
Sex Differences in Frequency of Instrumental Activities of Daily Living after Cardiac Rehabilitation and Its Impact on Outcomes in Patients with Heart Failure
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. IADL Measurement
2.4. Outcomes
2.5. Statistical Analyses
3. Results
3.1. Study Population
3.2. Differences in the Distribution of Total FAI Scores and Each of the Component Items between the Sexes
3.3. Cut-Off Values of FAI Score for All-Cause Mortality and Differences in Characteristics between the Groups
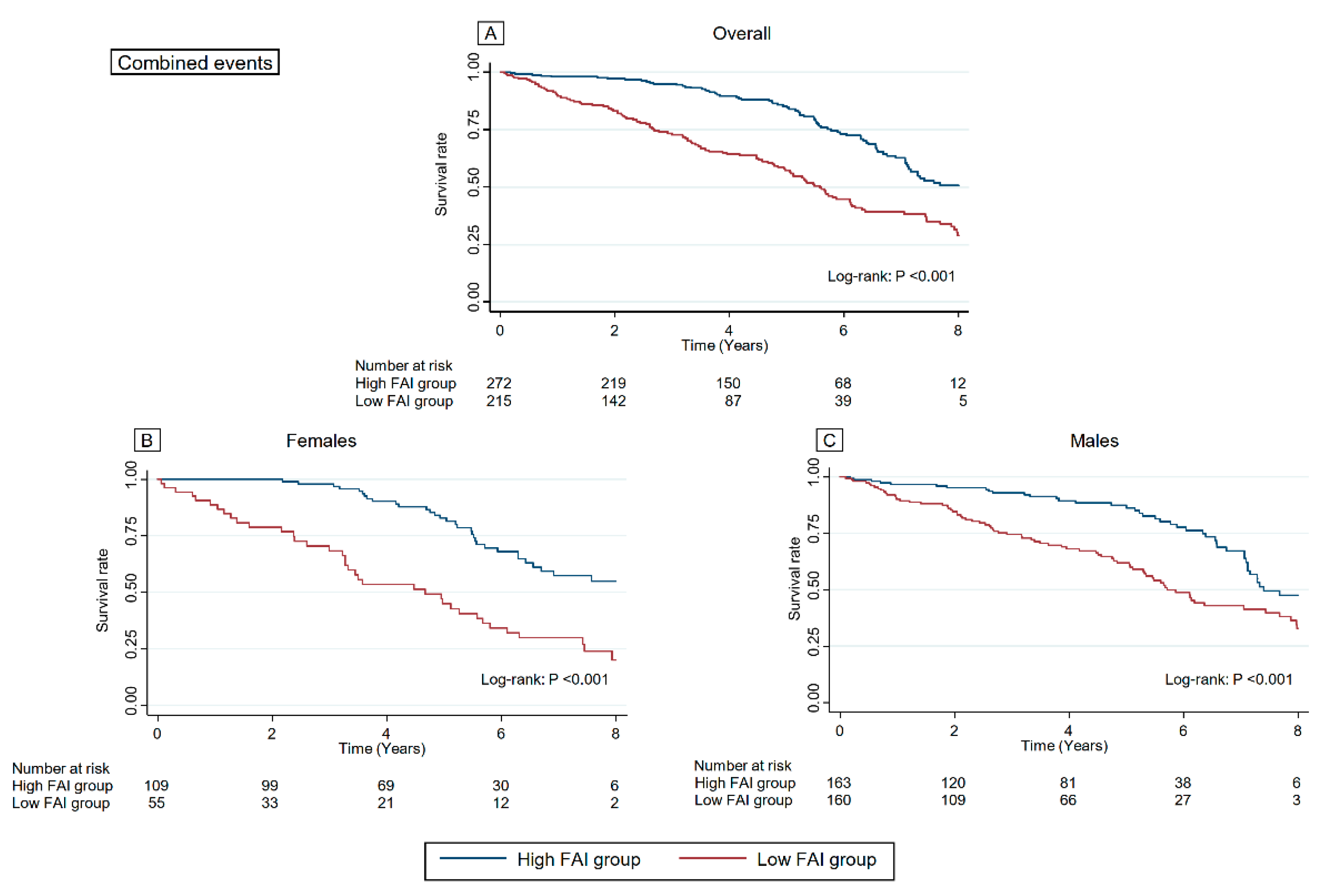
3.4. Association between FAI Score and Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; et al. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, Y.; Kohsaka, S.; Sato, N.; Takano, T.; Kitai, T.; Yoshikawa, T.; Matsue, Y. 9-Year Trend in the Management of Acute Heart Failure in Japan: A Report From the National Consortium of Acute Heart Failure Registries. J. Am. Heart Assoc. 2018, 7, e008687. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Sato, Y.; Takahashi, T.; Tsuchihashi-Makaya, M.; Kotooka, N.; Ikegame, T.; Takura, T.; Yamamoto, T.; Nagayama, M.; Goto, Y.; et al. Multidisciplinary Cardiac Rehabilitation and Long-Term Prognosis in Patients With Heart Failure. Circ. Heart Fail. 2020, 13, e006798. [Google Scholar] [CrossRef]
- Long, L.; Mordi, I.R.; Bridges, C.; Sagar, V.A.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; Taylor, R.S. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst. Rev. 2019, 1, CD003331. [Google Scholar] [CrossRef]
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat. Rev. Cardiol. 2022, 19, 180–194. [Google Scholar] [CrossRef]
- Kato, M.; Mori, Y.; Watanabe, D.; Onoda, H.; Fujiyama, K.; Toda, M.; Kito, K. Relationship between average daily rehabilitation time and decline in instrumental activity of daily living among older patients with heart failure: A preliminary analysis of a multicenter cohort study, SURUGA-CARE. PLoS ONE 2021, 16, e0254128. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Storeng, S.H.; Sund, E.R.; Krokstad, S. Factors associated with basic and instrumental activities of daily living in elderly participants of a population-based survey: The Nord-Trondelag Health Study, Norway. BMJ Open 2018, 8, e018942. [Google Scholar] [CrossRef]
- Bowling, C.B.; Fonarow, G.C.; Patel, K.; Zhang, Y.; Feller, M.A.; Sui, X.; Blair, S.N.; Alagiakrishnan, K.; Aban, I.B.; Love, T.E.; et al. Impairment of activities of daily living and incident heart failure in community-dwelling older adults. Eur. J. Heart Fail. 2012, 14, 581–587. [Google Scholar] [CrossRef]
- Ferreira, T.C.; Coimbra, A.M.; Falsarella, G.R.; Costallat, L.T.; Coimbra, I.B. Mortality in Brazilian community-dwelling older adults: 7 years of follow up in primary care. Geriatr. Gerontol. Int. 2016, 16, 804–809. [Google Scholar] [CrossRef]
