
Validity and Usage of the Seasonal Pattern Assessment Questionnaire (SPAQ) in a French Population of Patients with Depression, Bipolar Disorders and Controls

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Measures
2.2.1. SPAQ
2.2.2. Subsidiary Measures
2.3. Statistical Analyses
2.3.1. Confirmatory Factor Analyses
2.3.2. Month by Month Variation of the GSS Dimensions
2.3.3. Association between GSS, Questionnaires and Diagnosis
2.3.4. Association between Diagnosis and Type of Seasonality
3. Results
3.1. Confirmatory Factor Analysis of the GSS
3.2. Association between GSS, Questionnaires and Diagnosis
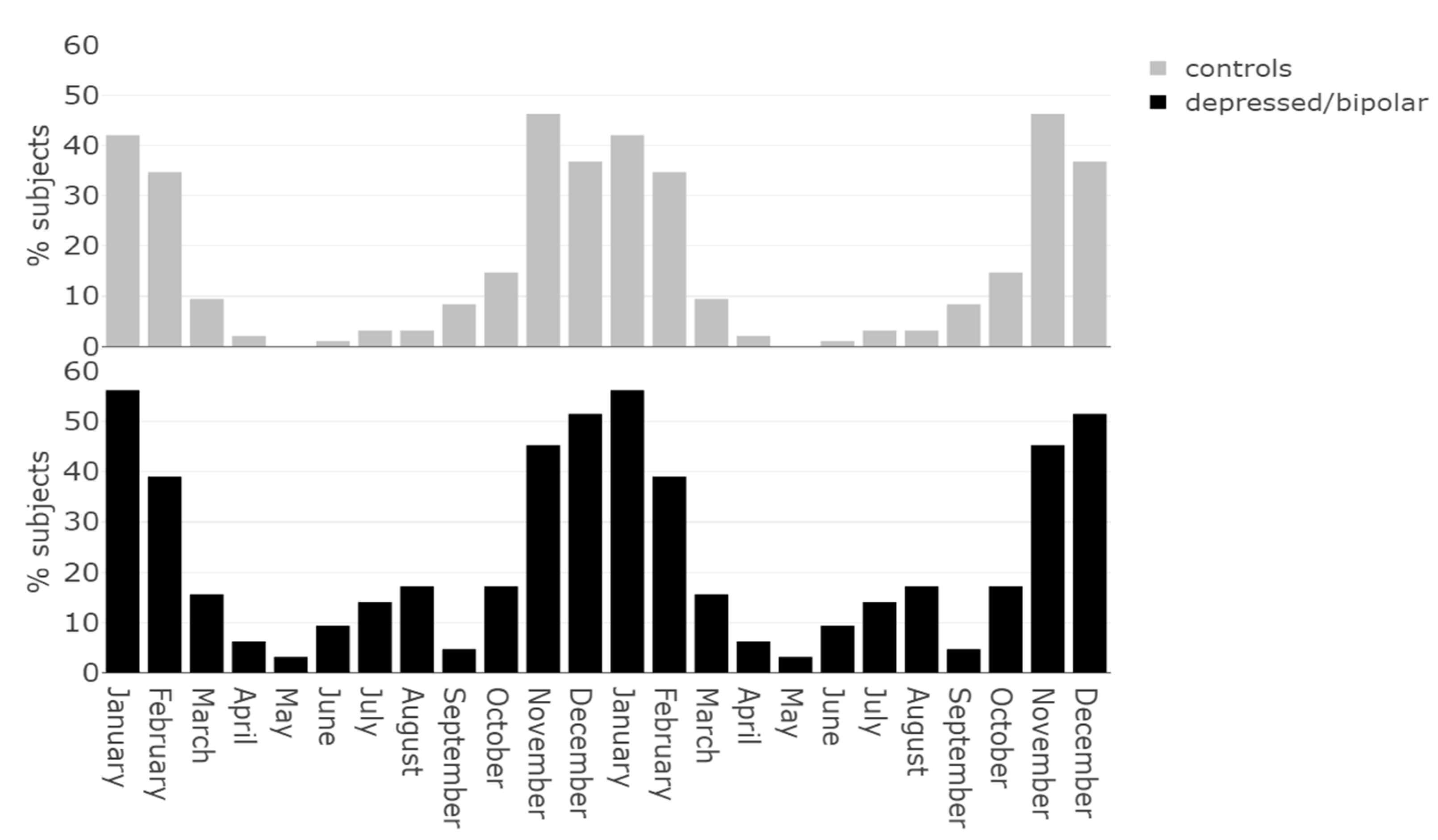
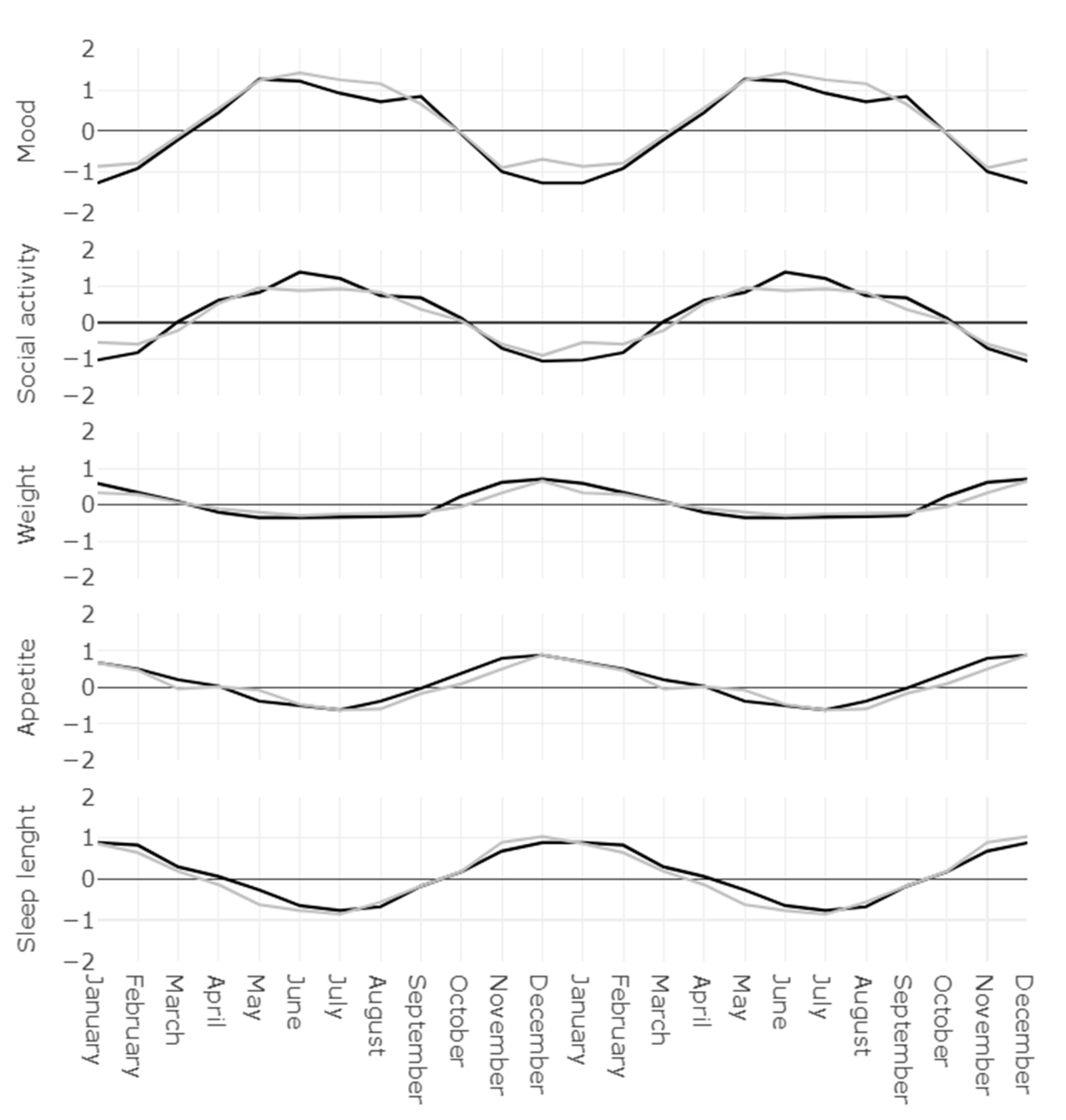
3.3. Monthly Variation of the GSS
3.4. Qualifying Seasonality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kasper, S.; Wehr, T.A.; Bartko, J.J.; Gaist, P.A.; Rosenthal, N.E. Epidemiological Findings of Seasonal Changes in Mood and Behavior. A Telephone Survey of Montgomery County, Maryland. Arch. Gen. Psychiatry 1989, 46, 823–833. [Google Scholar] [CrossRef]
- Mersch, P.P.A.; Middendorp, H.M.; Bouhuys, A.L.; Beersma, D.G.; van den Hoofdakker, R.H. The Prevalence of Seasonal Affective Disorder in The Netherlands: A Prospective and Retrospective Study of Seasonal Mood Variation in the General Population. Biol. Psychiatry 1999, 45, 1013–1022. [Google Scholar] [CrossRef] [Green Version]
- Murray, G.; Allen, N.B.; Trinder, J. A Longitudinal Investigation of Seasonal Variation in Mood. Chronobiol. Int. 2001, 18, 875–891. [Google Scholar] [CrossRef]
- Martinez, D.; Silva, R.P.D.; Cassol, C.M.; Pires, G.N. Scores of a Web-Based Version of the Seasonal Pattern Assessment Questionnaire in Brazil. Clin. Biomed. Res. 2015, 35. [Google Scholar] [CrossRef]
- Han, L.; Wang, K.; Du, Z.; Cheng, Y.; Simons, J.S.; Rosenthal, N.E. Seasonal Variations in Mood and Behavior Among Chinese Medical Students. Am. J. Psychiatry 2000, 157, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, N.; Ono, Y.; Ito, A.; Rosenthal, N.E. Prevalence of Seasonal Difficulties in Mood and Behavior among Japanese Civil Servants. Am. J. Psychiatry 1995, 152, 1225–1227. