Sleep Inertia Countermeasures in Automated Driving: A Concept of Cognitive Stimulation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Sleep and Sleep Inertia
- W: Wakefulness
- N1: Light sleep or dozing
- N2: Stable sleep
- N3: Deep sleep or slow wave sleep
- R: REM-sleep or dream sleep
1.2. Countering Sleep Inertia
1.3. Implications of Sleep Inertia in Automated Driving
- -
- cognitively and physiologically activating the driver after sleep.
- -
- motivating the driver after sleep.
- -
- assessing the driver’s alertness level to determine their readiness to drive.
2. Materials and Methods
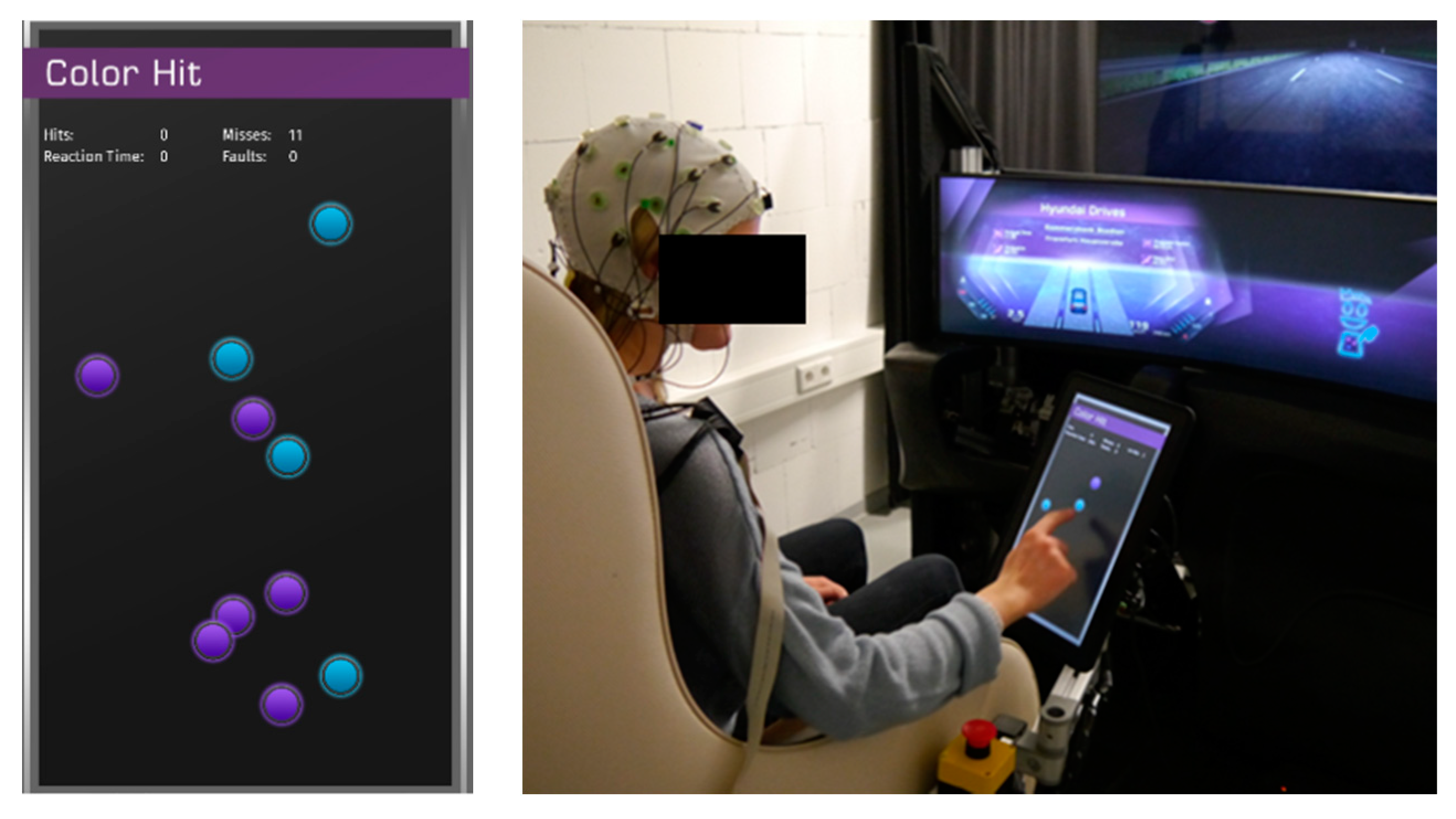
2.1. The Concept of the Sleep-Inertia Counter-Procedure for Drivers
2.2. An L4 Concept Driving Simulator to Investigate Sleep
2.3. Study Design
2.4. Data Analysis
3. Results
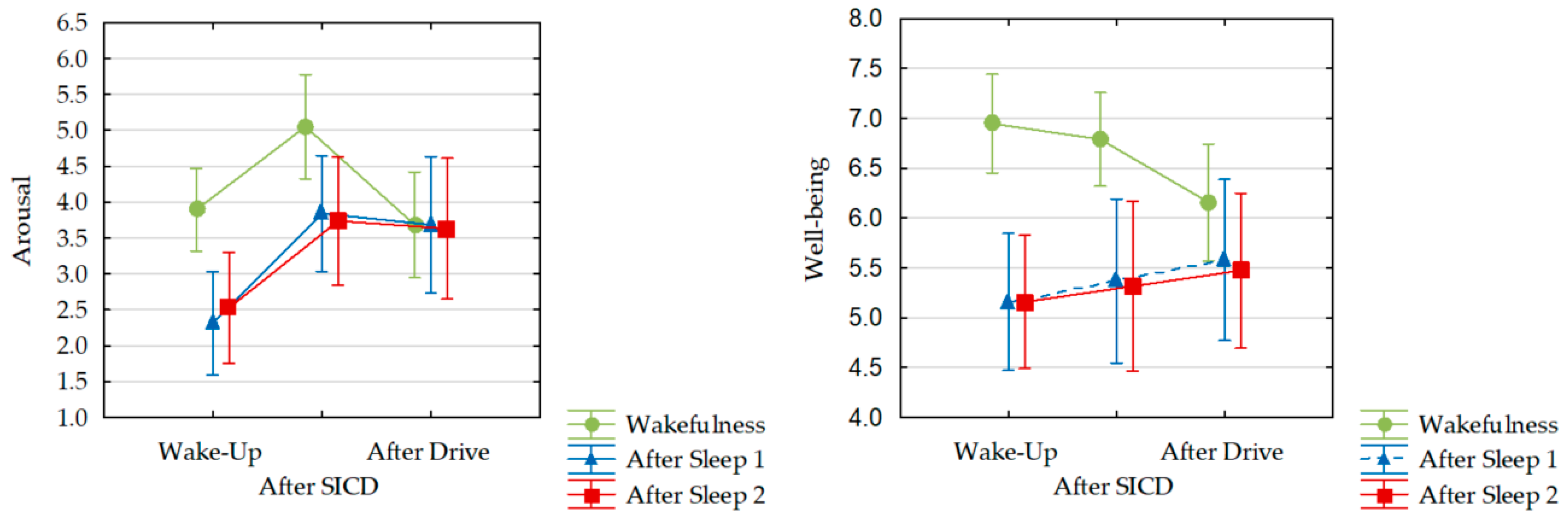
3.1. Subjective Arousal and Well-Being
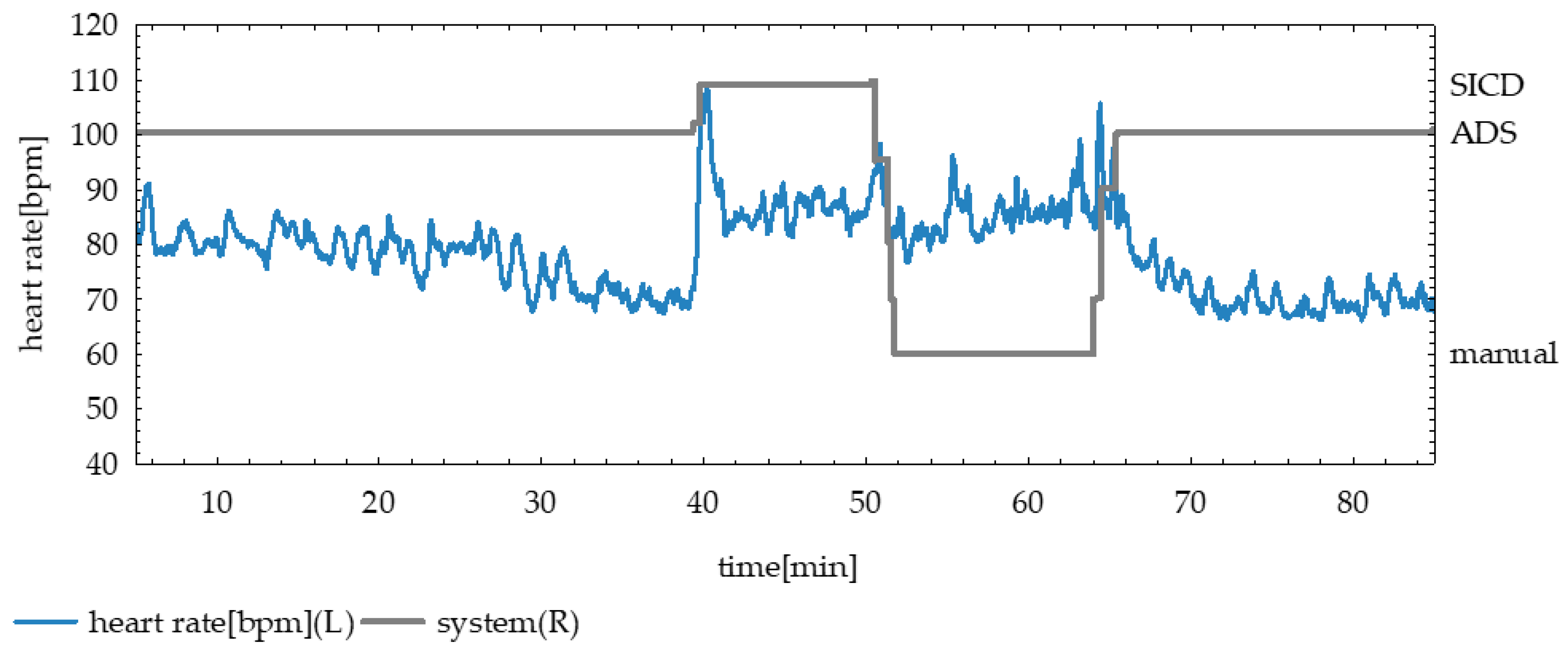
3.2. Physiological Activation
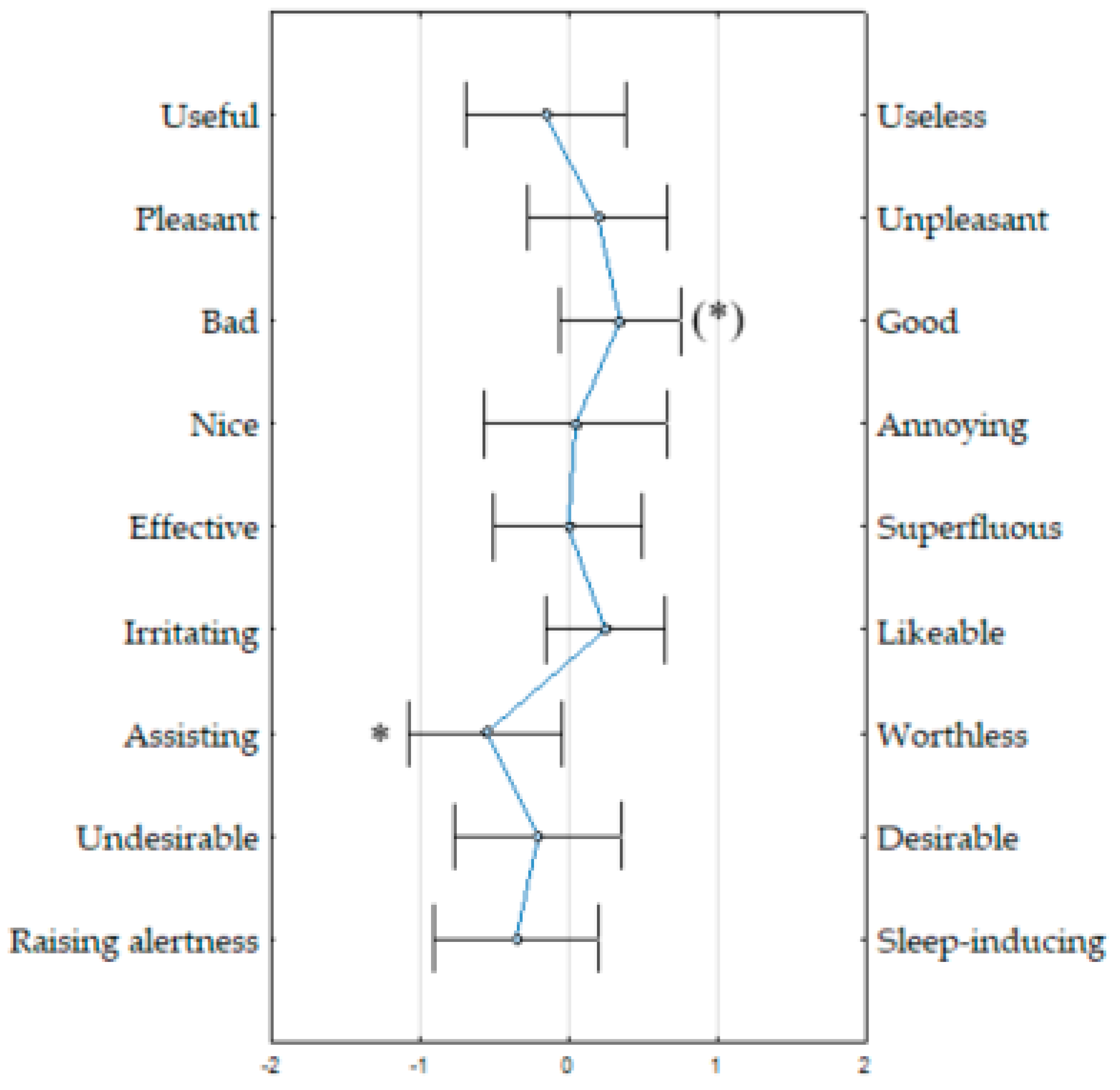
3.3. Subjective Evaluation of the SICD
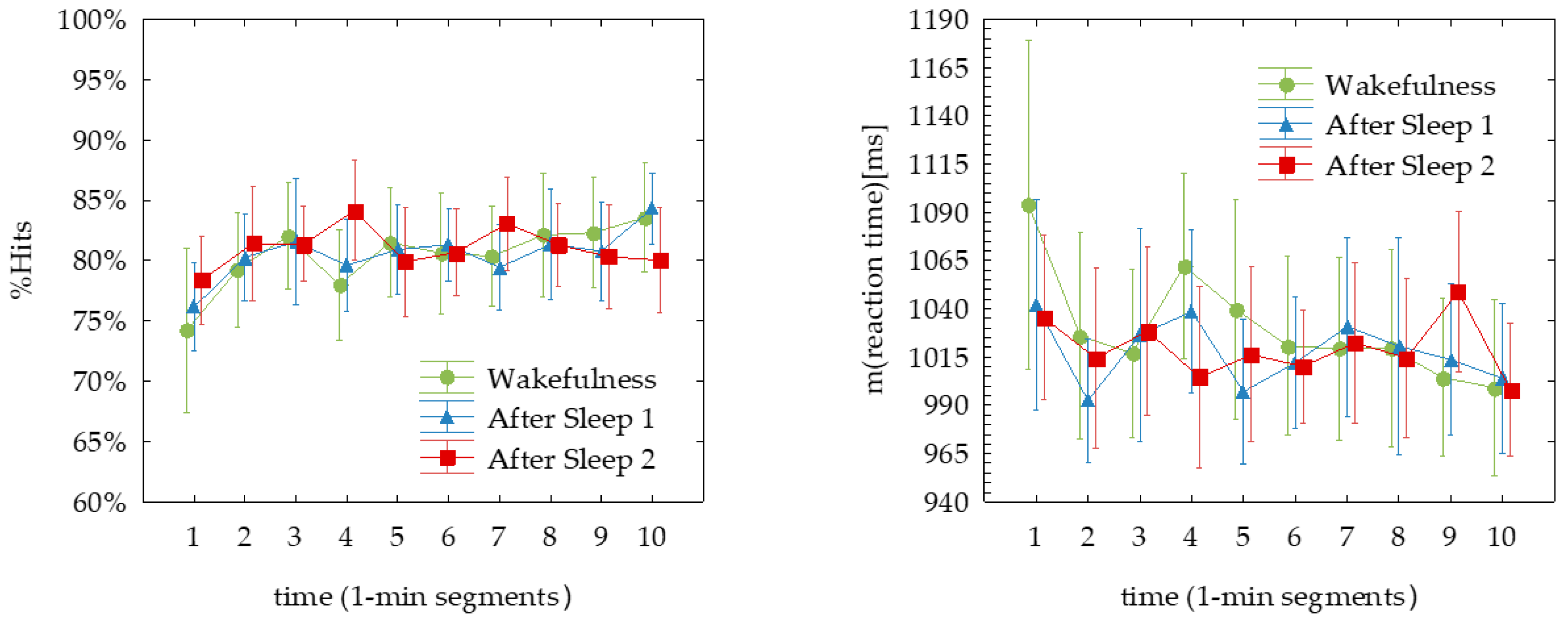
3.4. Performance on the SICD
4. Discussion
4.1. Activation of the Driver
4.2. Driver Mood and Attitude towards the SICD
4.3. Measuring Driver Alertness with the SICD
4.4. Conclusions
4.5. Limitations
