
Enhanced Recovery after Renal Transplantation Decreases Recipients’ Urological Complications and Hospital Stay: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Eligibility Criteria
- Randomized Clinical Trials (RCTs), retrospective and prospective cohort studies.
- Studies that included adults with ESRD undergoing renal transplantation.
- Studies including multiple ERAS interventions or streamlined protocols. Any intervention that aimed to minimize the peri-operative physiologic dysfunction and the surgical stress response in order to promote a swifter return to normal function was considered as an ERAS intervention. For a study to meet our eligibility criteria, two or more synergistic ERAS interventions were required.
- Studies where traditional perioperative practice was the main comparator.
- Studies reporting complications, grafts’ and patients’ survival, duration of hospitalization, unplanned readmissions and quality of life data in the intervention and the comparator groups.
- Studies in animals or cadavers, comments/letters to the editor, opinion papers, case studies, systematic reviews, meta-analyses, congress abstracts when an analytic report was not available and studies in which multiple synergistic ERAS interventions were not included.
- Studies enrolling pediatric patients or patients undergoing any different operation other than renal transplantation, as well as studies that excluded participants with significant post-operative complications.
- Studies involving a single intervention. Our meta-analysis seeks to investigate the synergistic effect of different ERAS interventions (care bundles) in the perioperative care of kidney transplant recipients. Thus, articles on solitary interventions were not included.
