Real-Time Location Systems for Asset Management in Nursing Homes: An Explorative Study of Ethical Aspects

 ,
,  ,
,
Abstract
:1. Introduction
2. Theoretical Framework
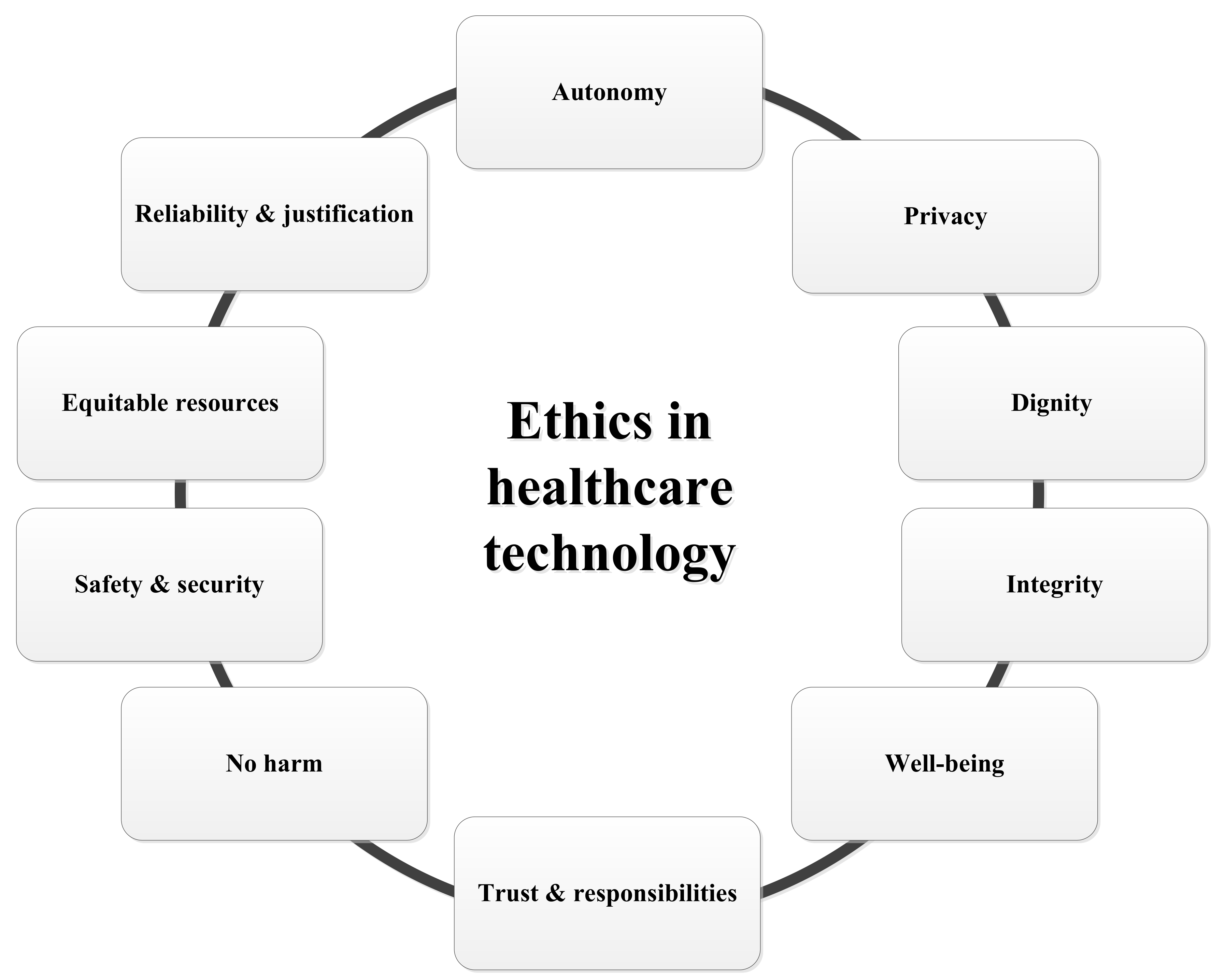
2.1. Ethics: An Overview of Principles
2.2. General Ethical Principles in Care
2.2.1. Autonomy
2.2.2. No Harm to the Client and Well-Being
2.2.3. The Equitable Distribution of Resources
2.3. Triple or Quadruple Aim of Care
2.4. Ethical Issues Related to Healthcare Technology
2.4.1. Privacy, Dignity and Integrity
2.4.2. Trust and Responsibilities
2.4.3. Security and Safety
2.5. The Ethics of Monitoring Technologies
2.6. Different Perspectives
3. Methodology
3.1. Focus Groups
3.2. Participants and Procedure
3.3. Data Analysis
4. Results
4.1. Insights Concerning Benefits and Disadvantages, Changing Roles And Behaviours
“It is matter of simply asking the system where [it] is, and you will easily find it!”[REL2]
“I think their attitude towards the residents would never change, with or without the use of a new system.”[REL1]
“I don’t want to access the system. It is probably too complicated for me to learn, but it may save me money and stress.”[REL4]
“I do spend quite a lot of time calling colleagues to ask where items have gone.”[CP3]
“Without or without the use of technology, my top priority will also be the resident.”[CP2]
“Data on the use of items may help me improve my services to nursing homes.”[SME5]
“Some nurses may develop sloppy routines, as they might think that technology will compensate for that.”[SME6]
4.2. Sense of Responsibility
“They are our parents, and they have always taken care of us. Now they need us.”[REL1]
“I don’t want to have any responsibility; it is part of the work flow of the nursing home organisation.”[REL4]
“Well, I do think it matters. I mean, of course you’ll start searching, and you want to get it back, and you will call your colleagues, but once you have searched for two hours without success, then that’s it. They’d better arrange an area where people have to return the devices to.”[CP1]
“Some of the assistive devices are very expensive, and you don’t want to lose them. It is not like it should be done the proper way.”[CP4]
“What the care professional eventually does with [the RTLS], is his or her own concern.”[SME2]
“We cannot be held accountable for the use of technology in hospitals and nursing homes. We just have to make sure the design and installation is done correctly.”[SME4]
4.3. Impact of RTLS on the Perception Of Space
“Out of sight, out of mind. The system is not like a set of cameras producing clear images.”[REL1]
“Why would I change my work place if the items I use are being tracked by a system that logs data?”[CP2]
“People do not know that their stuff is connected to a system. Maybe, they have never given permission.”[CP4]
4.4. Impact of RTLS on the Sense of Safety and Security
“People won’t notice that assistive devices are being monitored. But companies should not have access to data, and no-one should be able to hack the system.”[REL1]
“I am already way too busy taking care of things. I don’t want any additional tasks.”[REL3]
“Technology is nice to have. But it needs to be up for discussion and evaluation by all people who use it.”[CP1]
