
Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Therapy with Direct-Acting Antivirals. A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search and Study Selection
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. HCC Recurrence
3.3. HCC Recurrence after DAA vs. IFN vs. No Intervention
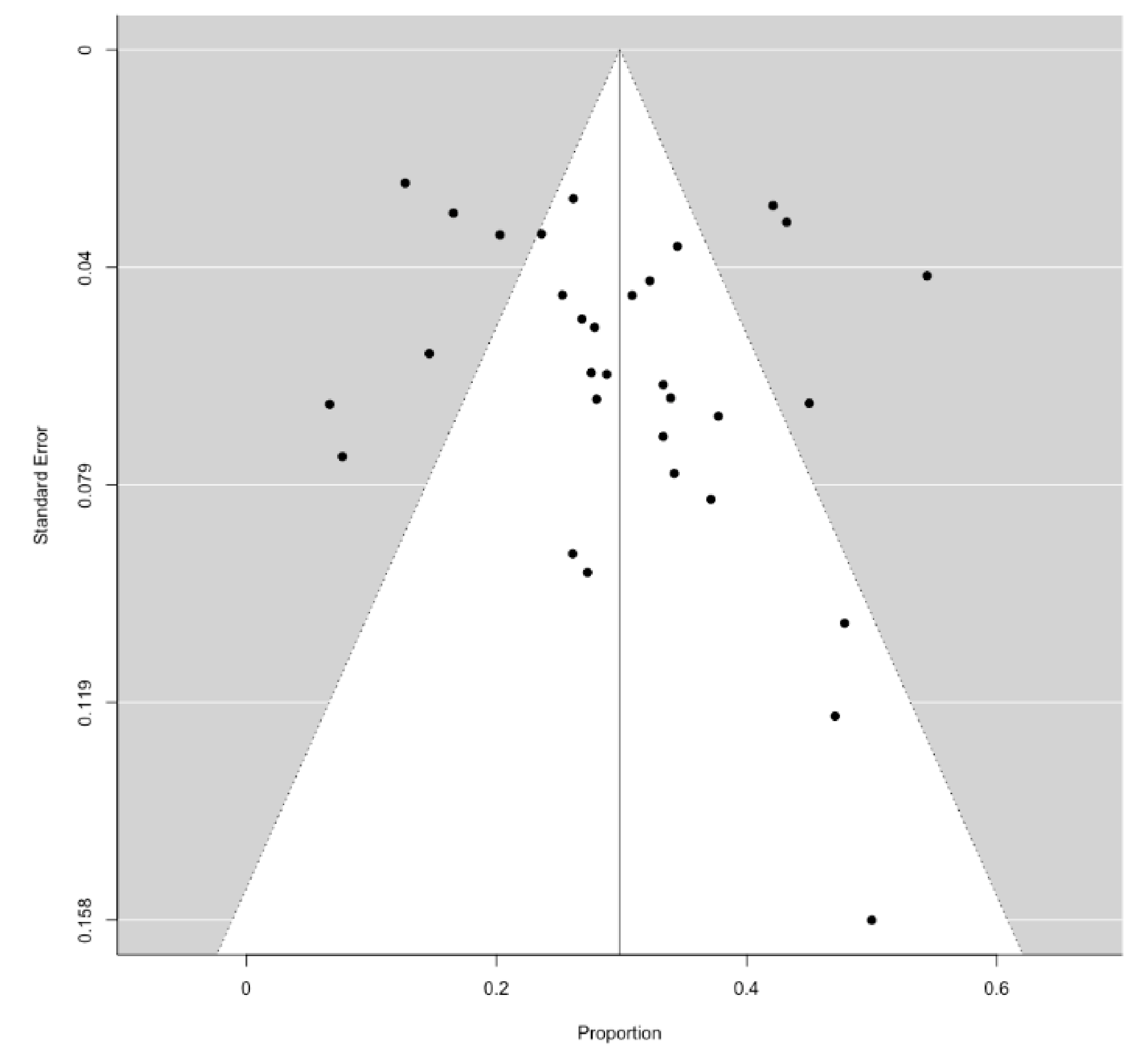
3.4. Study Quality and Publication Bias
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| DAA | direct-acting antivirals |
| HCC | hepatocellular carcinoma |
| HCV | hepatitis C virus |
| PEG-IFN | pegylated interferon |
| PRISMA | Preferred Reporting Items for Systematic Review and Meta-analysis |
| SVR | sustained virological response |
References
- El-Serag, H.B. Epidemiology of Viral Hepatitis and Hepatocellular Carcinoma. Gastroenterology 2012, 142, 1264–1273.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, S.K.; Steel, J.L.; Chen, H.-W.; DeMateo, D.J.; Cardinal, J.; Behari, J.; Humar, A.; Marsh, J.W.; Geller, D.A.; Tsung, A. Outcomes of Curative Treatment for Hepatocellular Cancer in Nonalcoholic Steatohepatitis versus Hepatitis C and Alcoholic Liver Disease. Hepatology 2012, 55, 1809–1819. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.A.; Rutledge, S.M.; Chung, R.T. Direct-Acting Antiviral Treatment for Hepatitis C. Lancet 2019, 393, 1392–1394. [Google Scholar] [CrossRef]
- Singal, A.G.; Volk, M.L.; Jensen, D.; Di Bisceglie, A.M.; Schoenfeld, P.S. A Sustained Viral Response Is Associated with Reduced Liver-Related Morbidity and Mortality in Patients with Hepatitis C Virus. Clin. Gastroenterol. Hepatol. 2010, 8, 280–288.e1. [Google Scholar] [CrossRef]
- Hsu, C.-S.; Chao, Y.-C.; Lin, H.H.; Chen, D.-S.; Kao, J.-H. Systematic Review: Impact of Interferon-Based Therapy on HCV-Related Hepatocellular Carcinoma. Sci. Rep. 2015, 5, 9954. [Google Scholar] [CrossRef] [Green Version]
- Waziry, R.; Hajarizadeh, B.; Grebely, J.; Amin, J.; Law, M.; Danta, M.; George, J.; Dore, G.J. Hepatocellular Carcinoma Risk Following Direct-Acting Antiviral HCV Therapy: A Systematic Review, Meta-Analyses, and Meta-Regression. J. Hepatol. 2017, 67, 1204–1212. [Google Scholar] [CrossRef]
- Conti, F.; Buonfiglioli, F.; Scuteri, A.; Crespi, C.; Bolondi, L.; Caraceni, P.; Foschi, F.G.; Lenzi, M.; Mazzella, G.; Verucchi, G.; et al. Early Occurrence and Recurrence of Hepatocellular Carcinoma in HCV-Related Cirrhosis Treated with Direct-Acting Antivirals. J. Hepatol. 2016, 65, 727–733. [Google Scholar] [CrossRef]
- Saraiya, N.; Yopp, A.C.; Rich, N.E.; Odewole, M.; Parikh, N.D.; Singal, A.G. Systematic Review with Meta-Analysis: Recurrence of Hepatocellular Carcinoma Following Direct-Acting Antiviral Therapy. Aliment. Pharmacol. Ther. 2018, 48, 127–137. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 January 2021).