4.6. Directions for Future Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Azmat, M.; Kummer, S.; Moura, L.T.; Gennaro, F.D.; Moser, R. Future Outlook of Highway Operations with Implementation of Innovative Technologies Like AV, CV, IoT and Big Data. Logistics 2019, 3, 15. [Google Scholar] [CrossRef] [Green Version]
- Kyriakidis, M.; Happee, R.; de Winter, J.C. Public opinion on automated driving: Results of an international questionnaire among 5000 respondents. Transp. Res. Part F Traffic Psychol. Behav. 2015, 32, 127–140. [Google Scholar] [CrossRef]
- Becker, T.; Herrmann, F.; Duwe, D.; Stegmüller, S.; Röckle, F.; Niko, U. Enabling the Value of Time; Fraunhofer Institute for Industrial Engineering IAO: Stuttgart, Germany, 2018; pp. 1–27. [Google Scholar]
- Upender, R.P. Sleep Medicine, Public Policy, and Public Health. In Principles and Practices of Sleep Medicine; Kryger, M., Roth, T., Eds.; Elsevier: Philadelphia, PA, USA, 2017; Volume 6, pp. 638–645. [Google Scholar]
- SAE. Taxonomy and Definitions for Terms Related to Driving Automation Systems for On-Road Motor Vehicles; SAE: Warrendale, PA, USA, 2018; Volume J3016. [Google Scholar]
- Ferrara, M.; De Gennaro, L. The sleep inertia phenomenon during the sleep-wake transition: Theoretical and operational issues. Aviat. SpaceEnviron. Med. 2000, 71, 843–848. [Google Scholar]
- Rosekind, M.R.; Smith, R.M.; Miller, D.L.; Co, E.L.; Gregory, K.B.; Webbon, L.L.; Gander, P.H.; Lebacqz, J.V. Alertness management: Strategic naps in operational settings. J. Sleep Res. 1995, 4, 62–66. [Google Scholar] [CrossRef]
