
Stay Home! Stay Safe! First Post-Discharge Cardiologic Evaluation of Low-Risk–Low-BNP Heart Failure Patients in COVID-19 Era

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Baseline Characteristics
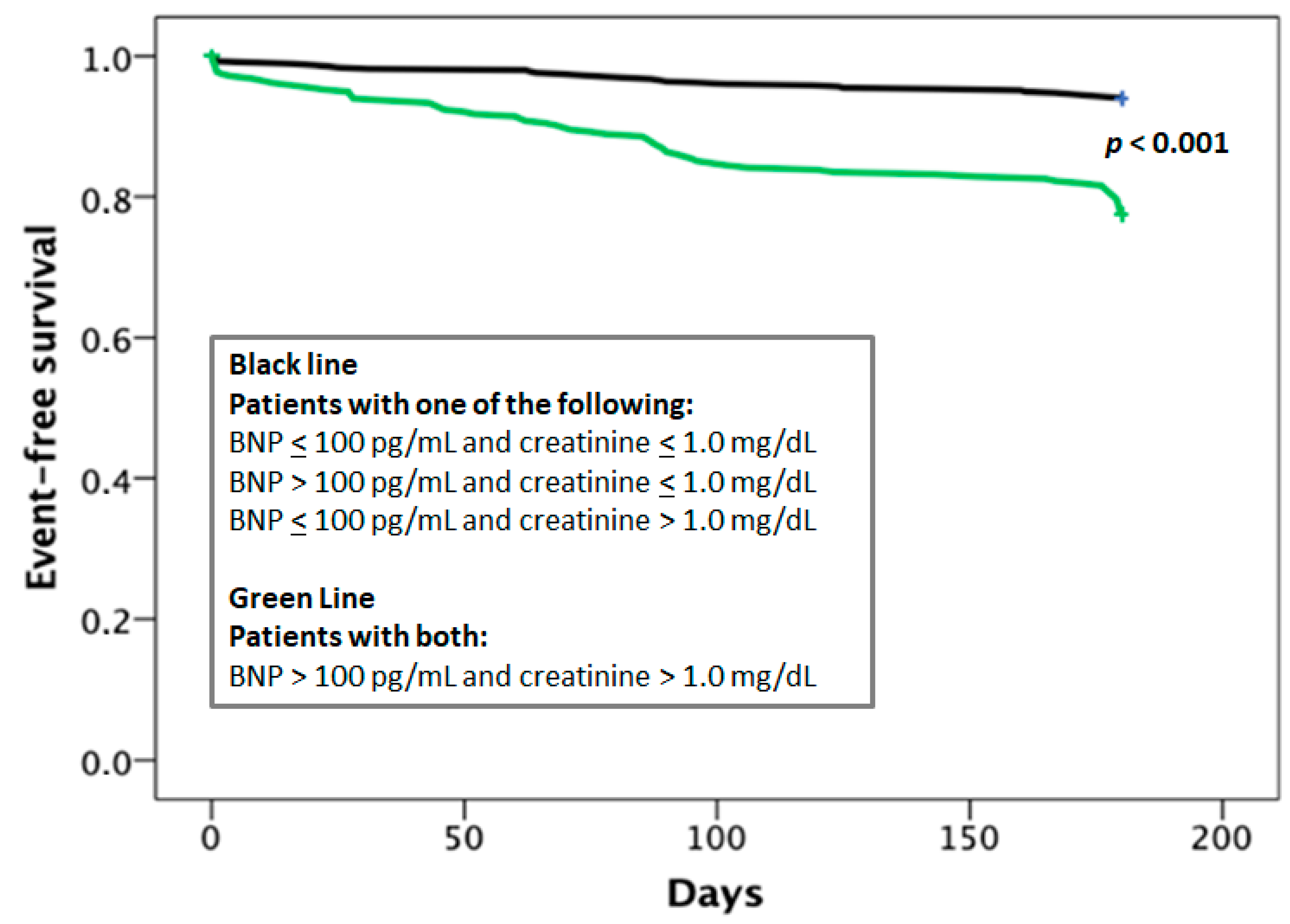
3.2. Clinical Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cappannoli, L.; Scacciavillani, R.; Iannaccone, G.; Anastasia, G.; Di Giusto, F.; Loria, V.; Aspromonte, N. 2019 novel-coronavirus: Cardiovascular insights about risk factors, myocardial injury, therapy and clinical implications. Chronic Dis. Transl. Med. 2020, 6, 246–250. [Google Scholar] [CrossRef]
- Iannaccone, G.; Scacciavillani, R.; Del Buono, M.G.; Camilli, M.; Ronco, C.; Lavie, C.J.; Abbate, A.; Crea, F.; Massetti, M.; Aspromonte, N. Weathering the Cytokine Storm in COVID-19: Therapeutic Implications. Cardiorenal Med. 2020, 10, 277–287. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Hartshorne-Evans, N.; Redmond-Lyon, S.; Wilson, J.; Essa, H.; Gray, A.; Clayton, L.; Barton, C.; Ahmed, F.Z.; Cunnington, C.; et al. The impact of COVID-19 on the management of heart failure: A United Kingdom patient questionnaire study. ESC Heart Fail 2021, 8, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Doust, J.A.; Pietrzak, E.; Dobson, A.; Glasziou, P.P. How well does B-type natriuretic peptide predict death and cardiac events in patients with heart failure: Systematic review. BMJ 2005, 330, 625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogenhuis, J.; Voors, A.A.; Jaarsma, T.; Hillege, H.L.; Hoes, A.W.; van Veldhuisen, D.J. Low prevalence of B-type natriuretic peptide levels <100 pg/mL in patients with heart failure at hospital discharge. Am. Heart J. 2006, 151, 1012.e1–1012.e5. [Google Scholar] [CrossRef] [PubMed]
- Philbin, E.F.; DiSalvo, T.G. Prediction of hospital readmission for heart failure: Development of a simple risk score based on administrative data. J. Am. Coll. Cardiol. 1999, 33, 1560–1566. [Google Scholar] [CrossRef] [Green Version]
- Valle, R.; Aspromonte, N.; Giovinazzo, P.; Carbonieri, E.; Chiatto, M.; di Tano, G.; Feola, M.; Milli, M.; Fontebasso, A.; Barro, S.; et al. B-type natriuretic Peptide-guided treatment for predicting outcome in patients hospitalized in sub-intensive care unit with acute heart failure. J. Card. Fail. 2008, 14, 219–224. [Google Scholar] [CrossRef]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The natural history of congestive heart failure: The Framingham study. New Engl. J. Med. 1971, 285, 1441–1446. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H., 3rd; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Okabe, T.; Yakushiji, T.; Kido, T.; Kimura, T.; Asukai, Y.; Shimazu, S.; Saito, J.; Oyama, Y.; Igawa, W.; Ono, M.; et al. Poor prognosis of heart failure patients with in-hospital worsening renal function and elevated BNP at discharge. ESC Heart Fail. 2020, 7, 2912–2921. [Google Scholar] [CrossRef]