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Dunner, D. Validity of Seasonal Pattern as a Modifier for Recurrent Mood Disorders for DSM-IV. Compr. Psychiatry 1993. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Bellivier, F.; Scott, J.; Etain, B. Seasonality and Bipolar Disorder: A Systematic Review, from Admission Rates to Seasonality of Symptoms. J. Affect. Disord. 2014, 168, 210–223. [Google Scholar] [CrossRef] [PubMed]
- Murray, G. The Seasonal Pattern Assessment Questionnaire as a Measure of Mood Seasonality: A Prospective Validation Study. Psychiatry Res. 2003, 120, 53–59. [Google Scholar] [CrossRef]
- Rosenthal, N.E.; Sack, D.A.; Gillin, J.C.; Lewy, A.J.; Goodwin, F.K.; Davenport, Y.; Mueller, P.S.; Newsome, D.A.; Wehr, T.A. Seasonal Affective Disorder. A Description of the Syndrome and Preliminary Findings with Light Therapy. Arch. Gen. Psychiatry 1984, 41, 72–80. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Byrne, B.; Brainard, G.C. Seasonal Affective Disorder and Light Therapy. Sleep Med. Clin. 2008, 3, 307–315. [Google Scholar] [CrossRef]
- Michalak, E.E.; Lam, R.W. Seasonal Affective Disorder: The Latitude Hypothesis Revisited. Can. J. Psychiatry Rev. Can. Psychiatr. 2002, 47, 787–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnusson, A. An Overview of Epidemiological Studies on Seasonal Affective Disorder. Acta Psychiatr. Scand. 2000, 101, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Chotai, J.; Smedh, K.; Johansson, C.; Nilsson, L.-G.; Adolfsson, R. An Epidemiological Study on Gender Differences in Self-Reported Seasonal Changes in Mood and Behaviour in a General Population of Northern Sweden. Nord. J. Psychiatry 2004, 58, 429–437. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Bellivier, F.; Scott, J.; Boudebesse, C.; Lajnef, M.; Gard, S.; Kahn, J.-P.; Azorin, J.-M.; Henry, C.; Leboyer, M.; et al. Bipolar Disorder with Seasonal Pattern: Clinical Characteristics and Gender Influences. Chronobiol. Int. 2013, 30, 1101–1107. [Google Scholar] [CrossRef] [Green Version]
