Development of p-Coumaric Acid Analysis in Human Plasma and Its Clinical Application to PK/PD Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Analysis of p-Coumaric Acid and Pharmacokinetic Application
2.1.1. Chemicals and Reagents
2.1.2. Preparation of Standards
2.1.3. Sample Preparation
2.1.4. UPLC-MS/MS Conditions
2.1.5. Pharmacokinetic Assay
2.2. Pilot Study with p-Coumaric Acid for Pharmacodynamic Application Study Population
Randomization and Experimental Procedure
2.3. Statistical Analysis
3. Results
3.1. Analysis of p-Coumaric Acid
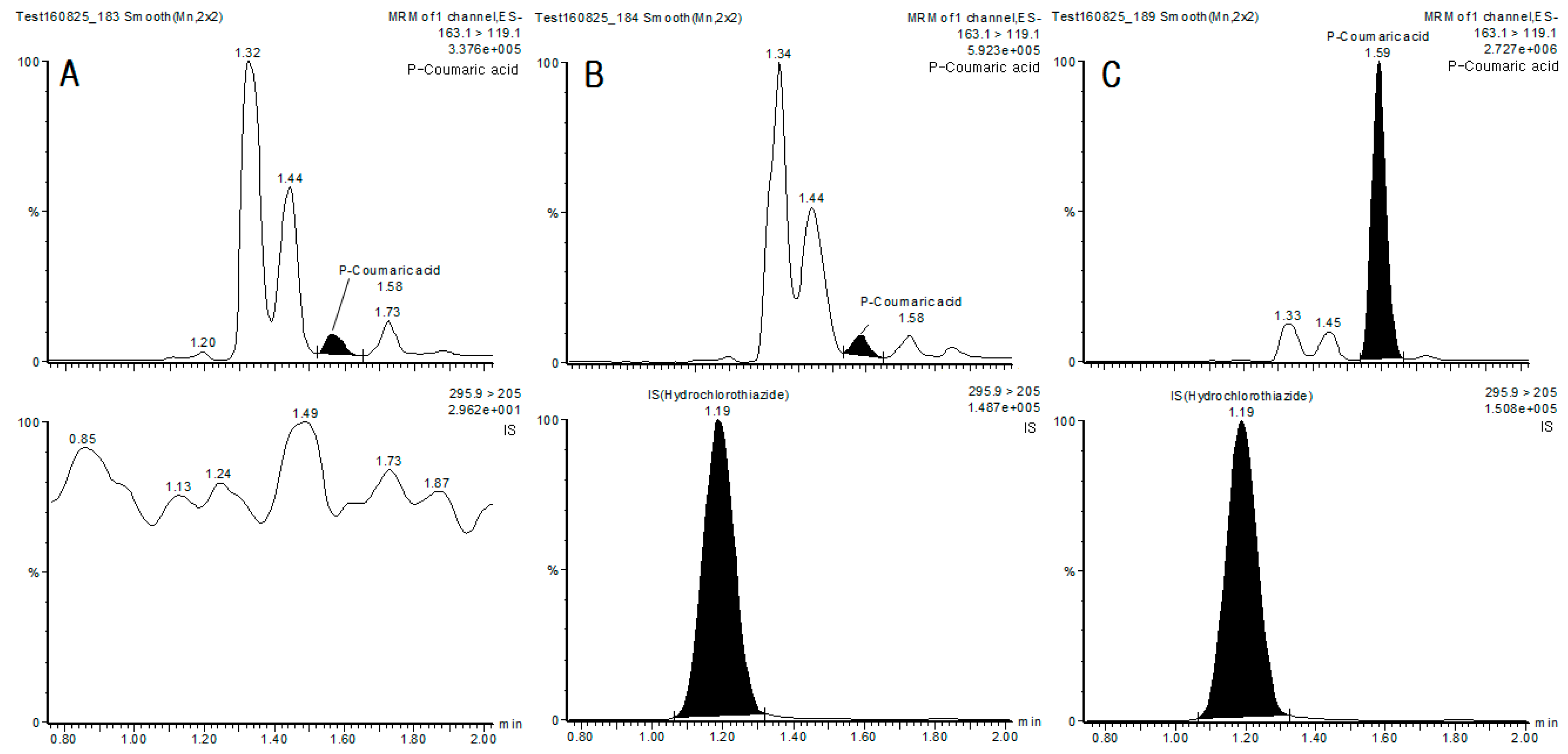
3.1.1. Specificity
3.1.2. Matrix Effect and Recovery
3.1.3. Accuracy and Precision
3.1.4. Sensitivity and Calibration Curve
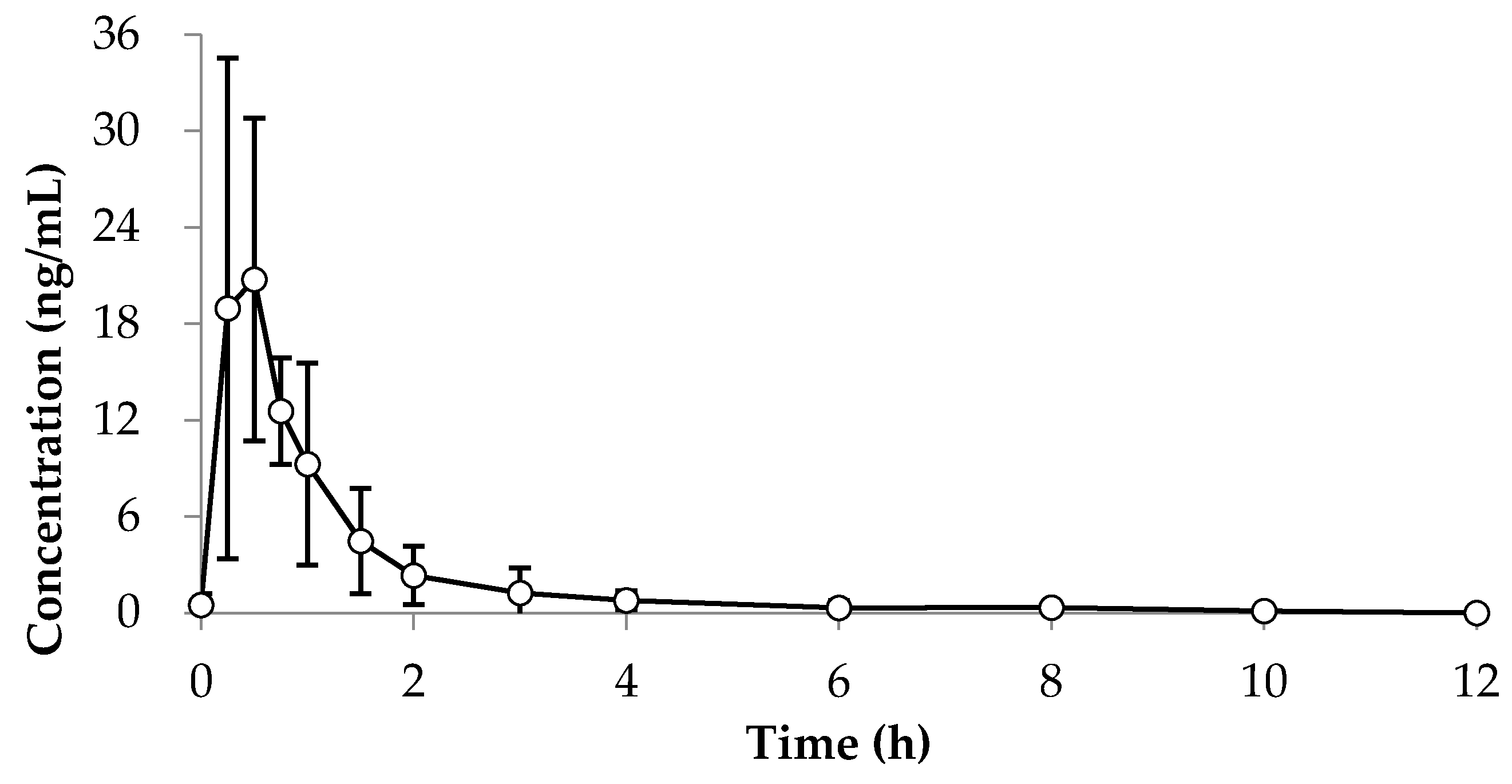
3.1.5. Pharmacokinetic Application
3.2. Pilot Study of Bambusae Caulis in Taeniam
3.3. Sample Size Calculation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chung, Y.H.; Lee, D.Y.; Lee, H.S.; Hong, S.A.; Park, E.S.; Nam, Y.; Kim, H.C.; Lee, S.J.; Sohn, U.D.; Kim, H.; et al. Effects of Aqueous Extract of Phyllostachyos Caulis in Taeniam on Longitudinal Bone Growth in Adolescent Rats. Planta Med. 2016, 82, 330–336. [Google Scholar] [CrossRef] [PubMed]
- McArthur, R.G. Growth retardation: An approach to management. Can. Fam. Phys. 1985, 31, 1039. [Google Scholar]
- Isgaard, J.; Carlsson, L.; Isaksson, O.G.; Jansson, J.O. Pulsatile intravenous growth hormone (GH) infusion to hypophysectomized rats increases insulin-like growth factor I messenger ribonucleic acid in skeletal tissues more effectively than continuous GH infusion. Endocrinology 1988, 123, 2605–2610. [Google Scholar] [CrossRef] [PubMed]
