3. Optimization over a Single Week of Treatment
In the present section (as well as in
Section 4), we assume that the period of radiation treatment administration consists of an integer number of weeks,
, and that treatment breaks are left at each weekend according to the standard medical practice. The total number of delivered fractions
n and the overall treatment time
T of the Equations (
1)–(
3) become
We assume that , and then the overall treatment time T, is assigned. Then, the optimization problem considered here is to minimize the logarithm of the tumor surviving fraction S with respect to the fractional dose sizes only. Noting that does not depend on the doses, the problem is equivalent to that of minimizing the quantity . To simplify the optimization problem, we also assume that the cumulative damages to normal tissues, and , are equi-distributed over the treatment weeks. This choice allows us to reformulate the problem over a single week of treatment, thus reducing the number of variables and, at the same time, to strengthen the constraints on the normal tissue damage. The obtained solution is then repeated for each treatment week.
Let us introduce the notations
We observe that the radiosensitivity ratios are in general greater than 1 Gy either for tumors and for normal tissues. Typical values of
reported in the literature range from about 2–3 to 50 Gy or more, whereas for the early and late normal tissues it is
[
4,
29,
30]. Let us now define the 5-dimensional vector
d with components
. The constraints in Equation (
5) can be written in the form
and we can formulate the optimization problem to be solved over a single treatment week.
Problem 1. Minimize the functionon the admissible set It is important to note that Problem 1 certainly admits some optimal solutions in view of the Weierstrass theorem [
31]. As the problem is not convex, the set of solution candidates is found by means of the Karush–Kuhn–Tucker necessary conditions of optimality. Theorems 1 and 2, reported here without demonstrations (see the complete proofs in [
7]), illustrate how these candidates are structured, evidencing how they can be grouped into classes of equivalent, i.e., providing the same value of
J, extremal solutions. The equivalence of the elements within each class is easily understood noticing that
J,
,
depends only on the quantities
,
, and
.
Theorem 1. There are possible structures for the solutions d of Problem 1, including the trivial vector . The non-trivial solutions may be grouped into 10 mutually exclusive classes, as reported in Table 1. The classes are characterized by the number of non-zero doses, as well as by the number of consecutive non-zero doses. The possible structures in each class are equivalent, in that they have the same size of the non-zero doses and then give the same value of the cost function J. Proof. A formal proof can be found in [
7]. The values of the non-zero doses in
Table 1 depend on
,
,
,
,
, and
through the Lagrangian multipliers in a rather complicated manner. If the interaction between adjacent fractions is absent or negligible, explicit expressions of the non-zero fraction doses can be given in terms of the normal tissue parameters only, as it is shown below. □
Since the parameters
,
, and
are very large for the majority of tumors and normal tissues, the repair process can be considered completed within the interfraction interval
, which means that the incomplete repair term can be disregarded in the model formulation. Under this assumption, the solutions reduce to only five mutually exclusive classes of (equivalent) solutions, having simple component expressions in terms of the model parameters. Then, the following results hold [
7].
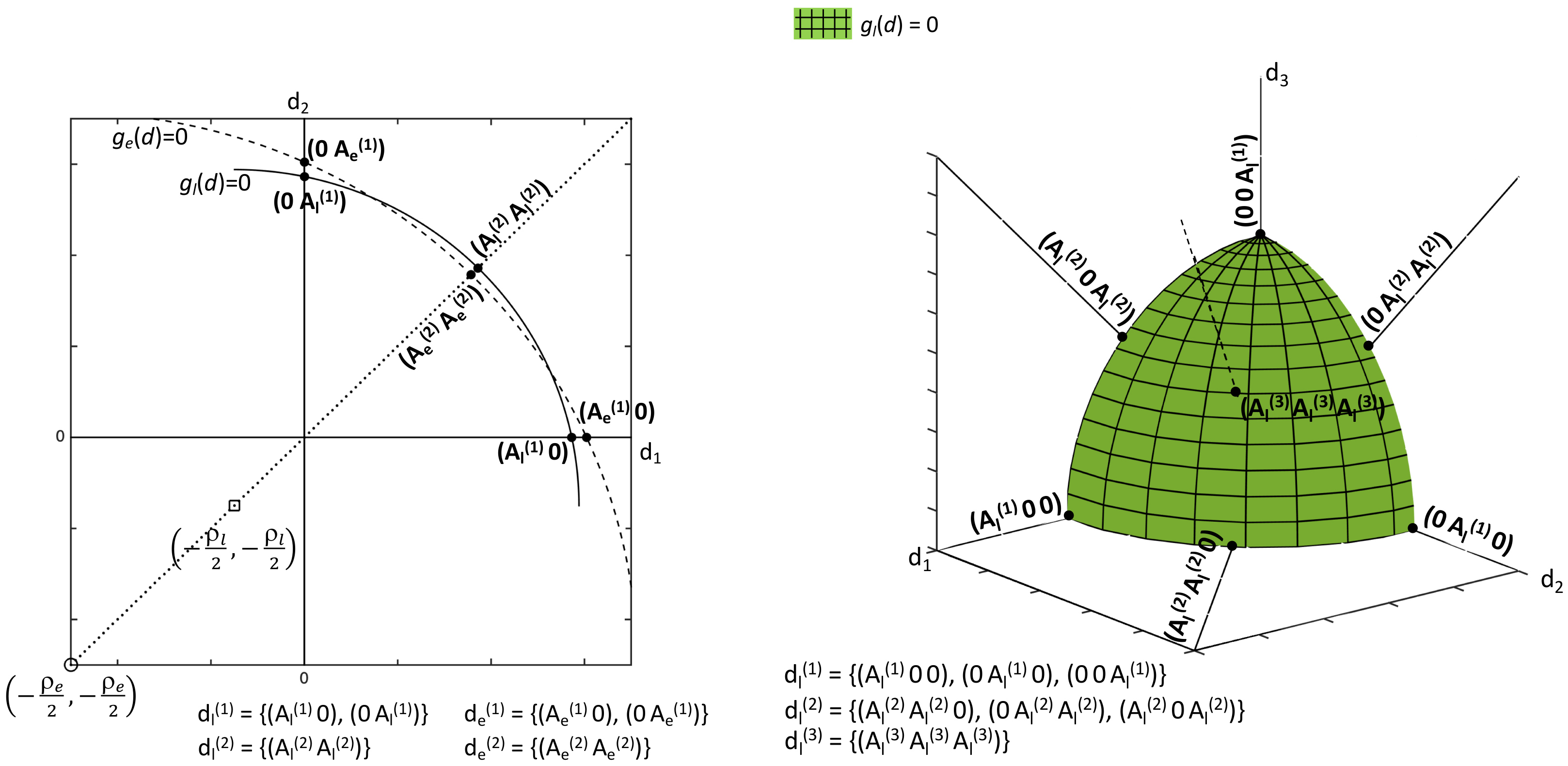
