
Zinc Administration and Improved Serum Markers of Hepatic Fibrosis in Patients with Autoimmune Hepatitis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
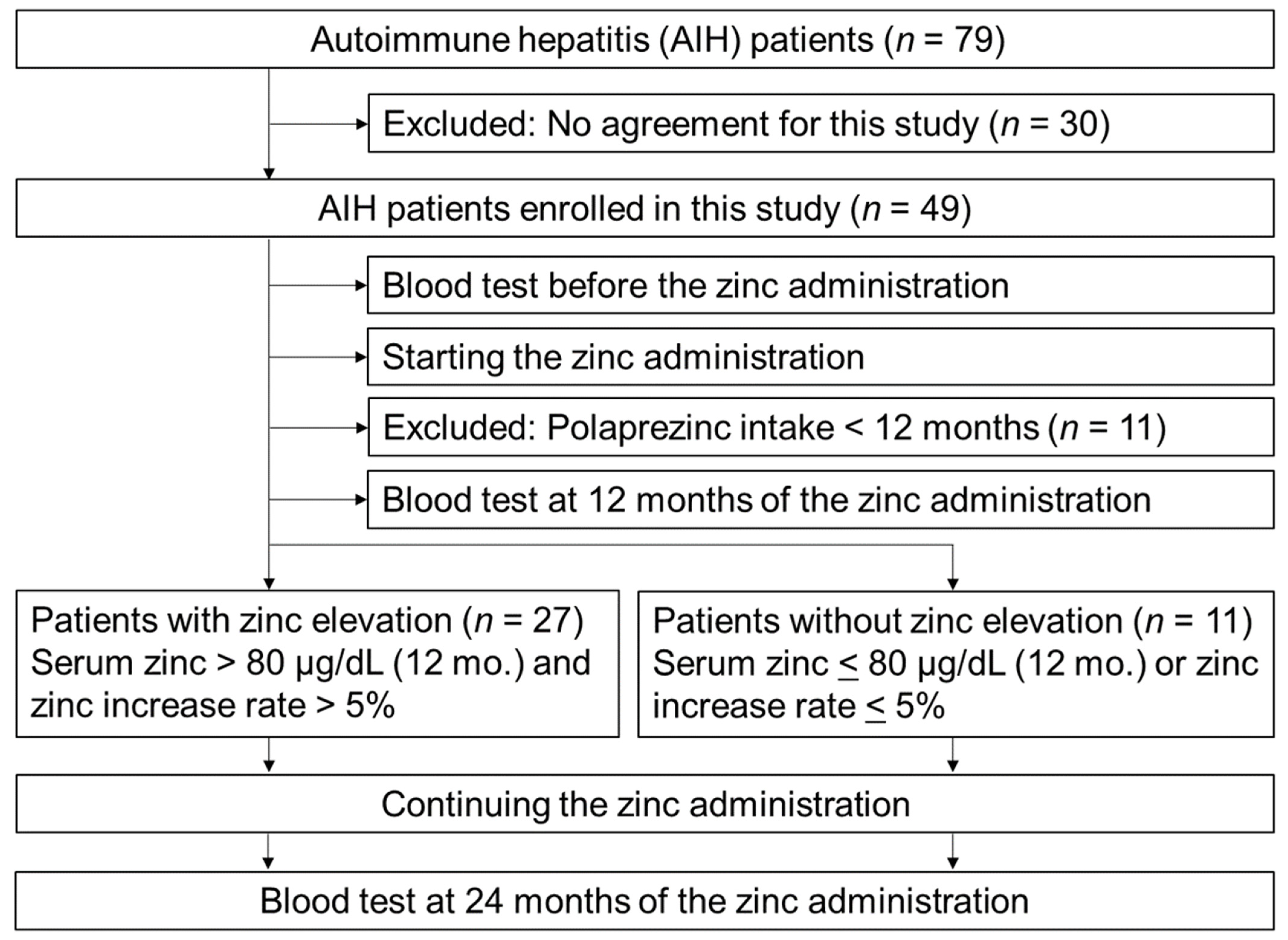
2.1. Patients
2.2. Laboratory Assessments
2.3. Histological Assessments
2.4. Statistical Analyses and Ethical Issues
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AIH | autoimmune hepatitis |
| ALT | alanine aminotransferase |
| MMP | matrix metalloproteinase |
| PBC | primary biliary cirrhosis |
| TIMP | tissue inhibitor of matrix metalloproteinase |
| TGF-β | transforming growth factor-β |
References
- Tanaka, A.; Mori, M.; Matsumoto, K.; Ohira, H.; Tazuma, S.; Takikawa, H. Increase Trend in the Prevalence and male-to-female Ratio of Primary Biliary Cholangitis, Autoimmune Hepatitis, and Primary Sclerosing Cholangitis in Japan. Hepatol. Res. 2019, 49, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A. Emerging Novel Treatments for Autoimmune Liver Diseases. Hepatol. Res. 2019, 49, 489–499. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef] [PubMed]
- Yoshizawa, K.; Matsumoto, A.; Ichijo, T.; Umemura, T.; Joshita, S.; Komatsu, M.; Tanaka, N.; Tanaka, E.; Ota, M.; Katsuyama, Y.; et al. Long-term outcome of Japanese patients with type 1 Autoimmune hepatitis. Hepatology 2012, 56, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Chew, L.-C.; Maceda-Galang, L.M.; Tan, Y.K.; Chakraborty, B.; Thumboo, J. Pneumocystis Jirovecii Pneumonia in Patients With Autoimmune Disease on High-Dose Glucocorticoid. J. Clin. Rheumatol. 2015, 21, 72–75. [Google Scholar] [CrossRef]
- Brenner, E.J.; Ungaro, R.C.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Ruemmele, F.M.; et al. Corticosteroids, but not TNF antagonists, are associated with adverse COVID-19 outcomes in patients with inflammatory bowel diseases: Results from an international registry. Gastroenterology 2020, 159, 481–491. [Google Scholar] [CrossRef]
- Consani Fernández, S.A.; Díaz Cuña, C.L.; Fernández Rey, L.; Rostán Sellanes, S.; Maciel Oleggini, G.; Facal Castro, J.A. Infections in systemic autoimmune diseases. Reumatol. Clin. 2020, in press. [Google Scholar]
- Dhaliwal, H.K.; Hoeroldt, B.; Dube, A.K.; McFarlane, E.; Underwood, J.C.; Karajeh, M.A.; Gleeson, D. Long-Term Prognostic Significance of Persisting Histological Activity Despite Biochemical Remission in Autoimmune Hepatitis. Am. J. Gastroenterol. 2015, 110, 993–999. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Björnsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients With nonalcoholic fatty liver disease. Gastroenterology 2015, 149, 389–397. [Google Scholar] [CrossRef] [Green Version]
- Niederau, C.; Lange, S.; Heintges, T.; Erhardt, A.; Buschkamp, M.; Hürter, D.; Nawrocki, M.; Kruska, L.; Hensel, F.; Petry, W.; et al. Prognosis of chronic hepatitis C: Results of a large, prospective cohort study. Hepatology 1998, 28, 1687–1695. [Google Scholar] [CrossRef] [PubMed]
