
Acupuncture for Poor Ovarian Response: A Randomized Controlled Trial

 , ,
, ,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
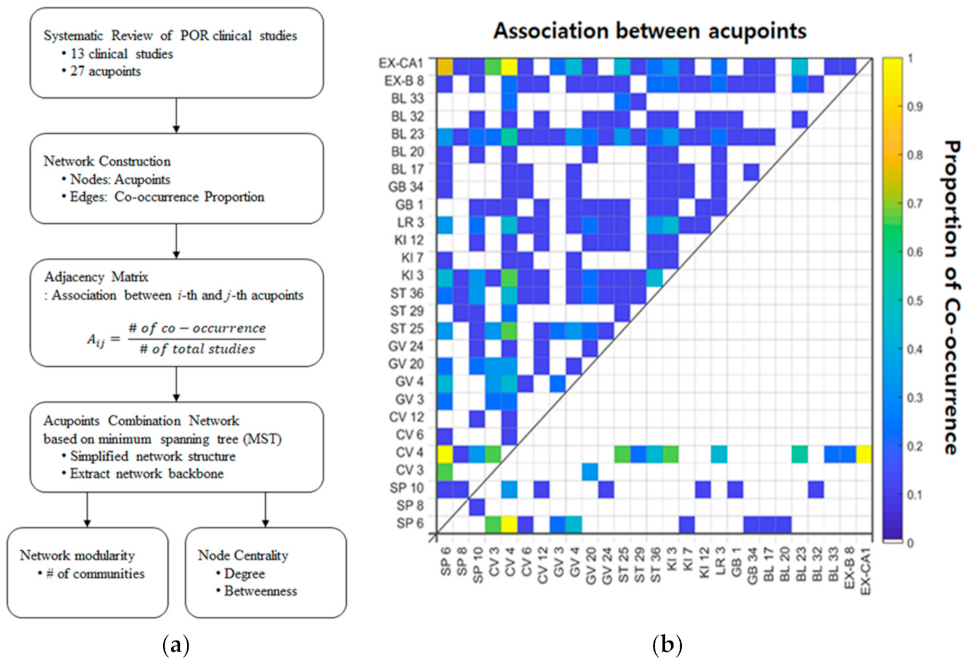
2.1. Extraction of Candidate Acupoints for POR Treatment
2.2. Selection of Optimal Acupoint Combination Using Network Analysis
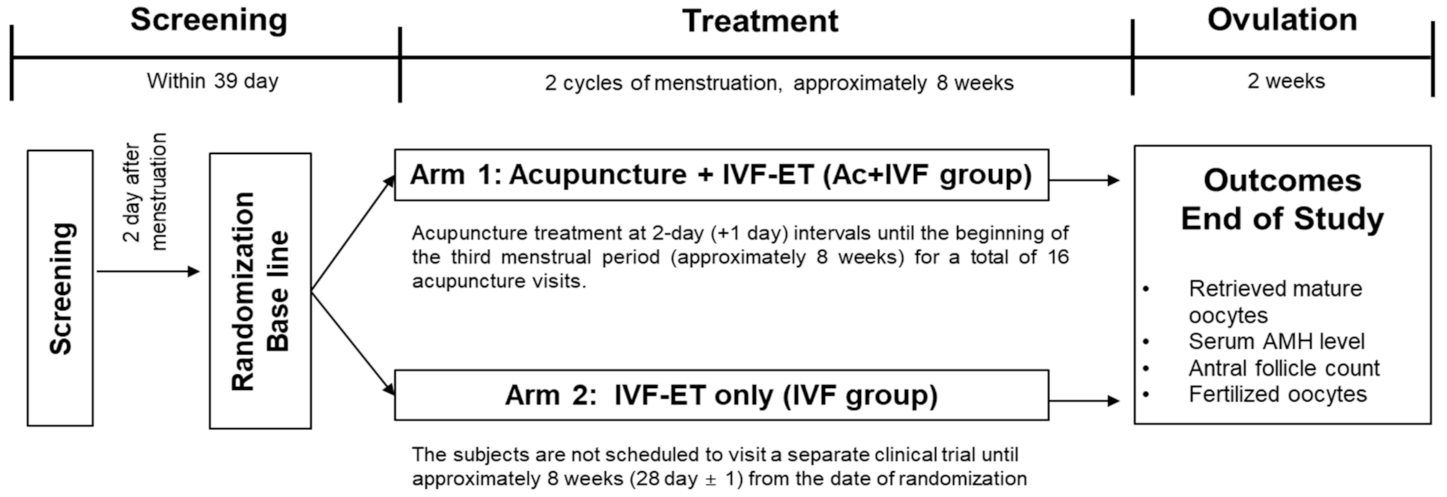
2.3. Study Design
2.4. Safety and Effectiveness
2.5. Statistical Analyses
3. Results
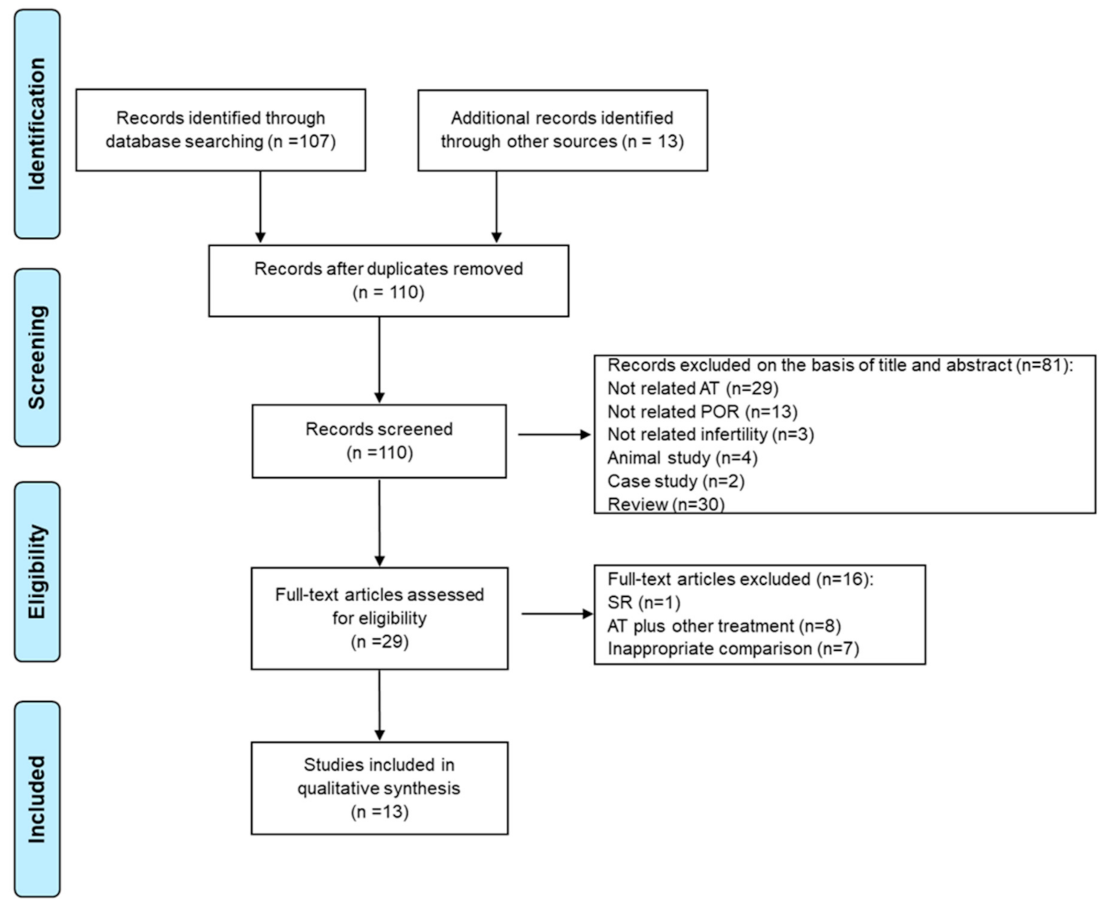
3.1. Extraction of Candidate Acupoints for POR Treatment
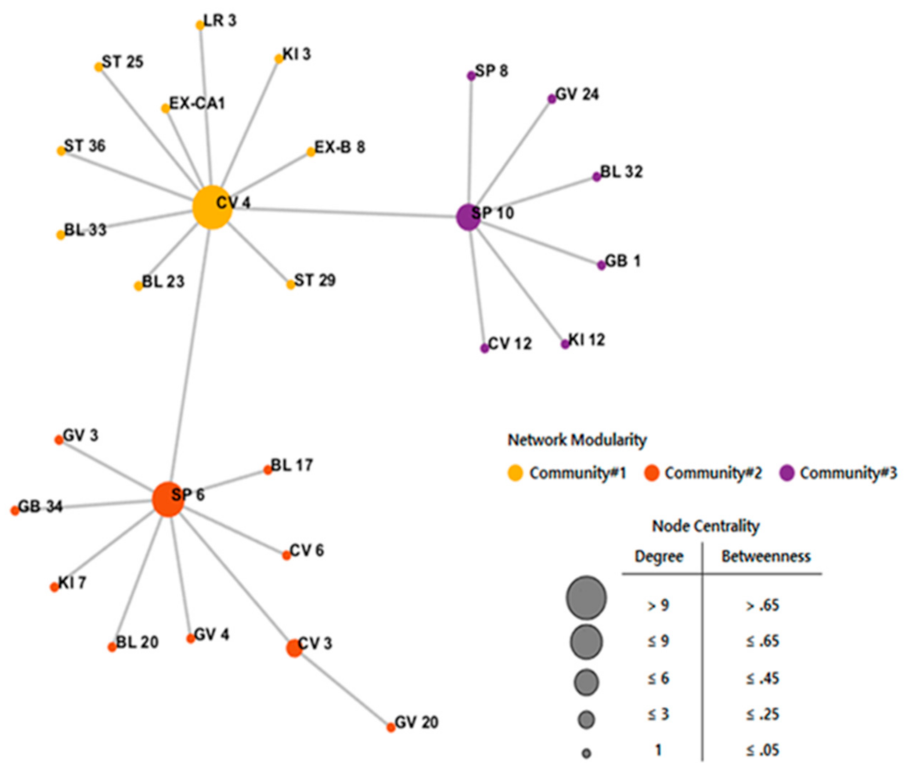
3.2. Selection of Optimal Acupoint Combination for POR Treatment Using Network Analysis
3.3. Participant Characteristics
3.4. Effectiveness of Acupuncture by Needling at Eight Acupoints Followed by IVF for POR Treatment
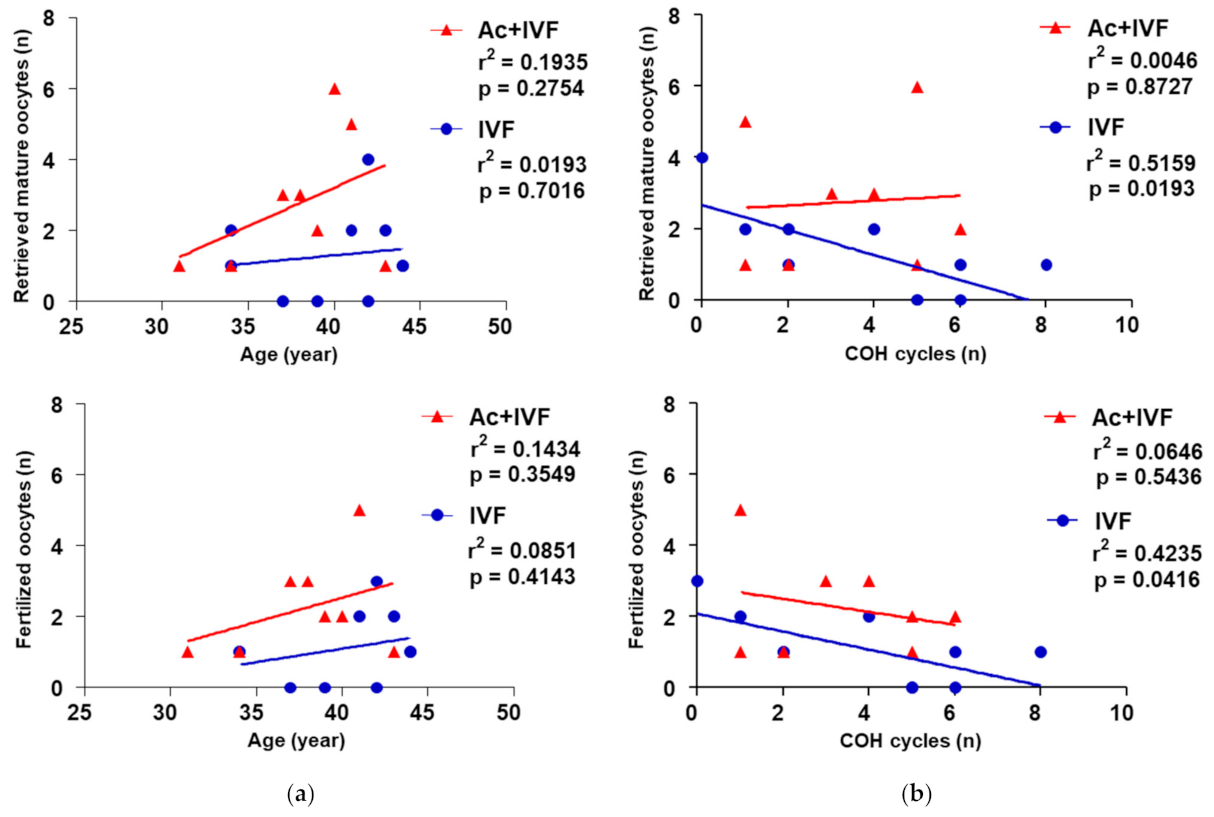
3.5. Inverse Correlation between the Number of Retrieved Mature Oocytes and COH Cycles Disappeared Following the Acupuncture Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. A Proposed Standard International Acupuncture Nomenclature: Report of a WHO Scientific Group; World Health Organization: Genève, Switzerland, 1991; ISBN 9789241544177. [Google Scholar]
- Shetty, G.B.; Shetty, B.; Mooventhan, A. Efficacy of acupuncture in the management of primary dysmenorrhea: A randomized controlled trial. J. Acupunct. Meridian Stud. 2018, 11, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Armour, M.; Ee, C.C.; Hao, J.; Wilson, T.M.; Yao, S.S.; Smith, C.A. Acupuncture and acupressure for premenstrual syndrome. Cochrane Database Syst. Rev. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, H.; Fang, Y.; Shang, J.; Yang, H.; Zhou, X.; Zhang, M. Acupuncture with regulating menstruation to promote pregnancy for diminished ovarian reverse: A prospective case series study. Zhongguo Zhen Jiu 2017, 37, 1061–1065. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Haimovici, F.; Ginsburg, E.S.; Schust, D.J.; Wayne, P.M. In vitro fertilization and acupuncture: Clinical efficacy and mechanistic basis. Altern. Ther. Health Med. 2007, 13, 38–48. [Google Scholar] [PubMed]
- Ma, R.; Song, J.; Si, J.; Liu, Y.; Li, X.; Cheng, R.; Hu, Z.; Xia, T.; Zhai, J. Acupuncture for diminished ovarian reserve: Protocol for a systematic review and meta-analysis. Medicine (Baltimore) 2019, 98, e16852. [Google Scholar] [CrossRef]
- Xu, S.; Wang, L.; Cooper, E.; Zhang, M.; Manheimer, E.; Berman, B.; Shen, X.; Lao, L. Adverse events of acupuncture: A systematic review of case reports. Evid. Based Complement Alternat. Med. 2013, 2013, 581203. [Google Scholar] [CrossRef] [Green Version]
- Jaiswar, S.P.; Natu, S.M.; Sankhwar, P.L.; Manjari, G. Prediction of Poor Ovarian response by Biochemical and Biophysical Markers: A Logistic Regression Model. J. Obstet. Gynaecol. India 2015, 65, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Cochrane, S.; Smith, C.A.; Possamai-Inesedy, A.; Bensoussan, A. Acupuncture and women’s health: An overview of the role of acupuncture and its clinical management in women’s reproductive health. Int. J. Womens Health 2014, 17, 313–325. [Google Scholar] [CrossRef] [Green Version]
- Rasool, S.; Shah, D. Fertility with early reduction of ovarian reserve: The last straw that breaks the Camel’s back. Fertil. Res. Pract. 2017, 3, 15. [Google Scholar] [CrossRef] [Green Version]