Theorem 2. In the absence of the incomplete repair term, there are at most five different extremal candidates of Problem 1 given by the following representative structures:whereand Proof. A detailed proof of this result based on solving the Karush–Kuhn–Tucker system of necessary optimality conditions, is reported in [
7]. In the present simpler, but practically meaningful, case of negligible interaction among dose fractions, a geometrical interpretation of the extremal solutions can be given and it is qualitatively illustrated by
Figure 1 for
and 3. It can be noticed that the expressions of the boundaries of Equations (
8) and (
9) represent hyperspheres with centers on the five-dimensional bisect line at
,
, for any
i. Then, the problem extremals lie on the positive portions of the boundaries of
,
, and precisely of the most restrictive constraint boundary (see Equation (
12)) as shown in the left panel of
Figure 1. Increasing
n, the set of candidates is enriched with additional structures, as illustrated in the right panel of
Figure 1 for the simplified situation of a single prevalent quadratic constraint (for instance
). The examples of
Figure 1 can be considered representative of the more complex situation depicted by Theorem 1 (problem including dose interaction). Then, the problem geometry is similar to that of
Figure 1 except for the fact that Equations (
8)–(
10) have elliptic contours, which makes the extremal set wider and the problem resolution more complicated. □
We remind that
and we notice from
Figure 1 that the admissibility of the structures of Theorem 2 depends on the relative position of the early and late constraint boundaries, i.e., on
and
. Moreover, since the level surfaces of the cost function in Equation (
10) are again hyperspheres with (fixed) center on the bisect line at
,
, aligned with the early and late boundary centers, the optimum among the five structures depends on the value of
with respect to
and
. Denoting by
and
,
, the vectors with
i non-zero entries equal to
and
, respectively, we define the quantity
which, as suggested by the geometrical interpretation of
Figure 1, determines whether the early or instead the late constraint is prevalent. Here follows a sketch of the solutions for the simplified problem without incomplete repair term.
Theorem 3. In the absence of the incomplete repair term, Problem 1 admits a unique optimal solution, apart from the previously mentioned equivalence of the structures in each class, when and . Table 2 reports the optimal solutions for and , while Table 3 reports the optimal solutions for and . Proof. A rigorous proof is reported in [
7] and it basically consists in expressing the cost function for any extremal point provided by Theorem 2 in terms of model parameters and in comparing its values. We remark that the result of this comparison depends on the value of
with respect to
and
. Reminding that the cost function level surfaces are concentric hyperspheres, the geometrical interpretation of the problem can give a hint on the optimal solution. Moreover, we note that, when
v is an integer number between 1 and 5, then, for suitable
, the optimal solution is such that
, i.e., these vectors satisfy simultaneously the early and the late constraints with the equality sign. □
In
Table 2 and
Table 3, it emerges how the tumor radiosensitivity ratio
determines the kind of optimal fractionation scheme. Indeed, hypofractionation is convenient for small
, whereas the optimal fractionation tends to be uniform for large
. This result formalizes in mathematical terms and confirms previous observations [
32,
33]. Other papers have then reported expressions of the optimal solution for similar problems in a form substantially equivalent to Equation (
13) [
11,
34,
35,
36,
37,
38].
We consider now some applications that further specialize the previous results in terms of the important practical situation of prevalent late constraint.
