The Revised Mood Rhythm Instrument: A Large Multicultural Psychometric Study

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Sample Characterization
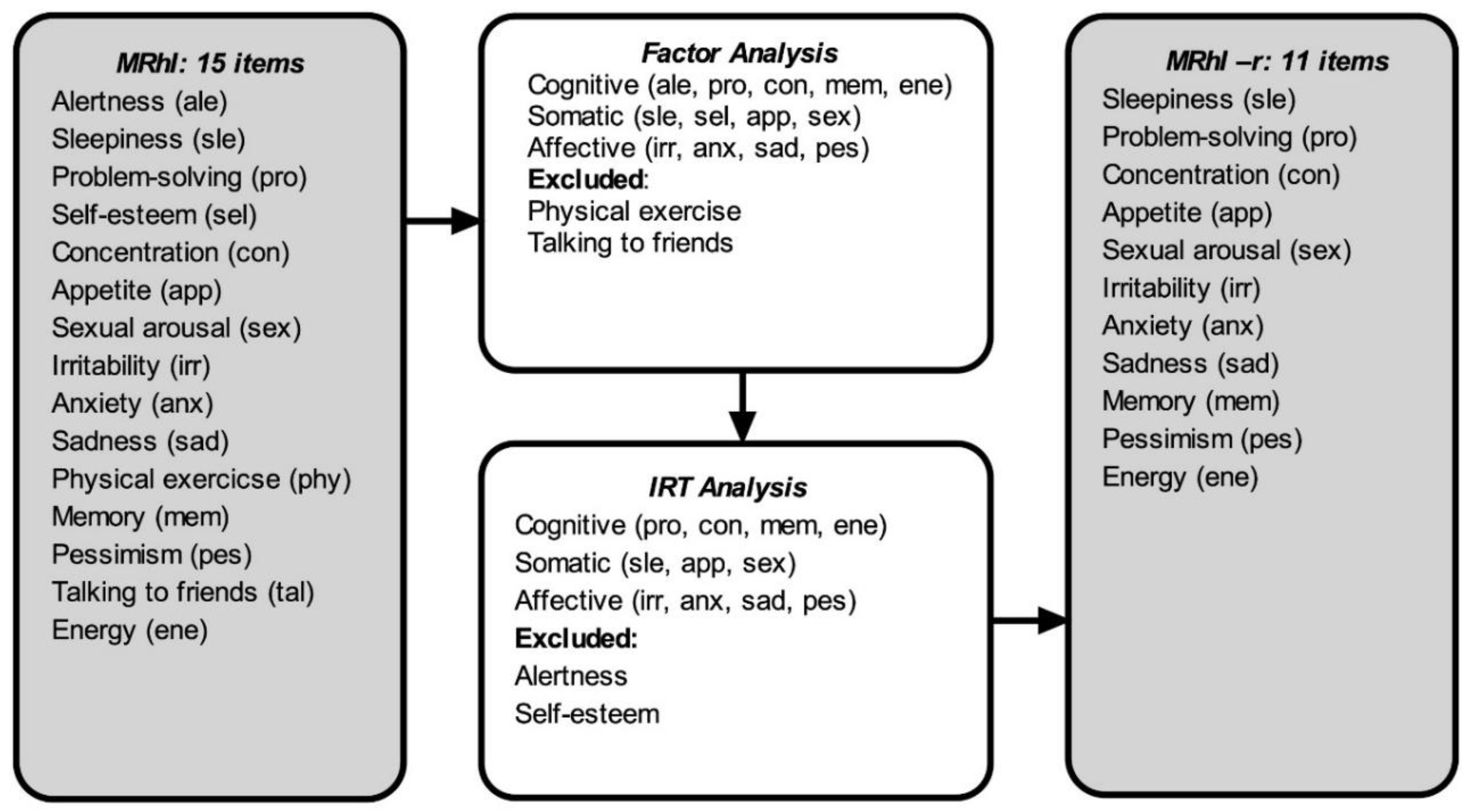
2.2. Mood Rhythm Instrument (MRhI)
2.3. Self-Reporting Questionnaire (SRQ-20)
2.4. Data Analysis Procedures
3. Results
3.1. Factor Analysis
3.2. Rasch Analysis
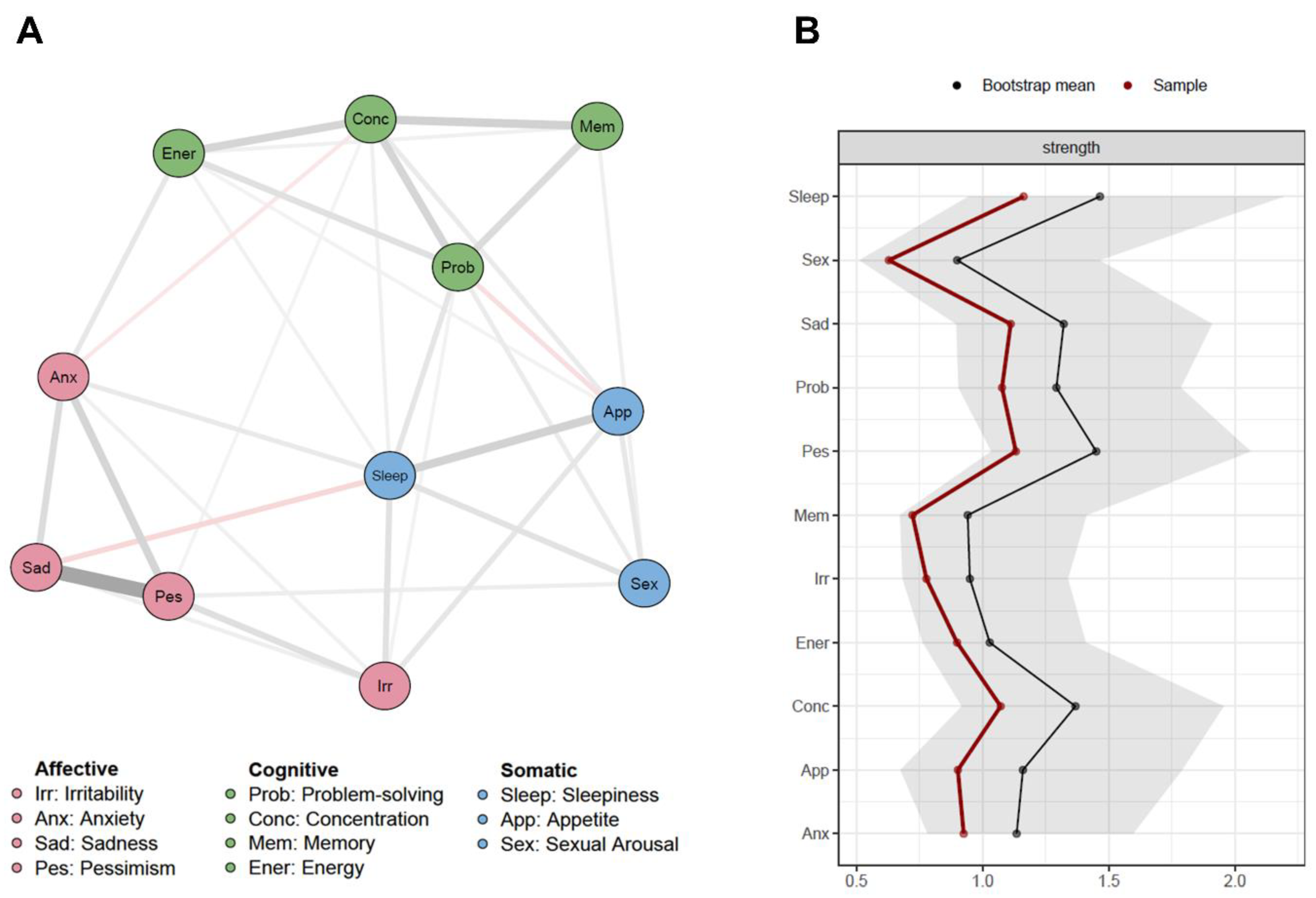
3.3. Network Analysis
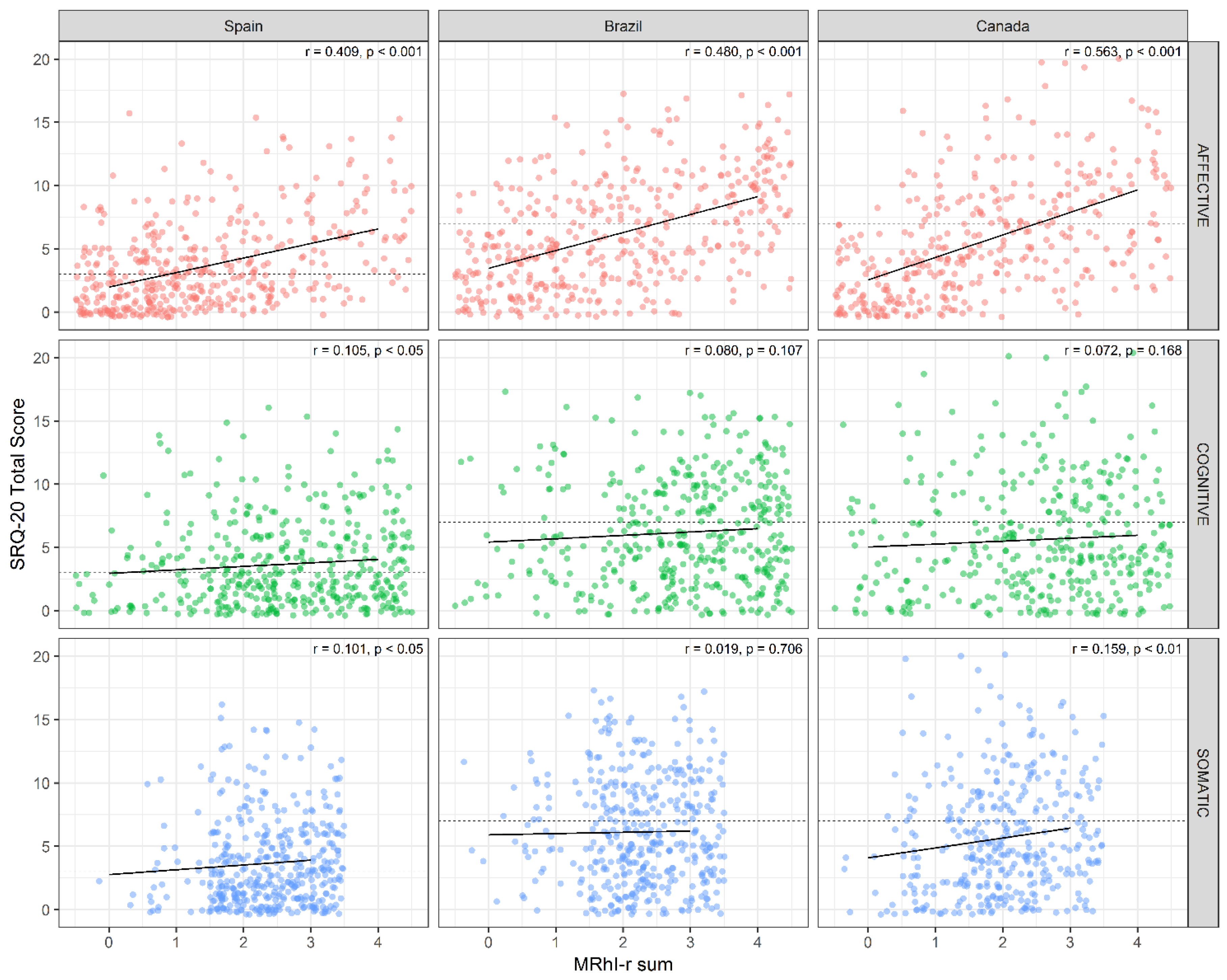
3.4. Correlation with Psychiatric Disorders Screening
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Statement of Ethics
References
- Adan, A.; Archer, S.N.; Hidalgo, M.P.; Di Milia, L.; Natale, V.; Randler, C. Circadian typology: A comprehensive review. Chrono. Int. 2012, 29, 1153–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allega, O.R.; Leng, X.; Vaccarino, A.; Skelly, M.; Lanzini, M.; Hidalgo, M.P.L.; Soares, C.N.; Kennedy, S.H.; Frey, B.N. Performance of the biological rhythms interview for assessment in neuropsychiatry: An item response theory and actigraphy analysis. J. Affect. Disord. 2018, 225, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Moraes, C.Á.; Cambras, T.; Díez-Noguera, A.; Schimitt, R.L.; Dantas, G.; Levandovski, R.M.; Hidalgo, M.P.L. A new chronobiological approach to discriminate between acute and chronic depression using peripheral temperature, rest-activity, and light exposure parameters. BMC Psychiatry 2013, 13, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, R.W.; McClung, C.A. Rhythms of life: Circadian disruption and brain disorders across the lifespan. Nat. Rev. Neurosci. 2018, 20, 49–65. [Google Scholar] [CrossRef]