- Bryant, J.; Baxter, L.; Cave, C.B.; Milne, R. Recombinant growth hormone for idiopathic short stature in children and adolescents. Cochrane Database Syst. Rev. 2007, 3, CD004440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, A.; Im, M.; Yim, N.H.; Jung, Y.P.; Ma, J.Y. Aqueous extract of Bambusae Caulis in Taeniam inhibits PMA-induced tumor cell invasion and pulmonary metastasis: Suppression of NF-kB activation through ROS signaling. PLoS ONE 2013, 8, e78061. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Lim, D.; Kim, J. p-Coumaric acid, A Major Active Compound of Bambusae Caulis in Taeniam, Suppresses Cigarette Smoke-Induced Pulmonary Inflammation. Am. J. Chin. Med. 2018, 46, 407–421. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Zhang, Y.; Lou, D.; Wu, X.; Zhang, Y. Antihyperlipidemic and antihypertensive effect of a triterpenoid-rich extract from bamboo shavings and vasodilator effect of friedelin on phenylephrine-induced vasoconstriction in thoracic aortas of rats. Phytother. Res. 2007, 21, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.H.; Lee, J.M.; Lee, H.J.; Kim, C.Y.; Lee, E.H.; Um, B.H. Aldose reductase and advanced glycation endproducts inhibitory effect of Phyllostachys nigra. Biol. Pharm. Bull. 2007, 30, 1569–1572. [Google Scholar] [CrossRef] [Green Version]
- Rafiee, Z.; Moaiedi, M.Z.; Gorji, A.V.; Mansouri, E. p-Coumaric Acid Mitigates Doxorubicin-Induced Nephrotoxicity through Suppression of Oxidative Stress, Inflammation and Apoptosis. Arch. Med. Res. 2020, 51, 32–40. [Google Scholar] [CrossRef]
- Guven, M.; Aras, A.B.; Akman, T.; Sen, H.M.; Ozkan, A.; Salis, O.; Sehitoglu, I.; Kalkan, Y.; Silan, C.; Deniz, M.; et al. Neuroprotective effect of p-Coumaric acid in rat model of embolic cerebral ischemia. Iran. J. Basic Med. Sci. 2015, 18, 356–363. [Google Scholar]
- Ferguson, L.R.; Lim, I.F.; Pearson, A.E.; Ralph, J.; Harris, P.J. Bacterial antimutagenesis by hydroxycinnamic acids from plant cell walls. Mutat. Res. 2003, 542, 49–58. [Google Scholar] [CrossRef]
- Ueda, T.; Ito, T.; Kurita, H.; Inden, M.; Hozumi, I. p-Coumaric acid has protective effects against mutant copper–zinc superoxide dismutase 1 via the activation of autophagy in N2a cells. Int. J. Mol. Sci. 2019, 20, 2942. [Google Scholar] [CrossRef] [Green Version]
