
Reduced Levels of Lacrimal Glial Cell Line-Derived Neurotrophic Factor (GDNF) in Patients with Focal Epilepsy and Focal Epilepsy with Comorbid Depression: A Biomarker Candidate
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Patients and the Healthy Control Groups
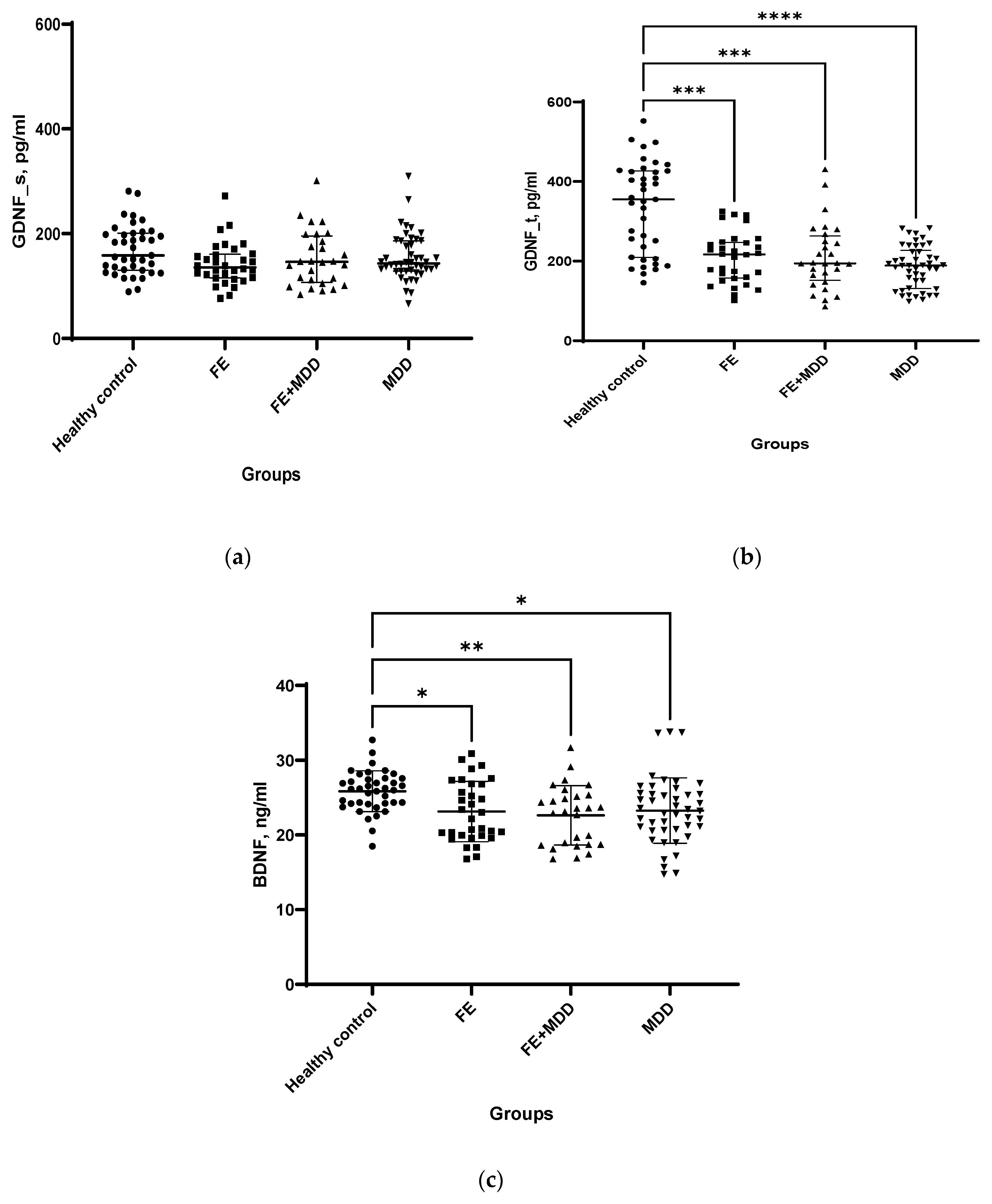
2.2. Neurotrophic Factors
2.3. Cortisol and TNF-α
2.4. Effects of Age, Gender, Medical Treatment, Etiology of Epilepsy, Type and Frequency of Seizures on Lacrimal and Serum GDNF, Serum BDNF, Cortisol, and TNF-α Levels
2.4.1. Age
2.4.2. Gender
2.4.3. Medical Treatment
2.4.4. Type or Frequency of Seizures
2.4.5. Etiology of Focal Epilepsy
2.4.6. Correlation Analysis
2.5. Combinations of Biochemical Indices—Potential Predictors for the Probability Assessment of FE, MDD, or FE with MDD
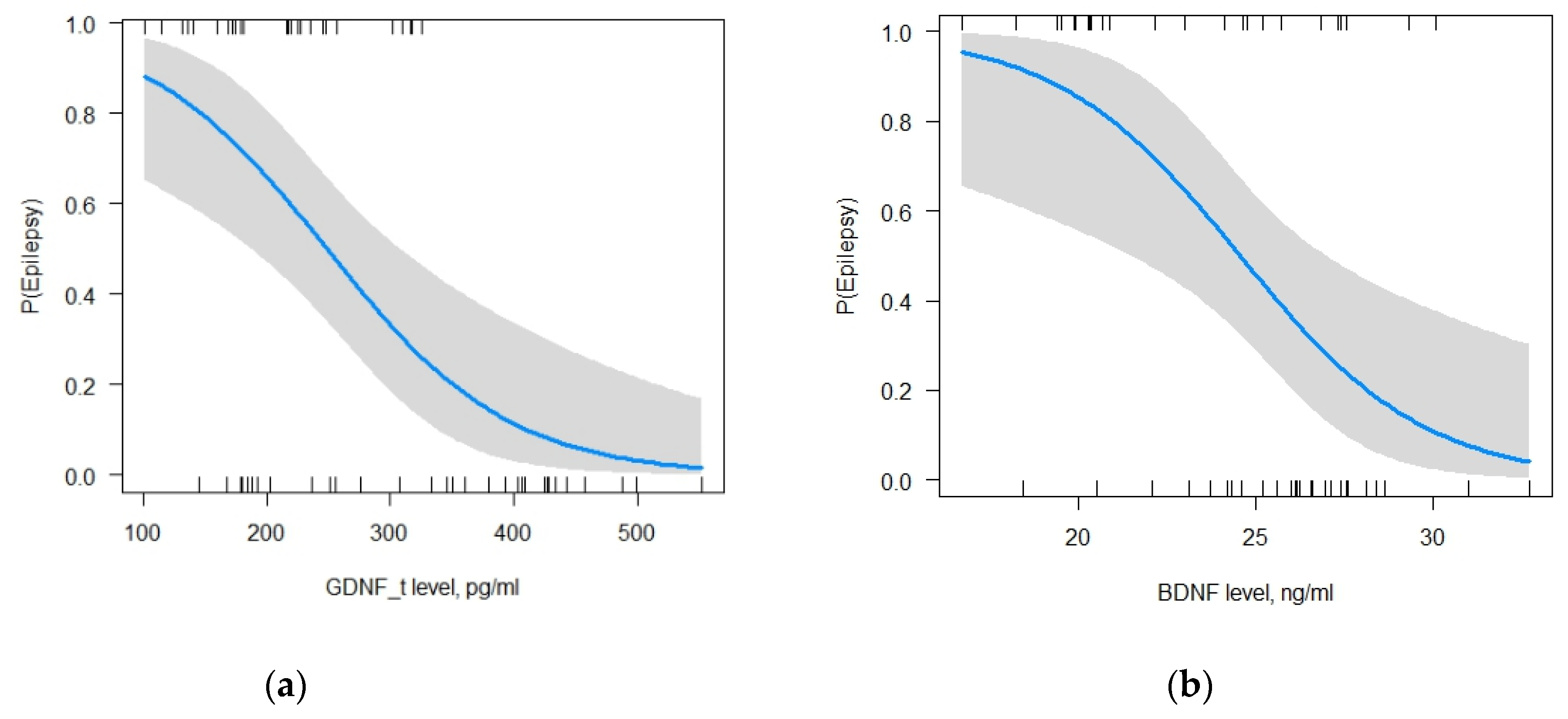
2.5.1. The Model for FE
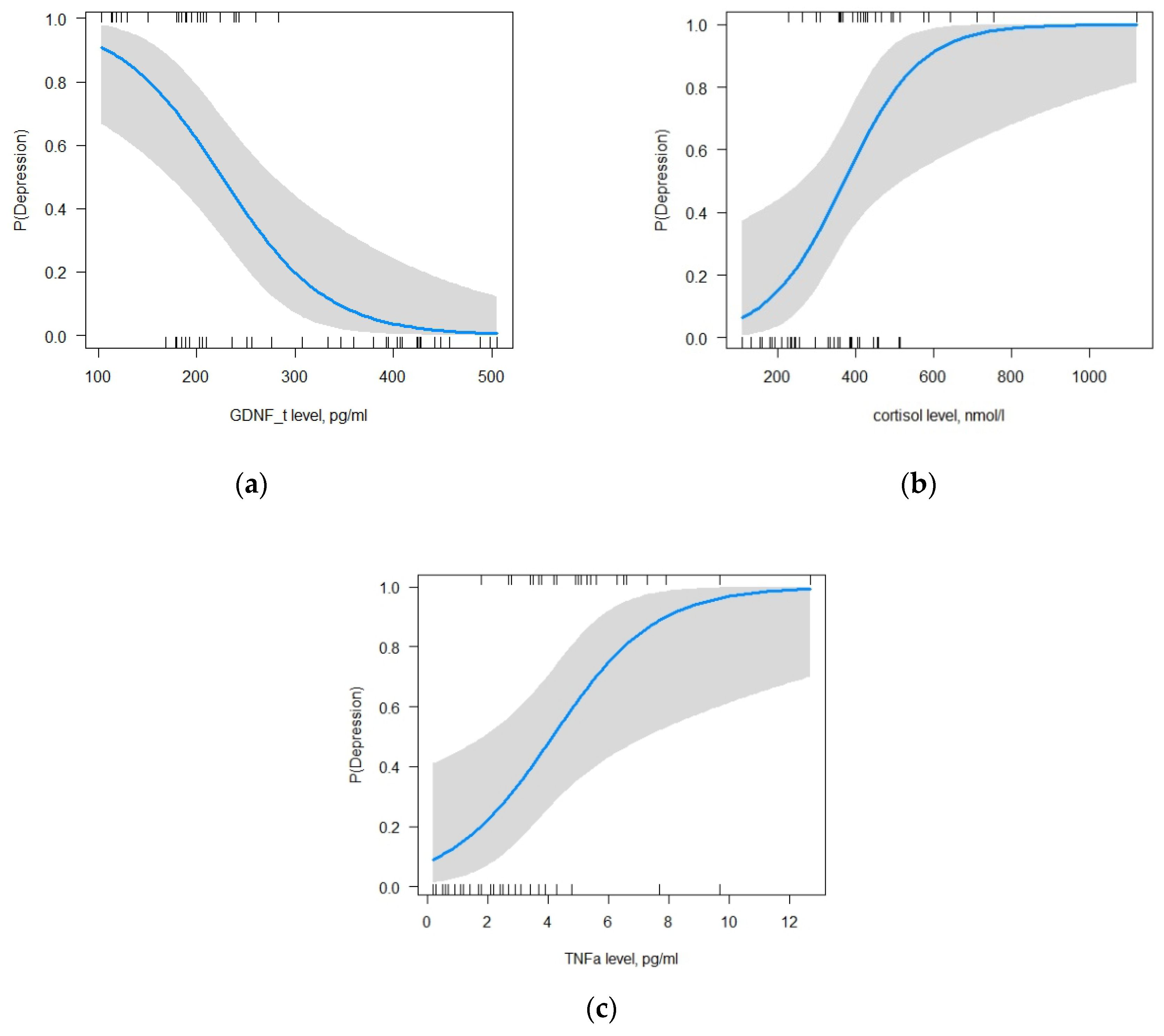
2.5.2. The Model for MDD
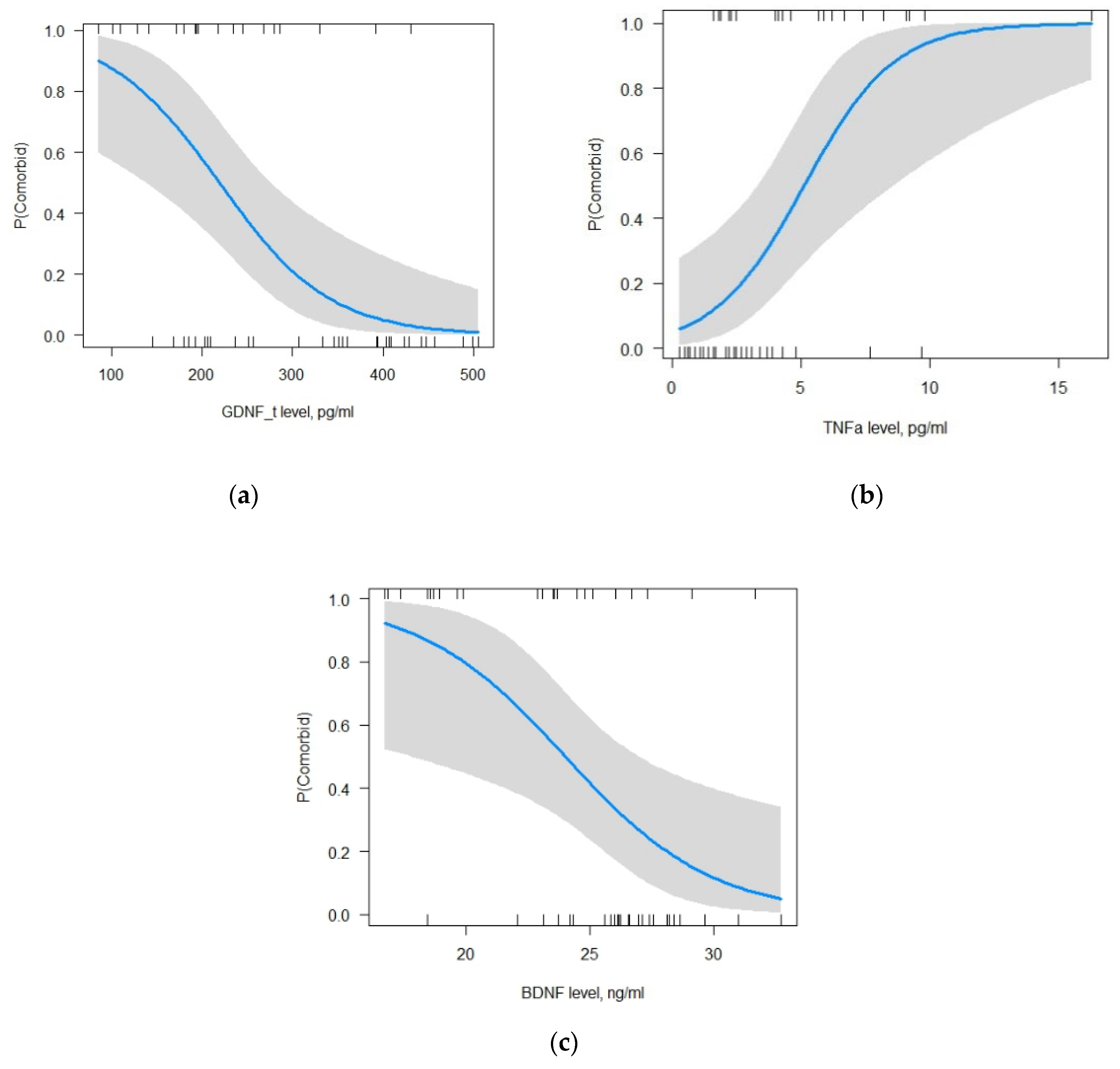
2.5.3. The Model for Focal Epilepsy with MDD
3. Discussion
3.1. Neurotrophic Factors in Epilepsy
3.2. Relationship between Neurotrophic Factors, HPA Axis, and Inflammation
4. Materials and Methods
4.1. Subjects
4.2. Samples
4.3. Assessment of Biochemical Indices and Hormones
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Price, R.B.; Duman, R. Neuroplasticity in cognitive and psychological mechanisms of depression: An integrative model. Mol. Psychiatry 2020, 25, 530–543. [Google Scholar] [CrossRef] [PubMed]
- Kanner, A.M. Psychiatric comorbidities in new onset epilepsy: Should they be always investigated? Seizure 2017, 49, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Vinti, V.; Dell’Isola, G.B.; Tascini, G.; Mencaroni, E.; Cara, G.D.; Striano, P.; Verrotti, A. Temporal Lobe Epilepsy and Psychiatric Comorbidity. Front. Neurol. 2021, 12, 775781. [Google Scholar] [CrossRef] [PubMed]
- Gulyaeva, N.V. Stress-Associated Molecular and Cellular Hippocampal Mechanisms Common for Epilepsy and Comorbid Depressive Disorders. Biochemistry 2021, 86, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Gulyaeva, N.V. Glucocorticoids Orchestrate Adult Hippocampal Plasticity: Growth Points and Translational Aspects. Biochemistry 2023, 88, 565–589. [Google Scholar] [CrossRef] [PubMed]