- EASA. Commission Regulation (EU) 965/2012 on air operations. Amendment 16. In Acceptable Means of Compliance (AMC) and Guidance Material (GM) to Annex IV: Commercial Air Transport Operations [Part-CAT]; EASA: Cologne, Germany, 2019. [Google Scholar]
- CASA. Safety Behaviours. In Human Factors Resource Guide for Engineers; Civil Aviation Safety Authority: Canberra, Australia, 2013. [Google Scholar]
- Wörle, J.; Metz, B.; Othersen, I.; Baumann, M. Sleep in Highly Automated Driving: Take-over Performance after Waking Up. Accid. Anal. Prev. 2020, 144. [Google Scholar] [CrossRef]
- Wörle, J.; Metz, B.; Baumann, M. Investigating sleep inertia in automated driving: Methodological considerations and results from a driving simulator study. Accid. Anal. Prev. 2020. Under review. [Google Scholar]
- EuroNCAP. Euro NCAP 2025 Roadmap; EuroNCAP: Leuven, Belgium, 2017; pp. 1–17. [Google Scholar]
- Tassi, P.; Muzet, A. Sleep inertia. Sleep Med. Rev. 2000, 4, 341–353. [Google Scholar] [CrossRef]
- Carskadon, M.A.; Dement, W.C. Normal human sleep: An overview. In Principles and Practice of Sleep Medicine, 6th ed.; Kryger, M., Roth, T., Eds.; Elsevier: Philadelphia, PA, USA, 2017; Volume 4, pp. 15–24. [Google Scholar]
- AASM. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Darien, IL, USA, 2017. [Google Scholar]