- Werner, M.; Wallerstedt, S.; Lindgren, S.; Almer, S.; Björnsson, E.; Bergquist, A.; Prytz, H.; Sandberg-Gertzén, H.; Hultcrantz, R.; Sangfelt, P.; et al. Characteristics and long-term outcome of patients with autoimmune hepatitis related to the initial treatment response. Scand. J. Gastroenterol. 2010, 45, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Hoeroldt, B.; McFarlane, E.; Dube, A.; Basumani, P.; Karajeh, M.; Campbell, M.J.; Gleeson, D. Long-term outcomes of patients with autoimmune hepatitis managed at a nontransplant center. Gastroenterology 2011, 140, 1980–1989. [Google Scholar] [CrossRef] [PubMed]
- Danielsson Borssén, Å.; Marschall, H.U.; Bergquist, A.; Rorsman, F.; Weiland, O.; Kechagias, S.; Nyhlin, N.; Verbaan, H.; Nilsson, E.; Werner, M. Epidemiology and causes of death in a Swedish cohort of patients with autoimmune hepatitis. Scand. J. Gastroenterol. 2017, 52, 1022–1028. [Google Scholar] [CrossRef]
- Powell, S.R. The antioxidant properties of zinc. J. Nutr. 2000, 130 (Suppl. S5), 1447S–1454S. [Google Scholar] [CrossRef] [Green Version]
- Stamoulis, I.; Kouraklis, G.; Theocharis, S. Zinc and the liver: An active interaction. Dig. Dis. Sci. 2007, 52, 1595–1612. [Google Scholar] [CrossRef] [PubMed]
- Rojkind, M.; Giambrone, M.-A.; Biempica, L. Collagen Types in Normal and Cirrhotic Liver. Gastroenterology 1979, 76, 710–719. [Google Scholar] [CrossRef]
- Anttinen, H.; Ryhänen, L.; Puistola, U.; Arranto, A.; Oikarinen, A. Decrease in Liver Collagen Accumulation in Carbon Tetrachloride-Injured and Normal Growing Rats Upon Administration of Zinc. Gastroenterology 1984, 86, 532–539. [Google Scholar] [CrossRef]
- Seltzer, J.L.; Jeffrey, J.J.; Eisen, A.Z. Evidence for Mammalian Collagenases As Zinc Ion Metalloenzymes. Biochim. Biophys. Acta Enzym. 1977, 485, 179–187. [Google Scholar] [CrossRef]
- Yuasa, J.; Mitsui, A.; Kawai, T. Emission from a tetrazine derivative complexed with zinc ion in aqueous solution: A unique water-soluble fluorophore. Chem. Commun. 2011, 47, 5807–5809. [Google Scholar] [CrossRef]
- Kojima-Yuasa, A.; Ohkita, T.; Yukami, K.; Ichikawa, H.; Takami, N.; Nakatani, T.; Kennedy, D.O.; Nishiguchi, S.; Matsui-Yuasa, I. Involvement of Intracellular Glutathione in Zinc Deficiency-Induced Activation of Hepatic Stellate Cells. Chem. Interactions 2003, 146, 89–99. [Google Scholar] [CrossRef]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural History and Prognostic Indicators of Survival in Cirrhosis: A Systematic Review of 118 Studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef]