- Drakopoulos, P.; Bardhi, E.; Boudry, L.; Vaiarelli, A.; Makrigiannakis, A.; Esteves, S.C.; Tournaye, H.; Blockeel, C. Update on the management of poor ovarian response in IVF: The shift from Bologna criteria to the Poseidon concept. Ther. Adv. Reprod. Health 2020, 14, 2633494120941480. [Google Scholar] [CrossRef]
- Zhang, C.; Xu, X. Advancement in the treatment of diminished ovarian reserve by traditional Chinese and Western medicine. Exp. Ther. Med. 2016, 11, 1173–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolibianakis, E.; Osmanagaoglu, K.; Camus, M.; Tournaye, H.; Van Steirteghem, A.; Devroey, P. Effect of repeated assisted reproductive technology cycles on ovarian response. Fertil. Steril. 2002, 77, 967–970. [Google Scholar] [CrossRef]
- Cimadomo, D.; Fabozzi, G.; Vaiarelli, A.; Ubaldi, N.; Ubaldi, F.M.; Rienzi, L. Impact of maternal age on oocyte and embryo competence. Front. Endocrinol. (Lausanne) 2018, 9, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruskal, J.B. On the shortest spanning subtree of a graph and the traveling salesman problem. Proc. Am. Math. Soc. 1956, 7, 48–50. [Google Scholar] [CrossRef]
- Tewarie, P.; van, D.E.; Hillebrand, A.; Stam, C.J. The minimum spanning tree: An unbiased method for brain network analysis. Neuroimage 2015, 104, 177–188. [Google Scholar] [CrossRef]
- Blondel, V.D.; Guillaume, J.L.; Lambiotte, R.; Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. Theory Exp. 2008, 2008, 10008. [Google Scholar] [CrossRef] [Green Version]
- Newman, M. Modularity and community structure in networks. Proc. Natl. Acad. Sci. USA 2006, 103, 8577. [Google Scholar] [CrossRef] [Green Version]
- Ferraretti, A.; La Marca, A.; Fauser, B.C.; Tarlatzis, B.; Nargund, G.; Gianaroli, L. ESHRE consensus on the definition of ‘Poor Response’ to ovarian stimulation for in vitro fertilization: The Bologna criteria. Hum. Reprod. 2011, 26, 1616–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Lee, H.; Choi, T.Y.; Shim, E.H.; Choi, J.; Joo, J.K.; Joo, B.S.; Lee, M.S.; Choi, J.-Y.; Ha, K.-T.; You, S.; et al. A randomized, open phase IV exploratory clinical trial to evaluate the efficacy and safety of acupuncture on the outcome of induction of ovulation in women with poor ovarian response: A study protocol for a randomized controlled trial. Medicine 2018, 97, e11813. [Google Scholar] [CrossRef]
- Corfman, R.S.; Milad, M.P.; Bellavance, T.L.; Ory, S.J.; Erickson, L.D.; Ball, G.D. A novel ovarian stimulation protocol for use with the assisted reproductive technologies. Fertil. Steril. 1993, 60, 864–870. [Google Scholar] [CrossRef]
- Zheng, Y.; Feng, X.; Mi, H.; Yao, Y.; Zhao, Y.; Li, J.; Jiao, J.; Gong, A.; Sun, W.; Deng, X. Effects of transcutaneous electrical acupoint stimulation on ovarian reserve of patients with diminished ovarian reserve in in vitro fertilization and embryo transfer cycles. J. Obstet. Gynaecol. Res. 2015, 41, 1905–1911. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Xia, Y.B.; Ma, X.; Tang, L.M.; Lu, J.; Tang, Q.Q.; Wang, Y.P. Effects of “menstrual cycle-based acupuncture therapy” on IVF-ET in patients with decline in ovarian reserve. Zhongguo Zhen Jiu 2016, 36, 25–28. [Google Scholar] [PubMed]
- Zhang, C.; Xu, X. Clinical study on acupuncture treatment of kidney deficiency and blood stasis of diminished ovarian reserve. Exp. Ther. Med. 2016, 11, 1173–1176. [Google Scholar] [CrossRef] [Green Version]