- Lo, A.X.; Donnelly, J.P.; McGwin, G., Jr.; Bittner, V.; Ahmed, A.; Brown, C.J. Impact of gait speed and instrumental activities of daily living on all-cause mortality in adults ≥65 years with heart failure. Am. J. Cardiol. 2015, 115, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, C.M.; Oliveira, C.; Firmo, J.O.A.; Lima-Costa, M.F.; Peixoto, S.V. Prognostic value of disability on mortality: 15-year follow-up of the Bambui cohort study of aging. Arch. Gerontol. Geriatr. 2018, 74, 112–117. [Google Scholar] [CrossRef] [PubMed]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The natural history of congestive heart failure: The Framingham study. N. Engl. J. Med. 1971, 285, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Izawa, H.; Yoshida, T.; Ikegame, T.; Izawa, K.P.; Ito, Y.; Okamura, H.; Osada, N.; Kinugawa, S.; Kubozono, T.; Kono, Y.; et al. Standard Cardiac Rehabilitation Program for Heart Failure. Circ. J. 2019, 83, 2394–2398. [Google Scholar] [CrossRef] [PubMed]
- Sone, S. [Ethical Guidelines for Clinical Trials in Medical Research Involving Human Subjects]. Gan Kagaku Ryoho 2015, 42, 893–902. [Google Scholar]
- Ando, Y.; Ito, S.; Uemura, O.; Kato, T.; Kimura, G.; Nakao, T.; Hattori, M.; Fukagawa, M.; Horio, M.; Mitarai, T.; et al. CKD Clinical Practice Guidebook. The essence of treatment for CKD patients. Clin. Exp. Nephrol. 2009, 13, 191–248. [Google Scholar] [CrossRef]
- Holbrook, M.; Skilbeck, C.E. An activities index for use with stroke patients. Age Ageing 1983, 12, 166–170. [Google Scholar] [CrossRef]
- Barnard, J.; Rubin, D.B. Small-Sample Degrees of Freedom with Multiple Imputation. Biometrika 1999, 86, 948–955. [Google Scholar] [CrossRef]
- Boyde, M.; Peters, R.; New, N.; Hwang, R.; Ha, T.; Korczyk, D. Self-care educational intervention to reduce hospitalisations in heart failure: A randomised controlled trial. Eur. J. Cardiovasc. Nurs. 2018, 17, 178–185. [Google Scholar] [CrossRef]
- Desai, A.S.; Stevenson, L.W. Rehospitalization for heart failure: Predict or prevent? Circulation 2012, 126, 501–506. [Google Scholar] [CrossRef]
- Hamazaki, N.; Kamiya, K.; Nozaki, K.; Yamashita, M.; Uchida, S.; Noda, T.; Maekawa, E.; Meguro, K.; Yamaoka-Tojo, M.; Matsunaga, A.; et al. Correlation between respiratory muscle weakness and frailty status as risk markers for poor outcomes in patients with cardiovascular disease. Eur. J. Cardiovasc. Nurs. 2022, in press. [CrossRef]
- Son, Y.J.; Shim, D.K.; Seo, E.K.; Won, M.H. Gender differences in the impact of frailty on 90-day hospital readmission in heart failure patients: A retrospective cohort study. Eur. J. Cardiovasc. Nurs. 2021, 20, 485–492. [Google Scholar] [CrossRef]
- Fukui, S.; Kawakami, M.; Otaka, Y.; Ishikawa, A.; Yashima, F.; Hayashida, K.; Oguma, Y.; Fukuda, K.; Liu, M. Preoperative Instrumental Activities of Daily Living Predicts Survival After Transcatheter Aortic Valve Implantation. Circ. Rep. 2020, 2, 83–88. [Google Scholar] [CrossRef]
