
Testosterone and Bone Health in Men: A Narrative Review


Department of Integrative Cancer Therapy and Urology, Kanazawa University Graduate School of Medical Science, 13-1, Kanazawa, Ishikawa 920-8641, Japan
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2021, 10(3), 530; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030530
Submission received: 15 December 2020
/
Revised: 20 January 2021
/
Accepted: 23 January 2021
/
Published: 2 February 2021
(This article belongs to the Special Issue Osteoporosis and Related Bone Metabolic Disease)
Abstract
:Bone fracture due to osteoporosis is an important issue in decreasing the quality of life for elderly men in the current aging society. Thus, osteoporosis and bone fracture prevention is a clinical concern for many clinicians. Moreover, testosterone has an important role in maintaining bone mineral density (BMD) among men. Some testosterone molecular mechanisms on bone metabolism have been currently established by many experimental data. Concurrent with a decrease in testosterone with age, various clinical symptoms and signs associated with testosterone decline, including decreased BMD, are known to occur in elderly men. However, the relationship between testosterone levels and osteoporosis development has been conflicting in human epidemiological studies. Thus, testosterone replacement therapy (TRT) is a useful tool for managing clinical symptoms caused by hypogonadism. Many recent studies support the benefit of TRT on BMD, especially in hypogonadal men with osteopenia and osteoporosis, although a few studies failed to demonstrate its effects. However, no evidence supporting the hypothesis that TRT can prevent the incidence of bone fracture exists. Currently, TRT should be considered as one of the treatment options to improve hypogonadal symptoms and BMD simultaneously in symptomatic hypogonadal men with osteopenia.
1. Introduction
Serum testosterone levels decrease by 1% annually with age in elderly men [1], which may induce various clinical symptoms of late-onset hypogonadism (LOH) syndrome [2]. LOH syndrome is involved in a cluster of clinical symptoms, including depression, irritability, sexual dysfunction, decreased muscle mass and strength, and decreased bone mineral density (BMD), visceral obesity, and metabolic syndrome, which have been thought to be associated with aging [3,4]. These symptoms and signs often impair the quality of life (QOL) in elderly men and are considered a serious public health concern in the current aging society. Thus, testosterone replacement therapy (TRT) is expected to be one of the tools for improving these clinical conditions and QOL in men with LOH syndrome. Consequently, its clinical use has substantially increased over the past years [5].
In particular, osteoporosis often causes compression spine fractures and femoral neck fractures in elderly men, resulting in a decrease of activities of daily living (ADL) and QOL. Estrogen, which is important for maintaining BMD, decreases immediately in women during menopause. However, testosterone, which decreases slowly with age, plays an important role in maintaining BMD in men. Therefore, osteoporosis occurs more commonly in elderly women than in men [6,7]. The prevalence of osteoporosis increases with age at <10%, 13%, 18%, and 21% for 40, 70–75, 75–80, and >80 year old men in Japan, respectively [8]. Moreover, about 12 million people are estimated to suffer from osteoporosis [6,7]. The incidence frequency of femoral neck fracture is fourfold more in men than in women with osteoporosis [9]. Thus, osteoporosis prevention is an important issue in maintaining ADL and QOL in elderly men.
BMD has a close correlation with serum testosterone levels in men. Moreover, testosterone levels immediately decrease because of androgen deprivation therapy (ADT) for prostate cancer, resulting in a decrease of BMD and osteoporosis. In addition, estradiol (E2) converted from testosterone by aromatase is deeply related to BMD maintenance. A relative decrease in estrogen level due to ADT also poses a risk for BMD loss [10,11]. In general, BMD decreases by about 2%–8% in 1 year after the commencement of ADT [12]. Furthermore, ADT increases the risk of decreased BMD at five- to tenfold compared to prostate cancer patients with normal testosterone levels. A meta-analysis demonstrated that 9%–53% of osteoporosis incidence was caused by ADT [13]. Consequently, patients with ADT have a definite higher risk of sustaining a fracture. Furthermore, ADT can increase the risk of proximal femur fractures by 1.5- to 1.8-fold [14,15]. The BMD decrease in these patients is caused by a decline in serum testosterone and estrogen levels by ADT.
As aforementioned, the association between testosterone deficiency and BMD loss has been currently clarified. It is believed that TRT can contribute to maintaining and increasing BMD among hypogonadal men. However, the efficacy of TRT for bone health in hypogonadal men has been currently less in consensus and more conflicting [16,17,18,19,20,21]. Therefore, this article reviewed the relationship between testosterone and BMD in men and mentioned the benefits of TRT on BMD among hypogonadal men.
2. Materials and Methods
A review of PubMed, MEDLINE, and EMBASE databases was conducted to search for original articles, systematic review, and meta-analysis under key words as following; “testosterone” or “hypogonadism”, “bone mineral density” or “osteoporosis” or “bone fracture”, and “men”. There was no limitation on language, publication status, and study design. Papers published from January 1990 through to October 2020 were collected. We also checked the references of systematic reviews and meta-analyses carefully to identify additional original articles for inclusion. Two reviewers screened the search results, and the data were collected on 4 November 2020.
All papers suitable for three topics including “The Relationship between Hypogonadism and BMD in human”, “The Relationship between Testosterone and Bone Fracture”, and “The Effects of TRT on Bone Health among Hypogonadal Men” from the journal databases were adopted for the present analysis.
3. Molecular Roles of Sex Hormones on Bone Metabolism
Testosterone is converted to highly active dihydrotestosterone (DHT) by 5α-reductase in the cytoplasm of target cells [22,23]. Consequently, DHT can induce androgenic activity by binding to the androgen receptor (AR). Moreover, testosterone is converted to E2 by aromatase. E2 binds to the estrogen receptor (ER) and exerts estrogenic action. ERα and ERβ are the two ER subtypes. ERα is mainly associated with bone metabolism [10,24].