- Harbord, R.M.; Egger, M.; Sterne, J.A.C. A Modified Test for Small-Study Effects in Meta-Analyses of Controlled Trials with Binary Endpoints. Stat. Med. 2006, 25, 3443–3457. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- ANRS Collaborative Study Group on Hepatocellular. Lack of Evidence of an Effect of Direct-Acting Antivirals on the Recurrence of Hepatocellular Carcinoma: Data from Three ANRS Cohorts. J. Hepatol. 2016, 65, 734–740. [Google Scholar] [CrossRef] [Green Version]
- Bielen, R.; Moreno, C.; Van Vlierberghe, H.; Bourgeois, S.; Mulkay, J.-P.; Vanwolleghem, T.; Verlinden, W.; Brixco, C.; Decaestecker, J.; de Galocsy, C.; et al. The Risk of Early Occurrence and Recurrence of Hepatocellular Carcinoma in Hepatitis C-Infected Patients Treated with Direct-Acting Antivirals with and without Pegylated Interferon: A Belgian Experience. J. Viral Hepat. 2017, 24, 976–981. [Google Scholar] [CrossRef]
- Cabibbo, G.; Petta, S.; Calvaruso, V.; Cacciola, I.; Cannavò, M.R.; Madonia, S.; Distefano, M.; Larocca, L.; Prestileo, T.; Tinè, F.; et al. Is Early Recurrence of Hepatocellular Carcinoma in HCV Cirrhotic Patients Affected by Treatment with Direct-Acting Antivirals? A Prospective Multicentre Study. Aliment. Pharmacol. Ther. 2017, 46, 688–695. [Google Scholar] [CrossRef]
- Chan, P.P.Y.; Levy, M.T.; Shackel, N.; Davison, S.A.; Prakoso, E. Hepatocellular Carcinoma Incidence Post Direct-Acting Antivirals in Hepatitis C-Related Advanced Fibrosis/Cirrhosis Patients in Australia. Hepatobiliary Pancreat. Dis. Int. 2020, 19, 541–546. [Google Scholar] [CrossRef]
- Chi, C.-T.; Chen, C.-Y.; Su, C.-W.; Chen, P.-Y.; Chu, C.-J.; Lan, K.-H.; Lee, I.-C.; Hou, M.-C.; Huang, Y.-H. Direct-Acting Antivirals for Patients with Chronic Hepatitis C and Hepatocellular Carcinoma in Taiwan. J. Microbiol. Immunol. Infect. 2019. [Google Scholar] [CrossRef]
- Degasperi, E.; D’Ambrosio, R.; Iavarone, M.; Sangiovanni, A.; Aghemo, A.; Soffredini, R.; Borghi, M.; Lunghi, G.; Colombo, M.; Lampertico, P. Factors Associated with Increased Risk of De Novo or Recurrent Hepatocellular Carcinoma in Patients with Cirrhosis Treated With Direct-Acting Antivirals for HCV Infection. Clin. Gastroenterol. Hepatol. 2019, 17, 1183–1191.e7. [Google Scholar] [CrossRef] [Green Version]
- El Kassas, M.; Funk, A.L.; Salaheldin, M.; Shimakawa, Y.; Eltabbakh, M.; Jean, K.; El Tahan, A.; Sweedy, A.T.; Afify, S.; Youssef, N.F.; et al. Increased Recurrence Rates of Hepatocellular Carcinoma after DAA Therapy in a Hepatitis C-Infected Egyptian Cohort: A Comparative Analysis. J. Viral Hepat. 2018, 25, 623–630. [Google Scholar] [CrossRef]
- Ikeda, K.; Kawamura, Y.; Kobayashi, M.; Kominami, Y.; Fujiyama, S.; Sezaki, H.; Hosaka, T.; Akuta, N.; Saitoh, S.; Suzuki, F.; et al. Direct-Acting Antivirals Decreased Tumor Recurrence After Initial Treatment of Hepatitis C Virus-Related Hepatocellular Carcinoma. Dig. Dis. Sci. 2017, 62, 2932–2942. [Google Scholar] [CrossRef]