- Fernando, D.A. Clinical Observation on Acupuncture Treatment of Diminished Ovarian Reserve. Master’s Thesis, Beijing University, Beijing, China, 6 June 2016. [Google Scholar]
- Yan, H.L.; He, S.Z.; Xie, Y.J.; Luo, X.D.; Lin, B.; Lai, H.H. Clinical study of embryo transfer techniques-acupuncture treatment in vitro fertilization. Guangzhou Med. J. 2015, 46, 13–16. [Google Scholar]
- Lian, F.; Chen, S.; Xaing, S. Improvement of the oocyte quality with electroacupuncture in infertility patients of kidney deficiency pattern. Chin. Acupunct. Moxibustion 2015, 35, 109–113. [Google Scholar]
- Wang, Y.; Li, Y.; Chen, R.; Cui, X.; Yu, J.; Liu, Z. Electroacupuncture for reproductive hormone levels in patients with diminished ovarian reserve: A prospective observational study. Acupunct. Med. 2016, 34, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Zhou, K.; Jiang, J.; Wu, J.; Liu, Z. Electroacupuncture modulates reproductive hormone levels in patients with primary ovarian insufficiency: Results from a prospective observational study. Evid. Based. Complement. Alternat. Med. 2013, 2013, 657234. [Google Scholar] [CrossRef]
- Chen, J.; Liu, L.L.; Cui, W.; Sun, W. Effects of electroacupuncture on in vitro fertilization-embryo transfer (IVF-ET) of patients with poor ovarian response. Zhongguo Zhen Jiu 2009, 29, 775–779. [Google Scholar]
- Liu, L.L. Study of the Effect of Electro-Acupuncture Treatment on Oocyte Quality and Outcome of the Patients Undergoing in-Vitro-Fertilization and Embryo Transfer. Master’s Thesis, Shandong University, Shandong, China, 10 April 2008. [Google Scholar]
- Lian, F.; Liu, F.; Shuai, Z.H. Effect of transcutaneous acupoint electrical stimulation on oocyte and bcl-2 and bax in the older women. Shanghai J. Acupunct. Moxibustion 2014, 33, 1097–1099. [Google Scholar]
- Chen, C. Study of the Effect of Transcutanclus Electrical Acupoint Stimulation Intervene in the Patients with Ovarian Poor Respond. Master’s Thesis, Shandong University, Shandong, China, 20 April 2011. [Google Scholar]
- Zhu, N. Study of the Effect of Transcutanclus Electrical Acupoint Stimulation to the Patients with Ovarian Poor Response in the Effect of Pregnancy Outcome. Master’s Thesis, Shandong University, Shandong, China, 20 April 2012. [Google Scholar]
- De Boer, E.J.; den Tonkelaar, I.; te Velde, E.R.; Burger, C.W.; Klip, H.; van Leeuwen, F.E. A low number of retrieved oocytes at in vitro fertilization treatment is predictive of early menopause. Fertil. Steril. 2002, 77, 978–985. [Google Scholar] [CrossRef]
- Zhang, J.; Zheng, Y.; Wang, Y.; Qu, S.; Zhang, S.; Wu, C.; Chen, J.; Ouyang, H.; Tang, C.; Huang, Y. Evidence of a synergistic effect of acupoint combination: A resting-state functional magnetic resonance imaging study. J. Altern. Complement. Med. 2016, 22, 800–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, C.E.; Lee, I.S.; Jung, W.M.; Kim, H.G.; Jang, H.; Kim, S.J.; Lee, H.; Park, H.J.; Chae, Y. Network analysis of acupuncture points used in the treatment of low back pain. Evid. Based Complement. Alterna. Med. 2013, 2013, 402180. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.M.; Jiang, F.; Longhurst, J.C. Point specificity in acupuncture. Chin. Med. 2012, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Pandian, Z.; McTavish Ar Fau-Aucott, L.; Aucott L Fau-Hamilton, M.P.; Hamilton Mp Fau-Bhattacharya, S.; Bhattacharya, S. Interventions for ‘poor responders’ to controlled ovarian hyper stimulation (COH) in in-vitro fertilisation (IVF). Cochrane Database Syst. Rev. 2010, 1, CD004379. [Google Scholar] [CrossRef]