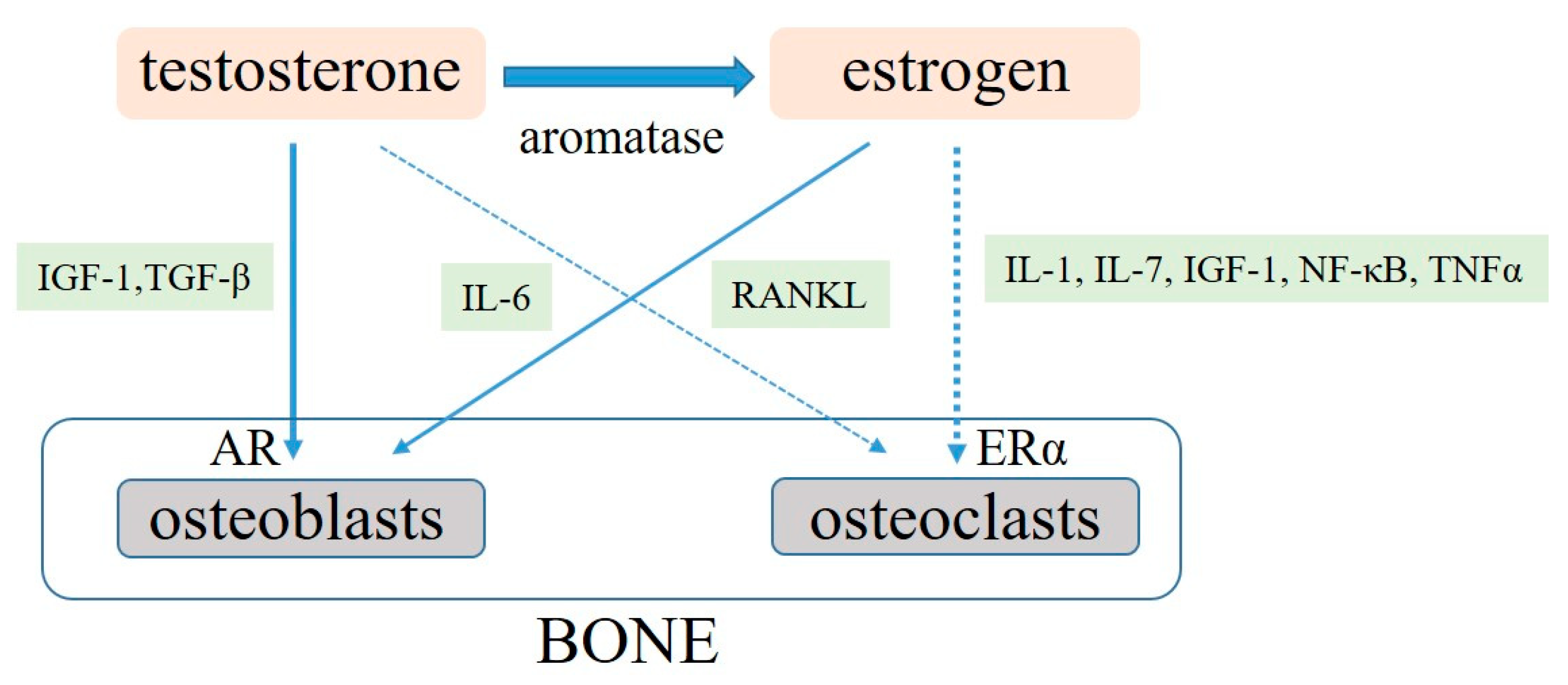
AR is present in chondrocytes and osteoblasts, although its expression level widely varies by age and bone sites. Testosterone acts directly on osteoblasts by AR and can consequently promote bone formation [17]. In addition, testosterone has some indirect effects on bone metabolism through various cytokines and growth factors [17,25,26,27,28] (Figure 1). Furthermore, testosterone can increase AR expression level in osteoblasts, resulting in differentiation promotion and osteoblast and chondrocyte apoptosis proliferation [17,29]. Consequently, less evidence supporting the hypothesis that testosterone has any direct effects on osteoclasts has been shown [30].
In addition, testosterone deficiency promotes the activation of nuclear factor kappa-B ligand (RANKL) production from osteoblasts, which contributes to the promotion of the differentiations and functions in osteoclasts. Increased RANKL level progresses bone resorption and decreases BMD [25,26]. Thus, testosterone positively regulates the expression of insulin-like growth factor-1 (IGF-1) and IGF-binding protein (IGF-BP) in osteoblasts. The differentiation and proliferation of chondrocytes and osteoblasts are induced by IGF and IGF-BP, and the suppression of apoptosis of chondrocytes promotes bone formation. Moreover, testosterone activates the expression of transforming growth factor-β (TGF-β) in osteoblasts and promotes the differentiation of osteoblasts [27]. Testosterone suppresses the activity of interleukins (IL)-6, which activates osteoclasts and promotes bone resorption. However, testosterone deficiency decreases in BMD through increased IL-6 activation [28].
E2 and ERα also play important roles in maintaining BMD in men and women. Estrogen has a greater effect than androgen in inhibiting bone resorption in men. Consequently, men with loss of ERα function exhibit extremely low BMD [31]. Male patients with aromatase deficiency have a marked decrease in BMD in trabecular and cortical bone. Thus, estrogen replacement therapy in these patients can improve BMD [32,33]. E2 generally regulates apoptosis and function of osteoclast, which contributes to BMD maintenance. Moreover, E2 deficiency may accelerate osteoclast apoptosis by increased tumor growth factor-β production [34,35]. IL-1, IL-6, IL-7, IGF-1, nuclear factor-κB (NF-κB), RANKL, and tumor necrotic factor-α (TNFα) are the E2 target genes [36,37,38,39]. However, E2 deficiency increases IL-6, which reduces osteoblast proliferation and activity while increasing osteoclastic activity and increasing the expression of RANKL-mediated osteoclastogenesis [36,37]. Some experimental data showed that estrogen decrease also induces inflammatory cytokine, IL-1, and TNFα, resulting in BMD loss. However, this phenomenon does not occur in IL-1 receptor- or TNFα-deficient mice [38,39].
4. The Relationship between Hypogonadism and BMD in Humans
The apparent relationship between testosterone deficiency and low BMD has been currently established [5]. In particular, this relationship is much stronger in young adult men with moderate to severe hypogonadism [40,41]. However, epidemiological information on male osteoporosis attributed to hypogonadism, especially in elderly men, has been less available. Therefore, the prevalence of hypogonadism among men with osteoporosis or bone fracture has not been clarified.
Some previous studies demonstrated that hypogonadism was the cause of male osteoporosis (6.9%–58%) [42,43,44,45,46,47] (Table 1). However, these studies are limited by their small sizes and various potential biases. In addition, case–control studies comparing the prevalence of hypogonadism between subjects with osteoporosis and controls have been limited.
A case–control study found that the prevalence rates of hypogonadism in men with osteoporotic fracture and control were 58% and 18%, respectively [42]. A cross-sectional and longitudinal study involving 2447 community-dwelling elderly men stated that the prevalence rates of hypogonadism among men with osteoporosis and normal BMD were 6.9% and 3.2%. Conversely, the prevalence of osteoporosis in men with hypogonadism was significantly higher in those with eugonadism (12.3% and 6.0%, respectively) [45]. Furthermore, a recent meta-analysis involving 300 patients from five case–control studies revealed that no significant difference was observed in testosterone level in both cases and controls [48]. Fewer exercise habits, cigarette smoking, various medications, and underlying diseases (e.g., metabolic syndrome, especially in elderly men) may modify the exact relationship between testosterone and osteoporosis, resulting in conflicting data. Further case–control studies involving a large number of subjects are likely required to better clarify whether prevalence of osteoporosis is higher in hypogonadal compared with eugonadal men.
In addition, whether low testosterone is a potential risk factor for developing male osteoporosis in men is still unclear. Several large-population observational trials have been performed to investigate the effects of testosterone deficiency on osteoporosis risk factors in men [45,49,50,51,52,53,54,55,56,57,58] (Table 2). Some previous studies supported the potential relationship between testosterone decline and low BMD [45,49,51,54], and other studies denied this association [50,52,53,55,56,57,58]. Conversely, some previous studies found that E2 was significantly correlated with BMD loss in elderly men [45,49,50,54,55,56,57], supporting the hypothesis that E2 is also significantly correlated with BMD in men. In men, 85% of serum E2 derives from testosterone conversion by aromatase [59]. Therefore, low testosterone leads to low E2 production via aromatase, which could provoke deleterious effects on BMD, but also on bone quality as assessed in vivo by some different diagnostic tools [60,61]. A previous study demonstrated that 12-month administration of aromatase inhibitor in elderly men with hypogonadism resulted in a further decrease in BMD [62].
The conflicting results on the role of testosterone in BMD may also be because serum testosterone levels do not always reflect local testosterone levels within bone tissues and localized testosterone metabolism. A sub-analysis of the prospective MrOS study in Sweden involving 631 elderly men showed that glucuronidated androgen metabolites, but not serum TT, had a significant correlation with BMD in elderly men, suggesting that localized testosterone levels may have an important role in maintaining BMD [63].