- Mentias, A.; Patel, K.; Patel, H.; Gillinov, A.M.; Rodriguez, L.L.; Svensson, L.G.; Mihaljevic, T.; Sabik, J.F.; Griffin, B.P.; Desai, M.Y. Prognostic Utility of Brain Natriuretic Peptide in Asymptomatic Patients with Significant Mitral Regurgitation and Preserved Left Ventricular Ejection Fraction. Am. J. Cardiol. 2016, 117, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Feola, M.; Lombardo, E.; Testa, M.; Avogadri, E.; Piccolo, S.; Vado, A. Prognostic factors of mid-term clinical outcome in congestive heart failure patients discharged after acute decompensation. Arch. Med. Sci. 2012, 8, 462–470. [Google Scholar] [CrossRef] [Green Version]
- Maisel, A.; Hollander, J.E.; Guss, D.; McCullough, P.; Nowak, R.; Green, G.; Saltzberg, M.; Ellison, S.R.; Bhalla, M.A.; Bhalla, V.; et al. Rapid Emergency Department Heart Failure Outpatient Investigators. Primary results of the Rapid Emergency Department Heart Failure Outpatient Trial (REDHOT). A multicenter study of B-type natriuretic peptide levels, emergency department decision making, and outcomes in patients presenting with shortness of breath. J. Am. Coll. Cardiol. 2004, 44, 1328–1333. [Google Scholar] [PubMed] [Green Version]
- Laramee, A.S.; Levinsky, S.K.; Sargent, J.; Ross, R.; Callas, P. Case management in a heterogeneous congestive heart failure population: A randomized controlled trial. Arch. Intern. Med. 2003, 163, 809–817. [Google Scholar] [CrossRef] [Green Version]
- Kitzman, D.W.; Little, W.C.; Brubaker, P.H.; Anderson, R.T.; Hundley, W.G.; Marburger, C.T.; Brosnihan, B.; Morgan, T.M.; Stewart, K.P. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA 2002, 288, 2144–2150. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.S.; McCord, J.; Nowak, R.M.; Hollander, J.E.; Wu, A.H.; Duc, P.; Omland, T.; Storrow, A.B.; Krishnaswamy, P.; Abraham, W.T.; et al. Breathing Not Properly Multinational Study Investigators. Bedside B-type natriuretic peptide in the emergency diagnosis of heart failure with reduced or preserved ejection fraction. Results from the Breathing Not Properly Multinational Study. J. Am. Coll. Cardiol. 2003, 41, 2010–2017. [Google Scholar] [CrossRef] [Green Version]