- Maruani, J.; Anderson, G.; Etain, B.; Lejoyeux, M.; Bellivier, F.; Geoffroy, P.A. The Neurobiology of Adaptation to Seasons: Relevance and Correlations in Bipolar Disorders. Chronobiol. Int. 2018, 35, 1335–1353. [Google Scholar] [CrossRef] [PubMed]
- Geoffroy, P.A.; Lajnef, M.; Bellivier, F.; Jamain, S.; Gard, S.; Kahn, J.-P.; Henry, C.; Leboyer, M.; Etain, B. Genetic Association Study of Circadian Genes with Seasonal Pattern in Bipolar Disorders. Sci. Rep. 2015, 5, 10232. [Google Scholar] [CrossRef] [Green Version]
- Kovanen, L.; Donner, K.; Kaunisto, M.; Partonen, T. CRY1 and CRY2 Genetic Variants in Seasonality: A Longitudinal and Cross-Sectional Study. Psychiatry Res. 2016, 242, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Hirano, A.; Hsu, P.-K.; Jones, C.R.; Sakai, N.; Okuro, M.; McMahon, T.; Yamazaki, M.; Xu, Y.; Saigoh, N.; et al. A PERIOD3 Variant Causes a Circadian Phenotype and Is Associated with a Seasonal Mood Trait. Proc. Natl. Acad. Sci. USA 2016, 113, E1536–E1544. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-I.; Lee, H.-J.; Cho, C.-H.; Kang, S.-G.; Yoon, H.-K.; Park, Y.-M.; Lee, S.-H.; Moon, J.-H.; Song, H.-M.; Lee, E.; et al. Association of CLOCK, ARNTL, and NPAS2 Gene Polymorphisms and Seasonal Variations in Mood and Behavior. Chronobiol. Int. 2015, 32, 785–791. [Google Scholar] [CrossRef]
- Lewy, A.J.; Lefler, B.J.; Emens, J.S.; Bauer, V.K. The Circadian Basis of Winter Depression. Proc. Natl. Acad. Sci. USA 2006, 103, 7414–7419. [Google Scholar] [CrossRef] [Green Version]
- Terman, M.; Terman, J.S.; Quitkin, F.M.; Cooper, T.B.; Lo, E.S.; Gorman, J.M.; Stewart, J.W.; McGrath, P.J. Response of the Melatonin Cycle to Phototherapy for Seasonal Affective Disorder. Short Note. J. Neural Transm. 1988, 72, 147–165. [Google Scholar] [CrossRef]
- Levitan, R.D. The Chronobiology and Neurobiology of Winter Seasonal Affective Disorder. Dialogues Clin. Neurosci. 2007, 9, 315–324. [Google Scholar]
- Tyrer, A.E.; Levitan, R.D.; Houle, S.; Wilson, A.A.; Nobrega, J.N.; Meyer, J.H. Increased Seasonal Variation in Serotonin Transporter Binding in Seasonal Affective Disorder. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2016, 41, 2447–2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuiper, S.; McLean, L.; Fritz, K.; Lampe, L.; Malhi, G.S. Getting Depression Clinical Practice Guidelines Right: Time for Change? Acta Psychiatr. Scand. 2013, 128, 24–30. [Google Scholar] [CrossRef]