- Non-comparative studies and articles in which the relevant outcome data were not reported.
2.3. Search Strategy
2.4. Selection of Studies
2.5. Data Collection
2.6. Extracted Data
- Recipients’ Baseline Characteristics: gender (number of male recipients, % percentage), age (in years, mean ± standard deviation or median, (range)), Body Mass Index (BMI in kg/m2), recipients’ smoking history, recipients’ comorbidities, hemodialysis (number of recipients receiving hemodialysis, % percentage), time in hemodialysis (in months), previous renal transplant (number of recipients who had previous renal transplant, % percentage), deceased donor kidney transplant (number of recipients receiving kidney from deceased donors, % percentage), diabetic nephropathy (number, % percentage), left kidney transplant (number, % percentage), ABO incompatibility with donor (number, % percentage), positive tissue crossmatch (number, % percentage), HLA mismatch (number, % percentage), graft’s warm ischemia time (in hours), cold ischemia time (in hours) and overall ischemia time (in hours).
- Enhanced Recovery and traditional practice interventions: preoperatively, intraoperatively and postoperatively (qualitative data).
- Recipients’ outcomes:
- One-year post-transplant patient survival (number, % percentage).
- Complications: overall postoperative complications, Clavien-Dindo I–II complications, Clavien-Dindo III–V complications, urological complications, urinary leakage, ureteral stenosis/obstruction, urinary tract infection (UTI), vascular complications, vascular anastomotic