- Barros, M.P.; Lemos, M.; Maistro, E.L.; Leite, M.F.; Sousa, J.P.B.; Bastos, J.K.; de Andrade, S.F. Evaluation of antiulcer activity of the main phenolic acids found in Brazilian Green Propolis. J. Ethnopharmacol. 2008, 120, 372–377. [Google Scholar] [CrossRef]
- Berthier, S. Handbook of Analytical Separations; Elsevier: Amsterdam, The Netherlands, 2004; pp. 113–128. [Google Scholar]
- Holly, J.M.; Wass, J.A. Insulin-like growth factors; autocrine, paracrine or endocrine? New perspectives of the somatomedin hypothesis in the light of recent developments. J. Endocrinol. 1989, 122, 611–618. [Google Scholar] [CrossRef]
- Patel, M.B.; Arden, N.K.; Masterson, L.M.; Phillips, D.I.W.; Swaminathan, R.; Syddall, H.E.; Byrne, C.D.; Wood, P.J.; Cooper, C.; Holt, R.I.G.; et al. Investigating the role of the growth hormone-insulin-like growth factor (GH-IGF) axis as a determinant of male bone mineral density (BMD). Bone 2005, 37, 833–841. [Google Scholar] [CrossRef]
- Ahmed, S.F.; Farquharson, C. The effect of GH and IGF1 on linear growth and skeletal development and their modulation by SOCS proteins. J. Endocrinol. 2010, 206, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merriman, H.L.; La Tour, D.; Linkhart, T.A.; Mohan, S.; Baylink, D.J.; Strong, D.D. Insulin-like growth factor-I and insulin-like growth factor-II induce c-fos in mouse osteoblastic cells. Calcif. Tissue Int. 1990, 46, 258–262. [Google Scholar] [CrossRef] [PubMed]
- DiGirolamo, D.J.; Mukherjee, A.; Fulzele, K.; Gan, Y.; Cao, X.; Frank, S.J.; Clemens, T.L. Mode of growth hormone action in osteoblasts. J. Biol. Chem. 2007, 282, 31666–31674. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nominal (ng/mL) | Precision CV (%) | Accuracy (%) | ||
|---|---|---|---|---|
| Intra (n = 5) | Inter (n = 3) | Intra (n = 5) | Inter (n = 3) | |