- Lam, R.W.; Levitt, A.J.; Levitan, R.D.; Enns, M.W.; Morehouse, R.; Michalak, E.E.; Tam, E.M. The Can-SAD Study: A Randomized Controlled Trial of the Effectiveness of Light Therapy and Fluoxetine in Patients with Winter Seasonal Affective Disorder. Am. J. Psychiatry 2006, 163, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Reeves, G.M.; Nijjar, G.V.; Langenberg, P.; Johnson, M.A.; Khabazghazvini, B.; Sleemi, A.; Vaswani, D.; Lapidus, M.; Manalai, P.; Tariq, M.; et al. Improvement in Depression Scores after 1 Hour of Light Therapy Treatment in Patients with Seasonal Affective Disorder. J. Nerv. Ment. Dis. 2012, 200, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Terman, M.; Terman, J.S.; Quitkin, F.M.; McGrath, P.J.; Stewart, J.W.; Rafferty, B. Light Therapy for Seasonal Affective Disorder. A Review of Efficacy. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 1989, 2, 1–22. [Google Scholar] [CrossRef]
- Geoffroy, P.; Schroder, C.; Reynaud, E.; Bourgin, E. Efficacy of Light Therapy versus Antidepressant Drugs, and of the Combination versus Monotherapy, in Major Depressive Episodes: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2019, 48. [Google Scholar] [CrossRef] [PubMed]
- Rohan, K.J.; Roecklein, K.A.; Haaga, D.A.F. Biological and Psychological Mechanisms of Seasonal Affective Disorder: A Review and Integration. Curr. Psychiatry Rev. 2009, 5, 37–47. [Google Scholar] [CrossRef]
- Kurlansik, S.L.; Ibay, A.D. Seasonal Affective Disorder. Am. Fam. Physician 2012, 86, 1037–1041. [Google Scholar]
- Geoffroy, P.A.; Godin, O.; Mahee, D.; Henry, C.; Aubin, V.; Azorin, J.-M.; Bougerol, T.; Courtet, P.; Gard, S.; Kahn, J.-P.; et al. Seasonal Pattern in Bipolar Disorders and Cardio-Vascular Risk Factors: A Study from the FACE-BD Cohort. Chronobiol. Int. 2017, 34, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, N.; Bradt, G.; Wehr, T. Seasonal Pattern Assessment Questionnaire (SPAQ); National Institute of Mental Health: Bethesda, MD, USA, 1984.