Since the radiation-induced damages to healthy tissues cannot be directly measured, it is common to evaluate them as the damages produced by a reference radiotherapy protocol according to a chosen dose–response model [
3,
5]. Then, it is useful to introduce the Biologically Effective Dose (BED) defined as the total radiation dose proportional to the logarithmic cell kill that globally produces the same damage of a given protocol [
39]. Using subscripts “e” and “l” as done previously, the maximal tolerable damages caused to normal tissue are expressed as
and
. We set as the reference scheme, the conventional equi-fractionated scheme (one fraction/day, five fractions/week), with
fractions of size
over the time
. Thus, we can write
To simplify the comparisons of the numerical results for Problem 1 with data of real clinical protocols, we take as a reference protocol a radiotherapy scheme that includes an integer number of weeks,
, with
. From Equation (
7), for the maximal weekly damages, we have
From Equation (
17), it is easy to verify that
, since
, and that
(see Equation (
14)). It has been shown in [
7] (see Th. 6) that, for
,
, the late constraint
dominates over
and the optimal solution is
when
or
when
.
We performed numerical simulations to verify the previous results and compare them to the relevant literature. The normal tissue parameters, for which rather homogeneous estimates are available, were set to
Gy,
Gy,
Gy
,
days, and
days [
3,
5]. To quantify
and
, we considered a reference radiotherapy protocol and computed the damages it produces on normal tissues according to Equation (
17). In particular, the “strong standard” fractionation schedule
days (
,
Gy) yields BED
Gy and BED
Gy [
5,
27].
Table 4 reports the optimal solutions as
changes in a meaningful value range. For a comparison with the literature,
Table 5 focuses on
Gy and
Gy, typically associated to slowly proliferating tumors (prostate) and fast proliferating tumors (head and neck, lung).
Table 5 includes the computation of a quantity often used to evaluate the treatment efficacy, i.e., the tumor “log cell kill” (LCK) defined by
and given by
with
S as in Equation (
4) and
,
, and
as in Equations (
1) and (
3). As expected, for
Gy, the optimal solution coincides with the corresponding reference protocol. Conversely, when
Gy, the optimal solution is not uniform and it consists of a single fractional dose of amplitude higher than the conventional (reference) value. Thus, in agreement with several literature results, we find that, when
, the optimum is given by hypo-fractionated protocols (see, e.g., [
5,
28,
32,
33]).
A remark can be made about the normal tissue constraints considered in the present study. In the problem formulation, only two kinds of healthy tissue reactions, early and late, were taken into account. Moreover, the radiation response of tissues is considered homogeneous disregarding the spatial or inter-individual differences. Although simplistic, this representation of surrounding organs at risk is thought to capture the essential aspects in the optimization of traditional radiotherapy schedules and it actually is most commonly considered in the literature. However, expressing the damages as in Equations (
1)–(
5), we assumed that the normal tissues receive the same amount of radiation, i.e., the same fraction doses
, of the tumor, which is not very realistic. Indeed, modern techniques make increasingly feasible to deliver high fractions to the tumor while reducing the fractions to the surrounding tissues by spatially modulating the radiation intensity. While modeling such remarkable aspects is beyond the scope of the present work, it can be interesting to give an idea of some resulting effects on the optimal solutions. In [
7], this was done by introducing a global coefficient,
, to represent, on average, the attenuation of the dose received by normal tissues with respect to the tumor. Then, the effective fractional doses acting on normal tissues are
, in the related constraint expressions, i.e., in all the damage terms of Equation (
5), or
in the expressions of
,
computed by the reference protocol as in Equations (
15) and (
16). Moreover, to get expressions of
,
of the kind in Equations (
8) and (
9), we have to redefine accordingly the notation related to the normal tissue parameters (see also [
7]). In particular, we upgrade the notation in Equation (
7) setting
The optimal solutions of Problem 1 computed with
are reported in
Table 6 for a comparison with the results of
Table 4 where
. In the simulation of
Table 6, the reference fraction dose
Gy is left unchanged, but the maximal damages
and
are computed from Equations (
15) and (
16) using
instead of
. Then, the limits
,
are evaluated from Equation (
19) obtaining expressions formally identical to Equation (
17), provided that the parameters
,
are given as in Equation (
19).
The optimal solutions are found to be structurally identical to those of
Table 4, but the solution pattern appears to be shifted towards higher
values (so allowing hypofractionation also for tumors with relatively high
,
Gy in the example), while larger optimal doses are permitted in hypofractionated schemes.
6. Numerical Results
We report a concise review of the main numerical results on the optimal solution of Problem 3. We concentrate on this latter problem because the results allow us to evidence also properties common to the solution of Problems 1 and 2.
On the basis of the analytical results of
Section 5.1, after setting
, the numerical procedure selects the optimal solution
for each
computing the related
. Then, the optimal fraction number
is the number for which
attains its minimum value. Moreover, still according to the theoretical results of the previous sections, our numerical investigation focuses on three tumor classes, each identified by an interval of radiosensitivity ratio values: high (
, fast proliferating tumors), low (
, slowly proliferating tumors), and intermediate (
).
As mentioned above, the classification of tumors based on their proliferative behavior and on estimates has been widely used in the literature, while the advantage of using different non-conventional protocols for different tumor classes has been evidenced only recently. Therefore, our simulations were organized to explore the effect on the optimum of changing the tumor parameters.