| 0.2 | 5.6 | 6.4 | 103.8 | 108.4 |
| 0.6 | 2.3 | 2.4 | 100.0 | 100.9 |
| 8 | 1.2 | 2.1 | 99.0 | 99.6 |
| 16 | 1.0 | 1.3 | 99.2 | 101.3 |
| Parameter | Unit | Value (Mean ± SD) |
|---|---|---|
| Cmax | ng/mL | 21.95 ± 11.36 |
| AUCt | ng·h/mL | 20.55 ± 1.50 |
| AUCinf | ng·h/mL | 20.82 ± 1.63 |
| AUCt/AUCinf | % | 98.7 ± 0.5 |
| Tmax | h | 0.50 ± 0.35 |
| T1/2 | h | 0.9 ± 0.5 |
| Variable | Group | p-Value | |
|---|---|---|---|
| Placebo | Treatment | ||
| All participants | 18 | 16 | |
| Sex | |||
| Male (n, %) | 13 (72.2%) | 9 (56.3%) | 0.3307 1 |
| Female (n, %) | 5 (27.8%) | 7 (43.8%) | |
| Age | |||
| Mean (SD) | 9.00 (1.37) | 7.94 (1.48) | 0.0531 2 |
| 6 | 1 (5.6%) | 3 (18.8%) | |
| 7 | 1 (5.6%) | 5 (31.3%) | |
| 8 | 5 (27.8%) | 1 (6.3%) | |
| 9 | 3 (16.7%) | 4 (25.0%) | |
| 10 | 6 (33.3%) | 3 (18.8%) | |
| 11 | 2 (11.1%) | 0 (0.0%) | |
| Variable | Value | p-Value 1 | |
|---|---|---|---|
| Placebo (n = 18) | Treatment (n = 16) | ||
| Height (cm) | 1.03 cm/3 month | 1.43 cm/3 month | |
| Screening | 126.93 ± 7.05 | 121.43 ± 7.89 | 0.0394 2 |
| Visit 1 | 127.38 ± 7.10 | 121.60 ± 7.98 | 0.0326 2 |
| Visit 2 | 127.88 ± 7.03 | 122.25 ± 8.18 | 0.0386 2 |
| Visit 3 | 128.41 ± 7.06 | 123.03 ± 7.84 | 0.0430 2 |
| Change from baseline | 1.03 ± 0.51 | 1.43 ± 0.68 | 0.0639 2 |
| IGF-1 | 0.27 | 9.57 | |
| Screening | 69.85 ± 16.36 | 64.95 ± 20.85 | 0.3496 3 |
| Visit 3 | 70.12 ± 19.94 | 74.52 ± 19.38 | 0.3162 3 |
| Change from baseline | 0.26 ± 13.69 | 9.57 ± 12.69 | 0.0488 2 |
| Osteocalcin | |||
| Screening | 66.80 ± 27.59 | 75.96 ± 30.49 | 0.3003 3 |
| Visit 3 | 58.72 ± 27.56 | 89.44 ± 19.92 | 0.0058 3 |
| Change from baseline | −8.08 ± 18.33 | 13.48 ± 25.12 | 0.0070 2 |
| Group | Group | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Placebo | Treatment | p-Value * | Variable | Placebo | Treatment | p-Value * |
| SBP | WBC | ||||||