5. The Relationship between Testosterone and Bone Fracture
Falling and fractures in elderly men have a great impact on ADL and life prognosis. Moreover, preventing them has become an important issue worldwide. The occurrence of fractures associated with aging is largely due to the decrease in physical function (e.g., muscle mass loss and muscle weakness, frailty, and sarcopenia) in addition to the decrease in BMD [64,65]. Consequently, various clinical conditions caused by testosterone deficiency with age can also affect falls and fractures [2,3,4,5]. Additionally, osteoporosis is a bone condition in which bone mass and strength decrease with aging [8]. Thus, falls are an important factor in the onset of fractures.
Many previous studies investigated the relationship between testosterone and bone fracture risk [45,51,57,58,66,67,68,69,70,71,72,73,74] (Table 3). In addition, several studies have found that elderly men with osteoporotic fractures had statistically significant lower testosterone levels compared with age-matched controls [45,51,66,67,68,70,72,74], and other studies failed to show any associations between testosterone levels and fracture risk [57,58,69,71]. A meta-analysis including 55 studies demonstrated that a significant association was observed in hypogonadism, independent of age, low body mass index, cigarette smoking, excessive alcohol drinking, steroid use, history of diabetes, and so on [62]. Many studies were likely to support the negative effect of testosterone deficiency on the incidences of fall and fracture [45,51,66,67,68,70,72,74], although a smaller number of studies denied this relationship [57,58,69,71]. The more predominant roles for testosterone bone fracture in comparison with BMD may be due to the other role of testosterone in muscle strength and physical performance in men, which leads to sarcopenia and falls risks.
Furthermore, one previous review stated that E2 levels predict the risk of bone fracture, independent of not only serum testosterone and androgens but also estrogens, which are important regulators of bone health in men [75].
6. The Effects of TRT on Bone Health among Hypogonadal Men
TRT for hypogonadal men can improve various symptoms (e.g., metabolic syndrome) and has been used worldwide for managing these symptoms and maintaining QOL [2,5]. Moreover, testosterone plays some potential roles in maintaining BMD among men, and TRT is expected to be useful for preventing and managing osteoporosis and improving BMD among hypogonadal men.
Many recent previous studies suggested the ameliorative effect of TRT on osteoporosis/osteopenia [76,77,78,79,80,81,82,83,84] (Table 4). A meta-analysis involving 1083 subjects from 29 randomized controlled studies (RCTs) demonstrated that TRT could improve BMD at the lumbar spine by +3.7% (confidence interval, 1.0%–6.4%) compared with placebo [20]. In particular, many of the previous reports published since 2010 suggest some benefits of TRT on BMD. By contrast, a smaller number of studies failed to find the positive effect of BMD [85,86,87]. However, the subjects of this study were limited to men with hypogonadism, but not always with a lower BMD at baseline. Three studies targeting hypogonadal men with osteopenia or osteoporosis demonstrated that TRT could significantly increase their BMD [76,78,83]. Currently, extremely limited studies, including long-term TRT over 3 years, are available. Further larger and longer RCTs are likely to be required to reach a conclusive result regarding the effects of TRT on bone health and to investigate the benefit of the severity of hypogonadism, degree of baseline BMD loss, and dose of testosterone supplement.
Currently, some guidelines have recommended TRT for symptomatic hypogonadal men with osteoporosis to prevent bone loss and help in acquiring peak bone mass [41,88,89,90,91]. However, the effects of TRT for decreasing the risk of fracture in hypogonadal men with osteopenia and osteoporosis remain unclear. Testosterone therapies have various inverse effects, including erythrocytosis, worsening of prostate hypertrophy and lower urinary tract symptoms, worsening of sleep apnea syndrome, and cardiovascular effects, which are likely to outweigh the beneficial effect for BMD improvement [2,3,5]. Therefore, TRT is not recommended as a tool solely to enhance and maintain BMD for hypogonadal men. At present, vitamin D formulation and antiresorptive drugs are understandably recommended to treat hypogonadism-related osteoporosis in elderly men [92,93,94,95]. On the other hand, TRT should be considered for the patients with any hypogonadal symptoms, and TRT may be an alternative tool for improving hypogonadal symptoms and BMD simultaneously in such cases.
7. Conclusions
Testosterone plays an important role in maintaining BMD and bone health among men. In addition, many molecular mechanisms of testosterone on bone metabolism have been currently established by many experimental data. Several recent studies demonstrated the benefit of TRT on BMD, especially in hypogonadal men with osteopenia and osteoporosis. However, a few studies failed to demonstrate its effects, and no evidence supporting the hypothesis that TRT can prevent bone fracture incidence exists. Further studies involving a large number of subjects and longer treatment duration are required to reach a more conclusive result regarding the effects of TRT on bone health.
Current evidence suggests that TRT is not recommended as a tool solely to enhance and maintain BMD for hypogonadal men. TRT should be considered as one of the treatment options to improve hypogonadal symptoms and BMD simultaneously in symptomatic hypogonadal men with osteopenia.
Author Contributions
Data collection, K.S., K.I., Y.K.; writing—original draft preparation, K.S.; writing—review and editing, K.S., K.I.; supervision, A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Feldman, H.A.; Longcope, C.; Derby, C.A.; Johannes, C.B.; Araujo, A.B.; Coviello, A.D.; Bremner, W.J.; McKinlay, J.B. Age trends in the level of serum testosterone and other hormones in middle-aged men: Longitudinal results from the Massachusetts male aging study. J. Clin. Endocrinol. Metab. 2002, 87, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Lunenfeld, B.; Mskhalaya, G.; Zitzmann, M.; Arver, S.; Kalinchenko, S.; Tishova, Y.; Morgentaler, A. Recommendations on the diagnosis, treatment and monitoring of hypogonadism in men. Aging Male 2015, 18, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunenfeld, B.; Arver, S.; Moncada, I.; Rees, D.A.; Schulte, H.M. How to help the aging male? Current approaches to hypogonadism in primary care. Aging Male 2012, 15, 187–197. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.A.; Carson, C.C.; Coward, R.M. Diagnosis and management of testosterone deficiency. Asian. J. Androl. 2015, 17, 177–186. [Google Scholar]
