
Association between Visceral Adipose Tissue and Non-Alcoholic Steatohepatitis Histology in Patients with Known or Suspected Non-Alcoholic Fatty Liver Disease

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
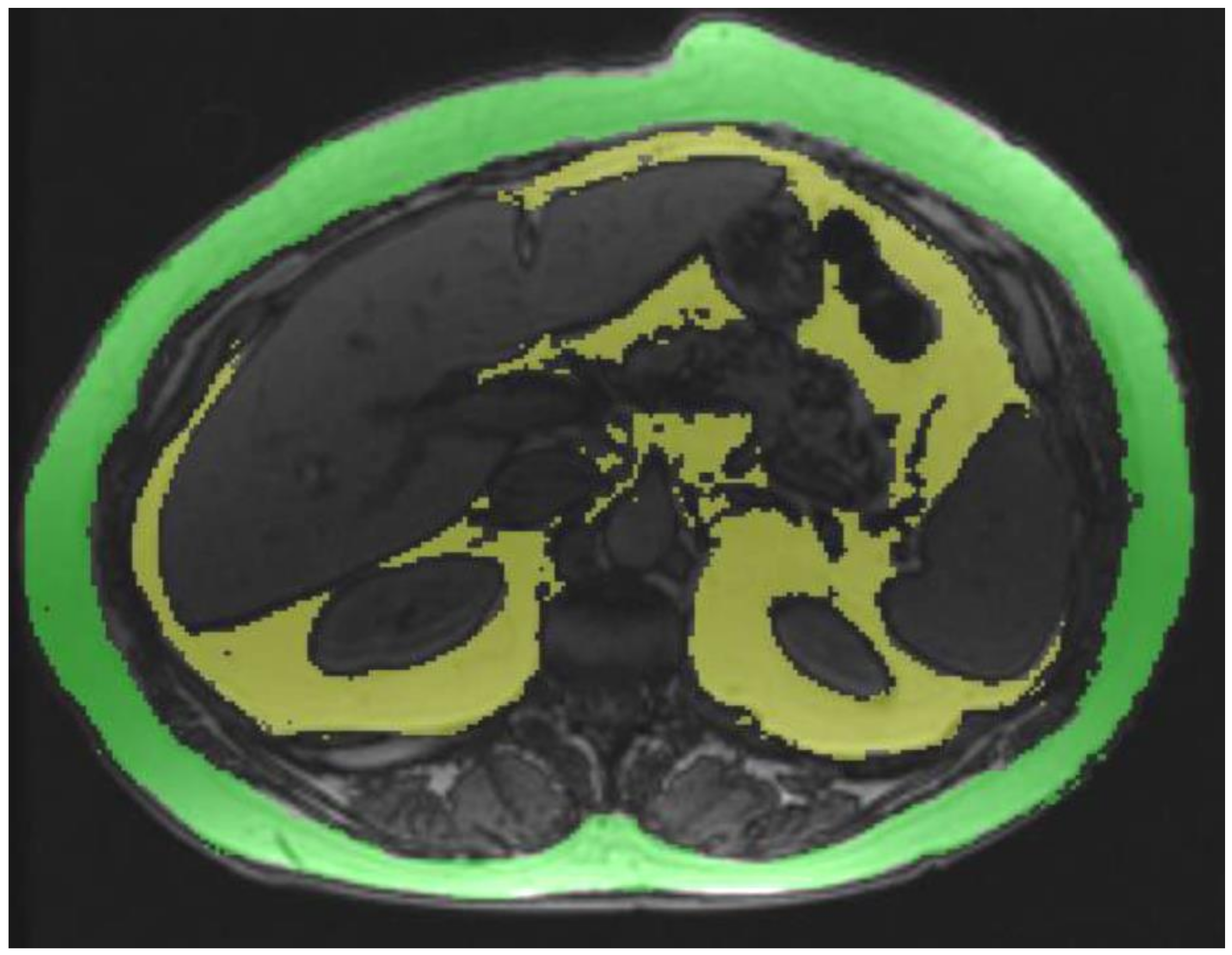
2.1. VAT and Subcutaneous Adipose Tissue (SAT) Estimation
2.2. Liver and Pancreas PDFF and Liver and Spleen Volumes
2.3. Histological Analysis
2.4. Statistical Analysis
3. Results
3.1. Associations among MRI Parameters
3.2. Histological Analyses
3.3. Associations between MRI Parameters and HS, NASH and HF
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Grundy, S.M.; Brewer, H.B., Jr.; Cleeman, J.I.; Smith, S.C., Jr.; Lenfant, C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kershaw, E.E.; Flier, J.S. Adipose tissue as an endocrine organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Matteoni, C.A.; Younossi, Z.M.; Gramlich, T.; Boparai, N.; Liu, Y.C.; McCullough, A.J. Nonalcoholic fatty liver disease: A spectrum of clinical and pathological severity. Gastroenterology 1999, 116, 1413–1419. [Google Scholar] [CrossRef]
- Nalbantoglu, I.L.; Brunt, E.M. Role of liver biopsy in nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 9026–9037. [Google Scholar] [PubMed]
- Feng, R.N.; Du, S.S.; Wang, C.; Li, Y.C.; Liu, L.Y.; Guo, F.C.; Sun, C.H. Lean-non-alcoholic fatty liver disease increases risk for metabolic disorders in a normal weight Chinese population. World J. Gastroenterol. 2014, 20, 7932–17940. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Desai, A.; Hamilton, G.; Wolfson, T.; Gamst, A.; Lam, J.; Clark, L.; Hooker, J.; Chavez, T.; Ang, B.D.; et al. Accuracy of MR imaging-estimated proton density fat fraction for classification of dichotomized histologic steatosis grades in nonalcoholic fatty liver disease. Radiology 2015, 274, 416–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhary, N.S.; Duseja, A.; Kalra, N.; Das, A.; Dhiman, R.K.; Chawla, Y.K. Correlation of adipose tissue with liver histology in Asian Indian patients with nonalcoholic fatty liver disease (NAFLD). Ann. Hepatol. 2012, 11, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.J.; Kim, W.; Kim, D.; Yoon, J.H.; Lee, K.; Kim, J.H.; Cho, E.J.; Lee, J.H.; Kim, H.Y.; Kim, Y.J.; et al. Visceral Obesity Predicts Significant Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Medicine 2015, 94, e2159. [Google Scholar] [CrossRef]
- Kim, D.; Chung, G.E.; Kwak, M.S.; Seo, H.B.; Kang, J.H.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Lee, H.S.; Kim, C.Y. Body Fat Distribution and Risk of Incident and Regressed Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2016, 14, 132–138.e4. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of a WHO Consultation: Definition of Metabolic Syndrome in Definition, Diagnosis and Classification of Diabetes Mellitus; World Health Organization, Department of Noncommunicable Disease Surveillance: Geneva, Switzerland, 1999. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Philbrick, K.A.; Weston, A.D.; Akkus, Z.; Kline, T.L.; Korfiatis, P.; Sakinis, T.; Kostandy, P.; Boonrod, A.; Zeinoddini, A.; Takahashi, N.; et al. RIL-Contour: A Medical Imaging Dataset Annotation Tool for and with Deep Learning. J. Digit. Imaging 2019, 32, 571–581. [Google Scholar] [CrossRef] [Green Version]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology; Pearson Education: Harlow, UK, 2007. [Google Scholar]