leak, renal artery stenosis, renal vein/renal artery thrombosis, symptomatic lymphocele, delayed graft function, graft rejection, electrolyte disorders, gastrointestinal complications, infections other than UTI, other complications (number, % percentage).
- One-year post-transplant graft survival (number, % percentage).
- Length of Stay (LOS) (in days, mean ± standard deviation or median, (range)).
- Readmissions (number, % percentage).
- Reasons for readmissions (qualitative data).
- Adverse events (qualitative data).
- Quality of recovery score [5]
2.7. Risk of Bias in Individual Studies
2.8. Summary Measures
2.9. Synthesis of the Results
2.10. Risk of Bias across Studies
2.11. Additional Analyses
3. Results
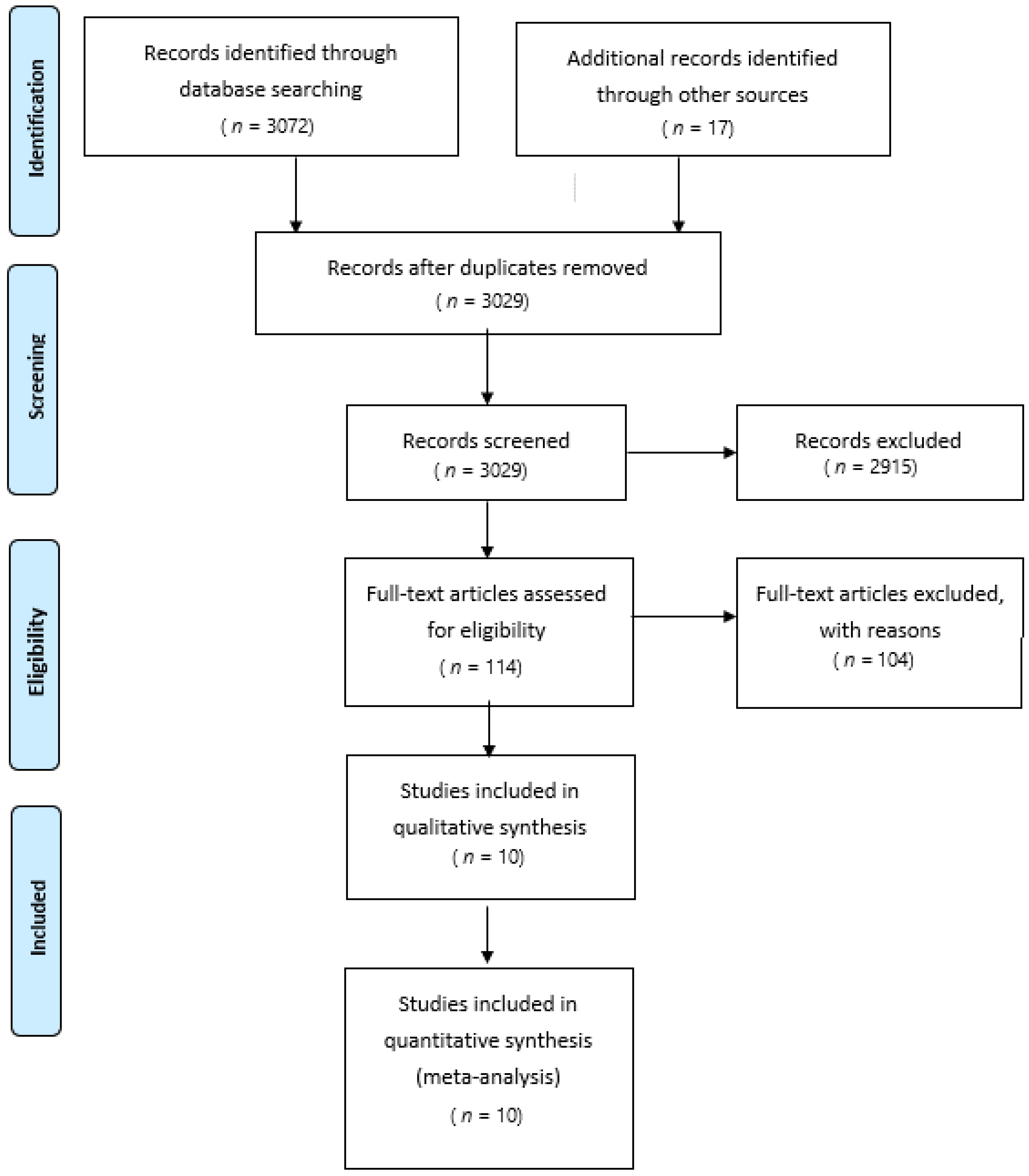
3.1. Selection of Studies
3.2. Study Characteristics and Bias Assessment
3.3. Included Studies’ Results
3.4. Synthesis of Results
3.4.1. Qualitative Synthesis
3.4.2. Quantitative Synthesis
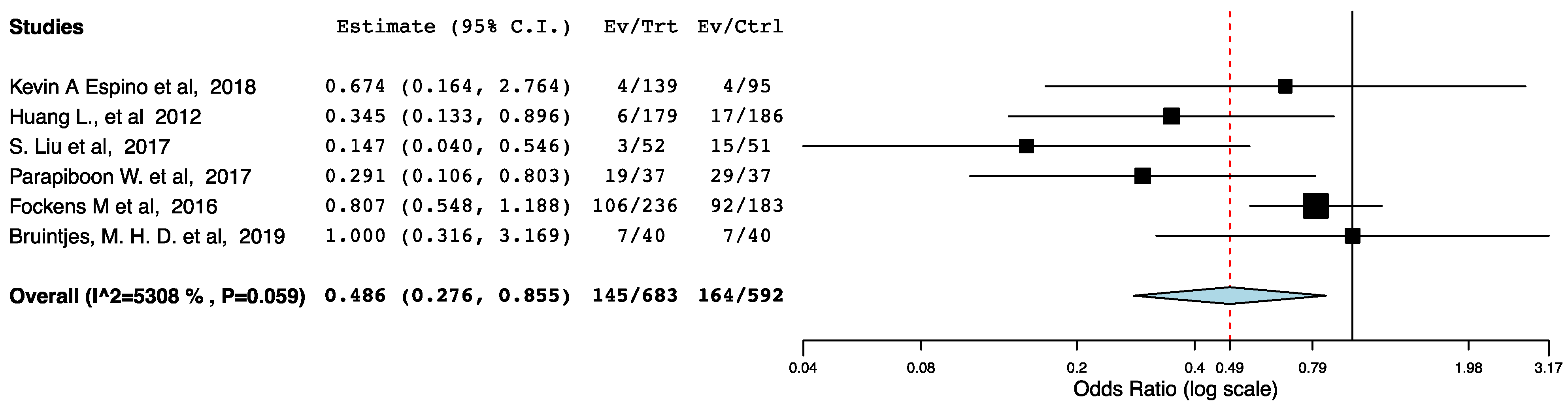
Post-Operative Complications
LOS
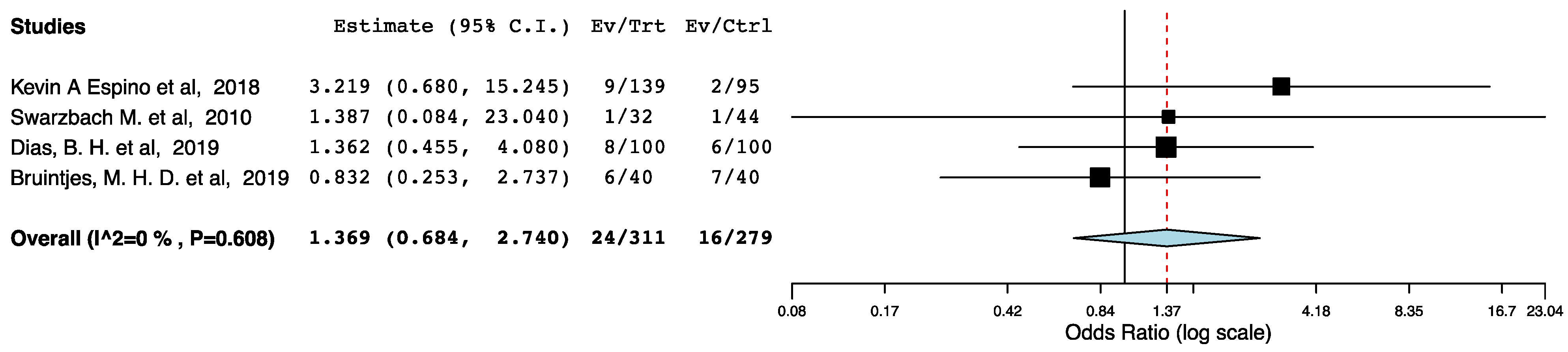
Readmission Rates
One-Year Post-Transplant Graft Survival
One-Year Post-Transplant Patient Survival
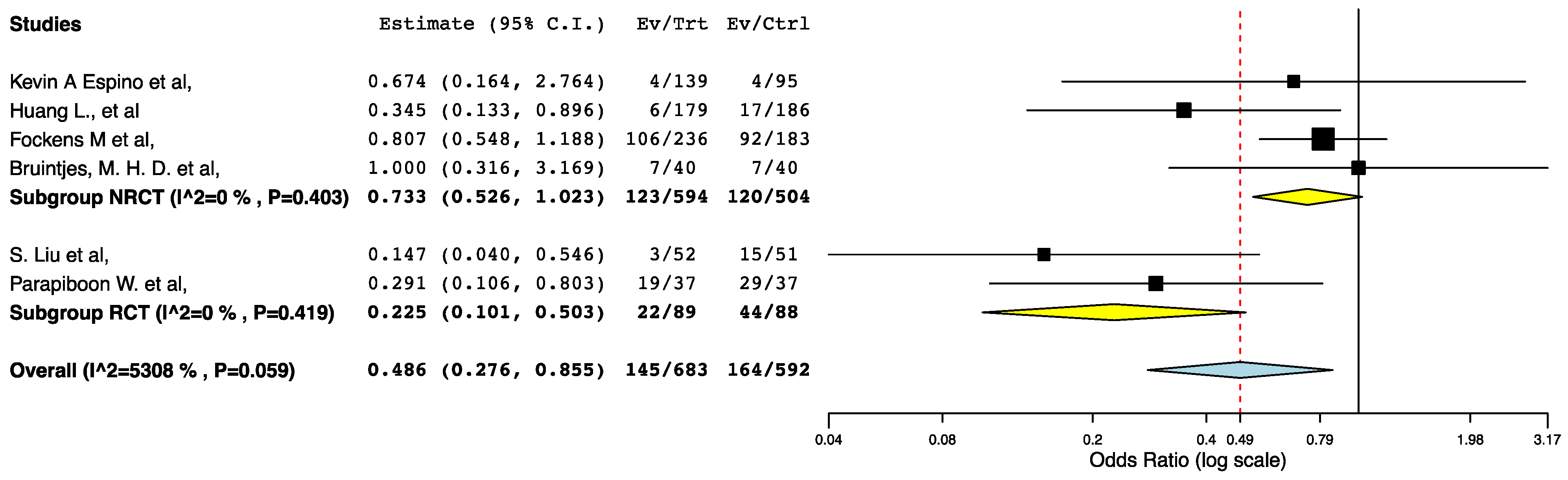
Additional Analyses
4. Discussion
4.1. Summary of Evidence
4.2. Implications of Study Findings
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic Review: Kidney Transplantation Compared With Dialysis in Clinically Relevant Outcomes. Arab. Archaeol. Epigr. 2011, 11, 2093–2109. [Google Scholar] [CrossRef]
- Global Observatory on Donation and Transplantation [Internet]. GODT. Available online: http://www.transplant-observatory.org (accessed on 15 October 2020).