For the computation of the maximal admissible damages
and
, again we chose an equi-fractionated reference protocol
, of the kind one fraction/day, five fractions/week. From Equations (
15) and (
23), we obtain
where the term
is independent of
n and entirely attributable to the reference protocol
From Equation (
16), we have
The simulations were carried out setting
so that it satisfies the reasonable condition
, where
is the fractional dose of the reference protocol and
is computed setting
and
in Equation (
33). The above condition ensures optimal treatments consisting of at least two fractions besides the admissibility of the reference protocol.
The values of the normal tissue parameters are relatively well assessed in the literature, whereas the tumor parameter estimates vary considerably, even for the same tumor type. A rather detailed literature search led us to fix in all the simulations the parameters of early and late normal tissue as
Gy,
Gy
, and
days and
days, and
Gy, respectively [
3,
4,
5,
42].
Concerning the tumor classes, fast proliferating tumors characterized by high radiosensitivity ratios are reckoned to include most human tumors, for instance head and neck, lung, and cervical cancers [
4,
27,
29,
30,
43]. We identify this tumor type with the range
. Currently, prostatic cancers are known as the most slowly proliferating human tumors; such tumors exhibit long potential doubling times, low proportions of cycling cells, and low radiosensitivity ratios, typically lower than late-responding normal tissues (
) [
32,
33,
44,
45,
46,
47,
48,
49]. Examples of tumors with
are breast cancer and some prostatic cancers observed to be not assimilable to slowly proliferating tumors [
30,
50,
51].
In view of the large variability of tumor parameters, we assumed a nominal set of parameter values for each tumor class, and then we explored how the optimal solution changes when the parameters vary in a meaningful range of values. Indeed, this is a crucial point for the application of our optimization procedure because it requires setting the values of parameters such as
and
, which can be affected by considerable estimation errors [
21,
35]. Interestingly, our simulations showed some robustness of the optimal protocols to variations of the parameters, as shown below.