- Iughetti, L.; Lucaccioni, L.; Fugetto, F.; Predieri, B.; Berardi, A.; Ferrari, F. Brain-derived neurotrophic factor and epilepsy: A systematic review. Neuropeptides 2018, 72, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Colucci-D’Amato, L.; Speranza, L.; Volpicelli, F. Neurotrophic Factor BDNF, Physiological Functions and Therapeutic Potential in Depression, Neurodegeneration and Brain Cancer. Int. J. Mol. Sci. 2020, 21, 7777. [Google Scholar] [CrossRef]
- Asiedu, K.; Markoulli, M.; Bonini, S.; Bron, A.J.; Dogru, M.; Kwai, N.; Poynten, A.; Willcox, M.D.; Krishnan, A.V. Tear film and ocular surface neuropeptides: Characteristics, synthesis, signaling and implications for ocular surface and systemic diseases. Exp. Eye Res. 2022, 218, 108973. [Google Scholar] [CrossRef]
- Kimura, A.; Namekata, K.; Guo, X.; Harada, C.; Harada, T. Neuroprotection, Growth Factors and BDNF-TrkB Signalling in Retinal Degeneration. Int. J. Mol. Sci. 2016, 17, 1584. [Google Scholar] [CrossRef]
- Paolone, G.; Falcicchia, C.; Lovisari, F.; Kokaia, M.; Bell, W.J.; Fradet, T.; Barbieri, M.; Wahlberg, L.U.; Emerich, D.F.; Simonato, M. Long-Term, Targeted Delivery of GDNF from Encapsulated Cells Is Neuroprotective and Reduces Seizures in the Pilocarpine Model of Epilepsy. J. Neurosci. 2019, 39, 2144–2156. [Google Scholar] [CrossRef]
- Mikroulis, A.; Waloschková, E.; Bengzon, J.; Woldbye, D.; Pinborg, L.H.; Jespersen, B.; Avila, A.S.; Laszlo, Z.I.; Henstridge, C.; Ledri, M.; et al. GDNF Increases Inhibitory Synaptic Drive on Principal Neurons in the Hippocampus via Activation of the Ret Pathway. Int. J. Mol. Sci. 2022, 23, 13190. [Google Scholar] [CrossRef]
- Ibáñez, C.F.; Andressoo, J.O. Biology of GDNF and its receptors—Relevance for disorders of the central nervous system. Neurobiol. Dis. 2017, 97 Pt B, 80–89. [Google Scholar] [CrossRef]
- Duarte Azevedo, M.; Sander, S.; Tenenbaum, L. GDNF, A Neuron-Derived Factor Upregulated in Glial Cells during Disease. J. Clin. Med. 2020, 9, 456. [Google Scholar] [CrossRef] [PubMed]
- Shpak, A.; Guekht, A.; Druzhkova, T.; Rider, F.; Gudkova, A.; Gulyaeva, N. Increased ciliary neurotrophic factor in blood serum and lacrimal fluid as a potential biomarkers of focal epilepsy. Neurol. Sci. 2022, 43, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Shpak, A.A.; Guekht, A.B.; Druzhkova, T.A.; Rider, F.K.; Gulyaeva, N.V. Brain-derived neurotrophic factor in blood serum and lacrimal fluid of patients with focal epilepsy. Epilepsy Res. 2021, 176, 106707. [Google Scholar] [CrossRef]