- Balkin, T.J.; Braun, A.R.; Wesensten, N.J.; Jeffries, K.; Varga, M.; Baldwin, P.; Belenky, G.; Herscovitch, P. The process of awakening: A PET study of regional brain activity patterns mediating the re-establishment of alertness and consciousness. Brain 2002, 125, 2308–2319. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, M.; Curcio, G.; Fratello, F.; Moroni, F.; Marzano, C.; Pellicciari, M.C.; De Gennaro, L. The electroencephalographic substratum of the awakening. Behav. Brain Res. 2006, 167, 237–244. [Google Scholar] [CrossRef]
- Marzano, C.; Ferrara, M.; Moroni, F.; De Gennaro, L. Electroencephalographic sleep inertia of the awakening brain. Neuroscience 2011, 176, 308–317. [Google Scholar] [CrossRef]
- Hilditch, C.J.; McHill, A.W. Sleep inertia: Current insights. Nat. Sci. Sleep 2019, 11, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dongen, H.P.; Price, N.J.; Mullington, J.M.; Szuba, M.P.; Kapoor, S.C.; Dinges, D.F. Caffeine eliminates psychomotor vigilance deficits from sleep inertia. Sleep 2001, 24, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Scheer, F.A.; Shea, T.J.; Hilton, M.F.; Shea, S.A. An endogenous circadian rhythm in sleep inertia results in greatest cognitive impairment upon awakening during the biological night. J. Biol. Rhythm. 2008, 23, 353–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilditch, C.J.; Centofanti, S.A.; Dorrian, J.; Banks, S. A 30-minute, but not a 10-minute nighttime nap is associated with sleep inertia. Sleep 2016, 39, 675–685. [Google Scholar] [CrossRef] [Green Version]