- Mersch, P.P.A.; Vastenburg, N.C.; Meesters, Y.; Bouhuys, A.L.; Beersma, D.G.M.; van den Hoofdakker, R.H.; den Boer, J.A. The Reliability and Validity of the Seasonal Pattern Assessment Questionnaire: A Comparison between Patient Groups. J. Affect. Disord. 2004, 80, 209–219. [Google Scholar] [CrossRef]
- Magnusson, A. Validation of the Seasonal Pattern Assessment Questionnaire (SPAQ). J. Affect. Disord. 1996, 40, 121–129. [Google Scholar] [CrossRef]
- Altman, E.G.; Hedeker, D.; Peterson, J.L.; Davis, J.M. The Altman Self-Rating Mania Scale. Biol. Psychiatry 1997, 42, 948–955. [Google Scholar] [CrossRef]
- Stange, J.P.; Molz, A.R.; Black, C.L.; Shapero, B.G.; Bacelli, J.M.; Abramson, L.Y.; Alloy, L.B. Positive Overgeneralization and Behavioral Approach System (BAS) Sensitivity Interact to Predict Prospective Increases in Hypomanic Symptoms: A Behavioral High-Risk Design. Behav. Res. 2012, 50, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Rush, A.J.; Trivedi, M.H.; Ibrahim, H.M.; Carmody, T.J.; Arnow, B.; Klein, D.N.; Markowitz, J.C.; Ninan, P.T.; Kornstein, S.; Manber, R.; et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), Clinician Rating (QIDS-C), and Self-Report (QIDS-SR): A Psychometric Evaluation in Patients with Chronic Major Depression. Biol. Psychiatry 2003, 54, 573–583. [Google Scholar] [CrossRef]
- Szende, A.; Janssen, B.; Cabases, J. (Eds.) Self-Reported Population Health: An International Perspective Based on EQ-5D; Springer: Berlin/Heidelberg, Germany, 2014; ISBN 978-94-007-7595-4. [Google Scholar]
- Feng, Y.-S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric Properties of the EQ-5D-5L: A Systematic Review of the Literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.S.; Reilly, C.; Midkiff, K. Evaluation of Three Circadian Rhythm Questionnaires with Suggestions for an Improved Measure of Morningness. J. Appl. Psychol. 1989, 74, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Di Milia, L.; Smith, P.A.; Folkard, S. A Validation of the Revised Circadian Type Inventory in a Working Sample. Pers. Individ. Differ. 2005, 39, 1293–1305. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mulen, M.R. Structural Equation Modelling: Guidelines Fordetermining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2015; ISBN 978-1-4625-2334-4. [Google Scholar]
- Thompson, C.; Stinson, D.; Fernandez, M.; Fine, J.; Isaacs, G. A Comparison of Normal, Bipolar and Seasonal Affective Disorder Subjects Using the Seasonal Pattern Assessment Questionnaire. J. Affect. Disord. 1988, 14, 257–264. [Google Scholar] [CrossRef]
- Young, M.A.; Blodgett, C.; Reardon, A. Measuring Seasonality: Psychometric Properties of the Seasonal Pattern Assessment Questionnaire and the Inventory for Seasonal Variation. Psychiatry Res. 2003, 117, 75–83. [Google Scholar] [CrossRef]
- Wirz-Justice, A.; Graw, P.; Kräuchi, K.; Wacker, H.R. Seasonality in Affective Disorders in Switzerland. Acta Psychiatr. Scand. Suppl. 2003, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Wirz-Justice, A. Seasonality in Affective Disorders. Gen. Comp. Endocrinol. 2018, 258, 244–249. [Google Scholar] [CrossRef]
- Teicher, M.H.; Glod, C.A.; Magnus, E.; Harper, D.; Benson, G.; Krueger, K.; McGreenery, C.E. Circadian Rest-Activity Disturbances in Seasonal Affective Disorder. Arch. Gen. Psychiatry 1997, 54, 124–130. [Google Scholar] [CrossRef]