- Bassil, N.; Alkaade, S.; Morley, J.E. The benefits and risks of testosterone replacement therapy: A review. Ther. Clin. Risk Manag. 2009, 5, 427–448. [Google Scholar]
- Yoshimura, N.; Muraki, S.; Oka, H.; Kawaguchi, H.; Nakamura, K.; Akune, T. Cohort profile: Research on osteoarthritis/osteoporosis disability study. Int. J. Epidemiol. 2010, 39, 988–995. [Google Scholar] [CrossRef] [Green Version]
- Melton, L.J.; Atkinson, E.J.; O’Connor, M.K.; O’Fallon, W.M.; Riggs, B.L. Bone density and fracture risk in men. J. Bone Miner. Res. 1998, 13, 1915–1923. [Google Scholar] [CrossRef]
- Yamamoto, L. Guideline for treatment of osteoporosis. Nippon Rinsho. 2002, 60, 280–287. [Google Scholar]
- van Staa, T.P.; Dennison, E.M.; Leufkens, H.G.; Cooper, C. Epidemiology of fractures in England and Wales. Bone 2001, 29, 517–522. [Google Scholar] [CrossRef] [Green Version]
- Almeida, M.; Laurent, M.R.; Dubois, V.; Claessens, F.; O’Brien, C.A.; Bouillon, R.; Vanderschueren, D.; Manolagas, S.C. Estrogens and Androgens in Skeletal Physiology and Pathophysiology. Physiol. Rev. 2017, 97, 135–187. [Google Scholar] [CrossRef]
- El Badri, S.A.; Salawu, A.; Brown, J.E. Bone Health in Men with Prostate Cancer: Review Article. Curr. Osteoporos. Rep. 2019, 17, 527–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsuzuka, K.; Arai, Y. Metabolic changes in patients with prostate cancer during androgen deprivation therapy. Int. J. Urol. 2018, 25, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lassemillante, A.C.; Doi, S.A.; Hooper, J.D.; Prins, J.B.; Wright, O.R. Prevalence of osteoporosis in prostate cancer survivors: A meta-analysis. Endocrine 2014, 45, 370–381. [Google Scholar] [CrossRef] [PubMed]
- Shahinian, V.B.; Kuo, Y.F.; Freeman, J.L.; Goodwin, J.S. Risk of fracture after androgen deprivation for prostate cancer. N. Engl. J. Med. 2005, 352, 154–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brahamsen, B.; Nielsen, M.F.; Esklldsen, P.; Andersen, J.T.; Walter, S.; Brixen, K. Fracture risk in Danish men with prostate cancer: A nationwide register study. BJU. Int. 2007, 100, 749–754. [Google Scholar] [CrossRef]
- Junjie, W.; Dongsheng, H.; Lei, S.; Hongzhuo, L.; Changying, S. Testosterone Replacement Therapy Has Limited Effect on Increasing Bone Mass Density in Older Men: A Meta-analysis. Curr. Pharm. Des. 2019, 25, 73–84. [Google Scholar] [CrossRef]
- Mohamad, N.V.; Soelaiman, I.N.; Chin, K.Y. A concise review of testosterone and bone health. Clin. Interv. Aging 2016, 11, 1317–1324. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Kang, D.; Li, H. The effects of testosterone on bone health in males with testosterone deficiency: A systematic review and meta-analysis. BMC Endocr. Disord. 2020, 20, 33. [Google Scholar] [CrossRef]
- Drake, M.T.; Murad, M.H.; Mauck, K.F.; Lane, M.A.; Undavalli, C.; Elraiyah, T.; Stuart, L.M.; Prasad, C.; Shahrour, A.; Mullan, R.J.; et al. Clinical review. Risk factors for low bone mass-related fractures in men: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2012, 97, 1861–1870. [Google Scholar] [CrossRef] [Green Version]
- Isidori, A.M.; Giannetta, E.; Greco, E.A.; Gianfrilli, D.; Bonifacio, V.; Isidori, A.; Lenzi, A.; Fabbri, A. Effects of testosterone on body composition, bone metabolism and serum lipid profile in middle-aged men: A meta-analysis. Clin. Endocrinol. 2005, 63, 280–293. [Google Scholar] [CrossRef]
- Tracz, M.J.; Sideras, K.; Boloña, E.R.; Haddad, R.M.; Kennedy, C.C.; Uraga, M.V.; Caples, S.M.; Erwin, P.J.; Montori, V.M. Testosterone use in men and its effects on bone health. A systematic review and meta-analysis of randomized placebo-controlled trials. J. Clin. Endocrinol. Metab. 2006, 91, 2011–2016. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.M.; Vermeulen, A. The decline of androgen levels in elderly men and its clinical and therapeutic implications. Endocr. Rev. 2005, 26, 833–876. [Google Scholar] [CrossRef] [PubMed]
- Labrie, F.; Cusan, L.; Gomez, J.L.; Martel, C.; Bérubé, R.; Bélanger, P.; Bélanger, A.; Vandenput, L.; Mellström, D.; Ohlsson, C. Comparable amounts of sex steroids are made outside the gonads in men and women: Strong lesson for hormone therapy of prostate and breast cancer. J. Steroid Biochem. Mol. Biol. 2009, 113, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Imai, Y.; Kondoh, S.; Kouzmenko, A.; Kato, S. Minireview: Osteoprotective action of estrogens is mediated by osteoclastic estrogen receptor-alpha. Mol. Endocrinol. 2010, 24, 877–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, K.Y.; Ima-Nirwana, S. The effects of orchidectomy and supraphysiological testosterone administration on trabecular bone structure and gene expression in rats. Aging Male 2015, 18, 60–66. [Google Scholar] [CrossRef]
- Li, X.; Ominsky, M.S.; Stolina, M.; Warmington, K.S.; Geng, Z.; Niu, Q.T.; Asuncion, F.J.; Tan, H.L.; Grisanti, M.; Dwyer, D.; et al. Increased RANK ligand in bone marrow of orchiectomized ra ts and prevention of their bone loss by the RANK ligand inhibitor osteoprotegerin. Bone 2009, 45, 669–676. [Google Scholar] [CrossRef]
- Gill, R.K.; Turner, R.T.; Wronski, T.J.; Bell, N.H. Orchiectomy markedly reduces the concentration of the three isoforms of transforming growth factor beta in rat bone, and reduction is prevented by testosterone. Endocrinology 1998, 139, 546–550. [Google Scholar] [CrossRef]
- Bellido, T.; Jilka, R.L.; Boyce, B.F.; Girasole, G.; Broxmeyer, H.; Dalrymple, S.A.; Murray, R.; Manolagas, S.C. Regulation of interleukin-6, osteoclastogenesis, and bone mass by androgens. The role of the androgen receptor. J. CIin. Investig. 1995, 95, 2886–2895. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Kaji, H.; Kanatani, M.; Sugimoto, T.; Chihara, K. Testosterone increases osteoprotegerin mRNA expression in mouse osteoblast cells. Horm. Metab. Res. 2004, 36, 674–678. [Google Scholar] [CrossRef]
- Kawano, H.; Sato, T.; Yamada, T.; Matsumoto, T.; Sekine, K.; Watanabe, T.; Nakamura, T.; Fukuda, T.; Yoshimura, K.; Yoshizawa, T.; et al. Suppressive function of androgen receptor in bone resorption. Proc. Natl. Acad. Sci. USA 2003, 100, 9416–9421. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.P.; Boyd, J.; Frank, G.R.; Takahashi, H.; Cohen, R.M.; Specker, B.; Williams, T.C.; Lubahn, D.B.; Korach, K.S. Estrogen resistance caused by a mutation in the estrogen-receptor gene in a man. N. Engl. J. Med. 1994, 331, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Morishima, A.; Grumbach, M.M.; Simpson, E.R.; Fisher, C.; Qin, K. Aromatase deficiency in male and female siblings caused by a novel mutation and the physiological role of estrogens. J. Clin. Endocrinol. Metab. 1995, 80, 3689–3698. [Google Scholar] [PubMed]
- Bilezikian, J.P.; Morishima, A.; Bell, J.; Grumbach, M.M. Increased bone mass as a result of estrogen therapy in a man with aromatase deficiency. N. Engl. J. Med. 1998, 339, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.E.; Dai, A.; Tiffee, J.C.; Li, H.H.; Mundy, G.R.; Boyce, B.F. Estrogen promotes apoptosis of murine osteoclasts mediated by TGF-beta. Nat. Med. 1996, 2, 1132–1136. [Google Scholar] [CrossRef]
