
Biological Variation in Rotational Thromboelastometry in Patients with Atrial Fibrillation Receiving Rivaroxaban


Abstract
:1. Introduction
2. Patients and Methods
Statistical Analysis
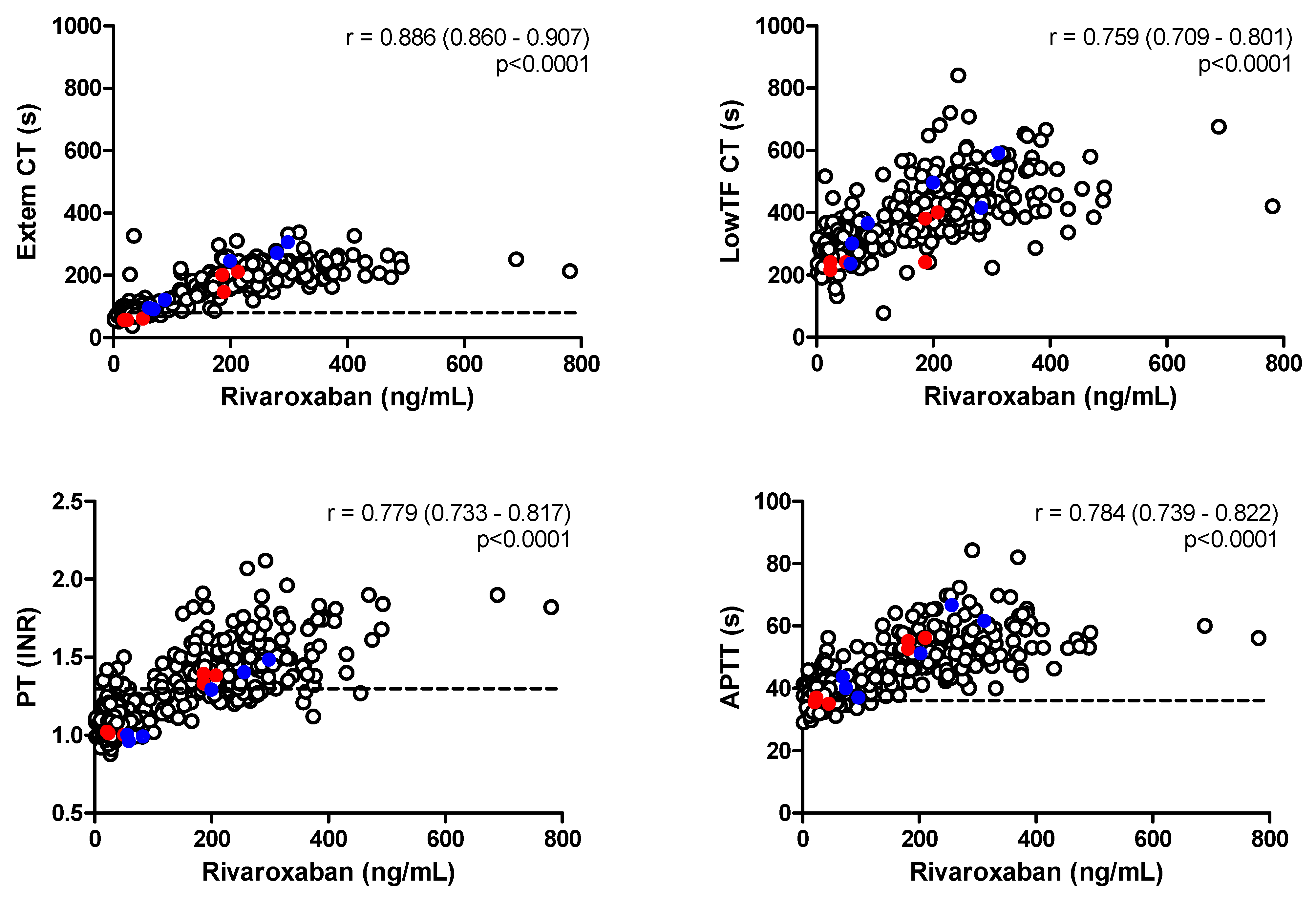
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wikkelsø, A.; Wetterslev, J.; Møller, A.M.; Afshari, A. Thromboelastography (TEG) or rotational thromboelastometry (ROTEM) to monitor haemostatic treatment in bleeding patients: A systematic review with meta-analysis and trial sequential analysis. Anaesthesia 2017, 72, 519–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korpallová, B.; Samoš, M.; Bolek, T.; Kühnelová, L.; Škorňová, I.; Kubisz, P.; Staško, J.; Mokáň, M. ROTEM Testing for Direct Oral Anticoagulants. Semin. Thromb. Hemost. 2021, 47, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Mijovski, M.B. Advances in monitoring anticoagulant therapy. Adv. Clin. Chem. 2019, 90, 197–213. [Google Scholar] [CrossRef]
- Cuker, A.; Siegal, D. Monitoring and reversal of direct oral anticoagulants. Hematol. Am. Soc. Hematol. Educ. Program. 2015, 2015, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Eller, T.; Busse, J.; Dittrich, M.; Flieder, T.; Alban, S.; Knabbe, C.; Birschmann, I. Dabigatran, rivaroxaban, apixaban, argatroban and fondaparinux and their effects on coagulation POC and platelet function tests. Clin. Chem. Lab. Med. 2014, 52, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Seyve, L.; Richarme, C.; Polack, B.; Marlu, R. Impact of four direct oral anticoagulants on rotational thromboelastometry (ROTEM). Int. J. Lab. Hematol. 2017, 40, 84–93. [Google Scholar] [CrossRef]
- Casutt, M.; Konrad, C.; Schuepfer, G. Effect of rivaroxaban on blood coagulation using the viscoelastic coagulation test ROTEM™. Anaesthesist 2012, 61, 948–953. [Google Scholar] [CrossRef]
- Fontana, P.; Alberio, L.; Angelillo-Scherrer, A.; Asmis, L.M.; Korte, W.; Mendez, A.; Schmid, P.; Stricker, H.; Studt, J.-D.; Tsakiris, D.A.; et al. Impact of rivaroxaban on point-of-care assays. Thromb. Res. 2017, 153, 65–70. [Google Scholar] [CrossRef]
- Chojnowski, K.; Górski, T.; Robak, M.; Treliński, J. Effects of Rivaroxaban Therapy on ROTEM Coagulation Parameters in Patients with Venous Thromboembolism. Adv. Clin. Exp. Med. 2015, 24, 995–1000. [Google Scholar] [CrossRef]