- Medici, C.R.; Vestergaard, C.H.; Hadzi-Pavlovic, D.; Munk-Jørgensen, P.; Parker, G. Seasonal Variations in Hospital Admissions for Mania: Examining for Associations with Weather Variables over Time. J. Affect. Disord. 2016, 205, 81–86. [Google Scholar] [CrossRef]
- Patten, S.B.; Williams, J.V.A.; Lavorato, D.H.; Bulloch, A.G.M.; Fiest, K.M.; Wang, J.L.; Sajobi, T.T. Seasonal Variation in Major Depressive Episode Prevalence in Canada. Epidemiol. Psychiatr. Sci. 2017, 26, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Young, J.W.; Dulcis, D. Investigating the Mechanism(s) Underlying Switching between States in Bipolar Disorder. Eur. J. Pharm. 2015, 759, 151–162. [Google Scholar] [CrossRef] [Green Version]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender Differences in Depression in Representative National Samples: Meta-Analyses of Diagnoses and Symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Panda, S.; Antoch, M.P.; Miller, B.H.; Su, A.I.; Schook, A.B.; Straume, M.; Schultz, P.G.; Kay, S.A.; Takahashi, J.S.; Hogenesch, J.B. Coordinated Transcription of Key Pathways in the Mouse by the Circadian Clock. Cell 2002, 109, 307–320. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, J.S.; Hong, H.-K.; Ko, C.H.; McDearmon, E.L. The Genetics of Mammalian Circadian Order and Disorder: Implications for Physiology and Disease. Nat. Rev. Genet. 2008, 9, 764–775. [Google Scholar] [CrossRef] [PubMed]
- Simonneaux, V.; Ribelayga, C. Generation of the Melatonin Endocrine Message in Mammals: A Review of the Complex Regulation of Melatonin Synthesis by Norepinephrine, Peptides, and Other Pineal Transmitters. Pharm. Rev. 2003, 55, 325–395. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.A.; Kayumov, L.; Shapiro, C.M. Antidepressant Action of Melatonin in the Treatment of Delayed Sleep Phase Syndrome. Sleep Med. 2010, 11, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.; Shen, H.; Zeng, L.-L.; Jiang, W.; Liu, L.; Hu, D. Predicting Clinical Responses in Major Depression Using Intrinsic Functional Connectivity. Neuroreport 2015, 26, 675–680. [Google Scholar] [CrossRef]
- La Morgia, C.; Carelli, V.; Carbonelli, M. Melanopsin Retinal Ganglion Cells and Pupil: Clinical Implications for Neuro-Ophthalmology. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Lambert, G.W.; Reid, C.; Kaye, D.M.; Jennings, G.L.; Esler, M.D. Effect of Sunlight and Season on Serotonin Turnover in the Brain. Lancet Lond. Engl. 2002, 360, 1840–1842. [Google Scholar] [CrossRef]
- Wirz-Justice, A.; Benedetti, F. Perspectives in Affective Disorders: Clocks and Sleep. Eur. J. Neurosci. 2020, 51, 346–365. [Google Scholar] [CrossRef]
- Gottlieb, J.F.; Benedetti, F.; Geoffroy, P.A.; Henriksen, T.E.G.; Lam, R.W.; Murray, G.; Phelps, J.; Sit, D.; Swartz, H.A.; Crowe, M.; et al. The Chronotherapeutic Treatment of Bipolar Disorders: A Systematic Review and Practice Recommendations from the ISBD Task Force on Chronotherapy and Chronobiology. Bipolar Disord. 2019, 21, 741–773. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Xi, Y.; Peng, Y.; Yang, Y.; Huang, X.; Fu, Y.; Tao, Q.; Xiao, J.; Yuan, T.; An, K.; et al. A Visual Circuit Related to Habenula Underlies the Antidepressive Effects of Light Therapy. Neuron 2019, 102, 128–142.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeGates, T.A.; Fernandez, D.C.; Hattar, S. Light as a Central Modulator of Circadian Rhythms, Sleep and Affect. Nat. Rev. Neurosci. 2014, 15, 443–454. [Google Scholar] [CrossRef]