- Kogiso, T.; Sagawa, T.; Kodama, K.; Taniai, M.; Katagiri, S.; Egawa, H.; Yamamoto, M.; Tokushige, K. Hepatocellular Carcinoma after Direct-Acting Antiviral Drug Treatment in Patients with Hepatitis C Virus. JGH Open 2019, 3, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, Y.-H.; Wang, J.-H.; Chang, K.-C.; Hung, C.-H.; Lu, S.-N.; Hu, T.-H.; Yen, Y.-H.; Kee, K.-M.; Chen, C.-H. The Influence of Direct-Acting Antivirals in Hepatitis C Virus Related Hepatocellular Carcinoma after Curative Treatment. Investig. New Drugs 2020, 38, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Lashen, S.A.; Shamseya, M.M.; Madkour, M.A. Hepatocellular Carcinoma Occurrence/Recurrence after Direct-Acting Antivirals for Hepatitis C in Egyptian Cohort: Single-Center Experience. Dig. Dis. 2019, 37, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-C.; Lin, Y.-S.; Chang, C.-W.; Chang, C.-W.; Wang, T.-E.; Wang, H.-Y.; Chen, M.-J. Impact of Direct-Acting Antiviral Therapy for Hepatitis C-Related Hepatocellular Carcinoma. PLoS ONE 2020, 15, e0233212. [Google Scholar] [CrossRef]
- Lithy, R.M.; Elbaz, T.; H Abdelmaksoud, A.; M Nabil, M.; Rashed, N.; Omran, D.; Kaseb, A.O.; O Abdelaziz, A.; I Shousha, H. Survival and Recurrence Rates of Hepatocellular Carcinoma after Treatment of Chronic Hepatitis C Using Direct Acting Antivirals. Eur. J. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef]
- Lleo, A.; Aglitti, A.; Aghemo, A.; Maisonneuve, P.; Bruno, S.; Persico, M.; Rendina, M.; Ciancio, A.; Lampertico, P.; Brunetto, M.R.; et al. Predictors of Hepatocellular Carcinoma in HCV Cirrhotic Patients Treated with Direct Acting Antivirals. Dig. Liver Dis. 2019, 51, 310–317. [Google Scholar] [CrossRef]
- Miuma, S.; Miyamoto, J.; Taura, N.; Fukushima, M.; Sasaki, R.; Haraguchi, M.; Shibata, H.; Sato, S.; Miyaaki, H.; Nakao, K. Influence of Interferon-Free Direct-Acting Antiviral Therapy on Primary Hepatocellular Carcinoma Recurrence: A Landmark Time Analysis and Time-Dependent Extended Cox Proportional Hazards Model Analysis. Intern. Med. 2020, 59, 901–907. [Google Scholar] [CrossRef] [Green Version]
- Nagaoki, Y.; Imamura, M.; Nishida, Y.; Daijo, K.; Teraoka, Y.; Honda, F.; Nakamura, Y.; Morio, K.; Fujino, H.; Nakahara, T.; et al. The Impact of Interferon-Free Direct-Acting Antivirals on Clinical Outcome after Curative Treatment for Hepatitis C Virus-Associated Hepatocellular Carcinoma: Comparison with Interferon-Based Therapy. J. Med. Virol. 2019, 91, 650–658. [Google Scholar] [CrossRef]