- Kisseleva, T.; Uchinami, H.; Feirt, N.; Quintana-Bustamante, O.; Segovia, J.C.; Schwabe, R.F.; Brenner, D. Bone Marrow-Derived Fibrocytes Participate in Pathogenesis of Liver Fibrosis. J. Hepatol. 2006, 45, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Higashiyama, R.; Moro, T.; Nakao, S.; Mikami, K.; Fukumitsu, H.; Ueda, Y.; Ikeda, K.; Adachi, E.; Bou–Gharios, G.; Okazaki, I.; et al. Negligible Contribution of Bone Marrow-Derived Cells to Collagen Production During Hepatic Fibrogenesis in Mice. Gastroenterology 2009, 137, 1459–1466. [Google Scholar] [CrossRef]
- Mederacke, I.; Hsu, C.C.; Troeger, J.S.; Huebener, P.; Mu, X.; Dapito, D.H.; Pradere, J.-P.; Schwabe, R.F. Fate Tracing Reveals Hepatic Stellate Cells As Dominant Contributors to Liver Fibrosis Independent of Its Aetiology. Nat. Commun. 2013, 4, 2823. [Google Scholar] [CrossRef] [Green Version]
- Jia, H.; Aw, W.; Saito, K.; Hanate, M.; Hasebe, Y.; Kato, H. Eggshell Membrane Ameliorates Hepatic Fibrogenesis in Human C3A Cells and Rats through Changes in PPARγ-Endothelin 1 Signaling. Sci. Rep. 2014, 4, 7473. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-Y.; Cho, B.H.; Kim, U.-H. CD38-mediated Ca2+ signaling contributes to angiotensin II-induced activation of hepatic stellate cells: Attenuation of hepatic fibrosis by CD38 ablation. J. Biol. Chem. 2010, 285, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Lu, D.-H.; Guo, X.-Y.; Qin, S.-Y.; Luo, W.; Huang, X.-L.; Chen, M.; Wang, J.-X.; Ma, S.-J.; Yang, X.-W.; Jiang, H.-X. Interleukin-22 Ameliorates Liver Fibrogenesis by Attenuating Hepatic Stellate Cell Activation and Downregulating the Levels of Inflammatory Cytokines. World J. Gastroenterol. 2015, 21, 1531–1545. [Google Scholar] [CrossRef]
- Pines, M. Halofuginone for fibrosis, regeneration and cancer in the gastrointestinal tract. World J. Gastroenterol. 2014, 20, 14778–14786. [Google Scholar] [CrossRef] [PubMed]
- Adorini, L.; Pruzanski, M.; Shapiro, D. Farnesoid X Receptor Targeting to Treat Nonalcoholic Steatohepatitis. Drug Discov. Today 2012, 17, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Chávez, E.; Castro-Sánchez, L.; Shibayama, M.; Tsutsumi, V.; Moreno, M.G.; Muriel, P. Sulfasalazine prevents the increase in TGF-β, COX-2, nuclear NFkappaB translocation and fibrosis in CCl4-induced liver cirrhosis in the rat. Hum. Exp. Toxicol. 2012, 31, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Crespo, I.; San-Miguel, B.; Fernández, A.; de Urbina, J.O.; González-Gallego, J.; Tuñón, M.J. Melatonin Limits the Expression of Profibrogenic Genes and Ameliorates the Progression of Hepatic Fibrosis in Mice. Transl. Res. 2015, 165, 346–357. [Google Scholar] [CrossRef]
- Wei, Y.; Kang, X.-L.; Wang, X. The Peripheral Cannabinoid Receptor 1 Antagonist VD60 Efficiently Inhibits Carbon Tetrachloride-Intoxicated Hepatic Fibrosis Progression. Exp. Biol. Med. 2014, 239, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Muhanna, N.; Abu Tair, L.; Doron, S.; Amer, J.; Azzeh, M.; Mahamid, M.; Friedman, S.; Safadi, R. Amelioration of Hepatic Fibrosis by NK Cell Activation. Gut 2010, 60, 90–98. [Google Scholar] [CrossRef]