- McClung, C.A. How might circadian rhythms control mood? Let me count the ways. Biol. Psychiatry 2013, 74, 242–249. [Google Scholar] [CrossRef]
- Wulff, K.; Gatti, S.; Wettstein, J.G.; Foster, R.G. Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nat. Rev. Neurosci. 2010, 11, 589–599. [Google Scholar] [CrossRef]
- Hickie, I.B.; Naismith, S.L.; Robillard, R.; Scott, E.M.; Hermens, D.F. Manipulating the sleep-wake cycle and circadian rhythms to improve clinical management of major depression. BMC Med. 2013, 11, 79. [Google Scholar] [CrossRef]
- Hühne, A.; Welsh, D.K.; Landgraf, D. Prospects for circadian treatment of mood disorders. Ann. Med. 2018, 50, 637–654. [Google Scholar] [CrossRef] [Green Version]
- Krawczak, E.M.; Minuzzi, L.; Hidalgo, M.P.L.; Frey, B.N. Do changes in subjective sleep and biological rhythms predict worsening in postpartum depressive symptoms? A prospective study across the perinatal period. Arch. Women’s Ment. Heal. 2016, 19, 591–598. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Wei, H.; Nievergelt, C.M.; Stautland, A.; Maihofer, A.X.; Welsh, D.K.; Shilling, P.; Alda, M.; Alliey-Rodriguez, N.; Anand, A.; et al. Chronotype and cellular circadian rhythms predict the clinical response to lithium maintenance treatment in patients with bipolar disorder. Neuropsychopharmacology 2018, 44, 620–628. [Google Scholar] [CrossRef]