- Stephenson, K.M.; Schroder, C.M.; Bertschy, G.; Bourgin, P. Complex Interaction of Circadian and Non-Circadian Effects of Light on Mood: Shedding New Light on an Old Story. Sleep Med. Rev. 2012, 16, 445–454. [Google Scholar] [CrossRef]
- Tyrer, A.E.; Levitan, R.D.; Houle, S.; Wilson, A.A.; Nobrega, J.N.; Rusjan, P.M.; Meyer, J.H. Serotonin Transporter Binding Is Reduced in Seasonal Affective Disorder Following Light Therapy. Acta Psychiatr. Scand. 2016, 134, 410–419. [Google Scholar] [CrossRef]
- Tsai, J.W.; Hannibal, J.; Hagiwara, G.; Colas, D.; Ruppert, E.; Ruby, N.F.; Heller, H.C.; Franken, P.; Bourgin, P. Melanopsin as a Sleep Modulator: Circadian Gating of the Direct Effects of Light on Sleep and Altered Sleep Homeostasis in Opn4(-/-) Mice. PLoS Biol. 2009, 7, e1000125. [Google Scholar] [CrossRef] [PubMed]
- Cajochen, C. Alerting Effects of Light. Sleep Med. Rev. 2007, 11, 453–464. [Google Scholar] [CrossRef]
- Comtet, H.; Geoffroy, P.A.; Kobayashi Frisk, M.; Hubbard, J.; Robin-Choteau, L.; Calvel, L.; Hugueny, L.; Viola, A.U.; Bourgin, P. Light Therapy with Boxes or Glasses to Counteract Effects of Acute Sleep Deprivation. Sci. Rep. 2019, 9, 18073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruani, J.; Geoffroy, P.A. Bright Light as a Personalized Precision Treatment of Mood Disorders. Front. Psychiatry 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Geoffroy, P.A. The Light of Hope in Antidepressant Strategies. Chronobiol. Med. 2020, 2, 57–60. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sleep Length | Social Activities | Mood | Energy Level | Weight | Appetite | |
|---|---|---|---|---|---|---|
| Sleep length | — | |||||
| Social activities | 0.379 *** | — | ||||
| Mood | 0.318 *** | 0.536 *** | — | |||
| Energy level | 0.432 *** | 0.560 *** | 0.663 *** | — | ||
| Weight | 0.322 *** | 0.269 *** | 0.246 *** | 0.408 *** | — | |
| Appetite | 0.301 *** | 0.270 *** | 0.335 *** | 0.441 *** | 0.698 *** | — |
| Factor | Dimension | Estimate | SE | Z | p |
|---|---|---|---|---|---|
| Psychological factor | Sleep length | 0.542 | 0.086 | 6.332 | <0.001 |
| Social activities | 0.714 | 0.081 | 8.783 | <0.001 | |
| Mood | 0.860 | 0.082 | 10.431 | <0.001 | |
| Energy level | 0.968 | 0.076 | 12.680 | <0.001 | |
| Food factor | Weight | 0.995 | 0.094 | 10.562 | <0.001 |
| Appetite | 0.872 | 0.090 | 9.665 | <0.001 |
| CSM-Chronotype | CTI FR-Flexibility/Rigidity Factor | CTI LV-Languid/Vigorous Factor | ASRM-Manic Symptoms | QIDS-Depressive Symptoms | EQ5D 1-Mobility | EQ5D 2-Self-Care | EQ5D 3-Usual Activities | EQ5D 4-Pain/Discomfort | EQ5D 5-Anxiety/Depression | EQ5D VAS-Global Health | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Psychological factor | −0.09 | 0.01 | 0.12 | 0.15 | 0.26 | 0.08 | 0.08 | 0.14 | 0.14 | 0.19 | −0.18 |
| Sleep length | −0.10 | −0.04 | 0.10 | 0.19 | 0.19 | 0.10 | 0.00 | 0.12 | 0.18 | 0.07 | −0.13 |
| Social activities | −0.03 | 0.03 | 0.06 | 0.03 | 0.15 | 0.04 | 0.09 | 0.09 | 0.00 | 0.15 | −0.19 |
| Mood | −0.04 | 0.01 | 0.08 | 0.16 | 0.28 | 0.06 | 0.16 | 0.15 | 0.14 | 0.28 | −0.19 |