- Zile, M.R.; Brutsaert, D.L. New concepts in diastolic dysfunction and diastolic heart failure: Part I: Diagnosis, prognosis, and measurements of diastolic function. Circulation 2002, 105, 1387–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kagiyama, N.; Kitai, T.; Hayashida, A.; Yamaguchi, T.; Okumura, T.; Kida, K.; Mizuno, A.; Oishi, S.; Inuzuka, Y.; Akiyama, E.; et al. Prognostic Value of BNP Reduction During Hospitalization in Patients with Acute Heart Failure. J. Card. Fail. 2019, 25, 712–721. [Google Scholar] [CrossRef]
- Santaguida, P.L.; Don-Wauchope, A.C.; Oremus, M.; McKelvie, R.; Ali, U.; Hill, S.A.; Balion, C.; Booth, R.A.; Brown, J.A.; Bustamam, A.; et al. BNP and NT-proBNP as prognostic markers in persons with acute decompensated heart failure: A systematic review. Heart Fail. Rev. 2014, 19, 453–470. [Google Scholar] [CrossRef]
- McAlister, F.A.; Stewart, S.; Ferrua, S.; McMurray, J.J. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: A systematic review of randomized trials. J. Am. Coll. Cardiol. 2004, 44, 810–819. [Google Scholar]
- DeBusk, R.F.; Miller, N.H.; Parker, K.M.; Bandura, A.; Kraemer, H.C.; Cher, D.J.; West, J.A.; Fowler, M.B.; Greenwald, G. Care management of low-risk patients with heart failure: A randomized, controlled trial. Ann. Intern. Med. 2004, 141, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Tavazzi, L.; Maggioni, A.P.; Lucci, D.; Cacciatore, G.; Ansalone, G.; Oliva, F.; Porcu, M.; Italian Survey on Acute Heart Failure Investigators. Nationwide survey on acute heart failure in cardiology ward services in Italy. Eur. Heart J. 2006, 27, 1207–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, A.F.; Greiner, M.A.; Fonarow, G.C.; Hammill, B.G.; Heidenreich, P.A.; Yancy, C.W.; Peterson, E.D.; Curtis, L.H. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA 2010, 303, 1716–1722. [Google Scholar] [CrossRef] [Green Version]
- Schou, M.; Gustafsson, F.; Videbaek, L.; Tuxen, C.; Keller, N.; Handberg, J.; Sejr Knudsen, A.; Espersen, G.; Markenvard, J.; Egstrup, K.; et al. NorthStar Investigators, all members of The Danish Heart Failure Clinics Network. Extended heart failure clinic follow-up in low-risk patients: A randomized clinical trial (NorthStar). Eur. Heart J. 2013, 34, 432–442. [Google Scholar] [CrossRef] [PubMed]
- McQuade, C.N.; Mizus, M.; Wald, J.W.; Goldberg, L.; Jessup, M.; Umscheid, C.A. Brain-Type Natriuretic Peptide and Amino-Terminal Pro-Brain-Type Natriuretic Peptide Discharge Thresholds for Acute Decompensated Heart Failure: A Systematic Review. Ann. Intern. Med. 2017, 166, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Omar, H.R.; Guglin, M. Discharge BNP is a stronger predictor of 6-month mortality in acute heart failure compared with baseline BNP and admission-to-discharge percentage BNP reduction. Int. J. Cardiol. 2016, 221, 1116–1122. [Google Scholar] [CrossRef]