- Groeger, J.A.; Lo, J.C.; Burns, C.G.; Dijk, D.-J. Effects of sleep inertia after daytime naps vary with executive load and time of day. Behav. Neurosci. 2011, 125, 252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHill, A.W.; Hull, J.T.; Cohen, D.A.; Wang, W.; Czeisler, C.A.; Klerman, E.B. Chronic sleep restriction greatly magnifies performance decrements immediately after awakening. Sleep 2019, 42, zsz032. [Google Scholar] [CrossRef]
- Dinges, D.F.; Orne, M.T.; Orne, E.C. Assessing performance upon abrupt awakening from naps during quasi-continuous operations. Behav. Res. MethodsInstrum. Comput. 1985, 17, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.J.; Duffy, J.F. Sleep inertia varies with circadian phase and sleep stage in older adults. Behav. Neurosci. 2008, 122, 928. [Google Scholar] [CrossRef]
- Bruck, D.; Pisani, D.L. The effects of sleep inertia on decision-making performance. J. Sleep Res. 1999, 8, 95–103. [Google Scholar] [CrossRef]
- Cavallero, C.; Versace, F. Stage at awakening, sleep inertia and performance. Sleep Res. Online 2003, 5, 89–97. [Google Scholar]
- Hayashi, M.; Motoyoshi, N.; Hori, T. Recuperative power of a short daytime nap with or without stage 2 sleep. Sleep 2005, 28, 829–836. [Google Scholar]