- Pailleret, C.; Jourdi, G.; Siguret, V.; Gouin-Thibault, I.; Gandrille, S.; Stepanian, A.; Curis, E.; Golmard, J.L.; Gaussem, P.; Le Bonniec, B.; et al. Modified ROTEM for the detection of rivaroxaban and apixaban anticoagulant activity in whole blood: A diagnostic test study. Eur. J. Anaesthesiol. 2019, 36, 449–456. [Google Scholar] [CrossRef]
- Tsantes, A.E.; Kyriakou, E.; Ikonomidis, I.; Katogiannis, K.; Papadakis, I.; Douramani, P.; Kopterides, P.; Kapsimali, V.; Lekakis, J.; Tsangaris, I.; et al. Comparative Assessment of the Anticoagulant Activity of Rivaroxaban and Dabigatran in Patients with Nonvalvular Atrial Fibrillation: A Noninterventional Study. Medicine 2016, 95, e3037. [Google Scholar] [CrossRef] [PubMed]
- Vedovati, M.C.; Mosconi, M.G.; Isidori, F.; Agnelli, G.; Becattini, C. Global thromboelastometry in patients receiving direct oral anticoagulants: The RO-DOA study. J. Thromb. Thrombolysis 2020, 49, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Klages, M.; Raimann, F.J.; Philipp, A.-L.; Lindhoff-Last, E.; Zacharowski, K.; Mutlak, H. Direct oral anticoagulants in point-of-care monitoring: An ex-vivo study. Minerva Anestesiol. 2021, 87, 514–522. [Google Scholar] [CrossRef]
- Adelmann, D.; Wiegele, M.; Wohlgemuth, R.K.; Koch, S.; Frantal, S.; Quehenberger, P.; Scharbert, G.; Kozek-Langenecker, S.; Schaden, E. Measuring the activity of apixaban and rivaroxaban with rotational thrombelastometry. Thromb. Res. 2014, 134, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Schafer, S.T.; Otto, A.C.; Acevedo, A.C.; Gorlinger, K.; Massberg, S.; Kammerer, T.; Groene, P. Point-of-care detection and differentiation of anticoagulant therapy—Development of thromboelastometry-guided decision-making support algorithms. Thromb. J. 2021, 19, 63. [Google Scholar] [CrossRef]
- Schäfer, S.T.; Wiederkehr, T.; Kammerer, T.; Acevedo, A.-C.; Feil, K.; Kellert, L.; Görlinger, K.; Hinske, L.C.; Groene, P. Real-time detection and differentiation of direct oral anticoagulants (rivaroxaban and dabigatran) using modified thromboelastometric reagents. Thromb. Res. 2020, 190, 103–111. [Google Scholar] [CrossRef]
- Available online: https://biologicalvariation.eu (accessed on 27 May 2022).