- Tonon, A.C.; Fuchs, D.F.P.; Gomes, W.B.; Levandovski, R.M.; Fleck, M.P.D.A.; Hidalgo, M.P.L.; Alencastro, L.D.S. Nocturnal motor activity and light exposure: Objective actigraphy-based marks of melancholic and non-melancholic depressive disorder. Brief report. Psychiatry Res. 2017, 258, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Bedrosian, T.A.; Nelson, R.J. Influence of the modern light environment on mood. Mol. Psychiatry 2013, 18, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Karatsoreos, I.N.; McEwen, B.S. Psychobiological allostasis: Resistance, resilience and vulnerability. Trends Cogn. Sci. 2011, 15, 576–584. [Google Scholar] [CrossRef] [PubMed]
- De Souza, C.M.; Carissimi, A.; Costa, D.; Francisco, A.P.; Medeiros, M.S.; Ilgenfritz, C.A.; De Oliveira, M.A.; Frey, B.N.; Hidalgo, M.P.L. The Mood Rhythm Instrument: Development and preliminary report. Rev. Bras. Psiquiatr. 2016, 38, 148–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carissimi, A.; Oliveira, M.A.B.; Frey, B.N.; Navarro, J.F.; Hidalgo, M.P.; Adan, A. Validation and psychometric properties of the Spanish Mood Rhythm Instrument. Biol. Rhythm. Res. 2019, 1–13. [Google Scholar] [CrossRef]
- Francisco, A.P.; De Oliveira, M.A.B.; Carissimi, A.; Fabris, R.C.; Ilgenfritz, C.A.V.; De Souza, C.M.; Medeiros, M.S.; Adan, A.; Hidalgo, M.P.L. Spanish translation of the mood rhythm instrument: A novel approach to mood evaluation. Clin. Biomed. Res. 2017, 37, 41–47. [Google Scholar] [CrossRef]