We are interested in comparing the obtained optimal protocols to real clinical schedules, which can be done evaluating by means of the LQ model the effects that they produce in terms of cell killing. As in
Section 1, we chose the commonly used “strong standard” reference protocol
days, which provides BED
Gy, BED
Gy [
5,
27] and consequently
Gy
,
Gy
. The “log cell kill” defined in Equation (
18) to quantify tumor radiation damages now takes the form
We notice that minimizing
with respect to
n is equivalent to maximizing the quantity in square brackets in Equation (
40). Furthermore, it can be noticed from Equation (
40) that LCK does not depend directly on the tumor doubling time
, but on the product
. The inverse quantity
can be seen as an indicator of the tumor aggressiveness, since high values of this quantity are associated to rapid tumor repopulation (short
) accompanied by reduced radiosensitivity. An increase of
tends to reduce LCK and has to be counterbalanced by reducing the treatment length.
Figure 4,
Figure 5 and
Figure 6 summarize our numerical exploration of the optimum behaviour with respect to
,
, and
for the tumor classes fast, slow, and intermediate, respectively.
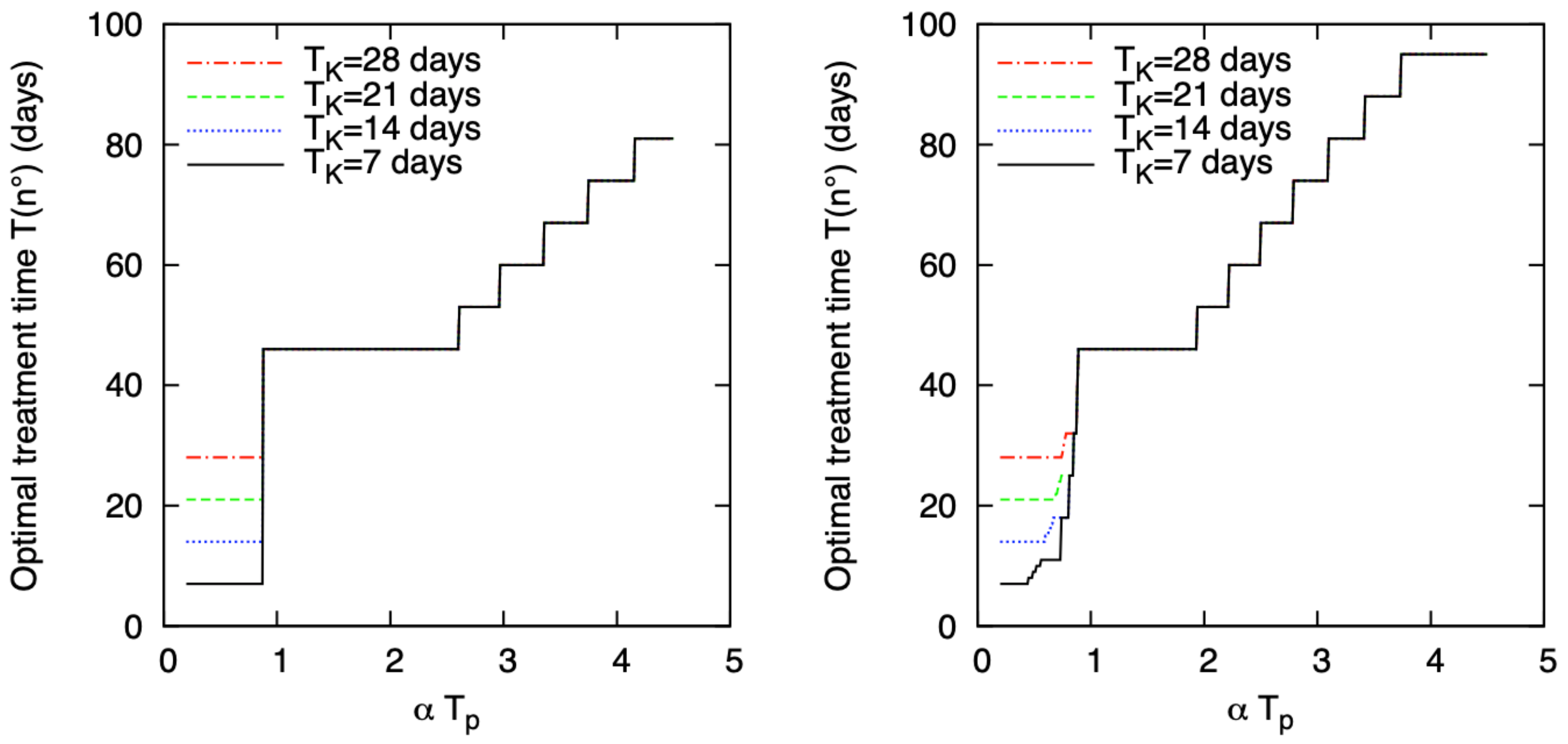
For fast proliferating tumors, the optimal fractionation scheme is uniform and made of fractions equal to
. By contrast, as observed by some authors, the optimal treatment length is affected by
and
(actually by
) [
4,
5].
Figure 4 shows the optimal treatment time as a function of the product
for
, 14, 21, and 28 days. Moreover,
(left) and 50 Gy (right), and
Gy. Taking into account that most typically the average
ranges in [1, 2.5] Gy
days, the most recurrent
is 46 days equal to the reference protocol duration. For very small
, schedules shorter than the standard reference are preferable and in particular as close as possible to
. When
is large, protracting the treatment time can be advantageous.
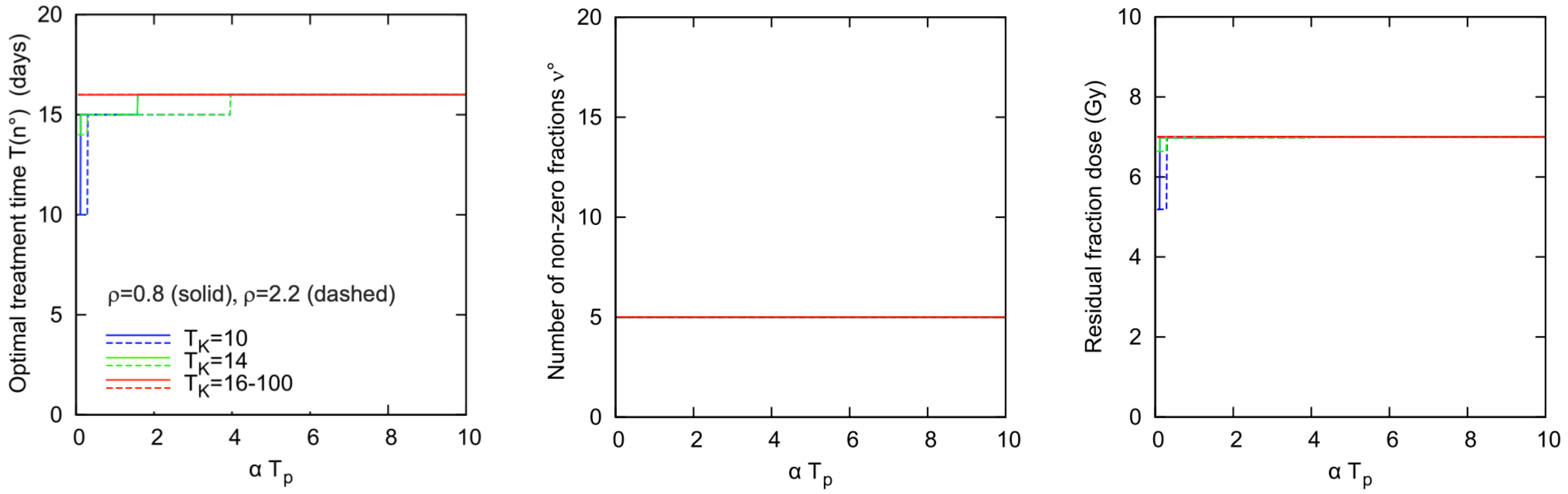
For tumors with low radiosensitivity ratios (), the optimal solution tends to be hypofractionated, i.e., composed by few fractions of large size, and in principle it would be made by a single fraction if could exceed . Hence, the choice of the limit is expected to strongly affect the optimal schedule. Higher tumor cell kill and lower normal tissue can be achieved using hypofractionated regimes rather than the conventional ones, provided that can be safely increased.