- Miklič, M.; Mavri, A.; Vene, N.; Söderblom, L.; Božič-Mijovski, M.; Pohanka, A.; Antovic, J.; Malmström, R.E. Intra- and inter- individual rivaroxaban concentrations and potential bleeding risk in patients with atrial fibrillation. Eur. J. Clin. Pharmacol. 2019, 75, 1069–1075. [Google Scholar] [CrossRef]
- Al-Aieshy, F.; Malmström, R.E.; Antovic, J.; Pohanka, A.; Rönquist-Nii, Y.; Berndtsson, M.; Al-Khalili, F.; Skeppholm, M. Clinical evaluation of laboratory methods to monitor exposure of rivaroxaban at trough and peak in patients with atrial fibrillation. Eur. J. Clin. Pharmacol. 2016, 72, 671–679. [Google Scholar] [CrossRef]
- Røraas, T.; Støve, B.; Petersen, P.H.; Sandberg, S. Biological Variation: The Effect of Different Distributions on Estimated Within-Person Variation and Reference Change Values. Clin. Chem. 2016, 62, 725–736. [Google Scholar] [CrossRef] [Green Version]
- Bardy, G.; Fischer, F.; Appert, A.; Baldin, B.; Stève, M.; Spreux, A.; Lavrut, T.; Drici, M.-D. Is anti-factor Xa chromogenic assay for Rivaroxaban appropriate in clinical practice? Advantages and comparative drawbacks. Thromb. Res. 2015, 136, 396–401. [Google Scholar] [CrossRef]
- Bento Matos Derogis, P.; Rentas Sanches, L.; De Aranda, V.F.; Colombini, M.P.; Mangueira, C.; Katz, M.; Caschera Leme Faulhaber, A.; Mendes, C.E.A.; Ferreira, C.E.D.S.; França, C.N.; et al. Determination of rivaroxaban in patient’s plasma samples by anti-Xa chromogenic test associated to High Performance Liquid Chromatography tandem Mass Spectrometry (HPLC-MS/MS). PLoS ONE 2017, 12, e0171272. [Google Scholar] [CrossRef]
- Cini, M.; Legnani, C.; Padrini, R.; Cosmi, B.; Dellanoce, C.; De Rosa, G.; Marcucci, R.; Pengo, V.; Poli, D.; Testa, S.; et al. DOAC plasma levels measured by chromogenic anti-Xa assays and HPLC-UV in apixaban- and rivaroxaban-treated patients from the START-Register. Int. J. Lab. Hematol. 2020, 42, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Baglin, T.; Hillarp, A.; Tripodi, A.; Elalamy, I.; Buller, H.; Ageno, W. Measuring Oral Direct Inhibitors (ODIs) of thrombin and factor Xa: A recommendation from the Subcommittee on Control of Anticoagulation of the Scientific and Standardisation Committee of the International Society on Thrombosis and Haemostasis. J. Thromb. Haemost. 2013, 11, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Jilma-Stohlawetz, P.; Fritsche-Polanz, S.; Quehenberger, P.; Schoergenhofer, C.; Bartko, J.; Ristl, R.; Jilma, B. Evaluation of between-, within- and day-to-day variation of coagulation measured by rotational thrombelastometry (ROTEM). Scand. J. Clin. Lab. Investig. 2017, 77, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Falay, M.; Senes, M.; Korkmaz, S.; Turhan, T.; Okay, M.; Öztürk, B.A.; Yücel, D.; Ozet, G. Biological variation estimates of prothrombin time, activated partial thromboplastin time, and fibrinogen in 28 healthy individuals. Int. J. Lab. Hematol. 2018, 40, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Henskens, Y.M.C.; Gulpen, A.J.W.; Van Oerle, R.; Wetzels, R.; Verhezen, P.; Spronk, H.; Schalla, S.; Crijns, H.J.; Cate, H.T.; Cate-Hoek, A.T. Detecting clinically relevant rivaroxaban or dabigatran levels by routine coagulation tests or thromboelastography in a cohort of patients with atrial fibrillation. Thromb. J. 2018, 16, 3. [Google Scholar] [CrossRef]


{kind=link}
| R20 | R15 | p | |