- Glässner, A.; Eisenhardt, M.; Kokordelis, P.; Kramer, B.; Wolter, F.; Nischalke, H.D.; Boesecke, C.; Sauerbruch, T.; Rockstroh, J.K.; Spengler, U.; et al. Impaired CD4+ T Cell Stimulation of NK Cell Anti-Fibrotic Activity May Contribute to Accelerated Liver Fibrosis Progression in HIV/HCV Patients. J. Hepatol. 2013, 59, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Ido, A.; Moriuchi, A.; Numata, M.; Murayama, T.; Teramukai, S.; Marusawa, H.; Yamaji, N.; Setoyama, H.; Kim, I.-D.; Chiba, T.; et al. Safety and Pharmacokinetics of Recombinant Human Hepatocyte Growth Factor (rh-HGF) in Patients With Fulminant Hepatitis: A Phase I/II Clinical Trial, Following Preclinical Studies to Ensure Safety. J. Transl. Med. 2011, 9, 55. [Google Scholar] [CrossRef] [Green Version]
- Bohanon, F.J.; Wang, X.; Graham, B.M.; Ding, C.; Ding, Y.; Radhakrishnan, G.L.; Rastellini, C.; Zhou, J.; Radhakrishnan, R.S. Enhanced Effects of Novel Oridonin Analog CYD0682 for Hepatic Fibrosis. J. Surg. Res. 2015, 199, 441–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, S.A.; O’Connor, K.S.; Suppiah, V.; Ahlenstiel, C.; Obeid, S.; Cook, K.; Cunningham, A.; Douglas, M.W.; Hogg, P.J.; Booth, D.; et al. Zinc Is a Potent and Specific Inhibitor of IFN-λ3 Signalling. Nat. Commun. 2017, 8, 15245. [Google Scholar] [CrossRef]
- Hara, T.; Takeda, T.-A.; Takagishi, T.; Fukue, K.; Kambe, T.; Fukada, T. Physiological Roles of Zinc Transporters: Molecular and Genetic Importance in Zinc Homeostasis. J. Physiol. Sci. 2017, 67, 283–301. [Google Scholar] [CrossRef]
- Andreini, C.; Banci, L.; Bertini, I.; Rosato, A. Counting the zinc-proteins encoded in the human genome. J. Proteome Res. 2006, 5, 196–201. [Google Scholar] [CrossRef]
- Fukada, T.; Yamasaki, S.; Nishida, K.; Murakami, M.; Hirano, T. Zinc homeostasis and signaling in health and diseases: Zinc signaling. J. Biol. Inorg. Chem. 2011, 16, 1123–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosui, A.; Kimura, E.; Abe, S.; Tanimoto, T.; Onishi, K.; Kusumoto, Y.; Sueyoshi, Y.; Matsumoto, K.; Hirao, M.; Yamada, T.; et al. Long-Term Zinc Supplementation Improves Liver Function and Decreases the Risk of Developing Hepatocellular Carcinoma. Nutrients 2018, 10, 1955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumura, H.; Nirei, K.; Nakamura, H.; Arakawa, Y.; Higuchi, T.; Hayashi, J.; Yamagami, H.; Matsuoka, S.; Ogawa, M.; Nakajima, N.; et al. Zinc Supplementation Therapy Improves the Outcome of Patients With Chronic Hepatitis C. J. Clin. Biochem. Nutr. 2012, 51, 178–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuoka, S.; Matsumura, H.; Nakamura, H.; Oshiro, S.; Arakawa, Y.; Hayashi, J.; Sekine, N.; Nirei, K.; Yamagami, H.; Ogawa, M.; et al. Zinc Supplementation Improves the Outcome of Chronic Hepatitis C and Liver Cirrhosis. J. Clin. Biochem. Nutr. 2009, 45, 292–303. [Google Scholar] [CrossRef] [Green Version]