- Nagata, H.; Nakagawa, M.; Asahina, Y.; Sato, A.; Asano, Y.; Tsunoda, T.; Miyoshi, M.; Kaneko, S.; Otani, S.; Kawai-Kitahata, F.; et al. Effect of Interferon-Based and -Free Therapy on Early Occurrence and Recurrence of Hepatocellular Carcinoma in Chronic Hepatitis C. J. Hepatol. 2017, 67, 933–939. [Google Scholar] [CrossRef]
- Nishibatake Kinoshita, M.; Minami, T.; Tateishi, R.; Wake, T.; Nakagomi, R.; Fujiwara, N.; Sato, M.; Uchino, K.; Enooku, K.; Nakagawa, H.; et al. Impact of Direct-Acting Antivirals on Early Recurrence of HCV-Related HCC: Comparison with Interferon-Based Therapy. J. Hepatol. 2019, 70, 78–86. [Google Scholar] [CrossRef]
- Ochi, H.; Hiraoka, A.; Hirooka, M.; Koizumi, Y.; Amano, M.; Azemoto, N.; Watanabe, T.; Yoshida, O.; Tokumoto, Y.; Mashiba, T.; et al. Direct-Acting Antivirals Improve Survival and Recurrence Rates after Treatment of Hepatocellular Carcinoma within the Milan Criteria. J. Gastroenterol. 2020. [Google Scholar] [CrossRef]
- Ogawa, E.F.N.; Kyushu University Liver Disease Study (KULDS) Group. Short-term risk of hepatocellular carcinoma after hepatitis C virus eradication following direct-acting anti-viral treatment. Aliment. Pharmacol. Ther. 2018, 47, 104–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ooka, Y.; Miho, K.; Shuntaro, O.; Nakamura, M.; Ogasawara, S.; Suzuki, E.; Yasui, S.; Chiba, T.; Arai, M.; Kanda, T.; et al. Prediction of the Very Early Occurrence of HCC Right after DAA Therapy for HCV Infection. Hepatol. Int. 2018, 12, 523–530. [Google Scholar] [CrossRef]
- Preda, C.M.; Baicus, C.; Sandra, I.; Oproiu, A.; Manuc, T.; Constantinescu, I.; Gavrila, D.; Diculescu, M.; Dumitru, R.; Vasilescu, C.; et al. Recurrence Rate of Hepatocellular Carcinoma in Patients with Treated Hepatocellular Carcinoma and Hepatitis C Virus-Associated Cirrhosis after Ombitasvir/Paritaprevir/Ritonavir+dasabuvir+ribavirin Therapy. UE Gastroenterol. J. 2019, 7, 699–708. [Google Scholar] [CrossRef]
- Reig, M.; Mariño, Z.; Perelló, C.; Iñarrairaegui, M.; Ribeiro, A.; Lens, S.; Díaz, A.; Vilana, R.; Darnell, A.; Varela, M.; et al. Unexpected High Rate of Early Tumor Recurrence in Patients with HCV-Related HCC Undergoing Interferon-Free Therapy. J. Hepatol. 2016, 65, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Rinaldi, L.; Rinaldi, L.; Di Francia, R.; Coppola, N.; Guerrera, B.; Imparato, M.; Monari, C.; Nevola, R.; Rosato, V.; Fontanella, L.; et al. Hepatocellular carcinoma in HCV Cirrhosis after viral clearance with direct acting antiviral therapy: Preliminary evidence and possible meanings. WCRJ 2016, 3, e748. [Google Scholar]
- Sangiovanni, A.; Alimenti, E.; Gattai, R.; Filomia, R.; Parente, E.; Valenti, L.; Marzi, L.; Pellegatta, G.; Borgia, G.; Gambato, M.; et al. Undefined/Non-Malignant Hepatic Nodules Are Associated with Early Occurrence of HCC in DAA-Treated Patients with HCV-Related Cirrhosis. J. Hepatol. 2020, 73, 593–602. [Google Scholar] [CrossRef]