- Jeve, Y.B.; Bhandari, H.M. Effective treatment protocol for poor ovarian response: A systematic review and meta-analysis. J. Hum. Reprod. Sci. 2016, 9, 70–81. [Google Scholar] [CrossRef]
- Badawy, A.; Wageah, A.; Gharib, M.E.; Osman, E.E. Prediction and diagnosis of poor ovarian response: The dilemma. J. Reprod. Infertil. 2011, 12, 241–248. [Google Scholar]
- Szafarowska, M.; Jerzak, M. Ovarian aging and infertility. Ginekol. Pol. 2013, 84, 298–304. [Google Scholar] [CrossRef]
- Ng, E.H.Y.; Tang, O.S.; Chan, C.C.W.; Ho, P.C. Ovarian stromal blood flow in the prediction of ovarian response during in vitro fertilization treatment. Hum Reprod. 2005, 20, 3147–3151. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, J.; Barber, J.; Kyei-Mensah, A.; Bekir, J.; Campbell, S.; Tan, S.L. Relationship of ovarian stromal blood flow at the baseline ultrasound scan to subsequent follicular response in an in vitro fertilization program. Obstet. Gynecol. 1996, 88, 779–784. [Google Scholar] [CrossRef]
- Kan, A.; Ng, E.H.Y.; Yeung, W.S.B.; Ho, P.C. Perifollicular vascularity in poor ovarian responders during IVF. Hum. Reprod. 2006, 21, 1539–1544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stener-Victorin, E.; Kobayashi, R.; Kurosawa, M. Ovarian blood flow responses to electro-acupuncture stimulation at different frequencies and intensities in anaesthetized rats. Neuroscience 2003, 108, 50–56. [Google Scholar] [CrossRef]
- Knardahl, S.; Elam, M.; Olausson, B.; Wallin, B.G. Sympathetic nerve activity after acupuncture in humans. Pain 1998, 75, 19–25. [Google Scholar] [CrossRef]
- Stener-Victorin, E.; Waldenstrom, U.; Andersson, S.A.; Wikland, M. Reduction of blood flow impedance in the uterine arteries of infertile women with electro-acupuncture. Hum. Reprod. 1996, 11, 1314–1317. [Google Scholar] [CrossRef] [Green Version]
- Rubinstein, M.; Marazzi, A.; de Fried, E.P. Low-dose aspirin treatment improves ovarian responsiveness, uterine and ovarian blood flow velocity, implantation, and pregnancy rates in patients undergoing in vitro fertilization: A prospective, randomized, double-blind placebo-controlled assay. Fertil. Steril. 1999, 71, 825–829. [Google Scholar] [CrossRef]
- Battaglia, C.; Salvatori, M.; Maxia, N.; Petraglia, F.; Facchinetti, F.; Volpe, A. Adjuvant L-arginine treatment for in-vitro fertilization in poor responder patients. Hum. Reprod. 1999, 14, 1690–1697. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Liu, Y.; Cui, E.; Zhao, H.; Gao, W.; Zhu, J.; Yang, D. A key node mining method based on acupoint-disease network (ADN): A new perspective for exploring acupoint specificity. Evid. Based Complement. Alternat. Med. 2020, 2020, 6031601. [Google Scholar] [CrossRef]
- Fan, H.; Ji, F.; Lin, Y.; Zhang, M.; Qin, W.; Zhou, Q.; Wu, Q. Electroacupuncture stimulation at CV4 prevents ovariectomy-induced osteoporosis in rats via Wnt-β-catenin signaling. Mol. Med. Rep. 2016, 13, 2485–2491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; Xiong, J.; Huang, G.-y.; Wang, W. Study on the underlying mechanism of acupuncture in regulating neuroendocrine activity in dysmenorrhea rats. Zhen Ci Yan Jiu Acupunct. Res. 2009, 34, 3–8. [Google Scholar]