Figure 5 shows the optimal solution for the class
as a function of
for
Gy. For this class, the optimal protocol is completely specified by the triple
(or
), number of non-zero fractions at optimum
, size of the “residual fraction". In fact, we remind that the optima of this class take the form
or
, where
u depends on
and is such that
(see
Table 8,
Table 9 and
Table 10) and the residual fraction is the only fraction different from zero and from
. We add some comments to
Figure 5. First, the optimal treatment time of 16 days is the minimal time allowing to satisfy the early tissue constraint with the equality sign. Second, and perhaps more interesting, for most of the considered parameter values, the plots of
Figure 5 give a sharp indication of the optimum scheme of fractionation. Thus, when
, our simulation indicates that the optimal solution is substantially insensitive to variations of the tumor parameters (for fixed values of the normal tissue parameters and
), which can be considered a very favorable feature of the problem under study, in view of the high heterogeneity of tumors and of the large uncertainty affecting the estimation of tumor parameters. Clearly, from a modeling point of view, the problem shifts towards that of accurately assessing the healthy tissue constraints and the related bounds on the tolerable radiation damage, as well as the value of
.
However, for the case considered here of two quadratic normal tissue constraints with fixed parameters and a given , the numerical simulation suggests that a single radiotherapy protocol can be adopted for the class . The mentioned protocol holds almost everywhere in tumor parameter interval, while it possibly represents a sub-optimal solution for some parameter value. We also observe that such a robust solution is a safe solution since it is in compliance with the normal tissue constraints for any considered set of tumor parameters.
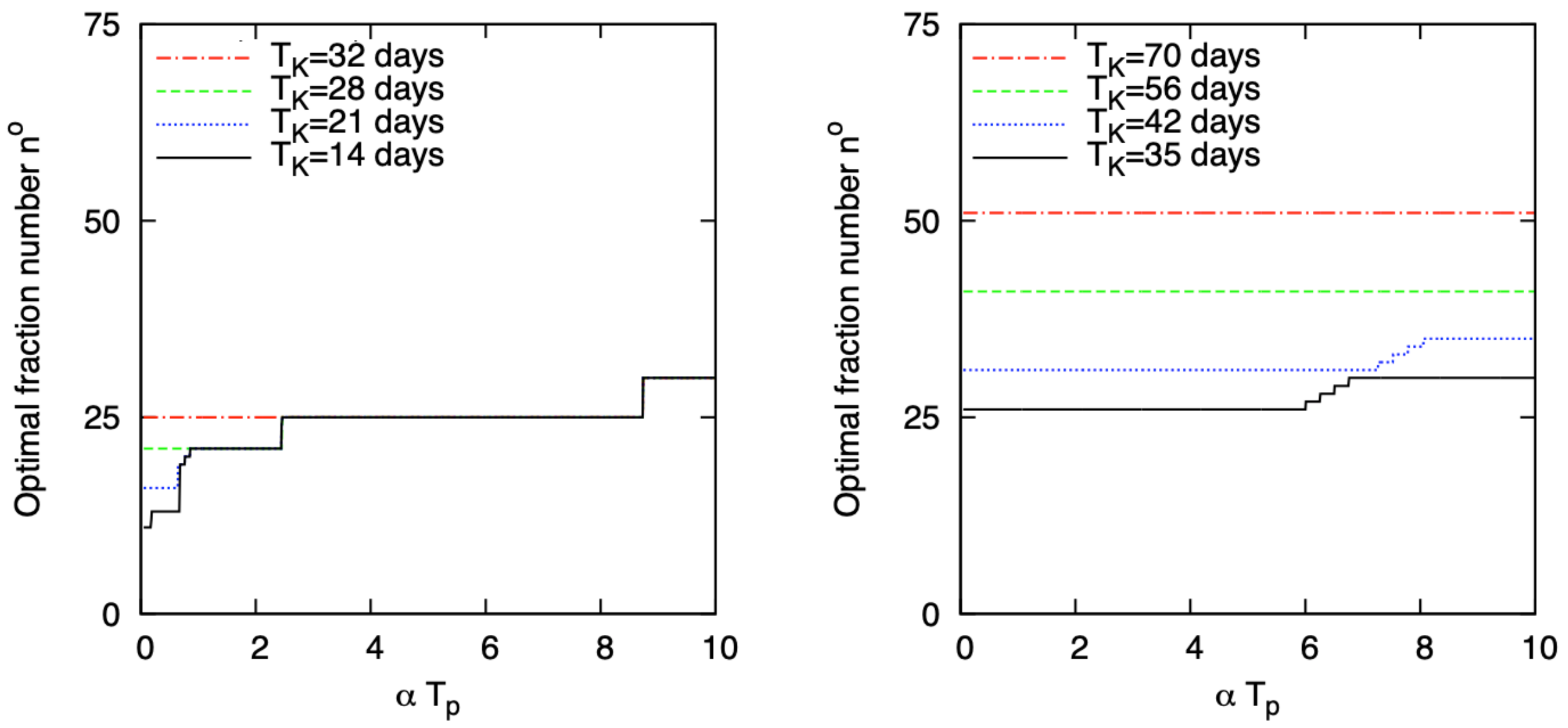
For intermediate
values,
, the optimal
as a function of
, for different values of
, for
Gy and setting
Gy is reported in
Figure 6. As before, all parameters have been set as the most recurrent in the literature. However, they are very scattered so that we expect to find different types of optimal schedules.