- Raisz, L.G. Pathogenesis of osteoporosis: Concepts, conflicts, and prospects. J. Clin. Investig. 2005, 115, 3318–3325. [Google Scholar] [CrossRef] [Green Version]
- Ding, K.H.; Wang, Z.Z.; Hamrick, W.M.; Deng, Z.B.; Zhou, L.; Kang, B.; Yan, S.L.; She, J.X.; Stern, D.M.; Isales, C.M.; et al. Disordered osteoclast formation in RAGE-deficient mouse establishes an essential role for RAGE in diabetes related bone loss. Biochem. Biophys. Res. Commun. 2006, 340, 1091–1097. [Google Scholar] [CrossRef]
- Xie, J.; Méndez, J.D.; Méndez-Valenzuela, V.; Aguilar-Hernández, M.M. Cellular signaling of the receptor for advanced glycation end products (RAGE). Cell Signal 2013, 25, 2185–2197. [Google Scholar] [CrossRef]
- Kimble, R.B.; Matayoshi, A.B.; Vannice, J.L.; Kung, V.T.; Williams, C.; Pacifici, R. Simultaneous block of interleukin-1 and tumor necrosis factor is required to completely prevent bone loss in the early postovariectomy period. Endocrinology 1995, 136, 3054–3061. [Google Scholar] [CrossRef]
- Lorenzo, J.A.; Naprta, A.; Rao, Y.; Alander, C.; Glaccum, M.; Widmer, M.; Gronowicz, G.; Kalinowski, J.; Pilbeam, C.C. Mice lacking the type I interleukin-1 receptor do not lose bone mass after ovariectomy. Endocrinology 1998, 139, 3022–3025. [Google Scholar] [CrossRef]
- Antonio, L.; Caerels, S.; Jardi, F.; Delaunay, E.; Vanderschueren, D. Testosterone replacement in congenital hypogonadotropic hypogonadism maintains bone density but has only limited osteoanabolic effects. Andrology 2019, 7, 302–306. [Google Scholar] [CrossRef]
- Rochira, V.; Antonio, L.; Vanderschueren, D. EAA clinical guideline on management of bone health in the andrological outpatient clinic. Andrology 2018, 6, 272–285. [Google Scholar] [CrossRef] [PubMed]
- Stanley, H.L.; Schmitt, B.P.; Poses, R.M.; Deiss, W.P. Does hypogonadism contribute to the occurrence of a minimal trauma hip fracture in elderly men? J. Am. Geriatr. Soc. 1991, 39, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Baillie, S.P.; Davison, C.E.; Johnson, F.J.; Francis, R.M. Pathogenesis of vertebral crush fractures in men. Age Ageing 1992, 21, 139–141. [Google Scholar] [CrossRef]
- Kelepouris, N.; Harper, K.D.; Gannon, F.; Kaplan, F.S.; Haddad, J.G. Severe osteoporosis in men. Ann. Intern. Med. 1995, 123, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Fink, H.A.; Ewing, S.K.; Ensrud, K.E.; Barrett-Connor, E.; Taylor, B.C.; Cauley, J.A.; Orwoll, E.S. Association of testosterone and estradiol deficiency with osteoporosis and rapid bone loss in older men. J. Clin. Endocrinol. Metab. 2006, 91, 3908–3915. [Google Scholar] [CrossRef]
- Ryan, C.S.; Petkov, V.I.; Adler, R.A. Osteoporosis in men: The value of laboratory testing. Osteoporos. Int. 2011, 22, 1845–1853. [Google Scholar] [CrossRef]
- Kotwal, N.; Upreti, V.; Nachankar, A.; Hari Kumar, K.V.S. A prospective, observational study of osteoporosis in men. Indian J. Endocrinol. Metab. 2018, 22, 62–66. [Google Scholar]
- Liu, Z.Y.; Yang, Y.; Wen, C.Y.; Rong, L.M. Serum Osteocalcin and Testosterone Concentrations in Adult Males with or without Primary Osteoporosis: A Meta-Analysis. Biomed. Res. Int. 2017, 2017, 9892048. [Google Scholar] [CrossRef] [Green Version]
- Greendale, G.A.; Edelstein, S.; Barrett-Connor, E. Endogenous sex steroids and bone mineral density in older women and men: The Rancho Bernardo Study. J. Bone Miner. Res. 1997, 12, 1833–1843. [Google Scholar] [CrossRef]
- Amin, S.; Zhang, Y.; Sawin, C.T.; Evans, S.R.; Hannan, M.T.; Kiel, D.P.; Wilson, P.W.; Felson, D.T. Association of hypogonadism and estradiol levels with bone mineral density in elderly men from the Framingham study. Ann. Intern. Med. 2000, 133, 951–963. [Google Scholar] [CrossRef]
- Mellström, D.; Johnell, O.; Ljunggren, O.; Eriksson, A.L.; Lorentzon, M.; Mallmin, H.; Holmberg, A.; Redlund-Johnell, I.; Orwoll, E.; Ohlsson, C. Free Testosterone is an Independent Predictor of BMD and Prevalent Fractures in Elderly Men: MrOS Sweden. J. Bone Miner. Res. 2006, 21, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Bjørnerem, A.; Emaus, N.; Berntsen, G.K.; Joakimsen, R.M.; Fønnebø, V.; Wilsgaard, T.; Oian, P.; Seeman, E.; Straume, B. Circulating sex steroids, sex hormone-binding globulin, and longitudinal changes in forearm bone mineral density in postmenopausal women and men: The Tromsø study. Calcif. Tissue Int. 2007, 81, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Kuchuk, N.O.; van Schoor, N.M.; Pluijm, S.M.; Smit, J.H.; de Ronde, W.; Lips, P. The association of sex hormone levels with quantitative ultrasound, bone mineral density, bone turnover and osteoporotic fractures in older men and women. Clin. Endocrinol. (Oxford) 2007, 67, 295–303. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, E.S.; Nielson, C.M.; Marshall, L.M.; Lapidus, J.A.; Barrett-Connor, E.; Ensrud, K.E.; Hoffman, A.R.; Laughlin, G.; Ohlsson, C.; Orwoll, E.S.; et al. The effects of serum testosterone, estradiol, and sex hormone binding globulin levels on fracture risk in older men. J. Clin. Endocrinol. Metab. 2009, 94, 3337–3346. [Google Scholar] [CrossRef] [Green Version]
- Vanderschueren, D.; Pye, S.R.; Venken, K.; Borghs, H.; Gaytant, J.; Huhtaniemi, I.T.; Adams, J.E.; Ward, K.A.; Bartfai, G.; Casanueva, F.F.; et al. EMAS Study Group. Gonadal sex steroid status and bone health in middle-aged and elderly European men. Osteoporos. Int. 2010, 21, 1331–1339. [Google Scholar] [CrossRef]
- Cauley, J.A.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Ensrud, K.E.; Bauer, D.C.; Barrett-Connor, E.; Marshall, L.; Orwoll, E.S.; Osteoporotic Fractures in Men Study (MrOS) Research Group. Sex steroid hormones in older men: Longitudinal associations with 4.5-year change in hip bone mineral density–the osteoporotic fractures in men study. J. Clin. Endocrinol. Metab. 2010, 95, 4314–4323. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.; Kwok, T.; Leung, J.C.; Ohlsson, C.; Vandenput, L.; Leung, P.C. Sex steroids and bone health in older Chinese men. Osteoporos. Int. 2012, 23, 1553–1562. [Google Scholar] [CrossRef]
- Hsu, B.; Seibel, M.J.; Cumming, R.G.; Blyth, F.M.; Naganathan, V.; Bleicher, K.; Le Couteur, D.G.; Waite, L.M.; Handelsman, D.J. Progressive temporal change in serum SHBG, but not in serum testosterone or estradiol, is associated with bone loss and incident fractures in older men: The concord health and ageing in men project. J. Bone Miner. Res. 2016, 31, 2115–2122. [Google Scholar] [CrossRef]
- Gennari, L. Aromatase activity and bone homeostasis in men. J. Clin. Endocrinol. Metab. 2004, 89, 5898–5907. [Google Scholar] [CrossRef]
- Catalano, A.; Gaudio, A.; Agostino, R.M.; Morabito, N.; Bellone, F.; Lasco, A. Trabecular bone score and quantitative ultrasound measurements in the assessment of bone health in breast cancer survivors assuming aromatase inhibitors. J. Endocrinol. Investig. 2019, 42, 1337–1343. [Google Scholar] [CrossRef]