- De Wit, G.A.; Ramsteijn, P.G.; de Charro, F.T. Economic evaluation of end stage renal disease treatment. Health Policy. 1998, 44, 215–232. [Google Scholar] [CrossRef]
- Scott, M.J.; Baldini, G.; Fearon, K.C.H.; Feldheiser, A.; Feldman, L.S.; Gan, T.J. Enhanced Recovery After Surgery (ERAS) for gas-trointestinal surgery, part 1: Pathophysiological considerations. Acta Anaesthesiol. Scand. 2015, 59, 1212–1231. [Google Scholar] [CrossRef] [Green Version]
- Myles, P.S.; Weitkamp, B.; Jones, K.; Melick, J.; Hensen, S. Validity and reliability of a postoperative quality of recovery score: The QoR-40. Br. J. Anaesth. 2000, 84, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Bruintjes, M.H.D.; Langenhuijsen, J.F.; Kusters, A.; Hilbrands, L.B.; d’Ancona, F.C.H.; Warlé, M.C. Double J stent is superior to exter-nally draining ureteric stent in enhancing recovery after kidney transplantation—A prospective cohort study. Int. J. Surg. 2019, 71, 175–181. [Google Scholar] [CrossRef]
- Dias, B.H.; Rana, A.A.M.; Olakkengil, S.A.; Russell, C.H.; Coates, P.T.H.; Clayton, P.A.; Bhattacharjya, S. Development and implementation of an enhanced recovery after surgery protocol for renal transplantation. ANZ J. Surg. 2019, 89, 1319–1323. [Google Scholar] [CrossRef]
- Espino, K.A.; Narvaez, J.R.F.; Ott, M.C.; Kayler, L.K. Benefits of multimodal enhanced recovery pathway in patients undergoing kidney transplantation. Clin. Transplant. 2018, 32, e13173. [Google Scholar] [CrossRef]
- Halawa, A.; Rowe, S.; Roberts, F.; Nathan, C.; Hassan, A.; Kumar, A.; Suvakov, B.; Edwards, B.; Gray, C. A Better Journey for Patients, a Better Deal for the NHS: The Successful Implementation of an Enhanced Recovery Program After Renal Transplant Surgery. Exp. Clin. Transplant. 2018, 16, 127–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simforoosh, N.; Obeid, K.; Javanmard, B.; Rezaeetalab, G.H.; Razmjoo, S.; Soltani, M.H. Stent Removal in 200 Kidney Transplant Recipients: Nonoperative Versus Endoscopic Removal. Exp. Clin. Transplant. 2016, 14, 385–388. [Google Scholar]
- Fockens, M.M.; Alberts, V.P.; Bemelman, F.J.; Laguna Pes, M.P.; Idu, M.M. Internal or External Stenting of the Ureterovesical Anas-tomosis in Renal Transplantation. Urol. Int. 2015, 96, 152–156. [Google Scholar] [CrossRef]
- Huang, L.; Wang, X.; Ma, Y.; Wang, J.; Tao, X.; Liao, L.; Tan, J. A Comparative Study of 3-Week and 6-Week Duration of Double-J Stent Placement in Renal Transplant Recipients. Urol. Int. 2012, 89, 89–92. [Google Scholar] [CrossRef]
- Schwarzbach, M.; Bönninghoff, R.; Harrer, K.; Weiss, J.; Denz, C.; Schnülle, P.; Birck, R.; Post, S.; Ronellenfitsch, U. Effects of a clinical pathway on quality of care in kidney transplantation: A non-randomized clinical trial. Langenbeck Arch. Surg. 2009, 395, 11–17. [Google Scholar] [CrossRef]
- Parapiboon, W.; Wiengpon, K.; Kitiyakara, C.; Phakdeekitcharoen, B.; Leenanupunth, C.; Wisoot, K. Early ureteric stent re-moval reduces urinary tract infection in kidney transplant recipients: A randomized controlled trial. Trends Transplant. 2017, 10, 1–6. [Google Scholar] [CrossRef]
- Liu, S.; Luo, G.; Sun, B.; Lu, J.; Zu, Q.; Yang, S.; Zhang, X.; Dong, J. Early Removal of Double-J Stents Decreases Urinary Tract Infections in Living Donor Renal Transplantation: A Prospective, Randomized Clinical Trial. Transplant. Proc. 2017, 49, 297–302. [Google Scholar] [CrossRef]
- Song, W.; Wang, K.; Zhang, R.; Dai, Q.; Zou, S. The Enhanced Recovery after Surgery (ERAS) Program in Liver Surgery: A Me-ta-Analysis of Randomized Controlled Trials; SpringerPlus: Berlin/Heidelberg, Germany, 2016; Volume 25. [Google Scholar]
- Greco, M.; Capretti, G.; Beretta, L.; Gemma, M.; Pecorelli, N.; Braga, M. Enhanced Recovery Program in Colorectal Surgery: A Me-ta-analysis of Randomized Controlled Trials. World J. Surg. 2013, 38, 1531–1541. [Google Scholar] [CrossRef]
- Visioni, A.; Shah, R.; Gabriel, E.; Attwood, K.; Kukar, M.; Nurkin, S. Enhanced Recovery After Surgery for Noncolorectal Surgery? Ann. Surg. 2018, 267, 57–65. [Google Scholar] [CrossRef]