Depending on
being shorter (left) or longer (right) than the total reference protocol time
, the optimum is of the kind
, with
or 25 for the majority of
values (from 0.86 to 8.73 days/Gy). For small
,
is smaller than the number of fractions of the reference protocol (
) and the solution can be either
(the vector with all
entries) or of the kind
, depending on
. As depicted in
Figure 6 right panel, when
,
turns out to be slightly greater or equal to
for almost any
. Overall, the plots of
Figure 6 show that the optimal solutions are longer than the reference (
) and with fraction doses smaller than
, which also implies that they are not affected by different
choices. However, protracting the solution beyond
does not provide significant advantages in terms of LCK. Hence, in view of the scarceness of information about the “real” parameter values, treating tumors with intermediate proliferative behavior by means of standard fractionation schemes appears to be advantageous.
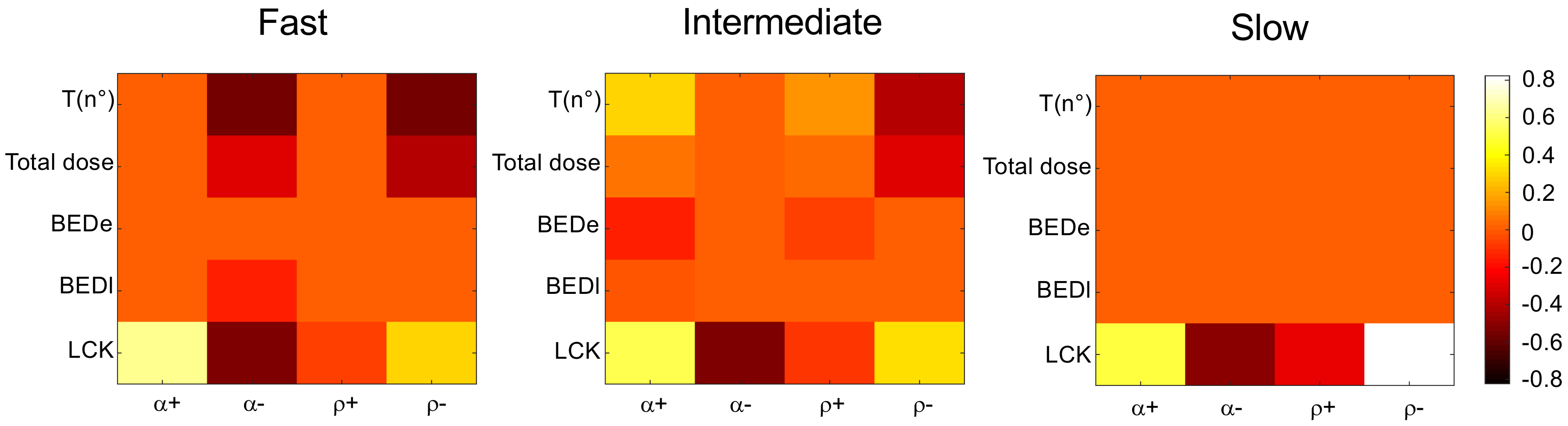
A final schematic view of the optimal protocol sensitivity for the tumor classes considered thus far is given in
Figure 7.
We applied relative perturbations of ±50% to the nominal values of
and
, computing the relative variations of the following output quantities at the optimum: total treatment time, total dose, normal tissues damages (BED
, BED
), and tumor LCK. For all tumor classes, the resulting LCK is the quantity that exhibits the most consistent relative variations, either positive or negative, and, in particular, it can be remarkably improved (up to 80% for slow proliferating tumors upon a −50% variation of
). Apart from the LCK variation at the optimum, as also shown by
Figure 4,
Figure 5 and
Figure 6, the solution for slow tumors is practically insensitive to the considered parameter variations, while the optimal solution for fast tumors is affected only by negative variations of
and
. For the class of intermediate tumors, upon both positive and negative ±50% parameter variations, we get output variations less than 30%. This is not surprising from the mathematical point of view, indicating that tumors with intermediate
can turn into the adjacent classes of fast or of slowly proliferating tumors.
We observe that
and the optimal total dose are moderately affected by the relative parameter variations, at least for slow and, in part, for intermediate tumors. On the contrary, for fast and intermediate tumors, significant variations for
(up to −54%, see
Figure 7, fast tumors panel,
and
columns) accompanied by noticeable variations of the optimal total dose (up to −35%) are obtained when the optimum
tends to equal the kick-off time (21 and 28 days, respectively) unlike the conventional reference time of 35 days. Finally, reminding that the optima for all tumor types maximize at least one of the prescribed normal tissue BEDs, we verify that at least one between BED
and BED
is unaffected by the parameter variations, while the other shows only small (obviously negative) variations not larger than −15%.
