentero-Garrido, P.; Casasnovas, J.A.; Leon-Latre, M.; Garcia-Barrera, T.; Gomez-Ariza, J.L.; Moreno, B.; et al. Arsenic Exposure and Human Blood DNA Methylation and Hydroxymethylation Profiles in Two Diverse Populations from Bangladesh and Spain. Environ. Res 2022, 204, 112021. [Google Scholar] [CrossRef] [PubMed]
- Graceli, J.B.; Sena, G.C.; Lopes, P.F.I.; Zamprogno, G.C.; da Costa, M.B.; Godoi, A.F.L.; dos Santos, D.M.; de Marchi, M.R.R.; dos Santos Fernandez, M.A. Organotins: A Review of Their Reproductive Toxicity, Biochemistry, and Environmental Fate. Reprod. Toxicol. 2013, 36, 40–52. [Google Scholar] [CrossRef]
- Ema, M.; Harazono, A. Adverse Effects of Dibutyltin Dichloride on Initiation and Maintenance of Rat Pregnancy. Reprod. Toxicol. 2000, 14, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Ema, M.; Miyawaki, E.; Kawashima, K. Adverse Effects of Diphenyltin Dichloride on Initiation and Maintenance of Pregnancy in Rats. Toxicol. Lett. 1999, 108, 17–25. [Google Scholar] [CrossRef]
- Harazono, A.; Ema, M.; Ogawa, Y. Evaluation of Early Embryonic Loss Induced by Tributyltin Chloride in Rats: Phase- and Dose-Dependent Antifertility Effects. Arch. Environ. Contam. Toxicol. 1998, 34, 94–99. [Google Scholar] [CrossRef]
- Makoto, E.; Miyawaki, E.; Harazono, A.; Ogawa, Y. Effects of Triphenyltin Chloride on Implantation and Pregnancy in Rats. Reprod. Toxicol. 1997, 11, 201–206. [Google Scholar] [CrossRef]
- Ema, M.; Miyawaki, E. Suppression of Uterine Decidualization Correlated with Reduction in Serum Progesterone Levels as a Cause of Preimplantation Embryonic Loss Induced by Diphenyltin in Rats. Reprod. Toxicol. 2002, 16, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Ema, M.; Harazono, A.; Hirose, A.; Kamata, E. Protective Effects of Progesterone on Implantation Failure Induced by Dibutyltin Dichloride in Rats. Toxicol. Lett. 2003, 143, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Campisano, R.; Hall, K.; Griggs, J.; Willison, S.; Reimer, S.; Mash, H.; Magnuson, M.; Boczek, L.; Rhodes, E. Selected Analytical Methods for Environmental Remediation and Recovery (SAM); U.S. Environmental Protection Agency: Washington, DC, USA, 2017; EPA/600/R-17/356. Available online: https://cfpub.epa.gov/si/si_public_record_Report.cfm?dirEntryId=355773&Lab=CESER (accessed on 5 September 2022).
- Hanson, B.M.; Kim, J.G.; Osman, E.K.; Tiegs, A.W.; Lathi, R.B.; Cheng, P.J.; Scott, R.T.; Franasiak, J.M. Impact of paternal age on embryology and pregnancy outcomes in the setting of a euploid single-embryo transfer with ejaculated sperm: Retrospective cohort study. F&S Rep. 2020, 1, 99–105. [Google Scholar] [CrossRef]
- Yoshida, K.; Bartel, A. Tableone: Create “Table 1” to Describe Baseline Characteristics with or without Propensity Score Weights, R Packag. Version 0.13.0; 2021. Available online: https://cran.r-project.org/package=tableone (accessed on 15 January 2022).
- Wei, T.; Simko, V. R Package “Corrplot”: Visualization of a Correlation Matrix, Version 0.92; 2021. Available online: https://github.com/taiyun/corrplot (accessed on 15 January 2022).
- Barnier, J.; Briatte, F.; Larmarange, J. Questionr: Functions to Make Surveys Processing Easier, R Packag. Version 0.7.7; 2022. Available online: https://www.rdocumentation.org/packages/questionr/versions/0.7.7 (accessed on 15 January 2022).