- Singal, A.G.; Rich, N.E.; Mehta, N.; Branch, A.; Pillai, A.; Hoteit, M.; Volk, M.; Odewole, M.; Scaglione, S.; Guy, J.; et al. Direct-Acting Antiviral Therapy Not Associated with Recurrence of Hepatocellular Carcinoma in a Multicenter North American Cohort Study. Gastroenterology 2019, 156, 1683–1692.e1. [Google Scholar] [CrossRef]
- Tahata, Y.; Sakamori, R.; Urabe, A.; Yamada, R.; Ohkawa, K.; Hiramatsu, N.; Hagiwara, H.; Oshita, M.; Imai, Y.; Kodama, T.; et al. Clinical Outcomes of Direct-Acting Antiviral Treatments for Patients with Hepatitis C after Hepatocellular Carcinoma Are Equivalent to Interferon Treatment. Hepatol. Res. 2020, 50, 1118–1127. [Google Scholar] [CrossRef]
- Virlogeux, V.; Pradat, P.; Hartig-Lavie, K.; Bailly, F.; Maynard, M.; Ouziel, G.; Poinsot, D.; Lebossé, F.; Ecochard, M.; Radenne, S.; et al. Direct-Acting Antiviral Therapy Decreases Hepatocellular Carcinoma Recurrence Rate in Cirrhotic Patients with Chronic Hepatitis C. Liver Int. 2017, 37, 1122–1127. [Google Scholar] [CrossRef]
- Yoshimasu, Y.; Furuichi, Y.; Kasai, Y.; Takeuchi, H.; Sugimoto, K.; Nakamura, I.; Itoi, T. Predictive Factors for Hepatocellular Carcinoma Occurrence or Recurrence after Direct-Acting Antiviral Agents in Patients with Chronic Hepatitis C. J. Gastrointest. Liver Dis 2019, 28, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Zou, W.Y.; Choi, K.; Kramer, J.R.; Yu, X.; Cao, Y.; El-Serag, H.B.; Kanwal, F. Risk of Hepatocellular Cancer Recurrence in Hepatitis C Virus+ Patients Treated with Direct-Acting Antiviral Agents. Dig. Dis. Sci. 2019, 64, 3328–3336. [Google Scholar] [CrossRef] [PubMed]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H.; European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C: Final Update of the Series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef] [PubMed]
- Probst, A.; Dang, T.; Bochud, M.; Egger, M.; Negro, F.; Bochud, P.-Y. Role of Hepatitis C Virus Genotype 3 in Liver Fibrosis Progression--a Systematic Review and Meta-Analysis. J. Viral Hepat. 2011, 18, 745–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.-H.; Yang, H.-I.; Lu, S.-N.; Jen, C.-L.; You, S.-L.; Wang, L.-Y.; L’Italien, G.; Chen, C.-J.; Yuan, Y.; REVEAL-HCV Study Group. Hepatitis C Virus Genotype 1b Increases Cumulative Lifetime Risk of Hepatocellular Carcinoma. Int. J. Cancer 2014, 135, 1119–1126. [Google Scholar] [CrossRef]
- Blach, S.; Zeuzem, S.; Manns, M.; Altraif, I.; Duberg, A.-S.; Muljono, D.H.; Waked, I.; Alavian, S.M.; Lee, M.-H.; Negro, F.; et al. Global Prevalence and Genotype Distribution of Hepatitis C Virus Infection in 2015: A Modelling Study. Lancet Gastroenterol. Hepatol. 2017, 2, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M.H.; Whittemore, A.S.; Garcia, R.T.; Tawfeek, S.A.; Ning, J.; Lam, S.; Wright, T.L.; Keeffe, E.B. Role of Ethnicity in Risk for Hepatocellular Carcinoma in Patients with Chronic Hepatitis C and Cirrhosis. Clin. Gastroenterol. Hepatol. 2004, 2, 820–824. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section/Topic | # | Checklist Item | Reported on Page |