- Xiang, S.; Xia, M.-F.; Song, J.-Y.; Liu, D.-Q.; Lian, F. Effect of electro-acupuncture on expression of IRS-1/PI3K/GLUT4 pathway in ovarian granulosa cells of infertile patients with polycystic ovary syndrome-insulin resistance of phlegm-dampness syndrome. Chin. J. Integr. Med. 2020. [Google Scholar] [CrossRef]
- Hernandez Gifford, J.A. The role of WNT signaling in adult ovarian folliculogenesis. Reproduction 2015, 150, R137–R148. [Google Scholar] [CrossRef] [Green Version]
- Yovich, J.L.; Ye, Y.; Regan, S.L.P.; Keane, K.N. The evolving concept of poor-prognosis for women undertaking IVF and the notion of growth hormone as an adjuvant; a single-center viewpoint. Front. Endocrinol. (Lausanne) 2019, 808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, M.A.; Kuijk, E.W.; Macklon, N.S. The impact of ovarian stimulation for IVF on the developing embryo. Reproduction 2010, 139, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Van Blerkom, J.; Davis, P. Differential effects of repeated ovarian stimulation on cytoplasmic and spindle organization in metaphase II mouse oocytes matured in vivo and in vitro. Hum. Reprod. 2001, 16, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Lin, S.; Zhu, M.; Li, C.; Chen, S.; Pu, L.; Lin, J.; Cao, L.; Zhang, Y. Acupuncture reduces apoptosis of granulosa cells in rats with premature ovarian failure via restoring the PI3K/Akt signaling pathway. Int. J. Mol. Sci. 2019, 20, 6311. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | Study Design; Sample Size; Age (y); Infertility Periods (y) | Intervention Group (A) Control Group (B, C, D) | Main Outcomes | Intergroup Differences | Acupoint | |
|---|---|---|---|---|---|---|
| Zhou (2016) [23] | RCT; 63; (A)(35 ± 5)/(B)(36 ± 5); (A)(5.3 ± 4.6)/(B)(6.9 ± 5.2) | (A) AT plus IVF-ET (n = 30) (B) IVF-ET (n = 33) | (1) FSH (2) E2 (3) AFC (4) Number of matured oocytes (5) Fertilization rate | (6) High-quality embryo rate (7) Cycle cancellation rate (8) Implantation rate (9) Clinical pregnancy rate | (1–6) p < 0.05 (7–9) p < 0.01 | SP6, CV4, CV6, GV4, ST36, KI3, KI7, LR3, GB34, BL17, BL23, EX-B8, EX-CA1 |
| Xu (2016) [22] | RCT; 56; n.r.; n.r. | (A) AT (n = 28) (B) Estrogen and progesterone therapy (n = 28) | (1) FSH (2) AMH | (1–2) p < 0.05 | SP6, SP10, CV4, GV20, ST36, KI3, LR3, BL20 | |
| Fernando (2016) [23] | Prospective observation study; 21; (A)(37.0 ± 5.4); (A)(3.2 ± 3.2) | (A) AT (n = 21) | (1) FSH (2) LH (3) E2 | (4) FSH/LH ratios (5) Symptom scale scores | (1–5) p < 0.05 | SP10, CV4, CV12, GV20, GV24, ST25, ST36, KI3, KI12, LR3, GB1, BL23, BL32, EX-B8 |
| Yan (2015) [24] | RCT; 108; (29.8 ± 4.6); (4.9 ± 0.8); | (A) AT (n = 36) (B) Sham AT (n = 36) (C) No treatment (n = 36) | (1) Response rate (2) Planting rate | (3) Clinical pregnancy rate (4) Live birth rate | (1–4) p < 0.05 | SP8, SP10, CV4, ST29, ST36, KI3, BL23, EX-CA1 |
| Lian (2015) [25] | RCT; 66; (A)(38 ± 1)/(B)(37 ± 1); (A)(4.1 ± 2.2)/(B)(3.9 ± 1.9) | (A) EA plus IVF-ET (n = 33) (B) Sham EA plus IVF-ET (n = 33) | (1) Kidney deficiency syndrome score (2) High-quality embryo rate | 3) Clinical pregnancy rate 4) IGF-1, IGF-2, β-EP | (1–2) p < 0.05 (3) p > 0.05 (5) p < 0.05 | SP6, CV3, CV4, EX-CA1 |