- Oliveira, M.A.B.; Epifano, K.; Mathur, S.; Carvalho, F.G.; Scop, M.; Carissimi, A.; Francisco, A.P.; Garay, L.L.S.; Adan, A.; Hidalgo, M.P.; et al. Validation of the English version of the Mood Rhythm Instrument. BMC Psychol. 2020, 8, 35. [Google Scholar] [CrossRef]
- Pilz, L.K.; Carissimi, A.; Francisco, A.P.; Oliveira, M.A.B.; Slyepchenko, A.; Epifano, K.; Garay, L.L.S.; Fabris, R.C.; Scop, M.; Streiner, D.L.; et al. Prospective assessment of daily patterns of mood-related symptoms. Front. Psychiatry 2018, 9, 370. [Google Scholar] [CrossRef]
- Pilz, L.K.; Carissimi, A.; Oliveira, M.A.B.; Francisco, A.P.; Fabris, R.C.; Medeiros, M.S.; Scop, M.; Frey, B.N.; Adan, A.; Hidalgo, M.P.L. Rhythmicity of mood symptoms in individuals at risk for psychiatric disorders. Sci. Rep. 2018, 8, 11402. [Google Scholar] [CrossRef]
- Pereira-Morales, A.J.; Casiraghi, L.P.; Adan, A.; Camargo-Sánchez, A. Mood rhythmicity is associated with depressive symptoms and caffeinated drinks consumption in South American young adults. Chrono. Int. 2018, 36, 225–236. [Google Scholar] [CrossRef]
- Beusenberg, M.; Orley, J.H.; World Health Organization. Division of Mental Health. A User’s Guide to the Self Reporting Questionnaire (SRQ/Compiled by M. Beusenberg and J. Orley. World Health Organization. 1994. Available online: https://apps.who.int/iris/handle/10665/61113 (accessed on 13 March 2019).