- Murakami, Y.; Koyabu, T.; Kawashima, A.; Kakibuchi, N.; Kawakami, T.; Takaguchi, K.; Kita, K.; Okita, M. Zinc Supplementation Prevents the Increase of Transaminase in Chronic Hepatitis C Patients During Combination Therapy With Pegylated Interferon Alpha-2b and Ribavirin. J. Nutr. Sci. Vitaminol. 2007, 53, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Himoto, T.; Hosomi, N.; Nakai, S.; Deguchi, A.; Kinekawa, F.; Matsuki, M.; Yachida, M.; Masaki, T.; Kurokochi, K.; Watanabe, S.; et al. Efficacy of Zinc Administration in Patients With Hepatitis C Virus-Related Chronic Liver Disease. Scand. J. Gastroenterol. 2007, 42, 1078–1087. [Google Scholar] [CrossRef]
- Shigefuku, R.; Iwasa, M.; Katayama, K.; Eguchi, A.; Kawaguchi, T.; Shiraishi, K.; Ito, T.; Suzuki, K.; Koreeda, C.; Ohtake, T.; et al. Hypozincemia Is Associated With Human Hepatocarcinogenesis in Hepatitis C virus-related Liver Cirrhosis. Hepatol. Res. 2019, 49, 1127–1135. [Google Scholar] [CrossRef]
- Iredale, J.P.; Thompson, A.; Henderson, N.C. Extracellular Matrix Degradation in Liver Fibrosis: Biochemistry and Regulation. Biochim. Biophys. Acta Mol. Basis Dis. 2013, 1832, 876–883. [Google Scholar] [CrossRef] [Green Version]
- Visse, R.; Nagase, H. Matrix metalloproteinases and tissue inhibitors of metalloproteinases: Structure, function, and biochemistry. Circ. Res. 2003, 92, 827–839. [Google Scholar] [CrossRef] [Green Version]
- Duarte, S.; Baber, J.; Fujii, T.; Coito, A.J. Matrix metalloproteinases in liver injury, repair and fibrosis. Matrix Biol. 2015, 44–46, 147–156. [Google Scholar] [CrossRef]
- Vandooren, J.; van den Steen, P.E.; Opdenakker, G. Biochemistry and molecular biology of gelatinase B or matrix metalloproteinase-9 (MMP-9): The next decade. Crit. Rev. Biochem. Mol. Biol. 2013, 48, 222–272. [Google Scholar] [CrossRef] [PubMed]
- Arpino, V.; Brock, M.; Gill, S.E. The Role of TIMPs in Regulation of Extracellular Matrix Proteolysis. Matrix Biol. 2015, 44–46, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Zhang, Z.; Zhu, L.; Lu, M.; Li, Y.; Zhou, J.; Lu, X.; Du, Q. Polaprezinc Inhibits Liver Fibrosis and Proliferation in Hepatocellular Carcinoma. Mol. Med. Rep. 2017, 16, 5523–5528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kono, T.; Asama, T.; Chisato, N.; Ebisawa, Y.; Okayama, T.; Imai, K.; Karasaki, H.; Furukawa, H.; Yoneda, M. Polaprezinc Prevents Ongoing Thioacetamide-Induced Liver Fibrosis in Rats. Life Sci. 2012, 90, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Sugino, H.; Kumagai, N.; Watanabe, S.; Toda, K.; Takeuchi, O.; Tsunematsu, S.; Morinaga, S.; Tsuchimoto, K. Polaprezinc Attenuates Liver Fibrosis in a Mouse Model of Non-Alcoholic Steatohepatitis. J. Gastroenterol. Hepatol. 2008, 23, 1909–1916. [Google Scholar] [CrossRef]