“We are here to safeguard the interests of our residents, also when it comes to the use of technology.”[CP3]
“Efficiency, privacy, better healthcare services… the discussion should be held in an integrated manner. I don’t know who is going to make the final decision on what is best.”[RES2]
4.5. Results in Brief
5. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Van Hoof, J.; Douven, B.; Janssen, B.M.; Bosems, W.P.H.; Oude Weernink, C.E.; Vossen, M.B. Losing items in the psychogeriatric nursing home: The perspective of residents and their informal caregivers. Gerontol. Geriatr. Med. 2016, 2. [Google Scholar] [CrossRef] [PubMed]
- Oude Weernink, C.E.; van Hoof, J.; Felix, E.; Verkuijlen, P.J.E.M.; Dierick-van Daele, A.T.M.; Kazak, J.K. Real-time location systems in nursing homes: State of the art and future applications. J. Enabling Technol. 2018, 12. [Google Scholar]
- Oude Weernink, C.E.; Sweegers, L.; Relou, L.; van der Zijpp, T.J.; van Hoof, J. Lost and found: Identifying problems and technological opportunities related to lost and misplaced items in nursing homes through participatory design research. Technol. Disabil. 2017, 29, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Krohn, R. The optimal RTLS solution for hospitals. Breaking through a complex environment. J. Healthc. Inf. Manag. 2008, 22, 14–15. [Google Scholar] [PubMed]
- Malik, A. RTLS for Dummies; Wiley Publishing: Hoboken, NJ, USA, 2009. [Google Scholar]
- Kamel Boulos, M.N.; Berry, G. Real-time locating systems (RTLS) in healthcare: A condensed primer. Int. J. Health Geogr. 2012, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.A.; Monahan, T. Evaluation of real-time location systems in their hospital contexts. Int. J. Med. Inform. 2012, 81, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Ebbers, C.W.J.M.; van Hoof, J.; Oude Weernink, C.E. Privacyaspecten van track-en-tracetechnologie in de zorg. Priv. Inf. 2017, 20, 24–32. (In Dutch) [Google Scholar]
- Ebbers, C.W.J.M.; van Hoof, J.; Oude Weernink, C.E. De toepassing van track-en-tracetechnologie in de zorg (2). Priv. Inf. 2017, 20, 256–263. (In Dutch) [Google Scholar]
- Leikas, J.; Kulju, M. Ethical consideration of home monitoring technology: A qualitative focus group study. Gerontechnology 2018, 17, 38–47. [Google Scholar] [CrossRef]
- McShane, R.; Hope, T.; Wilkinson, J. Tracking patients who wander: Ethics and technology. Lancet 1994, 343, 1274. [Google Scholar] [CrossRef]
- Bjørneby, S.; Topo, P.; Holthe, T. (Eds.) Technology, Ethics and Dementia: A Guidebook on How to Apply Technology in Dementia Care; Norwegian Centre for Dementia Research: Oslo, Norway, 1999. [Google Scholar]
- Hughes, J.C.; Louw, S.J. Electronic tagging of people with dementia who wander. Br. Med. J. 2002, 325, 847–848. [Google Scholar] [CrossRef]
- Mittelstadt, B. Ethics of the health-related internet of things: A narrative review. Ethics Inf. Technol. 2017, 19, 157–175. [Google Scholar] [CrossRef]
- Mittelstadt, B. Designing the health-related internet of things: Ethical principles and guidelines. Information 2017, 8, 77. [Google Scholar] [CrossRef]