- Zinchuk, M.S.; Guekht, A.B.; Druzhkova, T.A.; Gulyaeva, N.V.; Shpak, A.A. Glial cell line-derived neurotrophic factor (GDNF) in blood serum and lacrimal fluid of patients with a current depressive episode. J. Affect. Disord. 2022, 318, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Chiavellini, P.; Canatelli-Mallat, M.; Lehmann, M.; Goya, R.G.; Morel, G.R. Therapeutic potential of glial cell line-derived neurotrophic factor and cell reprogramming for hippocampal-related neurological disorders. Neural Regen. Res. 2022, 17, 469–476. [Google Scholar] [CrossRef]
- Dehelean, L.; Romosan, A.M.; Papava, I.; Bredicean, C.A.; Dumitrascu, V.; Ursoniu, S.; Romosan, R.S. Prolactin response to antipsychotics: An inpatient study. PLoS ONE 2020, 15, e0228648. [Google Scholar] [CrossRef]
- Simonato, M.; Tongiorgi, E.; Kokaia, M. Angels and demons: Neurotrophic factors and epilepsy. Trends Pharmacol. Sci. 2006, 27, 631–638. [Google Scholar] [CrossRef]
- Gliwińska, A.; Czubilińska-Łada, J.; Więckiewicz, G.; Świętochowska, E.; Badeński, A.; Dworak, M.; Szczepańska, M. The Role of Brain-Derived Neurotrophic Factor (BDNF) in Diagnosis and Treatment of Epilepsy, Depression, Schizophrenia, Anorexia Nervosa and Alzheimer’s Disease as Highly Drug-Resistant Diseases: A Narrative Review. Brain Sci. 2023, 13, 163. [Google Scholar] [CrossRef]
- Sharma, V.; Singh, T.G.; Kaur, A.; Mannan, A.; Dhiman, S. Brain-Derived Neurotrophic Factor: A Novel Dynamically Regulated Therapeutic Modulator in Neurological Disorders. Neurochem. Res. 2023, 48, 317–339. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Hu, Z.; Zhong, K. The Role of Brain-Derived Neurotrophic Factor in Epileptogenesis: An Update. Front. Pharmacol. 2021, 12, 758232. [Google Scholar] [CrossRef] [PubMed]
- Nowroozi, A.; Salehi, M.A.; Mohammadi, S. Brain-derived neurotrophic factor in patients with epilepsy: A systematic review and meta-analysis. Epilepsy Res. 2021, 178, 106794. [Google Scholar] [CrossRef]
- Martin, D.; Miller, G.; Rosendahl, M.; Russell, D.A. Potent inhibitory effects of glial derived neurotrophic factor against kainic acid mediated seizures in the rat. Brain Res. 1995, 683, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Kanter-Schlifke, I.; Georgievska, B.; Kirik, D.; Kokaia, M. Seizure suppression by GDNF gene therapy in animal models