- Takahashi, M.; Saito, H.; Higashimoto, M.; Hibi, T. Possible Inhibitory Effect of Oral Zinc Supplementation on Hepatic Fibrosis through Downregulation of TIMP-1: A Pilot Study. Hepatol. Res. 2007, 37, 405–409. [Google Scholar] [CrossRef]
- Latronico, T.; Mascia, C.; Pati, I.; Zuccala, P.; Mengoni, F.; Marocco, R.; Tieghi, T.; Belvisi, V.; Lichtner, M.; Vullo, V.; et al. Liver Fibrosis in HCV Monoinfected and HIV/HCV Coinfected Patients: Dysregulation of Matrix Metalloproteinases (MMPs) and Their Tissue Inhibitors TIMPs and Effect of HCV Protease Inhibitors. Int. J. Mol. Sci. 2016, 17, 455. [Google Scholar] [CrossRef] [Green Version]
- Kasahara, A.; Hayashi, N.; Mochizuki, K.; Oshita, M.; Katayama, K.; Kato, M.; Masuzawa, M.; Yoshihara, H.; Naito, M.; Miyamoto, T.; et al. Circulating Matrix Metalloproteinase-2 and Tissue Inhibitor of Metalloproteinase-1 As Serum Markers of Fibrosis in Patients With Chronic Hepatitis C: Relationship to Interferon Reponse. J. Hepatol. 1997, 26, 574–583. [Google Scholar] [CrossRef]
- Giannelli, G.; Bergamini, C.; Marinosci, F.; Fransvea, E.; Quaranta, M.; Lupo, L.; Schiraldi, O.; Antonaci, S. Clinical Role of MMP-2/TIMP-2 Imbalance in Hepatocellular Carcinoma. Int. J. Cancer 2002, 97, 425–431. [Google Scholar] [CrossRef]
- Watanabe, N.; Nishizaki, Y.; Kojima, S.-I.; Takashimizu, S.; Nagata, N.; Kagawa, T.; Shiraishi, K.; Mine, T.; Matsuzaki, S. Clinical Significance of Serum Matrix Metalloproteinases and Tissue Inhibitors of Metalloproteinases in Chronic Liver Disease. Tokai J. Exp. Clin. Med. 2006, 31, 96–101. [Google Scholar]
- Kadoya, H.; Uchida, A.; Kashihara, N. A case of copper deficiency-induced pancytopenia with maintenance hemodialysis outpatient treated with polaprezinc. Ther Apher. Dial. 2016, 20, 422–423. [Google Scholar] [CrossRef]
- Ozeki, I.; Nakajima, T.; Suii, H.; Tatsumi, R.; Yamaguchi, M.; Arakawa, T.; Kuwata, Y.; Toyota, J.; Karino, Y. Evaluation of Treatment With Zinc Acetate Hydrate in Patients With Liver Cirrhosis Complicated by Zinc Deficiency. Hepatol. Res. 2019, 50, 488–501. [Google Scholar] [CrossRef]
- Katayama, K.; Hosui, A.; Sakai, Y.; Itou, M.; Matsuzaki, Y.; Takamori, Y.; Hosho, K.; Tsuru, T.; Takikawa, Y.; Michitaka, K.; et al. Effects of Zinc Acetate on Serum Zinc Concentrations in Chronic Liver Diseases: A Multicenter, Double-Blind, Randomized, Placebo-Controlled Trial and a Dose Adjustment Trial. Biol. Trace Element Res. 2019, 195, 71–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamoto, T.; Hatakeyama, S.; Konishi, S.; Okita, K.; Tanaka, Y.; Imanishi, K.; Takashima, T.; Saitoh, F.; Suzuki, T.; Ohyama, C. Comparison of Zinc Acetate Hydrate and Polaprezinc for Zinc Deficiency in Patients on Maintenance Hemodialysis: A single-center, open-label, Prospective Randomized Study. Ther. Apher. Dial. 2020, 24, 568–577. [Google Scholar] [CrossRef]