- Zitzmann, M.; Brune, M.; Vieth, V.; Nieschlag, E. Monitoring bone density in hypogonadal men by quantitative phalangeal ultrasound. Bone 2002, 31, 422–429. [Google Scholar] [CrossRef]
- Burnett-Bowie, S.-A.M.; McKay, E.A.; Lee, H.; Leder, B.Z. Effects of aromatase inhibition on bone mineral density and bone turnover in older men with low testosterone levels. J. Clin. Endocrinol. Metab. 2009, 94, 4785–4792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenput, L.; Labrie, F.; Mellström, D.; Swanson, C.; Knutsson, T.; Peeker, R.; Ljunggren, O.; Orwoll, E.; Eriksson, A.L.; Damber, J.E.; et al. Serum Levels of Specific Glucuronidated Androgen Metabolites Predict BMD and Prostate Volume in Elderly Men. J. Bone Miner. Res. 2007, 22, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.M.Y.; Wong, H.; Zhang, N.; Chow, S.K.H.; Chau, W.W.; Wang, J.; Chim, Y.N.; Leung, K.S.; Cheung, W.H. The relationship between sarcopenia and fragility fracture-a systematic review. Osteoporos. Int. 2019, 30, 541–553. [Google Scholar] [CrossRef]
- Tarantino, U.; Piccirilli, E.; Fantini, M.; Baldi, J.; Gasbarra, E.; Bei, R. Sarcopenia and fragility fractures: Molecular and clinical evidence of the bone-muscle interaction. J. Bone Joint. Surg. Am. 2015, 97, 429–437. [Google Scholar] [CrossRef]
- Szulc, P.; Claustrat, B.; Marchand, F.; Delmas, P.D. Increased risk of falls and increased bone resorption in elderly men with partial androgen deficiency: The MINOS study. J. Clin. Endocrinol. Metab. 2003, 88, 5240–5247. [Google Scholar] [CrossRef]
- Kenny, A.M.; Prestwood, K.M.; Marcello, K.M.; Raisz, L.G. Determinants of bone density in healthy older men with low testosterone levels. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M492–M497. [Google Scholar] [CrossRef] [Green Version]
- Tuck, S.P.; Scane, A.C.; Fraser, W.D.; Diver, M.J.; Eastell, R.; Francis, R.M. Sex steroids and bone turnover markers in men with symptomatic vertebral fractures. Bone 2008, 43, 999–1005. [Google Scholar] [CrossRef]
- Mellstrom, D.; Vandenput, L.; Mallmin, H.; Holmberg, A.H.; Lorentzon, M.; Odén, A.; Johansson, H.; Orwoll, E.S.; Labrie, F.; Karlsson, M.K.; et al. Older men with low serum estradiol and high serum SHBG have an increased risk of fractures. J. Bone Miner. Res. 2008, 23, 1552–1560. [Google Scholar] [CrossRef]
- Meier, C.; Nguyen, T.V.; Handelsman, D.J.; Schindler, C.; Kushnir, M.M.; Rockwood, A.L.; Meikle, A.W.; Center, J.R.; Eisman, J.A.; Seibel, M.J. Endogenous sex hormones and incident fracture risk in older men: The Dubbo Osteoporosis Epidemiology Study. Arch. Intern. Med. 2008, 168, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Roddam, A.W.; Appleby, P.; Neale, R.; Dowsett, M.; Folkerd, E.; Tipper, S.; Allen, N.E.; Key, T.J. Association between endogenous plasma hormone concentrations and fracture risk in men and women: The EPIC-Oxford prospective cohort study. J. Bone Miner. Metab. 2009, 27, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Risto, O.; Hammar, E.; Hammar, K.; Fredrikson, M.; Hammar, M.; Wahlström, O. Elderly men with a history of distal radius fracture have significantly lower calcaneal bone density and free androgen index than age-matched controls. Aging Male 2012, 15, 59–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torremadé-Barreda, J.; Rodríguez-Tolrà, J.; Román-Romera, I.; Padró-Miquel, A.; Rius-Moreno, J.; Franco-Miranda, E. Testosterone-deficiency as a risk factor for hip fracture in elderly men. Actas. Urol. Esp. 2013, 37, 142–146. [Google Scholar] [CrossRef]
- Tran, T.S.; Center, J.R.; Seibel, M.J.; Eisman, J.A.; Kushnir, M.M.; Rockwood, A.L.; Nguyen, T.V. Relationship between Serum Testosterone and Fracture Risk in Men: A Comparison of RIA and LC-MS/MS. Clin. Chem. 2015, 61, 1182–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenput, L.; Ohlsson, C. Estrogens as regulators of bone health in men. Nat. Rev. Endocrinol. 2009, 5, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Kenny, A.M.; Kleppinger, A.; Annis, K.; Rathier, M.; Browner, B.; Judge, J.O.; McGee, D. Effects of transdermal testosterone on bone and muscle in older men with low bioavailable testosterone levels, low bone mass, and physical frailty. J. Am. Geriatr. Soc. 2010, 58, 1134–1143. [Google Scholar] [CrossRef]
- Aversa, A.; Bruzziches, R.; Francomano, D.; Greco, E.A.; Fornari, R.; Di Luigi, L.; Lenzi, A.; Migliaccio, S. Effects of long-acting testosterone undecanoate on bone mineral density in middle-aged men with late-onset hypogonadism and metabolic syndrome: Results from a 36 months controlled study. Aging Male 2012, 15, 96–102. [Google Scholar] [CrossRef]
- Wang, Y.J.; Zhan, J.K.; Huang, W.; Wang, Y.; Liu, Y.; Wang, S.; Tan, P.; Tang, Z.Y.; Liu, Y.S. Effects of low-dose testosterone undecanoate treatment on bone mineral density and bone turnover markers in elderly male osteoporosis with low serum testosterone. Int. J. Endocrinol. 2013, 2013, 570413. [Google Scholar] [CrossRef] [Green Version]
- Bouloux, P.M.; Legros, J.J.; Elbers, J.M.; Geurts, T.B.; Kaspers, M.J.; Meehan, A.G.; Meuleman, E.J.; Study 43203 Investigators. Effects of oral testosterone undecanoate therapy on bone mineral density and body composition in 322 aging men with symptomatic testosterone deficiency: A 1 year, a randomized, placebo-controlled, dose-ranging study. Aging Male 2013, 16, 38–47. [Google Scholar] [CrossRef]
- Rodriguez-Tolrà, J.; Torremadé, J.; di Gregorio, S.; Del Rio, L.; Franco, E. Effects of testosterone treatment on bone mineral density in men with testosterone deficiency syndrome. Andrology 2013, 1, 570–575. [Google Scholar] [CrossRef]
- Permpongkosol, S.; Khupulsup, K.; Leelaphiwat, S.; Pavavattananusorn, S.; Thongpradit, S.; Petchthong, T. Effects of 8–year treatment of long-acting testosterone undecanoate on metabolic parameters, urinary symptoms, bone mineral density, and sexual function in men with late-onset hypogonadism. J. Sex. Med. 2016, 13, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Rogol, A.D.; Tkachenko, N.; Bryson, N. Natesto™, a novel testosterone nasal gel, normalizes androgen levels in hypogonadal men. Andrology 2016, 4, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shigehara, K.; Konaka, H.; Koh, E.; Nakashima, K.; Iijima, M.; Nohara, T.; Izumi, K.; Kitagawa, Y.; Kadono, Y.; Sugimoto, K.; et al. Effects of testosterone replacement therapy on hypogonadal men with osteopenia or osteoporosis: A subanalysis of a prospective randomized controlled study in Japan (EARTH study). Aging Male 2017, 20, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Snyder, P.J.; Kopperdahl, D.L.; Stephens-Shields, A.J.; Ellenberg, S.S.; Cauley, J.A.; Ensrud, K.E.; Lewis, C.E.; Barrett-Connor, E.; Schwartz, A.V.; Lee, D.C.; et al. Effect of Testosterone Treatment on Volumetric Bone Density and Strength in Older Men With Low Testosterone: A Controlled Clinical Trial. JAMA Intern. Med. 2017, 177, 471–479. [Google Scholar] [CrossRef]