- Prionas, A.; Craddock, C.; Papalois, V. Feasibility, Safety and Efficacy of Enhanced Recovery After Living Donor Nephrectomy: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 10, 21. [Google Scholar] [CrossRef]
- Wilson, C.H.; Bhatti, A.A.; Rix, D.A.; Manas, D.M. Routine Intraoperative Stenting for Renal Transplant Recipients. Transplant 2005, 80, 877–882. [Google Scholar] [CrossRef] [Green Version]
- Visser, I.J.; Van Der Staaij, J.P.T.; Muthusamy, A.; Willicombe, M.; LaFranca, J.A.; Dor, F.J.M.F. Timing of Ureteric Stent Removal and Occurrence of Urological Complications after Kidney Transplantation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 689. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Mongha, R. Transplant ureter should be stented routinely. Indian J. Urol. 2010, 26, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Mangus, R.S.; Haag, B.W. Stented versus Nonstented Extravesical Ureteroneocystostomy in Renal Transplantation: A Metaanalysis. Arab. Archaeol. Epigr. 2004, 4, 1889–1896. [Google Scholar] [CrossRef]
- Friedersdorff, F.; Weinberger, S.; Biernath, N.; Plage, H.; Cash, H.; El-Bandar, N. The Ureter in the Kidney Transplant Setting: Ureteroneocystostomy Surgical Options, Double-J Stent Considerations and Management of Related Complications. Curr. Urol. Rep. 2020, 21, 3. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year | Study Size (ERAS/Standard Care) | Length of Follow Up | Risk of Bias | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Confounding | Selection of Participants | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of the Reported Result | Overall | Direction of Bias | |||
| Bruintjes, M. H. D. et al., 2019 [8] | 80 (40/40) | 14 days | Serious | Serious | Low | Low | Low | Moderate | Moderate | Serious | Favors ERAS |
| Dias, B. H. et al., 2019 [9] | 200 (100/100) | 365 days | Serious | Low | Serious | Low | Low | Low | Low | Serious | Unpredictable |
| Kevin A Espino et al., 2018 [10] | 234 (139/95) | 90 days | Serious | Low | Low | Moderate | Low | Low | Low | Serious | Favors Standard Care |
| Halawa, A. et al., 2018 [11] | 286 (135/151) | No info | Serious | Low | Serious | Low | Low | Low | Low | Serious | Unpredictable |
| Simforoosh N et al., 2016 [12] | 200 (100/100) | 365 days | Critical | No info | Serious | Low | Low | Low | Low | Critical | Unpredictable |
| Fockens M et al., 2016 [13] | 419 (236/183) | 365 days | Critical | Low | Low | Low | Moderate | Low | Low | Critical | Favors Standard Care |
| Huang L., et al. 2012 [14] | 365 (179/186) | 90 days | Low | Low | Low | Low | Low | Low | Low | Low | Towards null |
| Swarzbach M. et al., 2010 [15] | 76 (32/44) | 365 days | Serious | Low | Low | Low | Low | Low | Low | Serious | Unpredictable |
| Authors, Year | Study Size (ERAS/Standard Care) | Length of Follow Up | Risk of Bias | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Randomization Process | Effect of Assignment to Intervention | Effect of Adhering to Intervention | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall | Direction of Bias | |||
| S. Liu et al., 2017 [17] | 103 (52/51) | 90 days | Low | Low | Low | Some Concerns | Low | Low | Some Concerns | Towards null |
| Parapiboon W. et al., 2017 [16] | 74 (37/37) | 30 days | Low | Some Concerns | Some Concerns | Low | Low | Low | Some Concerns | Unpredictable |
| Authors, Year | Recipients Age | Male Recipients | Recipients’ BMI | Recipients’ Comorbidities | Diabetic Nephropathy | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | |
| Non-Randomized Studies | ||||||||||
| Bruintjes, M. H. D. et al., 2019 [8] | 46.4 ± 15.4 | 53.5 ± 13.0 | 25/40 (62.5%) | 17/40 (42.5%) | 25.2 ± 3.3 | 24.3 ± 3.6 | ASA (1/2/3/4): 0/8/30/2, Diabetes: 5/40 (12.5%) | ASA (1/2/3/4): 1/11/28/0, Diabetes: 3/40 (7.5%) | - | - |