of epilepsy. Mol.Ther. 2007, 15, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Alvim, M.K.M.; Morita-Sherman, M.E.; Yasuda, C.L.; Rocha, N.P.; Vieira, L.; Pimentel-Silva, L.R.; Nogueira, M.H.; Barbosa, R.; Watanabe, N.; Coan, A.C.; et al. Inflammatory and neurotrophic factor plasma levels are related to epilepsy independently of etiology. Epilepsia 2021, 62, 2385–2394. [Google Scholar] [CrossRef]
- Miyanishi, H.; Nitta, A. A Role of BDNF in the Depression Pathogenesis and a Potential Target as Antidepressant: The Modulator of Stress Sensitivity “Shati/Nat8l-BDNF System” in the Dorsal Striatum. Pharmaceuticals 2021, 14, 889. [Google Scholar] [CrossRef]
- Druzhkova, T.A.; Yakovlev, A.A.; Rider, F.K.; Zinchuk, M.S.; Guekht, A.B.; Gulyaeva, N.V. Elevated Serum Cortisol Levels in Patients with Focal Epilepsy, Depression, and Comorbid Epilepsy and Depression. Int. J. Mol. Sci. 2022, 23, 10414. [Google Scholar] [CrossRef]
- Castro, L.M.; Gallant, M.; Niles, L.P. Novel targets for valproic acid: Up-regulation of melatonin receptors and neurotrophic factors in C6 glioma cells. J. Neurochem. 2005, 95, 1227–1236. [Google Scholar] [CrossRef]
- Chen, L.W.; Zhang, J.P.; Kwok-Yan Shum, D.; Chan, Y.S. Localization of nerve growth factor, neurotrophin-3, and glial cell line-derived neurotrophic factor in nestin-expressing reactive astrocytes in the caudate-putamen of1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-treated C57/Bl mice. J. Comp. Neurol. 2006, 497, 898–909. [Google Scholar] [CrossRef]
- Wu, X.; Chen, P.S.; Dallas, S.; Wilson, B.; Block, M.L.; Wang, C.C.; Kinyamu, H.; Lu, N.; Gao, X.; Leng, Y.; et al. Histone deacetylase inhibitors up-regulate astrocyte GDNF and BDNF gene transcription and protect dopaminergic neurons. Int. J. Neuropsychopharmacol. 2008, 11, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- McGonigal, A.; Becker, C.; Fath, J.; Hammam, K.; Baumstarck, K.; Fernandes, S.; Giusiano, B.; Dufau, S.; Rheims, S.; Maillard, L.; et al. BDNF as potential biomarker of epilepsy severity and psychiatric comorbidity: Pitfalls in the clinical population. Epilepsy Res. 2023, 195, 107200. [Google Scholar] [CrossRef] [PubMed]
- Romoli, M.; Mazzocchetti, P.; D’Alonzo, R.; Siliquini, S.; Rinaldi, V.E.; Verrotti, A.; Calabresi, P.; Costa, C. Valproic Acid and Epilepsy: From Molecular Mechanisms to Clinical Evidences. Curr. Neuropharmacol. 2019, 17, 926–946. [Google Scholar] [CrossRef] [PubMed]