- Hu, Z.; Zheng, B.; Kaminga, A.C.; Zhou, F.; Xu, H. Association Between Functional Limitations and Incident Cardiovascular Diseases and All-Cause Mortality Among the Middle-Aged and Older Adults in China: A Population-Based Prospective Cohort Study. Front. Public Health 2022, 10, 751985. [Google Scholar] [CrossRef] [PubMed]
- Matsuzawa, R.; Kamitani, T.; Roshanravan, B.; Fukuma, S.; Joki, N.; Fukagawa, M. Decline in the Functional Status and Mortality in Patients on Hemodialysis: Results from the Japan Dialysis Outcome and Practice Patterns Study. J. Ren. Nutr. 2019, 29, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Omura, T.; Tamura, Y.; Sakurai, T.; Umegaki, H.; Iimuro, S.; Ohashi, Y.; Ito, H.; Araki, A.; Japanese Elderly Diabetes Intervention Trial Research Group. Functional categories based on cognition and activities of daily living predict all-cause mortality in older adults with diabetes mellitus: The Japanese Elderly Diabetes Intervention Trial. Geriatr. Gerontol. Int. 2021, 21, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Goto, C.; Higashi, Y.; Kimura, M.; Noma, K.; Hara, K.; Nakagawa, K.; Kawamura, M.; Chayama, K.; Yoshizumi, M.; Nara, I. Effect of different intensities of exercise on endothelium-dependent vasodilation in humans: Role of endothelium-dependent nitric oxide and oxidative stress. Circulation 2003, 108, 530–535. [Google Scholar] [CrossRef]
- Hegde, S.M.; Goncalves, A.; Claggett, B.; Evenson, K.R.; Cheng, S.; Shah, A.M.; Folsom, A.R.; Solomon, S.D. Cardiac structure and function and leisure-time physical activity in the elderly: The Atherosclerosis Risk in Communities Study. Eur. Heart J. 2016, 37, 2544–2551. [Google Scholar] [CrossRef]
- Judge, J.O.; Schechtman, K.; Cress, E. The relationship between physical performance measures and independence in instrumental activities of daily living. The FICSIT Group. Frailty and Injury: Cooperative Studies of Intervention Trials. J. Am. Geriatr. Soc. 1996, 44, 1332–1341. [Google Scholar] [CrossRef]
- Nourhashemi, F.; Andrieu, S.; Gillette-Guyonnet, S.; Vellas, B.; Albarede, J.L.; Grandjean, H. Instrumental activities of daily living as a potential marker of frailty: A study of 7364 community-dwelling elderly women (the EPIDOS study). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M448–M453. [Google Scholar] [CrossRef]
- Teo, N.; Gao, Q.; Nyunt, M.S.Z.; Wee, S.L.; Ng, T.P. Social Frailty and Functional Disability: Findings From the Singapore Longitudinal Ageing Studies. J. Am. Med. Dir. Assoc. 2017, 18, 637.e13–637.e19. [Google Scholar] [CrossRef] [PubMed]