|---|---|---|---|
| Title | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary including, as applicable, background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; and systematic review registration number. | 1 |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 1,2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 2 |
| Methods | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, and if and where it can be accessed (e.g., web address), and, if available, provide registration information including registration number. | - |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS and length of follow-up) and report characteristics (e.g., years considered, language, and publication status) used as criteria for eligibility, giving rationale. | 2–4 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 2–4 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 2–4 |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 2–4 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, and in duplicate) and any processes for obtaining and confirming data from investigators. | 2–4 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS and funding sources) and any assumptions and simplifications made. | 2–4 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 2–4 |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio and difference in means). | 4 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | 4 |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias and selective reporting within studies). | 4 |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, metaregression), if done, indicating which were pre-specified. | 4 |
| Results | |||
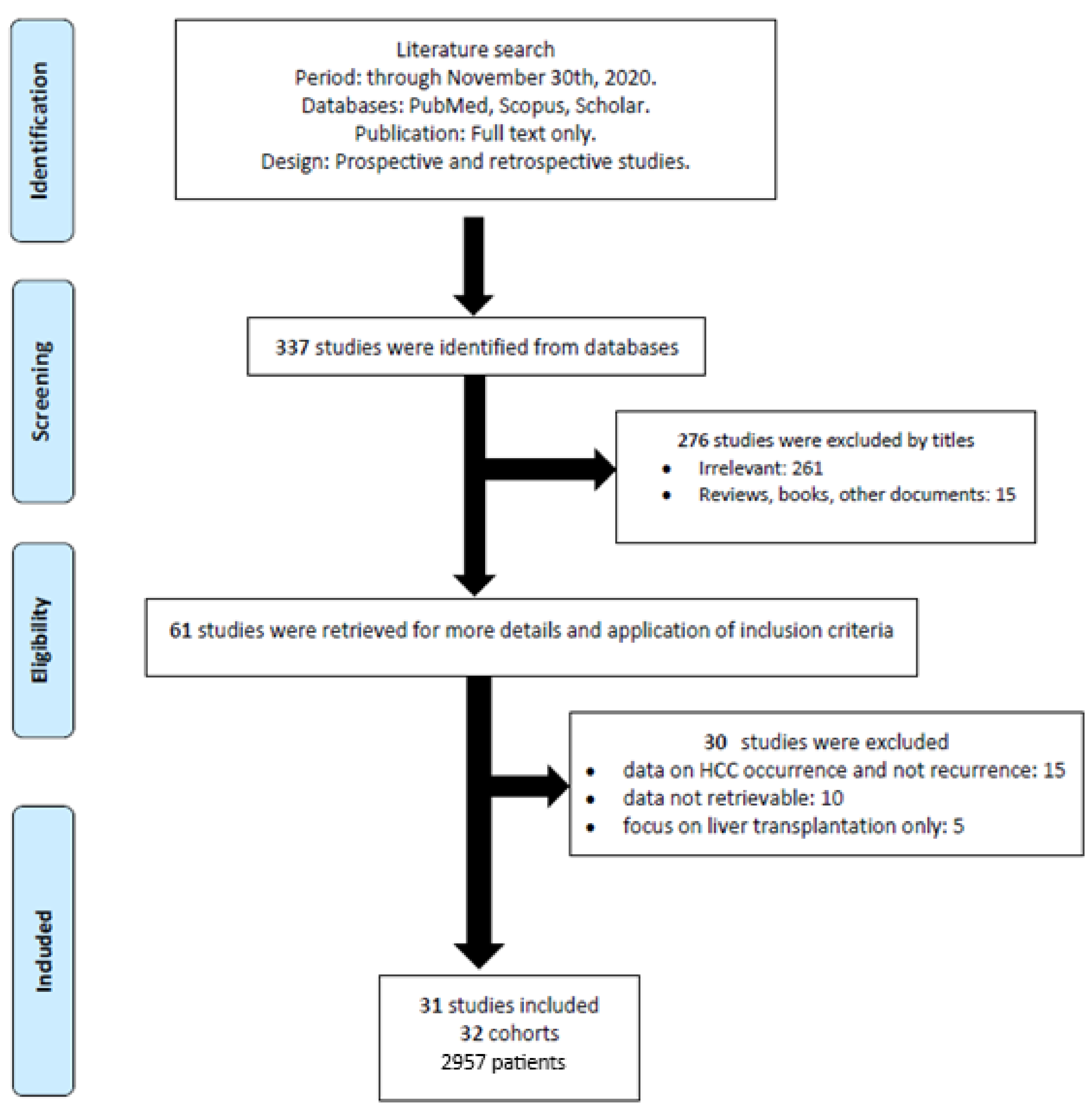
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 4,5, Figure 1 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 4,5, Table 2 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see Item 12). | Table 3 |
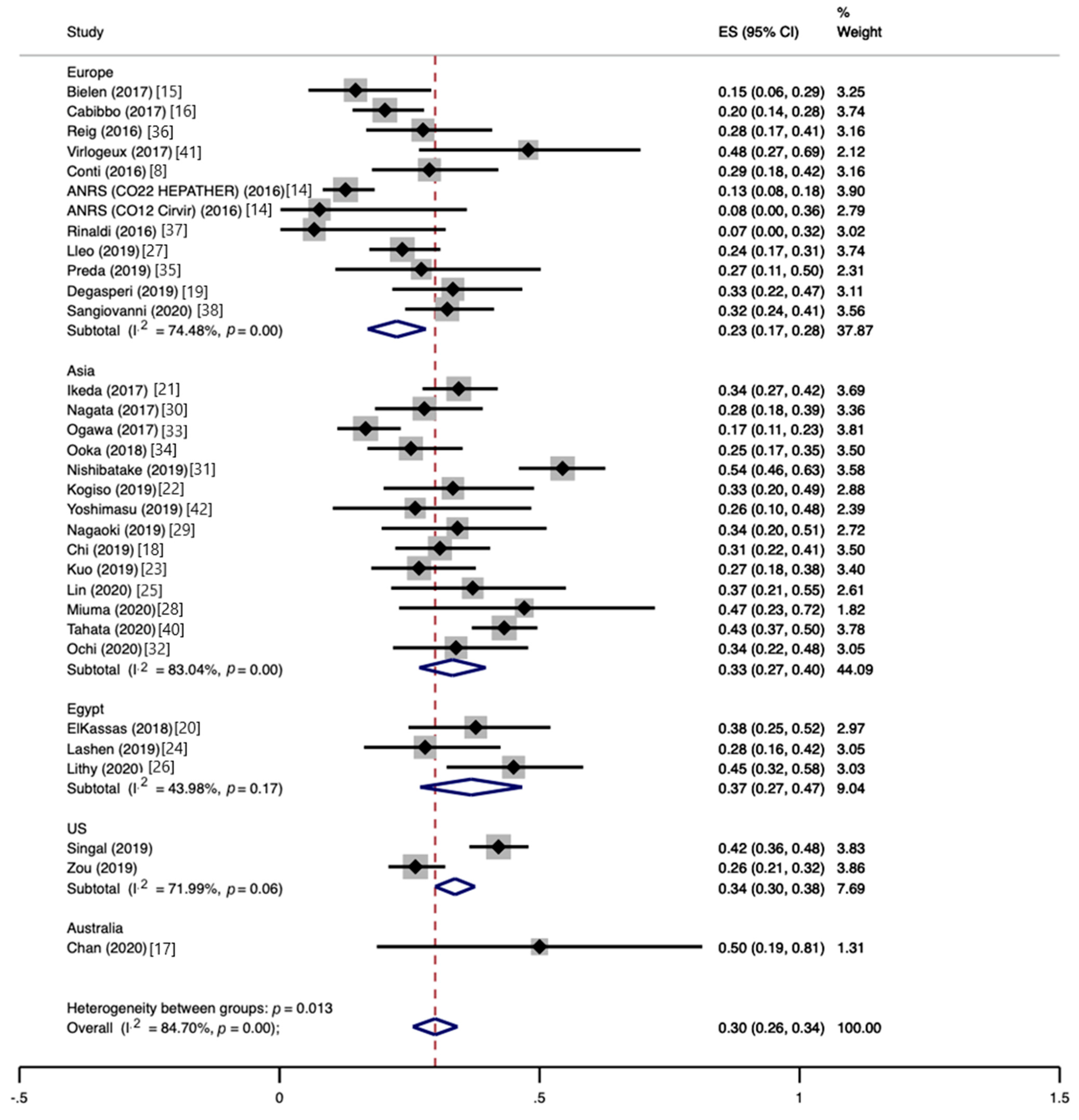
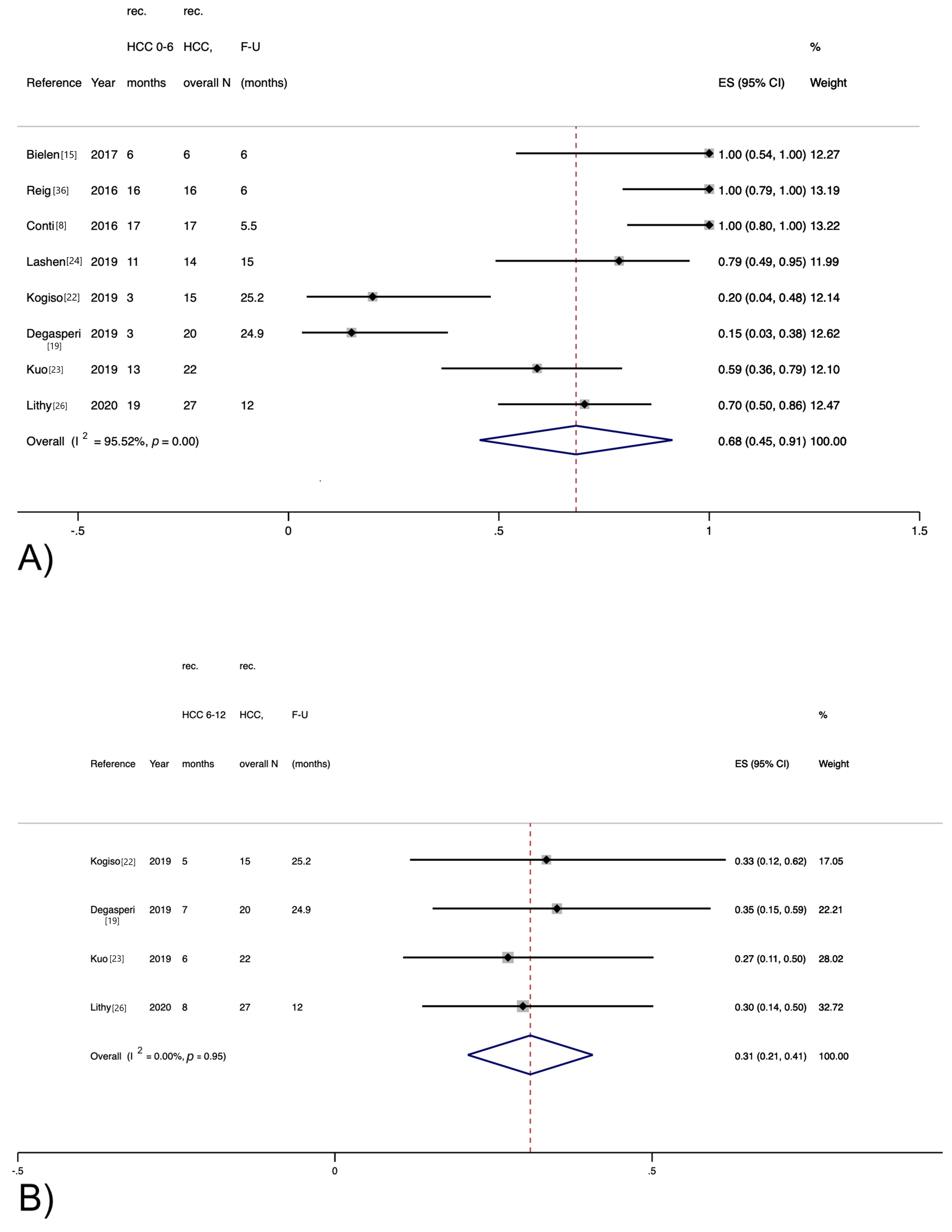
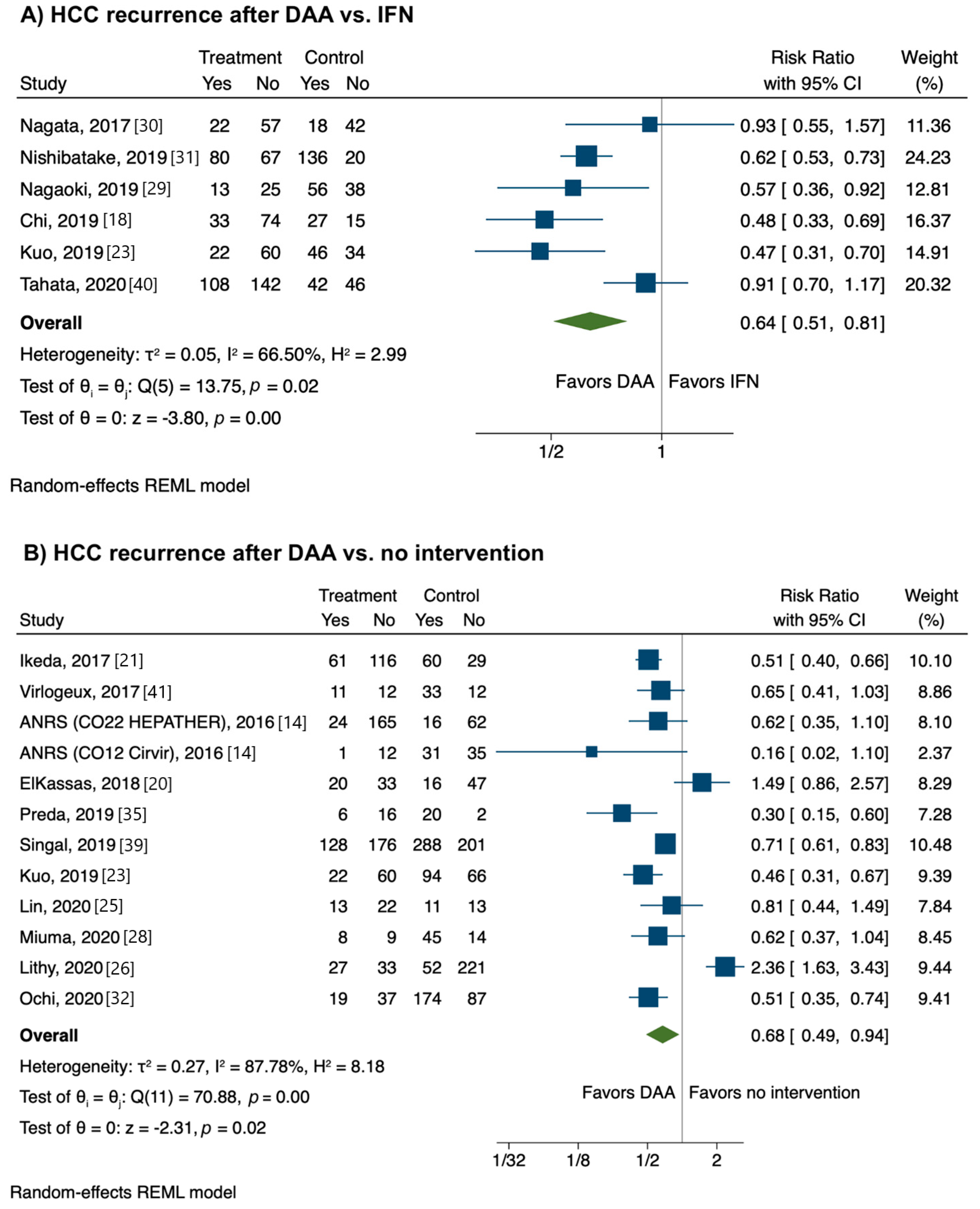
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study, (a) simple summary data for each intervention group, and (b) effect estimates and confidence intervals, ideally with a forest plot. | Figures 2–4 |
| Synthesis of results | 21 | Present results of each meta-analysis performed, including confidence intervals and measures of consistency. | Figures 2–4 |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | 10, Figure 5 |