- Porter, G.A.; O’Connor, J.C. Brain-derived neurotrophic factor and inflammation in depression: Pathogenic partners in crime? World J. Psychiatry 2022, 12, 77–97. [Google Scholar] [CrossRef] [PubMed]
- Vezzani, A.; Balosso, S.; Ravizza, T. Inflammation and epilepsy. In Handbook of Clinical Neurology; Elsevier B.V.: Amsterdam, The Netherlands, 2012; Volume 107, pp. 163–175. ISBN 9780444528988. [Google Scholar]
- de Vries, E.E.; Munckhof, B.V.D.; Braun, K.P.; van Royen-Kerkhof, A.; de Jager, W.; Jansen, F.E. Inflammatory mediators in human epilepsy: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2016, 63, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Debnath, M.; Berk, M.; Maes, M. Translational evidence for the Inflammatory Response System (IRS)/Compensatory Immune Response System (CIRS) and neuroprogression theory of major depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 111, 110343. [Google Scholar] [CrossRef]
- Cano-López, I.; Gonzalez-Bono, E. Cortisol levels and seizures in adults with epilepsy: A systematic review. Neurosci. Biobehav. Rev. 2019, 103, 216–229. [Google Scholar] [CrossRef]
- Guenther, S.; Bauer, S.; Hagge, M.; Knake, S.; Olmes, D.G.; Tackenberg, B.; Rosenow, F.; Hamer, H.M. Chronic valproate or levetiracetam treatment does not influence cytokine levels in humans. Seizure 2014, 23, 666–669. [Google Scholar] [CrossRef]
- Yamanaka, G.; Morichi, S.; Takamatsu, T.; Watanabe, Y.; Suzuki, S.; Ishida, Y.; Oana, S.; Yamazaki, T.; Takata, F.; Kawashima, H. Links between Immune Cells from the Periphery and the Brain in the Pathogenesis of Epilepsy: A Narrative Review. Int. J. Mol. Sci. 2021, 22, 4395. [Google Scholar] [CrossRef]
- Puangsri, P.; Jinanarong, V.; Ninla-Aesong, P. Impact of antidepressant treatmen on complete blood count parameters and inflammatory ratios in adolescents with major depressive disorder. J. Psychiatr. Res. 2023, 157, 26–35. [Google Scholar] [CrossRef]
- Fisher, R.S.; Cross, J.H.; French, J.A.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshé, S.L.; Peltola, J.; Roulet Perez, E.; et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshe, S.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for The Beck Depression Inventory, 2nd ed.; (BDI-II); Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Okragly, A.J.; Haak-Frendscho, M. An acid-treatment method for the enhanced detection of GDNF in biological samples. Exp. Neurol. 1997, 145, 592–596. [Google Scholar] [CrossRef]