- Cherian, V.I.; Peltzer, K.; Cherian, L. The factor-structure of the Self Reporting Questionnaire (SRQ-20) in South Africa. East Afr. Med. J. 1998, 75, 654–656. [Google Scholar] [PubMed]
- Iacoponi, E.; Mari, J.D.J. Reliability and factor structure of the portuguese version of self-reporting questionnaire. Int. J. Soc. Psychiatry 1989, 35, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Van Der Westhuizen, C.; Wyatt, G.E.; Williams, J.K.; Stein, D.J.; Sorsdahl, K. Validation of the Self Reporting Questionnaire 20-Item (SRQ-20) for use in a low-and middle-income country emergency centre setting. Int. J. Ment. Heal. Addict. 2016, 14, 37–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Upadhyaya, A.; Creed, F.; Upadhyaya, M. Psychiatric morbidity among mothers attending well-baby clinic: A cross-cultural comparison. Acta Psychiatr. Scand. 1990, 81, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, D.M.; Stein, A.T.; Kapczinski, F. Avaliação de desempenho do Self-Reporting Questionnaire como instrumento de rastreamento psiquiátrico: Um estudo comparativo com o Structured Clinical Interview for DSM-IV-TR. Cad. Saúde Pública 2008, 24, 380–390. [Google Scholar] [CrossRef] [Green Version]
- Livianos Aldana, L.; Rojo Moreno, L.; Domínguez Carabantes, A.; Bofill Moscardó, I. Validación del SRQ en los exámenes de salud mental en la población general. Actas Luso Esp Neurol Psiquiatr Cienc Afines 1990, 18, 286–289. [Google Scholar]
- Izquierdo, I.; Olea, J.; Abad, F.J. Exploratory factor analysis in validation studies: Uses and recommendations. Psicothema 2014, 26, 395–400. [Google Scholar]
- Muthén, L.K.; Muthén, B. Mplus User’s Guide, 6th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2010. [Google Scholar]
- Cattell, R.B. The scree test for the number of factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Beaujean, A.A. Latent Variable Modeling Using R: A Step-by-Step Guide, 1st ed.; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bond, T.; Fox, C. Applying the Rasch Model: Fundamental Measurement in the Human Sciences; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Linacre, J.M. What do infit and outfit, mean-square and standardized mean? Rasch Meas. Trans. 2002, 16, 878. [Google Scholar]
- Boone, W.J.; Staver, J.R.; Yale, M.S. Rasch Analysis in the Human Sciences; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2017, 50, 195–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmittmann, V.D.; Cramer, A.O.; Waldorp, L.J.; Epskamp, S.; Kievit, R.A.; Borsboom, D. Deconstructing the construct: A network perspective on psychological phenomena. New Ideas Psychol. 2013, 31, 43–53. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics 2008, 9, 432–441. [Google Scholar] [CrossRef] [Green Version]
- Psych: Procedures for Psychological, Psychometric, and Personality Research. Available online: https://cran.r-project.org/web/packages/psych/index.html (accessed on 21 May 2019).
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. qgraph: Network visualizations of relationships in psychometric data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- RStudio ggplot2: Create Elegant Data Visualisations Using the Grammar of Graphics. Available online: https://cran.r-project.org/web/packages/ggplot2/index.html (accessed on 21 May 2019).