|---|---|---|---|
| Age (years) | 71 ± 6 | 76 ± 6 | <0.01 |
| Sex (women/men) | 9/21 | 19/11 | 0.02 |
| Body weight (kg) | 90 ± 17 | 79 ± 16 | 0.01 |
| Creatinine (μmol/L) | 76 ± 14 | 98 ± 20 | <0.001 |
| CrCl (mL/min) | 99 ± 32 | 60 ± 26 | <0.001 |
| Arterial hypertension (N, %) | 26 (87) | 28 (93) | NS |
| Diabetes mellitus (N, %) | 4 (13) | 9 (30) | NS |
| Heart failure (N, %) | 6 (20) | 8 (27) | NS |
| Ischemic heart disease (N, %) | 6 (20) | 6 (20) | NS |
| Previous stroke or systemic embolism (N, %) | 3 (10) | 5 (17) | NS |
| Peripheral artery disease (N, %) | 1 (3) | 1 (3) | NS |
| CHADS2 score | 1.8 ± 1.3 | 2.5 ± 1.2 | 0.01 |
| HAS-BLED score | 0.9 ± 0.7 | 1.2 ± 0.5 | 0.02 |
| Measurand | Trough 1 | Trough 2 | Trough 3 | Peak 1 | Peak 2 | Peak 3 |
|---|---|---|---|---|---|---|
| Rivaroxaban (ng/mL) | 34 (19–52) | 33 (16–50) | 36 (24–50) | 244 (193–308) | 240 (190–286) | 244 (188–312) |
| ROTEM Extem | ||||||
| CT (s) | 85 (74–95) | 81 (73–93) | 83 (73–97) | 205 (176–232) | 189 (166–220) | 202 (179–242) |
| CFT (s) | 69 (58–80) | 72 (60–83) | 68 (58–81) | 73 (67–89) | 77 (70–88) | 74 (66–81) |
| MCF (mm) | 66 (64–70) | 66 (62–70) | 66 (63–69) | 66 (63–69) | 65 (63–68) | 65 (62–68) |
| ROTEM LowTF | ||||||
| CT (s) | 276 (253–311) | 262 (239–286) | 290 (260–319) | 452 (399–526) | 404 (363–465) | 448 (410–539) |
| CFT (s) | 101 (89–118) | 95 (86–121) | 99 (89–118) | 139 (113–164) | 128 (113–157) | 134 (119–168) |
| MCF (mm) | 63 (61–67) | 63 (61–67) | 63 (60–66) | 62 (58–65) | 62 (58–65) | 61 (57–64) |
| PT (INR) | 1.1 (1.0–1.1) | 1.1 (1.0–1.1) | 1.1 (1.0–1.1) | 1.5 (1.3–1.6) | 1.4 (1.3–1.6) | 1.4 (1.3–1.6) |
| APTT (s) | 38.1 (34.8–40.7) | 37.7 (35.2–40.5) | 37.6 (35.3–39.8) | 52.4 (46.9–59.0) | 51.5 (47.0–58.7) | 51.5 (46.9–55.9) |
| Anti-Xa (ng/mL) | 32 (19–46) | 29 (17–44) | 31 (19–44) | 237 (208–358) | 240 (220–317) | 243 (217–348) |
| Measurand | CVI Trough (%) | CVI Peak (%) | CVG Trough (%) | CVG Peak (%) |
|---|---|---|---|---|
| Rivaroxaban (ng/mL) | 35.4 | 19.9 | 80.0 | 37.1 |
| ROTEM Extem | ||||
| CT (s) | 12.7 | 11.8 | 23.8 | 21.2 |
| CFT (s) | 10.7 | 13.2 | 22.3 | 18.7 |
| MCF (mm) | 2.5 | 3.1 | 6.5 | 6.3 |
| ROTEM LowTF | ||||
| CT (s) | 13.2 | 19.0 | 17.8 | 24.5 |
| CFT (s) | 16.5 | 23.0 | 25.0 | 29.7 |
| MCF (mm) | 3.1 | 4.9 | 7.3 | 9.3 |
| PT (INR) | 2.3 | 5.8 | 8.9 | 15.2 |
| APTT (s) | 4.2 | 5.6 | 11.2 | 14.1 |
| Anti-Xa (ng/mL) | 34.7 | 16.7 | 86.7 | 35.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Božič Mijovski, M.; Antovic, J.P.; Malmström, R.E.; Mavri, A. Biological Variation in Rotational Thromboelastometry in Patients with Atrial Fibrillation Receiving Rivaroxaban. J. Cardiovasc. Dev. Dis. 2022, 9, 205. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070205
Božič Mijovski M, Antovic JP, Malmström RE, Mavri A. Biological Variation in Rotational Thromboelastometry in Patients with Atrial Fibrillation Receiving Rivaroxaban. Journal of Cardiovascular Development and Disease. 2022; 9(7):205. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070205
Chicago/Turabian StyleBožič Mijovski, Mojca, Jovan P. Antovic, Rickard E. Malmström, and Alenka Mavri. 2022. "Biological Variation in Rotational Thromboelastometry in Patients with Atrial Fibrillation Receiving Rivaroxaban" Journal of Cardiovascular Development and Disease 9, no. 7: 205. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070205