- Signal, T.L.; Gander, P.; van den Berg, M.; O’Keeffe, K. Magnitude and Time Course of Sleep Inertia; Sleep/Wake Research Center: Wellington, New Zealand, 2008. [Google Scholar]
- Hilditch, C.J.; Dorrian, J.; Banks, S. Time to wake up: Reactive countermeasures to sleep inertia. Ind. Health 2016, 54, 528–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solon, O. Who’s driving? Autonomous cars may be entering the most dangerous phase. Guardian 2018, 9, 2019. [Google Scholar]
- Guarino, B. Man Appears to Snooze at the Wheel of His Tesla while the Car Drives Itself on L.A. Highway; The Washington Post: Washington, DC, USA, 2016. [Google Scholar]
- Oh, K.T.; Shin, J.; Kim, J.; Ko, M. Analysis of a Wake-Up Task-Based Mobile Alarm App. Appl. Sci. 2020, 10, 3993. [Google Scholar] [CrossRef]
- Bradley, M.M.; Lang, P.J. Measuring emotion: The self-assessment manikin and the semantic differential. J. Behav. Ther. Exp. Psychiatry 1994, 25, 49–59. [Google Scholar] [CrossRef]
- Jasper, H. Report of the committee on methods of clinical examination in electroencephalography. Electroencephalogr. Clin. Neurophysiol. 1958, 10, 370–375. [Google Scholar]
- Gabehart, R.J.; van Dongen, H.P. Circadian Rhythms in Sleepiness, Alertness, and Performance. In Principles and Practice of Sleep Medicine; Kryger, M.H., Roth, T., Eds.; Elsevier: Philadelphia, PA, USA, 2017; Volume 5, pp. 388–394. [Google Scholar]