- Yatham, L.N.; Kennedy, S.H.; Parikh, S.V.; Schaffer, A.; Bond, D.J.; Frey, B.N.; Sharma, V.; Goldstein, B.I.; Rej, S.; Beaulieu, S.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018, 20, 97–170. [Google Scholar] [CrossRef]
- Boschloo, L.; Van Borkulo, C.D.; Borsboom, D.; Schoevers, R.A. A Prospective study on how symptoms in a network predict the onset of depression. Psychother. Psychosom. 2016, 85, 183–184. [Google Scholar] [CrossRef]
- Contreras, A.; Nieto, I.; Valiente, C.; Espinosa, R.; Vazquez, C. The study of psychopathology from the network analysis perspective: A systematic review. Psychother. Psychosom. 2019, 88, 71–83. [Google Scholar] [CrossRef]
- Borsboom, D. A network theory of mental disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Curtiss, J.; Fulford, D.; Hofmann, S.G.; Gershon, A. Network dynamics of positive and negative affect in bipolar disorder. J. Affect. Disord. 2019, 249, 270–277. [Google Scholar] [CrossRef]
- Vanzhula, I.A.; Calebs, B.; Fewell, L.; Levinson, C.A. Illness pathways between eating disorder and post-traumatic stress disorder symptoms: Understanding comorbidity with network analysis. Eur. Eat. Disord. Rev. 2018, 27, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Fried, E.I.; Epskamp, S.; Nesse, R.M.; Tuerlinckx, F.; Borsboom, D. What are ’good’ depression symptoms? Comparing the centrality of DSM and non-DSM symptoms of depression in a network analysis. J. Affect. Disord. 2016, 189, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Tu, S.; Sheng, J.; Shao, A. Depression in sleep disturbance: A review on a bidirectional relationship, mechanisms and treatment. J. Cell. Mol. Med. 2019, 23, 2324–2332. [Google Scholar] [CrossRef] [Green Version]
- Thorpy, M.J. Which clinical conditions are responsible for impaired alertness? Sleep Med. 2005, 6, S13–S20. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cognitive | Somatic | Affective | U | |
|---|---|---|---|---|
| Q5 Concentration | 0.83 * | −0.02 | −0.03 | 0.34 |
| Q1 Alertness | 0.64 * | −0.05 | 0.03 | 0.60 |
| Q15 Energy | 0.59 * | 0.02 | 0.13 | 0.55 |
| Q3 Problem-solving | 0.53 * | 0.22 * | 0.01 | 0.54 |
| Q12 Memory | 0.45 * | 0.21 * | 0.04 | 0.62 |
| Q11 Physical exercise | 0.28 * | 0.28 * | −0.26 * | 0.79 |
| Q4 Self-esteem | −0.01 | 0.57 * | 0.29 | 0.48 |
| Q7 Sexual arousal | −0.07 | 0.56 * | 0.10 | 0.67 |
| Q2 Sleepiness | 0.25 | 0.49 * | −0.03 | 0.58 |
| Q6 Appetite | 0.07 | 0.37 * | 0.08 | 0.79 |
| Q14 Talking to friends | 0.06 | 0.31 * | 0.21 * | 0.78 |
| Q13 Pessimism | 0.01 | −0.06 | 0.87 * | 0.27 |
| Q10 Sadness | −0.05 | 0.01 | 0.83 * | 0.32 |
| Q9 Anxiety | 0.10 | 0.01 | 0.62 * | 0.55 |
| Q8 Irritability | 0.06 | 0.22* | 0.44 * | 0.65 |
| Eigenvalues | 4.90 | 1.89 | 1.19 | |
| % variance | 32.7 | 12.7 | 8.0 |
| Difficulty | Infit | Difficulty Measure | Differential Item Functioning Contrast | ||||||
|---|---|---|---|---|---|---|---|---|---|
| SP | BR | CA | SP-BR | SP-CA | BR-CA | ||||
| Cognitive | Memory | 2.10 | 1.02 | 1.48 | 2.45 | 2.55 | −0.97 * | −1.07 * | −0.10 |
| Concentration | −1.33 | 0.84 | −1.67 | −1.33 | −1.01 | −0.34 | −0.66 | −0.32 | |