- Kim, K.; Steuerwald, A.J.; Parsons, P.J.; Fujimoto, V.Y.; Browne, R.W.; Bloom, M.S. Biomonitoring for Exposure to Multiple Trace Elements via Analysis of Urine from Participants in the Study of Metals and Assisted Reproductive Technologies (SMART). J. Environ. Monit. 2011, 13, 2413–2419. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Characteristics | |
|---|---|
| Age (years), median [IQR] | 33.40 [31.37, 36.50] |
| Body mass index (kg/m2), median [IQR] | 23.87 [21.57, 26.30] |
| Race/ethnic group, n (%) | |
| 43 (71.7%) |
| 2 (3.3%) |
| 6 (10.0%) |
| 6 (10.0%) |
| 3 (5.0%) |
| Post-secondary education, n (%) | 55 (94.8%) |
| Smoking habits, n (%) | |
| 49 (81.7%) |
| 10 (16.7%) |
| 1 (1.7%) |
| Reproductive Characteristics | |
| Serum anti-müllerian hormone (ng/mL), median [IQR] | 3.60 [2.49, 5.17] |
| Antagonist COS protocol, n (%) | 60 (100.0%) |
| Total FSH dose during stimulation (IU), median [IQR] | 2100.00 [1800.00, 2700.00] |
| Total LH dose during stimulation (IU), median [IQR] | 1125.00 [675.00, 1443.75] |
| Serum estradiol on trigger day (pg/mL), median [IQR] | 3750.65 [2622.20, 5204.62] |
| Number of oocytes recovered, median [IQR] | 17.00 [11.00, 24.25] |
| Number of mature (MII) oocytes, median [IQR] | 13.00 [8.75, 20.50] |
| Oocyte maturation rate, mean ± SD | 77.47 ± 14.30% |
| Number of fertilized embryos (2PN), median [IQR] | 11.00 [7.00, 15.25] |
| Fertilization rate, mean ± SD | 81.44 ± 16.29% |
| Number of blastocysts, median [IQR] | 6.00 [3.50, 10.50] |
| Blastulation rate, mean ± SD | 55.62 ± 21.47% |
| Number of euploid embryos, median [IQR] | 3.00 [2.00, 7.00] |
| Euploidy rate, mean ± SD | 60.17 ± 23.72% |
| Transfer rate, n (%) | 55 (91.7%) |
| Implantation (positive hCG) rate, n (%) | 44 (80.0%) |
| Clinical pregnancy rate, n (%) | 38 (69.1%) |
| Live births, n (%) | 35 (63.6%) |
| Reproductive goal, n (%) | 35 (58.3%) |
| Number of Available Samples for Analysis | LOD | Percentage of Samples below LOD (<LOD) | GM (SD) | |
|---|---|---|---|---|
| Follicular Fluid (ng/mL) | ||||
| Barium (Ba) | 51 | 2 | 3.9 | 2.082 (1.907) |
| Strontium (Sr) | 52 | 1 | 0 | 27.38 (7.595) |
| Rubidium (Rb) | 52 | 1 | 0 | 116.28 (22.915) |
| Arsenic (As) | 52 | 1 | 84.6 | 0.638 (1.271) |
| Tin (Sn) | 52 | 1 | 100 | |
| Cesium (Cs) | 52 | 1 | 100 | |
| Mercury (Hg) | 54 | 0.05 | 0 | 1.841 (2.567) |
| Titanium (Ti) | 52 | 1 | 0 | 2.636 (0.759) |
| Lead (Pb) | 48 | 1 | 93.8 | 0.542 (0.361) |
| Antimonium (Sb) | 52 | 1 | 100 | |
| Plasma (ng/mL) | ||||
| Barium (Ba) | 59 | 1 | 0 | 26.24 (121.34) |
| Strontium (Sr) | 59 | 1 | 0 | 37.99 (10.05) |
| Rubidium (Rb) | 59 | 1 | 0 | 361.6 (182.19) |
| Arsenic (As) | 59 | 2 | 11.9 | 4.16 (1.19) |
| Tin (Sn) | 59 | 5 | 0 | 9.55 (5.96) |
| Cesium (Cs) | 59 | 1 | 0 | 3.71 (7.53) |
| Mercury (Hg) | 17 | 0.5 | 0 | 1.8 (1.17) |
| Titanium (Ti) | 59 | 1 | 0 | 567.6 (386.27) |
| Lead (Pb) | 59 | 1 | 0 | 4.3 (1.87) |
| Antimonium (Sb) | 59 | 5 | 5.1 | 9.48 (6.09) |
| Urine | ||||
| Barium (Ba) (ng/mL) | 58 | 1 | 5.2 | 1.4 (2.69) |
| CR corrected (µg/g CR) | 0.016 (0.021) | |||
| Strontium (Sr) (ng/mL) | 58 | 1 | 0 | 84.16 (84.6) |
| CR corrected (µg/g CR) | 0.966 (0.895) | |||
| Rubidium (Rb) (ng/mL) | 57 | 1 | 0 | 1125.99 (810.16) |
| CR corrected (µg/g CR) | 13.072 (10.843) | |||
| Arsenic (As) (ng/mL) | 58 | 0.5 | 1.7 | 13.36 (61.02) |
| CR corrected (µg/g CR) | 0.153 (0.595) | |||
| Tin (Sn) (ng/mL) | 58 | 0.5 | 15.5 | 0.92 (1.13) |
| CR corrected (µg/g CR) | 0.011 (0.019) | |||
| Cesium (Cs) (ng/mL) | 58 | 0.2 | 0 | 5.54 (3.84) |
| CR corrected (µg/g CR) | 0.064 (0.045) | |||