- Vavilina, I.S.; Shpak, A.A.; Druzhkova, T.A.; Guekht, A.B.; Gulyaeva, N.V. Shedding Valuable Tears: Tear Fluid as a Promising Source of Disease Biomarkers. Neurochem. J. 2023, 17, 702–714. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter/ Group | HC M ± SD/M [Q1; Q3] (n = 39) | FE M ± SD/M [Q1; Q3] (n = 32) | FE + MDD M ± SD/M [Q1; Q3] (n = 28) | MDD M ± SD/M [Q1; Q3] (n = 46) |
|---|---|---|---|---|
| Age, years | 34.6 ± 10.6 | 37.4 ± 12.2 | 37.4 ± 10.6 | 36.7 ± 7.6 |
| Gender (male/female), % | 23/77 | 41/59 | 25/75 | 24/76 |
| Age, years (male/female) | 30.0 ± 4.6/35.6 ± 11.7 | 36.9 ± 12.6/37.7 ± 11.6 | 35.0 ± 6.2/37.9 ± 11.4 | 34.7 ± 7.7/37.3 ± 7.5 |
| Education(sec./higher), % | 49/51 | 44/56 | 68/32 | 56/44 |
| Employment (−/+), % | 13/87 | 59/41 | 52/48 | 54/46 |
| MMSE | - | 29 [28;30] | 27 [26;29] | 29 [28;30] |
| Beck II | - | 7 [3;13] | 28.5 [20;32] # | 30.5 [26;34] ** |
| Epilepsy duration, years | - | 16.9 ± 9.8 | 16.1 ± 10.7 | - |
| Take antipsychotics, % | - | 41 | 73 | 97 |
| Take antidepressants, % | - | 75 | 95 | 99 |
| Take tranquilizers, % | - | 53 | 64 | 68 |
| Take sodium channel blockers, % | - | 72 | 77 | 11 |
| Take GABA inhibitors, % | - | 0 | 9 | 0 |
| Take neurotransmitter release inhibitors, % | - | 41 | 36 | 0 |
| Take valproates, % | - | 34 | 32 | 5 |
| Take AMPA receptor antagonists, % | - | 16 | 5 | 0 |
| Take other (zonisamide, topiramate), % | - | 16 | 18 | 0 |
| Focal Onset Aware Seizure, % | - | 41 | 55 | - |
| Focal Onset Impaired Awareness, % | - | 72 | 64 | - |
| Focal to bilateral tonic–clonic seizure, % | - | 72 | 86 | - |
| Frequency of seizures: absence during the year/<1 per month/1–3 per month/1 or more seizures per week, % | - | 25/38/16/19 | 14/27/18/41 | - |
| Platelets, PLT, 103/µL | 250.0 ± 57.1 | 245.2 ± 69.5 | 266.1 ± 64.6 | 239.1 ± 58.0 |
| Erythrocytes, RBC, 106/µL | 4.7 ± 0.5 | 4.7 ± 0.4 | 4.5 ± 0.5 | 4.6 ± 0.5 |
| Hemoglobin, Hb, g/L | 138.4 ± 13.5 | 138.3 ± 14.2 | 138.2 ± 13.9 | 138.7 ± 13.8 |
| White blood cell, WBC, 103/µL | 6.6 ± 1.7 | 5.6 ± 1.5 * | 6.4 ± 1.8 | 6,3 ± 1.6 |
| Neutrophils, NE, % | 58.0 ± 7.2 | 54.5 ± 9.1 | 54.2 ± 8.4 | 52.1 ± 10.0 * |
| Lymphocytes, LY, % | 31.2 ± 6.8 | 33.6 ± 9.0 | 35.1 ± 7.9 * | 36.6 ± 9.3 * |