- Kodama, H.; Tanaka, M.; Naito, Y.; Katayama, K.; Moriyama, M. Japan’s Practical Guidelines for Zinc Deficiency With a Particular Focus on Taste Disorders, Inflammatory Bowel Disease, and Liver Cirrhosis. Int. J. Mol. Sci. 2020, 21, 2941. [Google Scholar] [CrossRef] [PubMed]
- Crofton, R.W.; Gvozdanovic, D.; Gvozdanovic, S.; Khin, C.C.; Brunt, P.W.; Mowat, N.A.; Aggett, P.J. Inorganic Zinc and the Intestinal Absorption of Ferrous Iron. Am. J. Clin. Nutr. 1989, 50, 141–144. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Zinc Elevation | Patients without Zinc Elevation | p | |||||
|---|---|---|---|---|---|---|---|
| (n = 27) | (n = 11) | ||||||
| Age (years) | 65.0 | ± | 11.0 | 69.2 | ± | 13.9 | 0.38 |
| Sex | 1.00 | ||||||
| Male | 7.4 | % | (2) | 9.1 | % | (1) | |
| Female | 92.6 | % | (25) | 90.9 | % | (10) | |
| Body Weights (kg) | 54.0 | ± | 9.8 | 53.0 | ± | 10.1 | 0.79 |
| Body Mass Index (kg/m2) | 23.0 | ± | 3.8 | 23.5 | ± | 4.2 | 0.74 |
| Fibrosis | 0.81 | ||||||
| F0 | 3.7 | % | (1) | 0.0 | % | (0) | |
| F1 | 44.4 | % | (12) | 54.5 | % | (6) | |
| F2 | 29.6 | % | (8) | 27.3 | % | (3) | |
| F3 | 14.8 | % | (4) | 9.1 | % | (1) | |
| F4 (Liver Cirrhosis) | 7.4 | % | (2) | 9.1 | % | (1) | |
| AIH type 1 | 100 | % | (27) | 100.0 | % | (11) | 1.00 |
| AIH type 2 | 0 | % | (0) | 0.0 | % | (0) | 1.00 |
| Morbidity periods (years) | 4 | ± | 3.4 | 5.3 | ± | 3.1 | 0.30 |
| Blood test | |||||||
| Zinc (µg/dL) | 70.8 | ± | 10.9 | 74.4 | ± | 13.0 | 0.44 |
| AST (U/L) | 24.6 | ± | 9.2 | 29.4 | ± | 13.6 | 0.31 |
| ALT (U/L) | 18.1 | ± | 10.1 | 20.3 | ± | 9.5 | 0.54 |
| ALP (U/L) | 233 | ± | 100 | 308 | ± | 152 | 0.15 |
| gamma GT (U/L) | 38.9 | ± | 61.2 | 69.5 | ± | 109 | 0.40 |
| Total bilirubin (mg/dL) | 0.79 | ± | 0.45 | 0.85 | ± | 0.29 | 0.65 |
| Albumin (g/dL) | 4.16 | ± | 0.26 | 4.11 | ± | 0.27 | 0.59 |
| HDL-cholesterol (mg/dL) | 67.6 | ± | 22.1 | 71.3 | ± | 19.5 | 0.61 |
| Ferritin (ng/mL) | 84.4 | ± | 95.6 | 97.7 | ± | 77.1 | 0.66 |
| Copper (µg/dL) | 121.8 | ± | 27.7 | 130.3 | ± | 23.1 | 0.38 |
| IgG (mg/dL) | 1389 | ± | 327 | 1495 | ± | 488 | 0.52 |
| Hyaluronic acid (ng/mL) | 92.2 | ± | 78.2 | 168 | ± | 187 | 0.25 |
| Pro-collagen type III (ng/mL) | 0.65 | ± | 0.30 | 0.55 | ± | 0.17 | 0.25 |
| Type IV collagen 7S (ng/mL) | 5.45 | ± | 3.13 | 4.09 | ± | 1.24 | 0.08 |
| Platelets (/µL) | 19.6 | ± | 5.7 | 18.9 | ± | 5.4 | 0.72 |
| Prothrombin time (%) | 95.4 | ± | 19.7 | 96.6 | ± | 16.6 | 0.84 |
| Treatments | |||||||
| PSL populations (%) | 51.9 | % | (14) | 36.4 | % | (4) | 0.48 |
| PSL dose (mg) | 5.8 | ± | 1.8 | 6.3 | ± | 1.9 | 0.48 |
| UDCA populations (%) | 88.9 | % | (24) | 90.9 | % | (10) | 1.00 |
| UDCA dose (mg) | 600 | ± | 177 | 630 | ± | 95 | 0.53 |