| Mercury (Hg) (ng/mL) | 57 | 0.1 | 0 | 1.15 (0.8) |
| CR corrected (µg/g CR) | 0.013 (0.029) | |||
| Titanium (Ti) (ng/mL) | 15 | 1 | 0 | 10.23 (7.34) |
| CR corrected (µg/g CR) | 0.121 (0.115) | |||
| Lead (Pb) (ng/mL) | 58 | 0.5 | 34.5 | 0.46 (0.74) |
| CR corrected (µg/g CR) | 0.005 (0.014) | |||
| Antimonium (Sb) (ng/mL) | 58 | 1 | 100 |
| Anti-Müllerian Hormone | Trigger Day Estradiol | Number of Retrieved Oocytes | Number of Mature Oocytes | Number of Fertilized Embryos | Number of Blastocysts | Number of Euploid Embryos | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p20 vs. p80 (95%CI) | p Trend | p20 vs. p80 (95%CI) | p Trend | p20 vs. p80 (95%CI) | p Trend | p20 vs. p80 (95%CI) | p Trend | p20 vs. p80 (95%CI) | p Trend | p20 vs. p80 (95%CI) | p Trend | p20 vs. p80 (95%CI) | p Trend | |
| Follicular Fluid | ||||||||||||||
| Barium (Ba) | 0.59 (0.27, 1.30) | 0.86 | 0.83 (0.70, 0.97) | * 0.019 | 0.81 (0.66, 0.99) | * 0.042 | 0.81 (0.66, 0.99) | * 0.041 | 0.79 (0.64, 0.99) | * 0.038 | 0.78 (0.63, 0.97) | * 0.027 | 0.73 (0.60, 0.90) | ** 0.004 |
| Strontium (Sr) | 0.41 (0.15, 1.14) | 0.085 | 0.88 (0.71, 1.10) | 0.251 | 0.83 (0.65, 1.05) | 0.123 | 0.81 (0.65, 1.01) | 0.062 | 0.81 (0.65, 1.01) | 0.06 | 0.76 (0.62, 0.94) | * 0.014 | 0.77 (0.63, 0.93) | ** 0.008 |
| Plasma | ||||||||||||||
| Strontium (Sr) | 0.37 (0.15, 0.91) | * 0.032 | 0.85 (0.70, 1.04) | 0.113 | 0.82 (0.64, 1.03) | 0.088 | 0.77 (0.62, 0.96) | * 0.022 | 0.77 (0.61, 0.98) | * 0.035 | 0.77 (0.60, 0.98) | 0.036 | 0.80 (0.62, 1.03) | 0.087 |
| Rubidium (Rb) | 0.25 (0.08, 0.81) | * 0.022 | 0.88 (0.68, 1.13) | 0.310 | 0.74 (0.55, 1.01) | 0.055 | 0.78 (0.58, 1.03) | 0.083 | 0.83 (0.61, 1.12) | 0.213 | 0.89 (0.65, 1.22) | 0.453 | 0.94 (0.69, 1.28) | 0.69 |
| Arsenic (As) | 0.52 (0.21, 1.33) | 0.17 | 0.93 (0.76, 1.13) | 0.451 | 0.74 (0.59, 0.92) | ** 0.009 | 0.75 (0.61, 0.92) | ** 0.008 | 0.77 (0.62, 0.97) | * 0.028 | 0.83 (0.65, 1.05) | 0.116 | 0.80 (0.63, 1.01) | 0.065 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomar, A.; Gonzalez-Martin, R.; Quiñonero, A.; Pellicer, N.; Fernandez-Saavedra, R.; Rucandio, I.; Fernandez-Martinez, R.; Conde-Vilda, E.; Quejido, A.J.; Zuckerman, C.; et al. Bioaccumulation of Non-Essential Trace Elements Detected in Women’s Follicular Fluid, Urine, and Plasma Is Associated with Poor Reproductive Outcomes following Single Euploid Embryo Transfer: A Pilot Study. Int. J. Mol. Sci. 2023, 24, 13147. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241713147
Palomar A, Gonzalez-Martin R, Quiñonero A, Pellicer N, Fernandez-Saavedra R, Rucandio I, Fernandez-Martinez R, Conde-Vilda E, Quejido AJ, Zuckerman C, et al. Bioaccumulation of Non-Essential Trace Elements Detected in Women’s Follicular Fluid, Urine, and Plasma Is Associated with Poor Reproductive Outcomes following Single Euploid Embryo Transfer: A Pilot Study. International Journal of Molecular Sciences. 2023; 24(17):13147. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241713147
Chicago/Turabian StylePalomar, Andrea, Roberto Gonzalez-Martin, Alicia Quiñonero, Nuria Pellicer, Rocio Fernandez-Saavedra, Isabel Rucandio, Rodolfo Fernandez-Martinez, Estefania Conde-Vilda, Alberto J. Quejido, Caroline Zuckerman, and et al. 2023. "Bioaccumulation of Non-Essential Trace Elements Detected in Women’s Follicular Fluid, Urine, and Plasma Is Associated with Poor Reproductive Outcomes following Single Euploid Embryo Transfer: A Pilot Study" International Journal of Molecular Sciences 24, no. 17: 13147. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms241713147