- Matsue, Y.; Kamiya, K.; Saito, H.; Saito, K.; Ogasahara, Y.; Maekawa, E.; Konishi, M.; Kitai, T.; Iwata, K.; Jujo, K.; et al. Prevalence and prognostic impact of the coexistence of multiple frailty domains in elderly patients with heart failure: The FRAGILE-HF cohort study. Eur. J. Heart Fail. 2020, 22, 2112–2119. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Yamashita, M.; Saito, H.; Kamiya, K.; Maeda, D.; Konishi, M.; Matsue, Y. Correction to: Multidomain Frailty in Heart Failure: Current Status and Future Perspectives. Curr. Heart Fail. Rep. 2021, 18, 121. [Google Scholar] [CrossRef]
- Kulzer, A.M.; Scolari, C.C.; Gus, M. Relationship between usual physical, cognitive and social activities and functional recovery at hospital discharge after acute stroke. J. Rehabil. Med. 2008, 40, 195–199. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Belohlavek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Petrie, M.C.; Verma, S.; Docherty, K.F.; Inzucchi, S.E.; Anand, I.; Belohlavek, J.; Bohm, M.; Chiang, C.E.; Chopra, V.K.; de Boer, R.A.; et al. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA 2020, 323, 1353–1368. [Google Scholar] [CrossRef]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.F.; de Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef]
- Kamiya, K.; Yamamoto, T.; Tsuchihashi-Makaya, M.; Ikegame, T.; Takahashi, T.; Sato, Y.; Kotooka, N.; Saito, Y.; Tsutsui, H.; Miyata, H.; et al. Nationwide Survey of Multidisciplinary Care and Cardiac Rehabilitation for Patients With Heart Failure in Japan- An Analysis of the AMED-CHF Study. Circ. J. 2019, 83, 1546–1552. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Missing Data | Overall (N = 490) | High FAI Score (N = 274) | Low FAI Score (N = 216) | p Value | |
|---|---|---|---|---|---|
| Age, years | 0 | 69 (58–76) | 67 (54–74) | 72 (63–78) | <0.001 |
| Female, n (%) | 0 | 166 (33.9) | 110 (40.1) | 56 (25.9) | 0.001 |
| BMI, kg/m2 | 0 | 21.9 (19.5–24.2) | 22.3 (19.7–25.3) | 21.4 (19.3–23.7) | 0.007 |
| Etiology of HF, n (%) | 0 | ||||
| Ischemic | 175 (35.7) | 94 (34.3) | 81 (37.5) | 0.102 | |
| Hypertension | 122 (24.9) | 76 (27.8) | 46 (21.3) | ||
| Valvular | 69 (14.1) | 41 (15.0) | 28 (13.0) | ||
| Others | 124 (25.3) | 63 (23.0) | 61 (28.2) | ||
| NYHA functional class, n (%) | 0 | <0.001 | |||
| Ⅰ/Ⅱ | 345 (490) | 225 (82.1) | 120 (55.6) | ||
| Ⅲ/Ⅳ | 145 (29.6) | 49 (17.9) | 96 (44.4) | ||
| LVEF, % | 27 | 48 (33–59) | 50 (35–61) | 47 (31–58) | 0.129 |
| LVEF <40, n (%) | 173 (35.3) | 90 (32.8) | 83 (38.4) | 0.293 | |
| LVEF ≥50, n (%) | 223 (45.5) | 129 (47.1) | 94 (43.5) | 0.366 | |
| Comorbidities, n (%) | |||||
| Hypertension | 0 | 308 (62.9) | 159 (58.0) | 149 (69.0) | 0.013 |
| Diabetes mellitus | 0 | 171 (34.9) | 78 (28.5) | 93 (43.0) | 0.001 |
| Dyslipidemia | 0 | 240 (49.0) | 128 (46.7) | 112 (51.9) | 0.259 |
| Atrial fibrillation | 0 | 68 (13.9) | 38 (13.9) | 30 (13.9) | 0.992 |
| Ischemic etiology | 0 | 203 (41.4) | 100 (36.5) | 103 (47.7) | 0.013 |
| Prior HF admission, n (%) | 0 | 243 (50.0) | 126 (46.0) | 117 (54.2) | 0.072 |