- Hamatani, Y.; Nagai, T.; Shiraishi, Y.; Kohsaka, S.; Nakai, M.; Nishimura, K.; Kohno, T.; Nagatomo, Y.; Asaumi, Y.; Goda, A.; et al. Investigators for the WET-NaDEF Collaboration Project. Long-Term Prognostic Significance of Plasma B-Type Natriuretic Peptide Level in Patients with Acute Heart Failure with Reduced, Mid-Range, and Preserved Ejection Fractions. Am. J. Cardiol. 2018, 121, 731–738. [Google Scholar] [CrossRef]
- Omar, H.R.; Guglin, M. Post-discharge rise in BNP and rehospitalization for heart failure. Herz 2019, 44, 450–454. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | Total (n = 1000) | BNP ≤ 100 pg/mL and crea ≤ 1 mg/dL (n = 161) Group a | BNP > 100 pg/mL and crea ≤ 1 mg/dL or BNP ≤ 100 pg/mL and crea > 1 mg/dL (n = 471) Group b | BNP > 100 pg/mL and crea > 1 mg/dL (n = 368) Group c |
|---|---|---|---|---|
| Age (years) | 72 ± 10 | 67 ± 12 | 72 ± 9a | 73 ± 10a |
| Male gender (%) | 54 | 56 | 55 | 52 |
| NYHA class | 2.1 ± 0.6 | 2.0 ± 0.5 | 2.1 ± 0.6 | 2.2 ± 0.6a |
| LVEF (%) | 46 ± 12 | 48 ± 11 | 46 ± 11 | 44 ± 13a, b |
| BNP (pg/mL) | 110 ± 73 | 45 ± 27 | 84 ± 65a | 173 ± 44a, b |
| Creatinine (mg/dL) | 1.3 ± 0.7 | 0.8 ± 0.1 | 1.3 ± 0.7a | 1.5 ± 0.8a, b |
| Ischemic heart disease | 38 | 36 | 37 | 40 |
| Atrial fibrillation | 26 | 24 | 24 | 28 |
| Diabetes mellitus (%) | 25 | 25 | 26 | 27 |
| Events (n, %) | ||||
| Death | 39 (3.9) | 1 (0.6) | 13 (2.8) | 25 (6.8) |
| Readmission for HF | 65 (6.5) | 6 (3.7) | 14 (3.0) | 45 (12.2) |
| Total | 104 (10.4) | 7 (4.3) | 27 (4.7) | 70 (19.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aspromonte, N.; Cappannoli, L.; Scicchitano, P.; Massari, F.; Pantano, I.; Massetti, M.; Crea, F.; Valle, R. Stay Home! Stay Safe! First Post-Discharge Cardiologic Evaluation of Low-Risk–Low-BNP Heart Failure Patients in COVID-19 Era. J. Clin. Med. 2021, 10, 2126. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102126
Aspromonte N, Cappannoli L, Scicchitano P, Massari F, Pantano I, Massetti M, Crea F, Valle R. Stay Home! Stay Safe! First Post-Discharge Cardiologic Evaluation of Low-Risk–Low-BNP Heart Failure Patients in COVID-19 Era. Journal of Clinical Medicine. 2021; 10(10):2126. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102126
Chicago/Turabian StyleAspromonte, Nadia, Luigi Cappannoli, Pietro Scicchitano, Francesco Massari, Ivan Pantano, Massimo Massetti, Filippo Crea, and Roberto Valle. 2021. "Stay Home! Stay Safe! First Post-Discharge Cardiologic Evaluation of Low-Risk–Low-BNP Heart Failure Patients in COVID-19 Era" Journal of Clinical Medicine 10, no. 10: 2126. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102126