7. Concluding Remarks
The present work illustrates an example of the application of fundamental principles of finite-dimensional nonlinear optimization to a problem of relevant interest in the clinical practice, which is the problem of finding the best fractionation scheme in cancer EBRT treatment. We present in a unitary framework an overview of the main results of our previous studies [
7,
8,
9]. The problem formulation is based on the LQ model describing the instantaneous relation between radiation dose and cell survival for homogeneous cell populations. The model incorporates exponential repopulation, but the analytical results for
n fixed are in principle valid for different modeling choices of the time-varying part of the cell population response. In its more general version, the optimization problem includes a variable number of treatment sessions and it is a mixed-integer problem that can be solved by means of two consecutive steps: (i) an analytical step to express the optimal size of the fractional doses as a function of the model parameters for a fixed, but arbitrarily chosen, number of fractions
n; and (ii) a numerical step to simulate a sequence of optima obtained in Step (i) for
n increasing in order to find the optimal treatment time for specific tumor types.
Concerning Step (i), we present a few versions of the problem formulation following the chronological order of the activity of our research group in this field. Our approach provides a framework to analytically determine the optimal fractionation of the total radiation dose as a function of tumor type for any arbitrarily fixed integer number of fractions. On the basis of KKT optimality conditions, we classify the optimal solutions according to the tumor radiosensitivity ratio (
) and to the possibly imposed upper limit on the dose fraction size (
). We express the optimal fraction sizes as a function of the normal tissue parameters, recognizing the crucial role of
on the fractionation scheme for different tumor types. In particular, we confirm the convenience of adopting hypofractionated schedules for small
(i.e., slowly proliferating tumors), as previously evidenced by many authors [
4,
32,
45], and uniform schedules of the kind commonly used in the clinical practice in any other case.
The second step implements the numerical search of the optimal number of treatment sessions, focusing on three classes of tumor types characterized by specific ranges of the radiosensitivity ratio. The numerical results confirm the influence, highlighted above, of the ratio
on the fractionation scheme. Recognizing that the uncertainty affecting the parameter estimation, especially in heterogeneous neoplastic cell populations, can constitute a drawback for the application of our approach, we let the tumor parameters vary in broad ranges of parameter values trying, at the same time, to provide a schematic summary of the results [
9]. In particular, the numerical simulations have evidenced the role of the product
in the optimality of treatment duration. The quantity
can be seen as an indicator of the tumor aggressiveness, since it takes high values when rapid tumor repopulation is associated to low intrinsic radiosensitivity. Here, we present an excerpt from previous simulations reporting the optimal solution as a function of the product
. Based on the discriminating role of
, a remarkable results of our simulations is that for the majority of
values and for the three tumor classes considered, basically two fractionated schedules appear to be preferable; for
, the conventional clinical protocols (e.g., the “strong standard” 2 Gy protocol) are optimal, while, for
, hypofractionated protocols are generally preferable. Moreover, if experimental or clinical evidence indicates very low
values, shorter protocols with overall duration close to
and/or hyperfractionation may be optimal. Indeed, in [
9], we obtained optimal schemes delivering multiple fractions per day (and with treatment length near
) providing reduced late toxicity and increased tumor damage with respect to protocols with a single daily fraction. In addition, the sensitivity of the optimal solutions to
variations of
and
around their nominal values was evaluated. We stress that such a sensitivity analysis can be of some interest since the practical estimation of the radiosensitivity parameters can be critically affected by consistent estimation errors. With the only exception of the cases of
approximating
, which can occur for fast tumors with low
or
, the sensitivity analysis revealed that the optimal protocol variations are rather limited, with absolute variations of
and of the optimal total dose lower than 15%.
We acknowledge that our results rely on some simplifying modeling assumptions such as, in primis, the representation of the tissue response by means of the standard LQ model based on a deterministic dose–response function with four parameters. The same LQ formalism is used to model the normal tissue response and to set suitable boundary levels of the constraints necessary to ensure treatment safety. This can be considered too simplistic, especially in regard to the many biological processes involved in the normal tissue regeneration. The description of the radiation-induced damage to normal tissue and of the subsequent healing kinetics, as well as the description of the post-irradiation toxicity, are modeling issues really worthy of investigation as far as we are concerned with the optimization of cancer treatments. As an example of more sophisticated normal tissue representation, we mention the mechanistic approach by Hanin and Zaider [
52] who combined a deterministic model of the normal tissue kinetics with a stochastic representation of the inter-patient variation of kinetic parameters. However, despite the criticism, the simple exponential law, starting after a “kick-off” time from the treatment beginning, has been and continues to be largely used to model the tumor repopulation, as well as to predict the tolerable radiation levels of acute reactions in healthy tissues (see, e.g., [
4,
5,
11,
35,
42]).
Thus, concerning the normal tissue constraints, we assume the maximal tolerable levels for early and late complications, as well as the fraction limit
, as input data values of the optimization procedure. Furthermore, the quantities
and
(or
and
) have been expressed by means of the Biologically Effective Dose to evaluate the extreme boundaries of early and late side-effects. Then, these values are dependent on the model used to represent the damage and on a known tolerable clinical protocol set as the reference protocol. At present, this kind of representation based on the BED formalism is very frequently adopted and applied in planning external beam radiation treatments, at least for the management of early-stage disease cases [
24].
Finally, the modeling framework based on few “essential” parameters adopted in the present study, allowed us to give a remarkably synthetic picture of the results of the optimal radiotherapy problem. These results were obtained from the application of fundamental principles of the nonlinear optimization and appear to be in good agreement with observations reported in the theoretical and clinical literature.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}