| Wang (2016) [26] | Prospective observation study; 21; (A)(37.0 ± 5.4); (A)(3.2 ± 3.2) | (A) EA (n = 21) | (1) FSH (2) LH (3) E2 | 4) FSH/LH ratios 5) Symptom scale scores | (1–5) p < 0.05 | CV4, ST25, BL33, EX-CA1 |
| Zhou (2013) [27] | Prospective observation study; 11; (A)25–39; (A) 0.33–10 | (A) EA (n = 11) | (1) E2 (2) FSH (3) LH | (1) p = 0.002 (2) p = 0.001 (3) p = 0.002 | CV4, ST25, ST29, BL33 | |
| Chen (2009) [28] | RCT; 60; (A)(34.3 ± 2.7)/(B)(34.6 ± 2.3); (A)(6.2 ± 4.3)/(B)(6.0 ± 4.6) | (A) EA plus IVF-ET (n = 30) (B) IVF-ET (n = 30) | (1) Kidney deficiency syndrome score (2) E2 (3) Fertilization rate (4) Number of matured oocytes | (5) High-quality embryo rate (6) Implantation rate (7) Pregnancy rate | (1–6) p < 0.05 (7) p > 0.05 | SP6, CV4, KI3 |
| Liu (2008) [29] | RCT; 60; (A)(34.3 ± 2.7)/(B)(34.6 ± 2.3); (A)(4.3 ± 1.4)/(B)(4.4 ± 1.3) | (A) EA plus GnRH antagonist (n = 30) (B) GnRH antagonist (n = 30) | (1) doses and days of GnRH (2) Thickness of endometrium (3) E2 (4) FSH (5) LH (6) SCF | (7) Fertilization rate (8) Number of matured oocytes (9) High-quality embryo rate (10) Pregnancy rate (11) Abortion rate | (1–2) p > 0.05 (3–11) p < 0.05 | SP6, CV3, CV4, KI3, LR3, EX-CA1 |
| Zheng (2015) [30] | RCT; 240; (A)(36.0 ± 5.4)/(B)(36.9 ± 4.3) (C)(36.8 ± 4.6)/(D)(36.8 ± 5.3); (A)(4.4 ± 2.9)/(B)(5.2 ± 3.2) (C)(4.7 ± 2.6)/(D)(4.8 ± 2.4); | (A) TEAS (n = 56) (B) No treatment (n = 60) (C) False Han’s placebo (n = 56) (D) Artificial endometrial cycle treatment (n = 54) | (1) E2 (2) FSH (3) AMH (4) LH (5) Number of matured oocytes (6) Number of embryos transferred | (7) Clinical pregnancy rate (8) Fertilization rate (9) Cleavage rate (10) High-quality embryo rate | (1–4) p < 0.01 (5–10) p < 0.05 | SP6, CV3, CV4, GV4, GV20, ST25, BL23, EX-CA1 |
| Lian (2014) [31] | RCT; 66; (A)(36 ± 2)/(B)(37 ± 3); (A)(4.4 ± 2.5)/(B)(4.3 ± 2.6) | (A) TEAS plus IVF-ET (n = 33) (B) Sham AT plus IVF-ET (n = 33) | (1) The kidney deficiency syndrome score (2) HCG E2/follicle count per day (3) High-quality follicle rate | (4) High-quality embryo rate (5) Clinical pregnancy rate | (1) p < 0.01 (2–3) p < 0.05 (4–5) p > 0.05 | SP6, CV3, CV4, EX-CA1 |
| Chen (2011) [32] | RCT; 80; (A)(37.1 ± 5.3)/(B)(36.6 ± 4.6); (A)(6.4 ± 4.4)/(B)(6.1 ± 3.0) | (A) TEAS plus IVF-ET (n = 40) (B) IVF-ET (n = 40) | (1) FSH (2) E2 (3) High-quality embryo rate | (4) Cryopreservation of embryo (5) Clinical pregnancy rate | (1–5) p < 0.05 | SP6, CV3, CV4, GV3, GV4, ST25, EX-CA1, |
| Zhu (2012) [33] | RCT; 60; (A)(36.2 ± 1.0)/(B)(36.6 ± 0.8); (A)(4.4 ± 0.3)/(B)(4.5 ± 0.2) | (A) TEAS plus IVF-ET (n = 30) (B) IVF-ET (n = 30) | (1) Kidney symptom scores (2) FSH (3) E2 (4) Number of matured oocytes | (5) High-quality embryo rate (6) Cryopreservation of embryo (7) Clinical pregnancy rate | (1–7) p < 0.05 | SP6, CV3, CV4, GV3, GV4, ST25, BL23, EX-CA1 |
| Acupoints | Acupuncture | Electro-Acupuncture | Transcutaneous Electrical Acupoint Stimulation | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Zhou 2016 [23] | Xu 2016 [24] | Fernando 2016 [25] | Yan 2015 [26] | Lian 2015 [27] | Wang 2016 [28] | Zhou 2013 [29] | Chen 2009 [30] | Liu 2008 [31] | Zheng 2015 [32] | Lian 2014 [33] | Chen 2011 [34] | Zhu 2012 [35] | ||
| Sanyinjiao | SP 6 | O | O | O | O | O | O | O | O | O | ||||
| Diji | SP 8 | O | ||||||||||||
| Xuehai | SP 10 | O | O | O | ||||||||||
| Zhongji | CV 3 | O | O | O | O | O | O | |||||||