| Energy level | −0.08 | 0.02 | 0.15 | 0.12 | 0.25 | 0.08 | 0.04 | 0.13 | 0.16 | 0.14 | −0.12 |
| Food factor | −0.12 | −0.01 | 0.16 | 0.13 | 0.17 | −0.09 | 0.00 | 0.04 | 0.00 | 0.03 | −0.04 |
| Weight | −0.10 | −0.04 | 0.13 | 0.14 | 0.17 | −0.11 | −0.05 | 0.03 | 0.00 | 0.04 | −0.09 |
| Appetite | −0.15 | 0.02 | 0.18 | 0.12 | 0.15 | −0.06 | 0.04 | 0.03 | −0.02 | 0.01 | 0.00 |
| GSS total | −0.10 | 0.00 | 0.13 | 0.15 | 0.26 | 0.04 | 0.07 | 0.12 | 0.10 | 0.15 | −0.15 |
| Depressed/Bipolar (n = 64) Mean (SD) | Control (n = 64) Mean (SD) | p | |
|---|---|---|---|
| Psychological factor | 8.33 (3.62) | 6.73 (3.29) | 0.013 |
| Sleep length | 1.80 (1.21) | 1.28 (1.03) | 0.017 |
| Social activities | 2.00 (1.10) | 1.70 (1.05) | 0.118 |
| Mood | 2.27 (1.19) | 1.73 (1.04) | 0.006 |
| Energy level | 2.27 (1.17) | 2.02 (1.12) | 0.187 |
| Food factor | 2.75 (2.29) | 2.13 (1.78) | 0.144 |
| Weight | 1.27 (1.24) | 0.94 (0.96) | 0.195 |
| Appetite | 1.48 (1.22) | 1.19 (1.04) | 0.184 |
| GSS total | 11.08 (5.05) | 8.86 (4.57) | 0.013 |
| No SAD (n = 23)Mean (SD) | SAD (n = 105)Mean (SD) | pa | No SAD or S-SAD (n = 66), Mean (SD) | SAD or S-SAD (n = 62), Mean (SD) | pb | |
|---|---|---|---|---|---|---|
| CSM | 35.92 (7.67) | 34.61 (7.68) | 0.479 | 37.02 (38.00) | 34.27 (34.00) | 0.025 |
| CTI_FR | 12.58 (4.61) | 12.22 (4.00) | 0.779 | 12.29 (11.00) | 12.76 (13.00) | 0.436 |
| CTI_LV | 19.42 (4.85) | 20.61 (4.69) | 0.245 | 18.79 (19.00) | 20.53 (21.00) | 0.039 |
| ASRM | 2.05 (2.82) | 3.83 (4.64) | 0.062 | 1.80 (0.00) | 2.97 (1.00) | 0.050 |
| QIDS | 5.42 (4.49) | 10.17 (6.10) | <0.001 | 5.33 (3.50) | 7.27 (6.00) | 0.004 |
| No SAD or S-SAD (n = 66) | Winter SAD or S-SAD (n = 28) | Summer SAD or S-SAD (n = 5) | Mixed SAD or S-SAD (n = 29) | p | |
|---|---|---|---|---|---|
| CSM | 37.0 (7.67) | 36.7 (5.82) | 30.2 (9.93) | 32.7 (7.92) | 0.044 |
| CTI_FR | 12.3 (4.72) | 12.3 (3.96) | 15.4 (6.15) | 12.7 (4.20) | 0.447 |
| CTI_LV | 18.8 (5.10) | 19.5 (4.54) | 24.0 (1.87) | 21.0 (4.21) | 0.119 |
| ASRM | 1.80 (2.61) | 3.00 (3.94) | 5.20 (5.07) | 2.55 (3.40) | 0.253 |
| QIDS | 5.33 (5.08) | 8.32 (5.56) | 6.00 (4.74) | 6.48 (4.49) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reynaud, E.; Berna, F.; Haffen, E.; Weiner, L.; Maruani, J.; Lejoyeux, M.; Schroder, C.M.; Bourgin, P.; Geoffroy, P.A. Validity and Usage of the Seasonal Pattern Assessment Questionnaire (SPAQ) in a French Population of Patients with Depression, Bipolar Disorders and Controls. J. Clin. Med. 2021, 10, 1897. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10091897
Reynaud E, Berna F, Haffen E, Weiner L, Maruani J, Lejoyeux M, Schroder CM, Bourgin P, Geoffroy PA. Validity and Usage of the Seasonal Pattern Assessment Questionnaire (SPAQ) in a French Population of Patients with Depression, Bipolar Disorders and Controls. Journal of Clinical Medicine. 2021; 10(9):1897. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10091897
Chicago/Turabian StyleReynaud, Eve, Fabrice Berna, Emmanuel Haffen, Luisa Weiner, Julia Maruani, Michel Lejoyeux, Carmen M. Schroder, Patrice Bourgin, and Pierre A. Geoffroy. 2021. "Validity and Usage of the Seasonal Pattern Assessment Questionnaire (SPAQ) in a French Population of Patients with Depression, Bipolar Disorders and Controls" Journal of Clinical Medicine 10, no. 9: 1897. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10091897