| Azathioprine populations (%) | 11.0 | % | (3) | 9.1 | % | (1) | 0.85 |
| Azathioprine dose (mg) | 100 | ± | 0 | 100 | ± | 0 | 1.00 |
| Patients with Zinc Elevation (n = 27) | Before | After 12 Months | After 24 Months | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | Mean | SD | p | ||||
| Zinc (µg/dL) | 70.8 | ± | 10.9 | 109.9 | ± | 35.5 | <0.001 | 105.1 | ± | 38.0 | <0.001 |
| AST (U/L) | 24.6 | ± | 9.2 | 24.4 | ± | 11.1 | 0.93 | 27.2 | ± | 17.8 | 0.51 |
| ALT (U/L) | 18.1 | ± | 10.1 | 17.0 | ± | 9.3 | 0.67 | 19.0 | ± | 13.4 | 0.79 |
| ALP (U/L) | 232.8 | ± | 100.0 | 275.2 | ± | 279.8 | 0.46 | 242.8 | ± | 86.4 | 0.70 |
| Gamma GT (U/L) | 38.9 | ± | 61.2 | 52.4 | ± | 140.5 | 0.65 | 32.3 | ± | 42.0 | 0.65 |
| Total bilirubin (mg/dL) | 0.79 | ± | 0.45 | 0.78 | ± | 0.42 | 0.93 | 0.81 | ± | 0.47 | 0.88 |
| Albumin (g/dL) | 4.16 | ± | 0.26 | 4.22 | ± | 0.23 | 0.41 | 4.21 | ± | 0.18 | 0.48 |
| HDL-cholesterol (mg/dL) | 67.6 | ± | 22.1 | 64.8 | ± | 19.0 | 0.63 | 67.9 | ± | 19.9 | 0.95 |
| Ferritin (ng/mL) | 84.4 | ± | 95.6 | 56.8 | ± | 50.8 | 0.19 | 54.3 | ± | 42.0 | 0.20 |
| Copper (µg/dL) | 121.8 | ± | 27.7 | 107.8 | ± | 17.7 | 0.34 | 113.8 | ± | 20.6 | 0.25 |
| IgG (mg/dL) | 1388.7 | ± | 327.3 | 1359.3 | ± | 279.5 | 0.72 | 1351.8 | ± | 351.7 | 0.71 |
| Hyaluronic acid (ng/mL) | 92.2 | ± | 78.2 | 65.3 | ± | 53.8 | 0.16 | 91.1 | ± | 73.3 | 0.97 |
| Pro-collagen type III (ng/mL) | 0.65 | ± | 0.30 | 0.52 | ± | 0.16 | 0.06 | 0.49 | ± | 0.15 | 0.06 |
| Type IV collagen 7S (ng/mL) | 5.45 | ± | 3.13 | 4.12 | ± | 1.68 | 0.07 | 4.30 | ± | 1.23 | 0.15 |
| Platelets (/µL) | 19.6 | ± | 5.7 | 20.4 | ± | 5.7 | 0.61 | 20.8 | ± | 5.8 | 0.45 |
| Prothrombin time (%) | 95.4 | ± | 19.7 | 98.7 | ± | 13.4 | 0.47 | 95.1 | ± | 13.9 | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moriya, K.; Nishimura, N.; Namisaki, T.; Takaya, H.; Sawada, Y.; Kawaratani, H.; Kaji, K.; Shimozato, N.; Sato, S.; Furukawa, M.; et al. Zinc Administration and Improved Serum Markers of Hepatic Fibrosis in Patients with Autoimmune Hepatitis. J. Clin. Med. 2021, 10, 2465. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112465
Moriya K, Nishimura N, Namisaki T, Takaya H, Sawada Y, Kawaratani H, Kaji K, Shimozato N, Sato S, Furukawa M, et al. Zinc Administration and Improved Serum Markers of Hepatic Fibrosis in Patients with Autoimmune Hepatitis. Journal of Clinical Medicine. 2021; 10(11):2465. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112465
Chicago/Turabian StyleMoriya, Kei, Norihisa Nishimura, Tadashi Namisaki, Hiroaki Takaya, Yasuhiko Sawada, Hideto Kawaratani, Kosuke Kaji, Naotaka Shimozato, Shinya Sato, Masanori Furukawa, and et al. 2021. "Zinc Administration and Improved Serum Markers of Hepatic Fibrosis in Patients with Autoimmune Hepatitis" Journal of Clinical Medicine 10, no. 11: 2465. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112465