- Van Der Laan, J.D.; Heino, A.; De Waard, D. A simple procedure for the assessment of acceptance of advanced transport telematics. Transp. Res. Part C Emerg. Technol. 1997, 5, 1–10. [Google Scholar] [CrossRef]
- Kovac, K.; Ferguson, S.A.; Paterson, J.L.; Aisbett, B.; Hilditch, C.J.; Reynolds, A.C.; Vincent, G.E. Exercising caution upon waking–can exercise reduce sleep inertia? Front. Physiol. 2020, 11, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wörle, J.; Kenntner-Mabiala, R.; Metz, B.; Fritzsch, S.; Purucker, C.; Befelein, D.; Prill, A. Sleep Inertia Countermeasures in Automated Driving: A Concept of Cognitive Stimulation. Information 2020, 11, 342. https://0-doi-org.brum.beds.ac.uk/10.3390/info11070342
Wörle J, Kenntner-Mabiala R, Metz B, Fritzsch S, Purucker C, Befelein D, Prill A. Sleep Inertia Countermeasures in Automated Driving: A Concept of Cognitive Stimulation. Information. 2020; 11(7):342. https://0-doi-org.brum.beds.ac.uk/10.3390/info11070342
Chicago/Turabian StyleWörle, Johanna, Ramona Kenntner-Mabiala, Barbara Metz, Samantha Fritzsch, Christian Purucker, Dennis Befelein, and Andy Prill. 2020. "Sleep Inertia Countermeasures in Automated Driving: A Concept of Cognitive Stimulation" Information 11, no. 7: 342. https://0-doi-org.brum.beds.ac.uk/10.3390/info11070342