| Additional analysis | 23 | Give results of additional analyses, if performed (e.g., sensitivity or subgroup analyses, and metaregression (see Item 16)). | 10 |
| Discussion | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policymakers). | 11 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review level (e.g., incomplete retrieval of identified research, and reporting bias). | 12 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 11–13 |
| Funding | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data), and role of funders for the systematic review. | 13 |
| Reference | Year | Study Design | Country | n Patients Treated with DAA | Mean Time from HCC Treatment to DAA (Months) | Mean Follow-Up (Months) |
|---|---|---|---|---|---|---|
| Bielen [15] | 2017 | retrospective | Belgium | 41 | 33 | 6 |
| Cabibbo [16] | 2017 | prospective | Italy | 143 | 1.8 | 9.1 |
| Ikeda [21] | 2017 | retrospective | Japan | 177 | 20.1 | 20.4 |
| Nagata [30] | 2017 | retrospective | Japan | 79 | 22.3 | |
| Ogawa [33] | 2017 | prospective | Japan | 157 | 35.2 | 16.6 |
| Reig [36] | 2016 | retrospective | Spain | 58 | 12.8 | 6 |
| Virlogeux [41] | 2017 | retrospective | France | 23 | 13 | 12 |
| Conti [8] | 2016 | retrospective | Italy | 59 | 17.6 | 5.5 |
| ANRS [14] (CO22 HEPATHER) | 2016 | retrospective | France | 189 | 19.2 | 20.2 |
| ANRS [14] (CO12 Cirvir) | 2016 | retrospective | France | 13 | ||
| Rinaldi [37] | 2016 | retrospective | Italy | 15 | 11.3 | 3 |
| El Kassas [20] | 2018 | prospective | Egypt | 53 | ||
| Ooka [34] | 2018 | prospective | Japan | 95 | 7.4 | |
| Lashen [24] | 2019 | retrospective | Egypt | 50 | 5.18 | 15 |
| Lleo [27] | 2019 | retrospective | Italy | 161 | 12 | |
| Preda [35] | 2019 | prospective | Romania | 22 | 27.7 | 49.7 |
| Nishibatake Kinoshita [31] | 2019 | retrospective | Japan | 147 | 7.1 | 1.8 |
| Kogiso [22] | 2019 | retrospective | Japan | 45 | 36.1 | 25.2 |
| Yoshimasu [42] | 2019 | retrospective | Japan | 23 | 16.5 | |
| Nagaoki [29] | 2019 | retrospective | Japan | 38 | 35.2 | |
| Degasperi [19] | 2019 | retrospective | Italy | 60 | 24.9 | |
| Singal [39] | 2019 | retrospective | USA and Canada | 304 | 6.8 | 12.3 |
| Zou [43] | 2019 | retrospective | USA | 264 | 30.9 | 23.3 |
| Chi [18] | 2019 | retrospective | Taiwan | 107 | 14.5 | 32.3 |
| Kuo [23] | 2019 | retrospective | Taiwan | 82 | 30.7 | |
| Chan [17] | 2020 | retrospective | Australia | 10 | 18.3 | 23.8 |
| Lin [25] | 2020 | retrospective | Taiwan | 35 | 29.3 | 18.9 |
| Miuma [28] | 2020 | retrospective | Japan | 17 | 26.4 | |
| Sangiovanni [38] | 2020 | prospective | Italy | 124 | 20.2 | 15.1 |
| Tahata [40] | 2020 | retrospective | Japan | 250 | 21.4 | 27 |
| Lithy [26] | 2020 | prospective | Egypt | 60 | 12 | |
| Ochi [32] | 2020 | retrospective | Japan | 56 | 5.7 | 39.9 |