| Alertness | −0.64 | 1.00 | −0.02 | −1.39 | −0.90 | 1.37 * | 0.88 * | −0.49 | |
| Energy | −0.16 | 0.94 | 0.71 | −0.72 | −0.83 | 1.43 * | 1.54 * | 0.11 | |
| Problem-solving | 0.04 | 0.91 | −0.10 | 0.34 | −0.10 | −0.44 | 0.00 | 0.44 | |
| Somatic | Sleepiness | −3.97 | 1.02 | −3.71 | −3.60 | −4.39 | −0.11 | 0.68 | 0.79 |
| Self-esteem | 2.75 | 0.99 | 3.35 | 2.53 | 2.30 | 0.82 * | 1.05 * | 0.23 | |
| Sexual arousal | 2.46 | 0.94 | 2.12 | 2.59 | 2.81 | −0.47 | −0.69 * | −0.22 | |
| Appetite | −1.25 | 0.96 | −1.63 | −1.20 | −0.98 | −0.42 | −0.64 | −0.22 | |
| Affective | Irritability | −1.65 | 1.16 | −2.16 | −1.35 | −1.39 | −0.81 * | −0.77 * | 0.04 |
| Pessimism | 1.00 | 0.88 | 0.80 | 1.14 | 1.08 | −0.34 | −0.28 | 0.06 | |
| Sadness | 0.57 | 0.91 | 0.88 | 0.50 | 0.32 | 0.38 | 0.56 | 0.18 | |
| Anxiety | 0.08 | 1.02 | 0.40 | −0.22 | 0.03 | 0.62 | 0.37 | −0.25 | |
| Difficulty | Infit | Difficulty Measure | Differential Item Functioning Contrast | ||||||
|---|---|---|---|---|---|---|---|---|---|
| SP | BR | CA | SP-BR | SP-CA | BR-CA | ||||
| Cognitive | Memory | 2.45 | 1.09 | 1.60 | 2.78 | 3.28 | −1.18 * | −1.68 * | −0.51 |
| Concentration | −1.87 | 0.97 | −2.31 | −1.87 | −1.43 | −0.44 | −0.88 * | −0.45 | |
| Energy | −0.40 | 1.00 | 0.61 | −1.12 | −1.19 | 1.73 * | 1.79 * | 0.06 | |
| Problem-solving | −0.17 | 0.91 | −0.36 | 0.17 | −0.27 | −0.53 | −0.09 | 0.44 | |
| Somatic | Sleepiness | −3.57 | 1.05 | −3.19 | −3.26 | −3.96 | 0.08 | 0.77 | 0.69 |
| Sexual arousal | 4.04 | 1.00 | 4.04 | 3.98 | 4.14 | 0.07 | −0.09 | −0.16 | |
| Appetite | −0.47 | 0.88 | −0.57 | −0.52 | −0.36 | −0.04 | −0.21 | −0.16 | |
| Affective | Irritability | −1.65 | 1.16 | −2.16 | −1.35 | −1.39 | −0.81 * | −0.77 * | 0.04 |
| Pessimism | 1.00 | 0.88 | 0.80 | 1.14 | 1.08 | −0.34 | −0.28 | 0.06 | |
| Sadness | 0.57 | 0.91 | 0.80 | 0.50 | 0.32 | 0.38 | 0.56 | 0.18 | |
| Anxiety | 0.08 | 1.02 | 0.40 | −0.22 | 0.03 | 0.62 | 0.37 | −0.25 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves Braga de Oliveira, M.; de Mendonça Filho, E.J.; Carissimi, A.; Lima dos Santos Garay, L.; Scop, M.; Ruschel Bandeira, D.; Gutiérrez Carvalho, F.; Mathur, S.; Epifano, K.; Adan, A.; et al. The Revised Mood Rhythm Instrument: A Large Multicultural Psychometric Study. J. Clin. Med. 2021, 10, 388. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030388
Alves Braga de Oliveira M, de Mendonça Filho EJ, Carissimi A, Lima dos Santos Garay L, Scop M, Ruschel Bandeira D, Gutiérrez Carvalho F, Mathur S, Epifano K, Adan A, et al. The Revised Mood Rhythm Instrument: A Large Multicultural Psychometric Study. Journal of Clinical Medicine. 2021; 10(3):388. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030388
Chicago/Turabian StyleAlves Braga de Oliveira, Melissa, Euclides José de Mendonça Filho, Alicia Carissimi, Luciene Lima dos Santos Garay, Marina Scop, Denise Ruschel Bandeira, Felipe Gutiérrez Carvalho, Salina Mathur, Kristina Epifano, Ana Adan, and et al. 2021. "The Revised Mood Rhythm Instrument: A Large Multicultural Psychometric Study" Journal of Clinical Medicine 10, no. 3: 388. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030388