| Dias, B. H. et al., 2019 [9] | 51.4± 14.2 | 53.1± 14.3 | 54/100 (54%) | 64/100 (64%) | - | - | Diabetes: 32/100 (32%), Hypertension: 72(72%), Previous abdominal surgery: 7/100 (7%) | Diabetes: 31/100 (31%), Hypertension: 69/100 (69%), previous abdominal surgery 6/100 (6%) | - | - |
| Kevin A Espino et al., 2018 [10] | - | - | 78/ 139 (56.1%) | 58/95 (61.1%) | - | - | Diabetes: 58/139 (41.7%) | Diabetes: 30/95 (31.6%) | - | - |
| Halawa, A. et al., 2018 [11] | 48 | 50 | 127/135 (94%) | 148/151 (98%) | - | - | - | - | - | - |
| Fockens M et al., 2016 [12] | 55.0± 13.3 | 54.2± 12.8 | 145/236 (61.4%) | 111/183 (60.7%) | 27.2 ± 5.4 | 25.5 ± 4.3 | Diabetes: 49/236 (20.8%) Cardiac history: 29/236 (12.3%) | Diabetes: 48/183 (26.2%) Cardiac history: 31/183 (26.2%) | 49/236 (40.8%) | 23/183 (12.6%) |
| Simforoosh N et al., 2016 [13] | 42 (18–58) | 40 (19–60) | 60/100 (60%) | 36/100 (36%) | 26.02 ± 5.87 | 24.2 ± 5.18 | Diabetes: 72/100 (72%) | Diabetes: 73/100 (73%) | - | - |
| Huang L., et al. 2012 [14] | 43.5 ± 8.1 | 42.8 ± 7.5 | 133/179 (74.3%) | 137/186 (73.6%) | - | - | - | - | 4/179 (2.2%) | 5/186 (2.7%) |
| Swarzbach M. et al., 2010 [15] | 55.5 | 48.9 | 20/32 (62.5%) | 29/44(65.9%) | - | - | ASA (1/2/3/4):0/23/9/0 | ASA (1/2/3/4): 0/25/19/0 | - | - |
| Randomized Clinical Trials | ||||||||||
| S. Liu et al., 2017 [17] | 34.9± 11.9 | 35.4 ± 12.6 | 41/52 (78%) | 38/51 (74%) | 22.5± 3.7 | 22.1 ± 3.8 | - | - | - | - |
| Parapiboon W. et al., 2017 [16] | 42.7 ± 12.4 | 43.8 ± 14.1 | 24/37 (65%) | 27/37(73%) | - | - | Diabetes: 9/37(24.3%) | Diabetes: 6/37 (16.2%) | 9/37 (24.3%) | 6/37 (16.2%) |
| Authors, Year | Hemodialysis | Time in Dialysis | Previous Renal Transplant | Deceased Donors | Cold Ischemia Time | Overall Ischemia Time | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | |
| Non-Randomized Studies | ||||||||||||
| Bruintjes, M. H. D. et al., 2019 [8] | 28/40 (70.0%) | 20 (50.0%) | - | - | - | - | 0/40 (0%) | 0/40 (0%) | - | - | 2.5 ± 0.41 | 2.5 ± 0.54 |
| Dias, B. H. et al., 2019 [9] | - | - | 18.8± 7.2 | 19.2± 6.5 | 12/100 (12%) | 13/100 (13%) | 71/100 (71%) | 78(78%) | - | - | 4.7 ± 2.5 | 3.7 ± 0.5 |
| Kevin A Espino et al., 2018 [10] | - | - | - | - | 20/139 (14.4%) | 13/95 (13.7%) | 125/139 (89.9%) | 84/95 (88.4%) | - | - | - | - |
| Halawa, A. et al., 2018 [11] | - | - | - | - | - | - | 75/135 (55.55%) | 66/155 (43.7%) | - | - | - | - |
| Fockens M et al., 2016 [12] | - | - | - | - | 22/236 (9.3%) | 35/183 (13.7%) | 236/236 (100%) | 183/183 (100%) | 17.5 ± 6.2 | 17.7 ± 6.4 | - | - |
| Simforoosh N et al., 2016 [13] | - | - | - | - | - | - | 24/100 (24%) | 33/100 (33%) | - | - | - | - |
| Huang L., et al. 2012 [14] | 172/179 (96.1%) | 175/186 (94.1%) | 24.8 ± 5.6 | 25.7 ± 4.8 | - | - | 179/179 (100%) | 186/186 (100%) | - | - | - | - |
| Swarzbach M. et al., 2010 [15] | - | - | - | - | - | - | 29/32 (90.6%) | 36/44 (81.8%) | 14.7 | 13.6 | - | - |
| Randomized Clinical Trials | ||||||||||||
| S. Liu et al., 2017 [17] | - | - | - | - | - | - | 0/52 (0%) | 0/51(0%) | - | - | 2.3 ± 0.6 | 2.4 ± 0.72 |
| Parapiboon W. et al., 2017 [16] | 36/37 (97.3%) | 31/37 (83.2%) | 45 | 24 | - | - | 15/37(40.5%) | 16/37 (43.3%) | - | - | - | - |
| A. ERAS Interventions: preoperatively |
| 1. Outpatient workup: body weight optimization, blood pressure control, spirometry and smoking cessation. |
| 2. Outpatient consultation for provision of information on the ERAS protocol, for managing expectations with regards to length of hospital stay and for obtaining informed consent. |
| 3. Carbohydrate loading in non-diabetic patients. Less than 4 h fasting, preoperatively. Avoid maintenance fluids in these patients during the immediate preoperative period. |
| 4. Antibiotic Prophylaxis. |
| 5. Application of Thrombo-Embolus Deterrent (TED) Stockings. |
| B. ERAS Interventions: intraoperatively |
| 1. Urinary catheter placement. |
| 2. JJ stent placement with an intention for early removal postoperatively. The stent can be attached to the tip of the catheter. |
| 3. Surgical Drain placement in the retroperitoneal space/transplanted iliac |