| Monocytes, MO, % | 7.5 [6;8.6] | 8.6 [7.3;10.3] * | 7.1 [6.2;9.5] | 7.8 ± 1.8 |
| Eosinophils, EO, % | 2 [1;2.6] | 2 [1.2;3.1] | 1.9 [1.6;2.7] | 2.6 [1.5;3.9] |
| Basophils, BA, % | 0.7 [0.5;1] | 0.6 [0.4;1.1] | 0.7 [0.45;0.9] | 0.9 [0.6;1.2] |
| NE/LY, NLR | 1.73 [2;1.5] | 1.7 [1.2;2.3] | 1.6 [1.1;2.1] | 1.4 [1.1;2] |
| LY/MO, LMR | 4.2 [3.6;5] | 3.9 [2.9;4.6] | 4.4 [3.5;6] | 4.7 [3.8;6] |
| PLT/NE, PNR | 68.66 [54.4;78.3] | 84.7 [69.2;111.4] * | 66.1 [49.3;89.6] | 78.4 [57.5;94.5] |
| PLT/LY, PLR | 123.7 [104.7;155.2] | 131.1 [101.1;161.2] | 103 [79;136] | 103.2 [87;138] |
| PLT/MO, PMR | 616 [448;639] | 551 [415.2;630.1] | 474 [383;589] | 505.5 [411;628] |
| Total bilirubin, µmol/L | 8.85 [6.6;12.1] | 9.7 [7.2;12.3] | 7.6 [6.6;10.2] | 10.7 [7.5;15.5] |
| Glucose, mmol/L | 4.95 [4.5;5.4] | 5.1 [4.8;5.5] | 5.1 [5;5.5] | 4.9 [4.6;5.2] |
| Creatinine, µmol/L | 78 [69;86] | 85 [75.5;93.5] | 79 [74;89] | 82 [73;92] |
| Urea, mmol/L | 4.3 [3.4;5.2] | 3.5 [3.1;5] | 3.9 [3.3;5] | 3.8 [3.4;4.5] |
| Cholesterol, mmol/L | 5.2 ± 1.2 | 6.0 ± 1.3 | 5.3 ± 1.3 | 4.2 ± 1.2 |
| Triglycerides, mmol/L | 1.4 ± 0.5 | 1.5 ± 0.8 | 1.3 ± 0.6 | 1.7 ± 0.6 |
| K, mmol/L | 4.3 ± 0.4 | 4.3 ± 0.5 | 4.4 ± 0.4 | 4.5 ± 0.4 |
| Na, mmol/L | 136.0 ± 4.0 | 140.5 ± 3.1 | 140.0 ± 4.7 | 139.4 ± 3.4 |
| Ca, mmol/L | 1.2 ± 0.1 | 1.3 ± 0.4 | 1.4 ± 0.5 | 1.2 ± 0.2 |
| TSH, ulU/mL | 1.7 [1.26;2.27] | 1.8 [1.3;2.6] | 2.2 [1.6;2.8] | 2 [1.3;2.8] |
| ACTH, pg/mL | 9.6 [7.9;15.7] | 10.1 [8;13] | 11.6 [7.5;15.7] | 12.5 [10.3;14.7] |
| Prolactin, ng/mL | 11.17 [8.2;15] | 11.7 [8.7;19.2] | 12 [9.3;16.7] | 23.3 [13.5;39.2] ∗ |
| GDNF_t, pg/mL | 355.2 [209.5;426.5] | 216.7 [157.5;247.5] * | 194.5 [151.8;263.4] * | 188.8 [131.5;227.5] * |
| GDNF_s, pg/mL | 158.3 [130.2;200.2] | 135.8 [115.5;160.8] | 146.1 [106.7;195.3] | 143.4 [128.6;186.6] |
| BDNF, ng/mL | 25.83 ± 2.74 | 23.12 ± 4 * | 22.61 ± 3.98 * | 23.25 ± 4.37 * |
| Cortisol, nmol/L | 295 [226;387] | 363 [264.2;478.3] | 409 [302.3;489] * | 426 [358;514.1] * |
| TNF-α, pg/mL | 1.8 [0.9;2.9] | 3.3 [2.3;4.8] * | 4.6 [2.5;6.7] * | 4.95 [3.78;6.43] * |
| GDNF in LF | GDNF in BS | BDNF | Cortisol | TNF-α | |
|---|---|---|---|---|---|
| N (number of observations) | 145 | 145 | 144 | 144 | 131 |
| R (Spearman) | −0.12 | −0.01 | 0.03 | 0.11 | 0.16 |
| p-value | 0.17 | 0.88 | 0.69 | 0.18 | 0.1 |