- Lie, M.; Brittain, K. Technology and trust: Older people’s perspectives of a home monitoring system [Technologie et confiance: Le point de vue des personnes âgées sur un système de télésurveillance à domicile]. Retraite Soc. 2016, 75, 47–72. (In French) [Google Scholar]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 6th ed.; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- McClelland, M. Ethics: Harm in the emergency department—Ethical drivers for change. Online J. Issues Nurs. 2015, 20. [Google Scholar] [CrossRef]
- Levinson, W. Time for leadership in teaching about care of chronic illness. J. Gen. Intern. Med. 2010, 25, 570–571. [Google Scholar] [CrossRef] [PubMed]
- Rietveld, P.; Hensher, D.A.; Button, K.J. Winners and losers in Transport Policy: On Efficiency, Equity, and Compensation. In Handbook of Transport and the Environment; Hensher, D.A., Button, K.J., Eds.; Elsevier: Amsterdam, The Netherlands, 2003; pp. 585–602. [Google Scholar]
- Van Zaalen-op’t Hof, Y.; McDonnell-Naughton, M.; Mikołajczyk, B.; Buttigieg, S.C.; del Carmen Requena, M.; Holtkamp, F.C. Technology implementation in delivery of healthcare to older people: How can the least voiced in society be heard? J. Enabling Technol. 2018, 12. [Google Scholar]
- UN General Assembly. Thematic Study on the Realization of the Right to Health of Older Persons by the Special Rapporteur on the Right of Everyone to the Enjoyment of the Highest Attainable Standard of Physical and Mental Health, Anand Grover; UN General Assembly: New York, NY, USA, 2011. [Google Scholar]
- Bodenheimer, T.; Sinsky, C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Gaertner, J.; Vent, J.; Greinwald, R.; Rothschild, M.A.; Ostgathe, C.; Kessel, R.; Voltz, R. Denying a patient’s final will: Public safety vs. medical confidentiality and patient autonomy. J. Pain Symptom Manag. 2011, 42, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Van den Hoven, J. Moral values, design and ICT. J. Hum. 2005, 23, 52–58. [Google Scholar]
- Miller, C.M.; Gruskin, S.; Subramanian, S.V.; Heymann, J. Emerging health disparities in Botswana: Examining the situation of orphans during the AIDS epidemic. Soc. Sci. Med. 2007, 64, 2476–2486. [Google Scholar] [CrossRef] [PubMed]
- Musschenga, B.; Schuijer, M.E.; Verstegen, G.; Vonk, M.; Dorrestijn, S.; Kalis, A. Praktische problemen in filosofisch perspectief. Filos. Prakt. 2016, 37, 48–56. (In Dutch) [Google Scholar]
- Van Hoof, J.; Kort, H.S.M.; Markopoulos, P.; Soede, M. Ambient intelligence, ethics, and privacy. Gerontechnology 2007, 6, 155–163. [Google Scholar] [CrossRef]
- Niemeijer, A.R.; Depla, M.F.; Frederiks, B.J.; Hertogh, C.M. The experiences of people with dementia and intellectual disabilities with surveillance technologies in residential care. Nurs. Ethics 2015, 22, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Marshall, M. Technology is the shape of the future. J. Dement. Care 1995, 3, 12–14. [Google Scholar]
- van Berlo, A. Ethics in domotics. Gerontechnology 2005, 3, 170. [Google Scholar] [CrossRef]
- Hertogh, C.M.P.M.; Wouters, E.J.M. Ethische aspecten bij het gebruik van toezichthoudende domotica. In Het Verpleeghuis van de Toekomst is (een) Thuis; van Hoof, J., Wouters, E.J.M., Eds.; Bohn Stafleu van Loghum: Houten, The Netherlands, 2014; pp. 73–74. (In Dutch) [Google Scholar]
- Verkerk, M. (Over)behandelen van kwetsbare ouderen. Een ethische benadering. Bijblijven 2016, 32, 180–188. [Google Scholar] [CrossRef]