| 4. Wound infiltration catheter placement for continuous administration of local anesthetic. Alternatively, long-lasting local anesthetic injection in the subfascial plane. |
| 5. Goal Directed Fluid Therapy with non-invasive cardiac output monitoring (transesophageal doppler) throughout the procedure is preferable. Target MAP of 75 mmHg. When the need for inotropes or thymocyte globulin induction is anticipated, a central venous catheter can be inserted. |
| 6. Opioid + non-opioid intraoperative analgesia |
| 7. Immunosuppression induction when necessary (basiliximab/thymocyte globulin) |
| C. ERAS Interventions: postoperatively |
| 1. Continue immunosuppression induction if necessary (basiliximab/ thymocyte globulin). Early initiation of tacrolimus/cyclosporine on post-operative day 1 (POD1). Target levels standardized for all patients. Use also of MMF/myfortic ± corticosteroid taper for maintenance. |
| 2. UTI antibiotic prophylaxis. |
| 3. Thromboprophylaxis with compression stockings and enoxaparin. |
| 4. Post-operative analgesia with paracetamol, morphine/fentanyl PCA (early wean before POD2) and local anesthetic infusion through the wound infiltration catheter (removal on POD2). When fluids are tolerated, convert IV analgesics to oral. |
| 5. Start sips of water and ice chips/chewing gum on POD0. Minimal IV fluids on POD0, stop IV fluids on POD1. Start liquid diet on POD1, build up to solid diet. Daily laxatives. Castor oil on POD1. |
| 6. Start early mobilization on POD1 along with respiratory exercises. Gradually advance mobilization. |
| 7. Surgical Drain removal on POD2 (if daily drain output ≤ 50 mls) |
| 8. Urinary Catheter Removal on POD2 (only if JJ stent is not attached to the catheter, otherwise catheter remains) |
| 9. POD4 is the target day for hospital discharge. Conditions that should be met: (i) clinical parameters within normal limits (no tachycardia, no temperature, no tachypnoea, no desaturation, no hypo/hypertension); (ii) adequate mobilization; (iii) solid diet tolerated, post-op ileus resolved; (iv) pain controlled with oral analgesics; (v) adequate education over the use of immunosuppressive drugs; (vi) adequate home support |
| 10. Telephone number for consultation available 24/7. If necessary, on-site post-kidney transplant dialysis for 3–4 weeks and use of walk-in infusion centers. Post-discharge outpatient review with surgeons and physicians in 24 h with subsequent visits tailored to patient needs |
| 11. Outpatient early JJ stent removal between POD7 and POD21: either with simple removal of the urinary catheter (if stent and catheter are attached) or with flexible cystoscopy (if catheter has been removed and JJ stent was not attached) |
| Authors, Year | Overall Complications | Clavien-Dindo I and II Complications | Clavien-Dindo III-V Complications | Recipients’ LOS | Recipients’ Readmissions | Graft Survival up to 1-Year Post Op | Recipients’ one-Year Survival | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ERAS | Standard Care | ERAS | Standard Care | ERAS | ERAS | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | |
| Non-Randomized Studies | ||||||||||||||
| Bruintjes, M. H. D. et al., 2019 [8] | 22/40 (55%) | 28/40 (70%) | 16/40 (40%) | 21/40 (52.5%) | 6/40 (15%) | 7/40 (17.5%) | 6.20 ± 1.56 | 7.95 ± 2.12 | - | - | - | - | - | - |
| Dias, B. H. et al., 2019 [9] | 12/100 (12%) | 11/100 (11%) | 4/100 (4%) | 5/100 (5%) | 8/100 (8%) | 6/100 (6%) | 5 (3–16) | 7 (5–14) | 11/100 (11%) | 9/100 (9%) | 96/98 (98%) | 94/97 (97%) | - | - |
| Kevin A Espino et al., 2018 [10] | - | - | - | - | 9/139 (6.5%) | 2/95 (2.1%) | 4.59 ± 0.76 | 5.65 ± 0.9 | 38/139 (27.3%) | 26/95 (27.4%) | - | - | 138/139 (99.29%) | 95/95 (100%) |
| Halawa, A. et al., 2018 [11] | - | - | - | - | - | - | 5 [3,4,5,6,7,8,9,10,11,12] | - | 7/135 (5.1%) | - | - | - | - | - |
| Fockens M et al., 2016 [12] | - | - | - | - | - | - | 15.0 ± 11.8 | 14.9 ± 8.8 | 37/236 (15.7%) | 23/183 (12.6%) | 220/236 (93.2%) | 174/183 (95.1%) | - | - |