| Guanyuan | CV 4 | O | O | O | O | O | O | O | O | O | O | O | O | O |
| Qihai | CV 6 | O | ||||||||||||
| Zhongwan | CV 12 | O | ||||||||||||
| Yaoyangguan | GV 3 | O | O | |||||||||||
| Mingmen | GV 4 | O | O | O | O | |||||||||
| Baihui | GV 20 | O | O | O | ||||||||||
| Shenting | GV 24 | O | ||||||||||||
| Tianshu | ST 25 | O | O | O | O | O | O | |||||||
| Guilai | ST 29 | O | O | |||||||||||
| Zusanli | ST 36 | O | O | O | O | |||||||||
| Taixi | KI 3 | O | O | O | O | O | O | |||||||
| Fuliu | KI 7 | O | ||||||||||||
| Dahe | KI 12 | O | ||||||||||||
| Taichong | LR 3 | O | O | O | O | |||||||||
| Tongziliao | GB 1 | O | ||||||||||||
| Yanglingquan | GB 34 | O | ||||||||||||
| Geshu | BL 17 | O | ||||||||||||
| Pishu | BL 20 | O | ||||||||||||
| Shenshu | BL 23 | O | O | O | O | O | ||||||||
| Ciliao | BL 32 | O | ||||||||||||
| Zhongliao | BL 33 | O | O | |||||||||||
| Shiqizhui | EX-B 8 | O | O | |||||||||||
| Zigong | EX-CA1 | O | O | O | O | O | O | O | O | O | ||||
| Characteristic | IVF (n = 10) | Ac + IVF (n = 8) | p-Value | |
|---|---|---|---|---|
| Age (y) | 40.00 ± 3.83 | 37.88 ± 3.87 | p = 0.2279 | |
| BMI (kg/m2) | 23.14 ± 3.81 | 20.69 ± 2.99 | p = 0.1728 | |
| Duration of infertility (months) | 48.30 ± 36.59 | 33.25 ± 27.06 | p = 0.5310 | |
| Number of COH cycles | 3.90 ± 2.56 | 3.38 ± 1.92 | p = 0.6530 | |
| Hormone (Basal level) | FSH (mIU/mL) | 8.61 ± 8.25 | 17.62 ± 16.69 | p = 0.2031 |
| LH (mIU/mL) | 1.80 ± 0.95 | 7.74 ± 8.63 | p = 0.0155 | |
| E2 (pg/mL) | 88.10 ± 69.62 | 120.86 ± 69.47 | p = 0.2370 | |
| TSH (µIU/mL) | 2.70 ± 1.44 | 2.19 ± 0.89 | p = 0.6334 | |
| DHEAS (µg/dL) | 139.87 ± 58.95 | 202.49 ± 144.60 | p = 0.4082 | |
| PRL (ng/mL) | 10.34 ± 5.33 | 9.27 ± 5.07 | p = 0.5726 | |
| AMH (ng/mL) | 0.44 ± 0.36 | 0.58 ± 0.44 | p = 0.4232 | |
| Antral follicle count (Basal level) | 3.80 ± 1.03 | 3.63 ± 0.92 | p = 0.6033 | |
| Outcome | IVF (n = 10) | Ac + IVF (n = 8) | p-Value |
|---|---|---|---|
| Number of retrieved mature oocytes | 1.30 ± 1.25 | 2.75 ± 1.91 | p = 0.0916 |
| Number of fertilized oocytes | 1.10 ± 0.99 | 2.25 ± 1.39 | p = 0.0714 |
| Fertilization rate * (No. of zygotes/No. of oocytes) | 89.29 ± 19.67% (11/13) | 91.67 ± 23.57% (18/22) | p = 0.8320 |
| AMH (ng/mL) Antral follicle count | 0.47 ± 0.43 | 0.55 ± 0.36 | p = 0.4232 |
| 5.60 ± 2.37 | 5.13 ± 1.89 | p = 0.6033 |
| Characteristic | IVF (n = 10) | Ac + IVF (n = 8) | p-Value | |
|---|---|---|---|---|
| Age (y) | 40.67 ± 3.39 | 39.67 ± 2.16 | p = 0.1724 | |
| BMI (kg/m2) | 23.45 ± 3.90 | 21.89 ± 2.23 | p = 0.2284 | |
| Duration of infertility (months) | 46.67 ± 38.42 | 40.17 ± 27.99 | p = 0.5511 | |
| Number of COH cycles | 3.44 ± 2.24 | 3.33 ± 2.07 | p = 0.7933 | |
| Hormone (Basal level) | FSH (mIU/mL) | 9.35 ± 8.39 | 11.25 ± 11.54 | p = 0.7982 |
| LH (mIU/mL) | 1.83 ± 1.00 | 4.59 ± 3.27 | p = 0.0537 | |
| E2 (pg/mL) | 70.83 ± 45.77 | 117.03 ± 64.12 | p = 0.1419 | |
| TSH (µIU/mL) | 2.80 ± 1.49 | 2.00 ± 0.96 | p = 0.3450 | |
| DHEAS (µg/dL) | 132.73 ± 57.76 | 222.75 ± 165.23 | p = 0.1812 | |
| PRL (ng/mL) | 8.90 ± 2.96 | 8.29 ± 5.10 | p = 0.4908 | |
| AMH (ng/mL) | 0.40 ± 0.37 | 0.59 ± 0.435.10 | p = 0.3319 | |
| Antral follicle count (Basal level) | 3.78 ± 1.09 | 3.67 ± 1.03 | p = 0.9451 | |
| Outcome | IVF (n = 10) | Ac + IVF (n = 8) | p-Value |
|---|---|---|---|