- Ten Have, H.A.M.J.; ter Meulen, R.H.J.; van Leeuwen, E. Medische Ethiek, 3rd ed.; Bohn Stafleu van Loghum: Houten, The Netherlands, 2009. (In Dutch) [Google Scholar]
- Van Hoof, J.; Dooremalen, A.M.C.; Wetzels, M.H.; Weffers, H.T.G.; Wouters, E.J.M. Exploring technological and architectural solutions for nursing home residents, care professionals and technical staff: Focus groups with professional stakeholders. Int. J. Innov. Res. Sci. Technol. 2014, 1, 90–105. [Google Scholar]
- Kitzinger, J. Qualitative research: Introducing focus groups. Br. Med. J. 1995, 311, 299–302. [Google Scholar] [CrossRef]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Morgan, D.L. Focus Groups as Qualitative Research, 2nd ed.; Sage: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects; Adopted by the 18th WMA General Assembly, Helsinki, Finland, 1964 and Last Amended by the 59th WMA General Assembly, Seoul, Korea, 1975; World Medical Association: Ferney-Voltaire, France, 2008. [Google Scholar]
- Van Hoof, J.; Wouters, E.J.M. Zorgdomotica; Bohn Stafleu van Loghum: Houten, The Netherlands, 2012. (In Dutch) [Google Scholar]
- Timmer, S. Ehealth in de Langdurige Zorg. De Praktijk van de Ouderen-en Gehandicaptenzorg, 2nd ed.; Bohn Stafleu van Loghum: Houten, The Netherlands, 2015. (In Dutch) [Google Scholar]
- Kazak, J.; van Hoof, J.; Świąder, M.; Szewrański, S. Real Estate for the Ageing Society—The Perspective of a New Market. Real Estate Manag. Valuat. 2017, 25, 13–24. [Google Scholar] [CrossRef]
- Boerenfijn, P.; Kazak, J.K.; Schellen, L.; van Hoof, J. A multi-case study of innovations in energy performance of social housing for older adults in the Netherlands. Energy Build. 2018, 158, 1762–1769. [Google Scholar] [CrossRef]
- Wiersinga, J. Chapter 13 Regulation of Medical Digital Technologies. In Mobile e-Health, Human–Computer Interaction Series; Marston, H.R., Freeman, S., Musslewhite, C., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 277–295. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Participants | |
|---|---|
| Group 1 | Six care professionals working in a nursing home for older people with a psychogeriatric background. Only female participants. |
| Group 2 | Four informal carers (one male) and two female residents. |
| Group 3 | Seven representatives of SMEs (4 males) and six researchers (3 females). |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Hoof, J.; Verboor, J.; Oude Weernink, C.E.; Sponselee, A.A.G.; Sturm, J.A.; Kazak, J.K.; Govers, G.M.J.; Van Zaalen, Y. Real-Time Location Systems for Asset Management in Nursing Homes: An Explorative Study of Ethical Aspects. Information 2018, 9, 80. https://0-doi-org.brum.beds.ac.uk/10.3390/info9040080
Van Hoof J, Verboor J, Oude Weernink CE, Sponselee AAG, Sturm JA, Kazak JK, Govers GMJ, Van Zaalen Y. Real-Time Location Systems for Asset Management in Nursing Homes: An Explorative Study of Ethical Aspects. Information. 2018; 9(4):80. https://0-doi-org.brum.beds.ac.uk/10.3390/info9040080
Chicago/Turabian StyleVan Hoof, J., J. Verboor, C.E. Oude Weernink, A.A.G. Sponselee, J.A. Sturm, J.K. Kazak, G.M.J. Govers, and Y. Van Zaalen. 2018. "Real-Time Location Systems for Asset Management in Nursing Homes: An Explorative Study of Ethical Aspects" Information 9, no. 4: 80. https://0-doi-org.brum.beds.ac.uk/10.3390/info9040080