| SFE (Multiple Cause) M ± SD/M [Q1; Q3] (n = 19) | SFE (after Epi Surgery) M ± SD/M [Q1; Q3] (n = 8) | SFE (Traumatic Brain Injury, Stroke, Cerebrovascular Disorders) M ± SD/M [Q1; Q3] (n = 13) | CFE (Not Established) M ± SD/M [Q1; Q3] (n = 20) | |
|---|---|---|---|---|
| Age, years | 36.9 ± 11.4 | 34.9 ± 9.0 | 40.4 ± 14.1 | 41.9 ± 11.4 |
| Gender (male/female), % | 37/63 | 25/75 | 31/69 | 30/70 |
| Education(secondary/higher), % | 47/53 | 62/38 | 46/54 | 65/35 |
| Employment (−/+), % | 43/57 | 62/38 | 62/38 | 61/39 |
| MMSE | 28 [26;29] | 30 [26;30] | 26 [25.5;28] | 29 [26;30] |
| Beck II | 13 [6;29] ** | 4.5 [2;16] | 21 [13;2] ** | 16 [10;25] ** |
| With MDD, % | 37 ** | 0 | 69 ** | 43 ** |
| Cortisol, nmol/L | 399 [300;460.5] | 337 [306.5;454.1] | 391 [366;461] | 411 [275.3;505.1] |
| TNF-α, pg/mL | 3 [2.1;4.45] | 3.8 [2.8;6] | 5.9 [3.95;8] * | 4.3 [2.52;5.9] |
| GDNF, pg/mL in LF | 156.8 ± 57.4 | 141.0 ± 38.3 | 149.2 ± 41.0 | 131.5 ± 33.5 |
| GDNF, pg/mL in BS | 209.0 ± 73.8 | 191.3 ± 47.8 | 213.6 ± 79.0 | 213.7 ± 79.7 |
| BDNF, ng/mL | 19.9 [18.5;24.3] | 24.3 [20.4;25.1] | 24.5 [18.9;26.2] | 22.67 [19.4;26.6] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shpak, A.A.; Rider, F.K.; Druzhkova, T.A.; Zhanina, M.Y.; Popova, S.B.; Guekht, A.B.; Gulyaeva, N.V. Reduced Levels of Lacrimal Glial Cell Line-Derived Neurotrophic Factor (GDNF) in Patients with Focal Epilepsy and Focal Epilepsy with Comorbid Depression: A Biomarker Candidate. Int. J. Mol. Sci. 2023, 24, 16818. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms242316818
Shpak AA, Rider FK, Druzhkova TA, Zhanina MY, Popova SB, Guekht AB, Gulyaeva NV. Reduced Levels of Lacrimal Glial Cell Line-Derived Neurotrophic Factor (GDNF) in Patients with Focal Epilepsy and Focal Epilepsy with Comorbid Depression: A Biomarker Candidate. International Journal of Molecular Sciences. 2023; 24(23):16818. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms242316818
Chicago/Turabian StyleShpak, Alexander A., Flora K. Rider, Tatiana A. Druzhkova, Marina Y. Zhanina, Sofya B. Popova, Alla B. Guekht, and Natalia V. Gulyaeva. 2023. "Reduced Levels of Lacrimal Glial Cell Line-Derived Neurotrophic Factor (GDNF) in Patients with Focal Epilepsy and Focal Epilepsy with Comorbid Depression: A Biomarker Candidate" International Journal of Molecular Sciences 24, no. 23: 16818. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms242316818