| Number of retrieved mature oocytes | 1.33 ± 1.32 | 3.33 ± 1.86 | p = 0.0426 |
| Number of fertilized oocytes | 1.11 ± 1.05 | 2.67 ± 1.37 | p = 0.0550 |
| Fertilization rate * (No. of zygotes/No. of oocytes) | 87.50 ± 20.92% (9/10) | 88.89 ± 27.22% (16/20) | p = 0.4884 |
| AMH (ng/mL) Antral follicle count | 0.51 ± 0.44 | 0.45 ± 0.35 | p = 0.8099 |
| 5.44 ± 2.46 | 5.67 ± 1.86 | p = 0.5542 |
| Characteristic | IVF (n = 10) | Ac + IVF (n = 8) | p-Value | |
|---|---|---|---|---|
| Age (y) | 40.43 ± 3.87 | 37.88 ± 3.87 | p = 0.3096 | |
| BMI (kg/m2) | 24.19 ± 4.16 | 20.69 ± 2.99 | p = 0.1672 | |
| Duration of infertility (months) | 43.43 ± 37.84 | 33.25 ± 27.06 | p = 0.5305 | |
| Number of COH cycles | 3.86 ± 2.12 | 3.38 ± 1.92 | p = 0.3797 | |
| Hormone (Basal level) | FSH (mIU/mL) | 10.45 ± 9.35 | 17.62 ± 16.69 | p = 0.1911 |
| LH (mIU/mL) | 1.68 ± 1.10 | 7.74 ± 8.63 | p = 0.0542 | |
| E2 (pg/mL) | 54.17 ± 18.94 | 120.86 ± 69.47 | p = 0.2359 | |
| TSH (µIU/mL) | 2.89 ± 1.53 | 2.19 ± 0.89 | p = 0.8884 | |
| DHEAS (µg/dL) | 141.37 ± 63.23 | 202.49 ± 144.60 | p = 0.5414 | |
| PRL (ng/mL) | 8.74 ± 3.38 | 9.27 ± 5.07 | p = 0.6730 | |
| AMH (ng/mL) | 0.39 ± 0.40 | 0.58 ± 0.44 | p = 0.2890 | |
| Antral follicle count (Basal level) | 3.71 ± 1.25 | 3.63 ± 0.92 | p = 0.6830 | |
| Outcome | IVF (n = 10) | Ac + IVF (n = 8) | p-value |
|---|---|---|---|
| Number of retrieved mature oocytes | 1.00 ± 0.87 | 2.75 ± 1.91 | p = 0.0300 |
| Number of fertilized oocytes | 0.71 ± 0.76 | 2.25 ± 1.39 | p = 0.0305 |
| Fertilization rate * (No. of zygotes/No. of oocytes) | 87.50 ± 25.00% (8/9) | 91.67 ± 23.57% (18/22) | p = 0.6271 |
| AMH (ng/mL) Antral follicle count | 0.31 ± 0.27 | 0.55 ± 0.36 | p = 0.3537 |
| 4.86 ± 2.34 | 5.67 ± 1.86 | p = 0.9610 |
| Number of COH Cycles | Group | Number of Retrieved Mature Oocytes | p-Value | Number of Fertilized Oocytes | p-Value |
|---|---|---|---|---|---|
| ≥1 | IVF (n = 9) | 1.00 ± 0.87 | p = 0.0300 | 0.74 ± 0.76 | p = 0.0305 |
| Ac + IVF (n = 8) | 2.75 ± 1.91 | 2.25 ± 1.39 | |||
| ≥2 | IVF (n = 8) | 0.88 ± 0.83 | p = 0.0389 | 0.75 ± 0.71 | p = 0.0252 |
| Ac + IVF (n = 6) | 2.67 ± 1.86 | 2.00 ± 0.89 | |||
| ≥3 | IVF (n = 6) | 0.67 ± 0.82 | p = 0.0253 | 0.67 ± 0.82 | p = 0.0308 |
| Ac + IVF (n = 5) | 3.00 ± 1.87 | 2.20 ± 0.84 | |||
| ≥4 | IVF (n = 6) | 0.67 ± 0.82 | p = 0.0485 | 0.67 ± 0.82 | p = 0.0599 |
| Ac + IVF (n = 4) | 3.00 ± 2.16 | 2.20 ± 0.82 | |||
| ≥5 | IVF (n = 5) | 0.40 ± 0.55 | p = 0.0600 | 0.40 ± 0.55 | p = 0.0600 |
| Ac + IVF (n = 3) | 3.00 ± 2.65 | 1.67 ± 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Lee, H.; Choi, T.-Y.; Kim, J.I.; Kang, B.-K.; Lee, M.S.; Joo, J.K.; Lee, K.S.; You, S. Acupuncture for Poor Ovarian Response: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 2182. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102182
Kim J, Lee H, Choi T-Y, Kim JI, Kang B-K, Lee MS, Joo JK, Lee KS, You S. Acupuncture for Poor Ovarian Response: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(10):2182. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102182
Chicago/Turabian StyleKim, Jihyun, Hoyoung Lee, Tae-Young Choi, Joong Il Kim, Byoung-Kab Kang, Myeong Soo Lee, Jong Kil Joo, Kyu Sup Lee, and Sooseong You. 2021. "Acupuncture for Poor Ovarian Response: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 10: 2182. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10102182