| Simforoosh N et al., 2016 [13] | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Huang L., et al. 2012 [14] | - | - | - | - | - | - | - | - | - | - | - | - | 179/179 (100%) | 186/186 (100%) |
| Swarzbach M. et al., 2010 [15] | 10/32 (31.3%) | 12/44 (27.3%) | 9/32 (28.1%) | 9/32 (28.1%) | 1/32 (3.1%) | 1/32 (3.1%) | 18.3 ± 3.1 | 21.4 ± 3.2 | - | - | 30/32 (93%) | 41/44 (93%) | 31/32 (96.9%) | 43/44 (97.7%) |
| Randomized Clinical Trials | ||||||||||||||
| S. Liu et al., 2017 [17] | - | - | - | - | - | - | - | - | - | - | - | - | 52/52 (100%) | 51/51 (100%) |
| Parapiboon W. et al., 2017 [16] | - | - | - | - | - | - | - | - | - | - | - | - | 37/37 (100%) | 37/37 (100%) |
| Authors, Year | Urological Complications | Urinary Leakage | Ureteral Stenosis/Obstruction | UTI | ||||
|---|---|---|---|---|---|---|---|---|
| ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | |
| Non-Randomized Studies | ||||||||
| Bruintjes, M. H. D. et al., 2019 [8] | 7/40 (17.5%) | 7/40 (17.5%) | 1/40 (2.5%) | 2/40 (5%) | 1/40 (2.5%) | 3/40 (7.5%) | 2/40 (5%) | 0/40 (0%) |
| Dias, B. H. et al., 2019 [9] | - | - | - | - | - | - | - | - |
| Kevin A Espino et al., 2018 [10] | 4/139 (2.9%) | 4/95 (4.2%) | 2/139 (1.4%) | 2/95 (2.1%) | - | - | - | - |
| Halawa, A. et al., 2018 [11] | - | - | - | - | - | - | - | - |
| Fockens M et al., 2016 [12] | 106/236 (44.9%) | 92/183 (50.3%) | 2/236 (0.9%) | 3/183 (1.6%) | 7/236 (3%) | 15/183 (8.2%) | 97/236 (41.1%) | 75/183 (45%) |
| Simforoosh N et al., 2016 [13] | - | - | 3/100 (3%) | 4/100 (4%) | 1/100 (1%) | 2/100 (2%) | 20/100 (20%) | 29/100 (29%) |
| Huang L., et al. 2012 [14] | 6/179 (3.3%) | 17/186 (9.1%) | 2/179 (1.1%) | 2/186 (1.1%) | 0/179 (0%) | 0/186 (0%) | 4/179 (2.2%) | 15/186 (8.1%) |
| Swarzbach M. et al., 2010 [15] | - | - | - | - | - | - | - | - |
| Randomized Clinical Trials | ||||||||
| S. Liu et al., 2017 [17] | 3/52 (5.8%) | 15/51 (29.4%) | 0/52 (0%) | 0/51 (0%) | 0/52 (0%) | 0/51 (0%) | 3/52 (5.8%) | 15/51 (29.4%) |
| Parapiboon W. et al., 2017 [16] | 19/37 (51.3%) | 29/37 (78.4%) | 4/37 (10.8%) | 2/37 (5.4%) | 0/37 (0%) | 0/37 (0%) | 15/37 (40.5%) | 27/37 (72.9%) |
| Authors, Year | Symptomatic Lymphocele | Delayed Graft Function | Acute Rejection | Gastroenterological Complications | Infection, Other than UTI | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | ERAS | Standard Care | |
| Non-Randomized Studies | ||||||||||
| Bruintjes, M. H. D. et al., 2019 [8] | 5/40 (12.5%) | 1/40 (2.5%) | 0/40 (0%) | 1/40 (2.5%) | 2/40 (5%) | 1/40 (2.5%) | 4/40 (10%) | 12/40 (30%) | 2/40 (5%) | 7/40 (17.5%) |
| Dias, B. H. et al., 2019 [9] | - | - | 31/100 (31%) | 36/100 (36%) | - | - | - | - | - | - |
| Kevin A Espino et al., 2018 [10] | - | - | 58/139 (46.4%) | 21/95 (25%) | - | - | 51/135 (37.7%) | 19/95 (20%) | - | - |
| Fockens M et al., 2016 [12] | 8/236 (3.4%) | 8/183 (4.4%) | 142/236 (60.2%) | 83/183 (45.4%) | 31/236 (13.1%) | 36/183 (19.7%) | - | - | - | - |
| Simforoosh N et al., 2016 [13] | - | - | - | - | 2/100 (2%) | 1/100 (1%) | - | - | 1/100 (1%) | 2/100 (2%) |
| Swarzbach M. et al., 2010 [15] | - | - | 2/32 (6.3%) | 10/44 (22.7%) | 0/32 (0%) | 5/44 (11.4%) | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prionas, A.; Craddock, C.; Papalois, V. Enhanced Recovery after Renal Transplantation Decreases Recipients’ Urological Complications and Hospital Stay: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2286. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112286
Prionas A, Craddock C, Papalois V. Enhanced Recovery after Renal Transplantation Decreases Recipients’ Urological Complications and Hospital Stay: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(11):2286. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112286
Chicago/Turabian StylePrionas, Apostolos, Charles Craddock, and Vassilios Papalois. 2021. "Enhanced Recovery after Renal Transplantation Decreases Recipients’ Urological Complications and Hospital Stay: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 11: 2286. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112286