- Permpongkosol, S.; Tantirangsee, N.; Ratana-olarn, K. Treatment of 161 men with symptomatic late onset hypogonadism with long-acting parenteral testosterone undecanoate: Effects on body composition, lipids, and psychosexual complaints. J. Sex. Med. 2010, 7, 3765–3774. [Google Scholar] [CrossRef]
- Konaka, H.; Sugimoto, K.; Orikasa, H.; Iwamoto, T.; Takamura, T.; Takeda, Y.; Shigehara, K.; Iijima, M.; Koh, E.; Namiki, M.; et al. Effects of long-term androgen replacement therapy on the physical and mental statuses of aging males with late-onset hypogonadism: A multicenter randomized controlled trial in Japan (EARTH Study). Asian. J. Androl. 2016, 18, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Ng Tang Fui, M.; Hoermann, R.; Nolan, B.; Clarke, M.; Zajac, J.D.; Grossmann, M. Effect of testosterone treatment on bone remodelling markers and mineral density in obese dieting men in a randomized clinical trial. Sci. Rep. 2018, 8, 9099. [Google Scholar] [CrossRef]
- Bhasin, S.; Cunningham, G.R.; Hayes, F.J.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Montori, V.M. Testosterone therapy in men with androgen deficiency syndromes: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2010, 95, 2536–2559. [Google Scholar] [CrossRef]
- Watts, N.B.; Adler, R.A.; Bilezikian, J.P.; Drake, M.T.; Eastell, R.; Orwoll, E.S.; Finkelstein, J.S. Osteoporosis in men: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 1802–1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vescini, F.; Attanasio, R.; Balestrieri, A.; Bandeira, F.; Bonadonna, S.; Camozzi, V.; Cassibba, S.; Cesareo, R.; Chiodini, I.; Francucci, C.M.; et al. Italian association of clinical endocrinologists (AME) position statement: Drug therapy of osteoporosis. J. Endocrinol. Investig. 2016, 39, 807–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoppé, E.; Bouvard, B.; Royer, M.; Chappard, D.; Audran, M.; Legrand, E. Is androgen therapy indicated in men with osteoporosis? Joint Bone Spine 2013, 80, 459–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, J.C.; Fowler, S.E.; Detter, J.R.; Sherman, S.S. Combination treatment with estrogen and calcitriol in the prevention of age-related bone loss. J. Clin. Endocrinol. Metab. 2001, 86, 3618–3628. [Google Scholar] [CrossRef]
- Smith, M.R.; Eastham, J.; Gleason, D.M.; Shasha, D.; Tchekmedyian, S.; Zinner, N. Randomized controlled trial of zoledronic acid to prevent bone loss in men receiving androgen deprivation therapy for nonmetastatic prostate cancer. J. Urol. 2003, 169, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Egerdie, B.; Hernández Toriz, N.; Feldman, R.; Tammela, T.L.; Saad, F.; Heracek, J.; Szwedowski, M.; Ke, C.; Kupic, A.; et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N. Engl. J. Med. 2009, 361, 745–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morabito, N.; Gaudio, A.; Lasco, A.; Catalano, A.; Atteritano, M.; Trifiletti, A.; Anastasi, G.; Melloni, D.; Frisina, N. Neridronate prevents bone loss in patients receiving androgen deprivation therapy for prostate cancer. J. Bone Miner. Res. 2004, 19, 1766–1770. [Google Scholar] [CrossRef]
Figure 1.
Molecular rules of testosterone and estrogen in bone metabolism. AR, androgen receptor; ERα, estrogen receptor α; IGF-1, insulin growth factor-1; TGFβ, transforming growth factor-β; IL, interleukins; RANKL, receptor activator of NF-κB ligand; NF-κB, nuclear factor-κB; TNFα, tumor necrotic factor-α.
Figure 1.
Molecular rules of testosterone and estrogen in bone metabolism. AR, androgen receptor; ERα, estrogen receptor α; IGF-1, insulin growth factor-1; TGFβ, transforming growth factor-β; IL, interleukins; RANKL, receptor activator of NF-κB ligand; NF-κB, nuclear factor-κB; TNFα, tumor necrotic factor-α.


{kind=link}
Table 1.
Prevalence of hypogonadism in men with osteopenia or bone fracture.
| Author | Year | Subjects | Prevalence of HG | Reference |
|---|---|---|---|---|
| Stanley | 1991 | 17 with MTHF | 58% | [42] |
| 61 controls | 18% | |||
| Baillie | 1992 | 70 with vertebral fracture | 16% | [43] |
| Kelepouris | 1995 | 47 with atraumatic fracture | 15% | [44] |
| Fink HA | 2006 | 2447 community-dwelling men including 130 with osteoporosis | 7% | [45] |
| Ryan | 2011 | 234 with osteoporosis | 24% | [46] |
| Kotwal N | 2018 | 200 male attendants of patients attending endocrine outpatient department | 35% | [47] |
HG, hypogonadism; MTHF, minimal trauma hip fracture.
Table 2.
The relationship between testosterone and BMD in men.
| Author | Year | Country | Study Subjects | Hormones | Results | Ref |
|---|---|---|---|---|---|---|
| Greendale (Rancho Bernardo Study) | 1997 | USA | 457 women and 534 men (50–89 years) | TT, DHT, E2, E1, BioT | Higher bioavailable (but not total) testosterone levels were associated with higher BMD. | [49] |
| Amin (Framingham Study) | 2000 | USA | 448 men (68–96 years) | TT, E2, LH | Hypogonadism related to aging has little influence on BMD. | [50] |
| Fink | 2006 | USA | 2447 community-dwelling men (>65 years) | TT, E2 | The incidence rates of hip bone loss in men with deficient and normal total testosterone were 22.5% and 8.6%. | [45] |
| Mellström (MrOS Sweden) | 2006 | Sweden | 2908 men (69–80 years) | TT, E2, FT, FE2, SHBG | FT levels were positively correlated with BMD in the hip, femur, and arm but not in the lumbar spine. | [51] |
| Bjørnerem (Tromsø Study) | 2007 | Norway | 927 women (37–80 years), 894 men (25–80 years) | TT, E2, cFT SHBG | The relationship between all gender steroids and bone loss was weak. | [52] |
| Kuchuk NO (Longitudinal Ageing Study Amsterdam) | 2007 | Netherlands | 623 men and 634 women (65–88 years) | TT, E2 SHBG | TT had no correlations with BMD | [53] |
| LeBlanc (MrOS Research) | 2009 | USA | 5995 community-dwelling men (>65 years) | BioT, BioE2 SHBG | The combination of low BioE2, low BaT, and high SHBG was associated with significantly faster rates of BMD loss. | [54] |
| Vanderschueren (EMAS study) | 2010 | Belgium | 3140 men (40–79 years) | TT, FT, E2 SHBG | TT and FT had no correlations with BMD. | [55] |
| Cauley (MrOS Research) | 2010 | USA | 1238 men (cross-sectional) 969 men (longitudinal) >65 years | BioT, BioE2 SHBG | No association existed between BioT and hip BMD loss. | [56] |
| Woo | 2012 | Hong Kong | 1448 men (>65 years) | TT, FT, E2, BioE2, SHBG | TT and FT were not correlated with bone loss. | [57] |
| Hsu (CHAMP Cohort) | 2016 | Australia | 1705, 1367, and 958 men (>70 men) | TT, DHT, E2 E1, SHBG, LH FSH, cFT | Both TT and cFT had no correlations with bone loss. | [58] |
BMD, bone mineral density; TT, total testosterone; DHT, dihydrotestosterone; E2, estradiol; E1, estriol; Bio, bioavailability; LH, luteinizing hormone; FT, free testosterone; FE2, free estradiol; SHBG, sex hormone-binding globulin; cFT, calculated free testosterone; FSH, follicle-stimulating hormone.