| Screening | 100 ± 5 | 100 ± 7 | 0.4772 | Screening | 6.65 ± 1.03 | 7.41 ± 0.93 | - |
| At week 12 | 100 ± 8 | 90 ± 8 | 0.2815 | At week 12 | 6.79 ± 2.06 | 7.15 ± 2.24 | 0.4971 |
| DBP | Uric acid | ||||||
| Screening | 65 ± 7 | 60 ± 8 | 0.2652 | Screening | 3.9 ± 0.6 | 4.1 ± 1.0 | 0.3695 |
| At week 12 | 60 ± 10 | 60 ± 9 | 0.3423 | At week 12 | 4.1 ± 1.0 | 3.8 ± 0.7 | 0.1371 |
| Pulse | Na | ||||||
| Screening | 82 ± 8 | 84 ± 6 | 0.4238 | Screening | 140 ± 1 | 140 ± 1 | 0.3813 |
| At week 12 | 78 ± 7 | 81 ± 5 | 0.1444 | At week 12 | 141 ± 2 | 140 ± 2 | 0.2341 |
| K | HDL-C | ||||||
| Screening | 4.2 ± 0.5 | 4.5 ± 0.4 | - | Screening | 66 ± 12 | 67 ± 12 | 0.4286 |
| At week 12 | 4.3 ± 0.3 | 4.1 ± 0.5 | 0.4787 | At week 12 | 62 ± 11 | 64 ± 14 | 0.4605 |
| Hemoglobin | LDL-C | ||||||
| Screening | 12.8 ± 0.8 | 13.2 ± 0.4 | 0.4078 | Screening | 90 ± 18 | 108 ± 29 | 0.4286 |
| At week 12 | 13.5 ± 0.8 | 13.3 ± 0.3 | 0.3671 | At week 12 | 89 ± 21 | 115 ± 22 | 0.4605 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Choi, Y.; An, Y.; Jung, Y.-R.; Lee, J.-Y.; Lee, H.-J.; Jeong, J.; Kim, Z.; Kim, K. Development of p-Coumaric Acid Analysis in Human Plasma and Its Clinical Application to PK/PD Study. J. Clin. Med. 2021, 10, 108. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010108
Kim H, Choi Y, An Y, Jung Y-R, Lee J-Y, Lee H-J, Jeong J, Kim Z, Kim K. Development of p-Coumaric Acid Analysis in Human Plasma and Its Clinical Application to PK/PD Study. Journal of Clinical Medicine. 2021; 10(1):108. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010108
Chicago/Turabian StyleKim, Hohyun, Yunkyoung Choi, Yongwun An, Young-Rim Jung, Jin-Yong Lee, Hong-Jin Lee, Jihoon Jeong, Zisoo Kim, and Kyeongsoon Kim. 2021. "Development of p-Coumaric Acid Analysis in Human Plasma and Its Clinical Application to PK/PD Study" Journal of Clinical Medicine 10, no. 1: 108. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010108