| Current smoker, n (%) | 0 | 87 (17.8) | 45 (16.4) | 42 (19.4) | 0.336 |
| Laboratory data | |||||
| Hemoglobin, g/dL | 1 | 12.3 (10.8–14.0) | 12.6 (11.1–14.0) | 12.1 (10.4–14.1) | 0.068 |
| Albumin, g/dL | 1 | 3.8 (3.4–4.0) | 3.8 (3.4–4.1) | 3.7 (3.4–4.0) | 0.036 |
| Creatinine, mg/dL | 1 | 0.98 (0.80–1.34) | 0.92 (0.77–1.24) | 1.07 (0.86–1.55) | <0.001 |
| eGFR, mL/min/1.73 m2 | 1 | 54.6 (37.7–69.6) | 57.7 (43.3–72.6) | 50.3 (28.1–65.6) | <0.001 |
| Sodium, mEq/mL | 1 | 139 (136–140) | 139 (136–141) | 138 (136–140) | 0.184 |
| BNP, pg/mL | 34 | 219 (104–463) | 191 (94–369) | 278 (126–684) | <0.001 |
| Medications, n (%) | |||||
| ACEI/ARB | 0 | 418 (85.3) | 237 (86.5) | 181 (66.1) | 0.402 |
| β blocker | 0 | 376 (76.7) | 218 (79.6) | 158 (73.1) | 0.095 |
| MRA | 0 | 220 (44.9) | 118 (43.1) | 102 (47.2) | 0.358 |
| Diuretics | 0 | 409 (83.5) | 224 (81.8) | 185 (85.6) | 0.100 |
| AHEAD score | 0 | 2 (1–3) | 1 (1–2) | 2 (1–3) | <0.001 |
| FAI | 0 | 24 (16–29) | 29 (26–32) | 15 (10–19) | <0.001 |
| Outcomes | No. of Events/Cases | Event Rate per 100 Persons-Years | HR (95% CI) | p Value |
|---|---|---|---|---|
| All-cause mortality (Per 1 point increase) | 95/490 (19.4%) | 4.2 | 0.961 (0.937–0.986) | 0.002 |
| High FAI score | 28/274 (10.2%) | 1.0 | 1 (Reference) | |
| Low FAI score | 67/216 (31.0%) | 6.5 | 2.69 (1.64–4.44) | <0.001 |
| Combined events (Per 1 point increase) | 213/490 (43.5%) | 9.1 | 0.968 (0.952–0.985) | <0.001 |
| High FAI score | 89/274 (32.5%) | 6.8 | 1 (Reference) | |
| Low FAI score | 114/216 (52.8%) | 11.0 | 1.552 (1.054–2.353) | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nozaki, K.; Hamazaki, N.; Kamiya, K.; Kariya, H.; Uchida, S.; Noda, T.; Ueno, K.; Maekawa, E.; Matsunaga, A.; Yamaoka-Tojo, M.; et al. Sex Differences in Frequency of Instrumental Activities of Daily Living after Cardiac Rehabilitation and Its Impact on Outcomes in Patients with Heart Failure. J. Cardiovasc. Dev. Dis. 2022, 9, 289. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9090289
Nozaki K, Hamazaki N, Kamiya K, Kariya H, Uchida S, Noda T, Ueno K, Maekawa E, Matsunaga A, Yamaoka-Tojo M, et al. Sex Differences in Frequency of Instrumental Activities of Daily Living after Cardiac Rehabilitation and Its Impact on Outcomes in Patients with Heart Failure. Journal of Cardiovascular Development and Disease. 2022; 9(9):289. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9090289
Chicago/Turabian StyleNozaki, Kohei, Nobuaki Hamazaki, Kentaro Kamiya, Hidenori Kariya, Shota Uchida, Takumi Noda, Kensuke Ueno, Emi Maekawa, Atsuhiko Matsunaga, Minako Yamaoka-Tojo, and et al. 2022. "Sex Differences in Frequency of Instrumental Activities of Daily Living after Cardiac Rehabilitation and Its Impact on Outcomes in Patients with Heart Failure" Journal of Cardiovascular Development and Disease 9, no. 9: 289. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9090289