| Reference | Representative Cohort | Ascertainment of Exposure | Outcome Not Present at Start | Outcome Assessment | Follow-Up Period | Follow-Up Adequacy |
|---|---|---|---|---|---|---|
| Bielen [15] | * | * | High | High | * | High |
| Cabibbo [16] | * | * | * | * | High | Unknown |
| Ikeda [21] | * | * | Medium | Medium | * | * |
| Nagata [30] | * | * | High | Medium | * | Unknown |
| Ogawa [33] | * | * | * | * | * | Unknown |
| Reig [36] | * | * | * | Medium | High | * |
| Virlogeux [41] | * | * | * | Medium | * | High |
| Conti [8] | * | * | Medium | Medium | High | * |
| ANRS [14] (CO22 HEPATHER) | * | * | Medium | High | * | Unknown |
| ANRS [14] (CO12 Cirvir) | * | * | Medium | High | * | Unknown |
| Rinaldi [37] | * | * | * | Medium | High | Unknown |
| El Kassas [20] | * | * | High | High | Unknown | Unknown |
| Ooka [34] | * | * | High | High | Medium | High |
| Lashen [24] | * | * | High | * | * | * |
| Lleo [27] | * | * | * | High | * | Medium |
| Preda [35] | High | * | * | High | * | High |
| Nishibatake Kinoshita [31] | * | * | Medium | High | High | * |
| Kogiso [22] | * | * | * | High | * | Unknown |
| Yoshimasu [42] | High | * | High | High | * | * |
| Nagaoki [29] | * | * | * | Medium | * | * |
| Degasperi [19] | * | * | High | High | * | * |
| Singal [39] | * | * | Medium | * | * | Unknown |
| Zou [43] | * | * | * | * | * | High |
| Chi [18] | * | * | * | * | * | * |
| Kuo [23] | * | * | * | * | Unknown | * |
| Chan [17] | High | * | * | High | * | High |
| Lin [25] | * | * | * | * | * | * |
| Miuma [28] | High | * | * | High | Unknown | Unknown |
| Sangiovanni [38] | * | * | * | * | * | * |
| Tahata [40] | * | * | * | Medium | * | Medium |
| Lithy [26] | * | * | High | High | * | * |
| Ochi [32] | * | * | Unknown | High | * | Medium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frazzoni, L.; Sikandar, U.; Metelli, F.; Sadalla, S.; Mazzella, G.; Bazzoli, F.; Fuccio, L.; Azzaroli, F. Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Therapy with Direct-Acting Antivirals. A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1694. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10081694
Frazzoni L, Sikandar U, Metelli F, Sadalla S, Mazzella G, Bazzoli F, Fuccio L, Azzaroli F. Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Therapy with Direct-Acting Antivirals. A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(8):1694. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10081694
Chicago/Turabian StyleFrazzoni, Leonardo, Usama Sikandar, Flavio Metelli, Sinan Sadalla, Giuseppe Mazzella, Franco Bazzoli, Lorenzo Fuccio, and Francesco Azzaroli. 2021. "Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Therapy with Direct-Acting Antivirals. A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 8: 1694. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10081694