Table 3.
The relationship between testosterone and bone fractures risk.
| Author | Year | Country | Study Subjects | Hormones | Results | Ref |
|---|---|---|---|---|---|---|
| Szulc (MINOS study) | 2003 | France | 1040 elderly men (19–85 years) | TT, FT | Hypogonadal men had increased rates of falls and markers of bone resorption. | [66] |
| Kenny | 2005 | USA | 83 community-dwelling white men (>65 years) | BioT | Fifty-two percent of men with low BioT levels had lower BMD and were likely at an increased risk of fracture. | [67] |
| Fink | 2006 | USA | 2447 community-dwelling men (>65 years) | TT, E2 | Prevalence rates of osteoporosis in men with deficient and normal total testosterone were 12.3% and 6.0%. | [45] |
| Mellström (MrOS Sweden) | 2006 | Sweden | 2908 men (69–80 years) | TT, E2, FT, FE2, SHBG | FT levels below the median were independent predictors of prevalent osteoporosis-related fractures and X-ray-verified vertebral fractures. | [51] |
| Tuck | 2008 | UK | 57 men with symptomatic vertebral fractures 57 age-matched controls | FT, BioT, SHBG | Calculated FT was lower in the fracture group than the controls. | [68] |
| Mellstrom (MrOS Sweden) | 2008 | Sweden | 2639 men (69–80 years) | TT, E2, FT, FE2, SHBG | TT and FT were not significantly associated with fracture risk. | [69] |
| Meier (The Dubbo Study) | 2008 | Switzerland | 609 men (>60 years) | TT, E2, SHBG | Lower testosterone increased the risk of osteoporotic fracture, particularly with hip and nonvertebral fractures. | [70] |
| Roddam (EPIC-Oxford Study) | 2009 | UK | 155 men and 281 women | TT, E2, SHBG | There were no associations between fracture risk and testosterone levels. | [71] |
| Risto | 2012 | Sweden | 39 treated for fracture 45 controls | TT, BioT, BioE2 | BioT was a possible marker for increased fracture risk. | [72] |
| Woo | 2012 | Hong Kong | 1448 men (>65 years) | TT, FT, E2, BioE2, SHBG | TT and FT had no correlations with an increased bone fracture. | [57] |
| Torremadé-Barreda | 2013 | Spain | 54 men with hip fracture 54 age-matched controls | TT, FT, BioT | Men with hip fractures had significantly lower calculated FT and BiaT levels. | [73] |
| Hsu (CHAMP Cohort) | 2016 | Australia | 1705, 1367, and 958 men over 70 men | TT, DHT, E2, E1, SHBG, LH FSH, cFT | Both TT and cFT had no correlations with incident fractures. | [58] |
| Tran | 2017 | Australia | 602 men with incident fractures | TT | TT was significantly correlated with the incidence of fracture risk. | [74] |
TT, total testosterone; FT, free testosterone; BioT, bioavailable testosterone; E2, estradiol; FE2, free estradiol; SHBG, sex hormone-binding globulin; BioE2, bioavailable estradiol; DHT, dihydrotestosterone; E1, estriol; LH, luteinizing hormone; FSH, follicle-stimulating hormone; cFT, calculated free testosterone.
Table 4.
The effects of TRT on BMD in hypogonadal men (from papers published since 2010).
| Author | Country | Design | Study Subjects | TRT | Periods | Results | Ref |
|---|---|---|---|---|---|---|---|
| Kenny (2010) | USA | RCT | 131 men with hypogonadism, bone fracture, low BMD, frailty | Transdermal testosterone (5 mg/day) | 12–24 months | TRT could increase axial BMD. | [76] |
| Permpongkosol (2010) | Thailand | Single arm | 161 hypogonadal men | 1000 mg TU (Nebido) | 54–150 weeks | No change in BMD was observed in TRT. | [85] |
| Aversa (2012) | Italy | Case–control | 40 hypogonadal men 20 aged-match control | Intramuscular TU (4 times/year) | 36 months | TRT increased vertebral and femoral BMD. | [77] |
| Wang (2013) | China | RCT | 186 men with osteoporosis and hypogonadism | TU (20 or 40 mg/day) | 24 months | TRT improved the lumbar spine and femoral neck BMD. | [78] |
| Bouloux (2013) | UK | RCT | 322 men with LOH syndrome | Oral TU (80, 160, 240 mg/day) | 1 year | Treatment with oral TU led to BMD improvement. | [79] |
| Rodriguez-Tolrà (2013) | Spain | Single arm | 50 men with LOH syndrome | TG (50 mg/day for 12 months) 1000 mg TU (every 2–3 months from 12–24 months) | 2 years | TRT improved lumbar spine and hip BMD. | [80] |
| Permpongkosol (2016) | Thailand | Single arm | 120 hypogonadal men | 1000 mg TU (Nebido) | 5–8 years | A statistically significant increase was found in vertebral and femoral BMD. | [81] |
| Rogol (2016) | USA | RCT | 306 hypogonadal men | TG (22 or 33 mg) | 90–360 days | BMD improved from baseline by TRT. | [82] |
| Konaka (2016) | Japan | RCT | 334 hypogonadal men | TE (250 mg/4 W) | 12 months | 12-month TRT could not improve BMD. | [86] |
| Shigehara (2017) | Japan | RCT | 74 hypogonadal men with osteopenia | TE (250 mg/4 W) | 12 months | TRT for 12 months could improve BMD. | [83] |
| Snyder (2017) | USA | RCT | 211 hypogonadal men | TG (5 mg/day initially) | 1 year | TRT increased BMD and bone strength, more in trabecula. | [84] |
| Ng Tang Fui (2018) | Australia | RCT | 100 obese men with hypogonadism | TU (1000 mg/0, 6, 26, 36, and 46 weeks) | 56 weeks | No significant changes in the lumbar spine and femoral BMD were observed. | [87] |
TRT, testosterone replacement therapy; BMD, bone mineral density; RCT, randomized controlled study; TU, testosterone undecanoate; TG, testosterone gel; TE, testosterone enanthate; LOH, late-onset hypogonadism.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shigehara, K.; Izumi, K.; Kadono, Y.; Mizokami, A. Testosterone and Bone Health in Men: A Narrative Review. J. Clin. Med. 2021, 10, 530. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030530
AMA Style
Shigehara K, Izumi K, Kadono Y, Mizokami A. Testosterone and Bone Health in Men: A Narrative Review. Journal of Clinical Medicine. 2021; 10(3):530. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030530
Chicago/Turabian StyleShigehara, Kazuyoshi, Kouji Izumi, Yoshifumi Kadono, and Atsushi Mizokami. 2021. "Testosterone and Bone Health in Men: A Narrative Review" Journal of Clinical Medicine 10, no. 3: 530. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030530
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.