- Wildman-Tobriner, B.; Middleton, M.M.; Moylan, C.A.; Rossi, S.; Flores, O.; Chang, Z.A.; Abdelmalek, M.F.; Sirlin, C.B.; Bashir, M.R. Association Between Magnetic Resonance Imaging-Proton Density Fat Fraction and Liver Histology Features in Patients With Nonalcoholic Fatty Liver Disease or Nonalcoholic Steatohepatitis. Gastroenterology 2018, 155, 1428–1435.e2. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.S.; Peterson, M.R.; Lin, G.Y.; Feldstein, A.; Schnabl, B.; Bettencourt, R.; Seki, E.; Sirlin, C.B.; Loomba, R. Insulin Resistance Increases MRI-Estimated Pancreatic Fat in Nonalcoholic Fatty Liver Disease and Normal Controls. Gastroenterol. Res. Pract. 2013, 2013, 498296. [Google Scholar] [CrossRef] [Green Version]
- Tushuizen, M.E.; Bunck, M.C.; Pouwels, P.J.; Bontemps, S.; Van Waesberghe, J.H.T.; Schindhelm, R.K.; Mari, A.; Heine, R.J.; Diamant, M. Pancreatic fat content and beta-cell function in men with and without type 2 diabetes. Diabetes Care 2007, 30, 2916–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Idilman, I.S.; Tuzun, A.; Savas, B.; Elhan, A.H.; Celik, A.; Idilman, R.; Karcaaltincaba, M. Quantification of liver, pancreas, kidney, and vertebral body MRI-PDFF in non-alcoholic fatty liver disease. Abdom. Imaging 2015, 40, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Sarma, M.K.; Saucedo, A.; Darwin, C.H.; Felker, E.R.; Umachandran, K.; Kohanghadosh, D.; Xu, E.; Raman, S.; Thomas, M.A. Noninvasive assessment of abdominal adipose tissues and quantification of hepatic and pancreatic fat fractions in type 2 diabetes mellitus. Magn. Reson. Imaging 2020, 72, 95–102. [Google Scholar] [CrossRef]
- Kühn, J.P.; Berthold, F.; Mayerle, J.; Völzke, H.; Reeder, S.B.; Rathmann, W.; Lerch, M.M.; Hosten, N.; Hegenscheid, K.; Meffert, P.J. Pancreatic Steatosis Demonstrated at MR Imaging in the General Population: Clinical Relevance. Radiology 2015, 276, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, N.S.; Peterson, M.R.; Brenner, D.A.; Heba, E.; Sirlin, C.; Loomba, R. Association between novel MRI-estimated pancreatic fat and liver histology-determined steatosis and fibrosis in non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2013, 37, 630–639. [Google Scholar] [CrossRef]
- Jakobsen, M.U.; Berentzen, T.; Sørensen, T.I.; Overvad, K. Abdominal obesity and fatty liver. Epidemiol. Rev. 2007, 29, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, A.H.; Duan-Mu, Y.Y.; Zhang, Y.; Wang, L.; Guo, Z.; Yu, Y.Q.; Wang, Y.S.; Cheng, X.G. Correlation between Non-Alcoholic Fatty Liver Disease and Visceral Adipose Tissue in Non-Obese Chinese Adults: A CT Evaluation. Korean J. Radiol. 2018, 19, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Chiyanika, C.; Chan, D.F.Y.; Hui, S.C.N.; So, H.K.; Deng, M.; Yeung, D.K.W.; Nelson, E.A.S.; Chu, W.C.W. The relationship between pancreas steatosis and the risk of metabolic syndrome and insulin resistance in Chinese adolescents with concurrent obesity and non-alcoholic fatty liver disease. Pediatr. Obes. 2020, 15, e12653. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| BMI | Lvol | Svol | Liver PDFF | Pancreas PDFF | |
|---|---|---|---|---|---|
| VAT | r = 0.11 (p > 0.05) | r = 0.38 (p < 0.001) | r = 0.19 (p = 0.025) | r = 0.41 (p < 0.001) | rs = 0.29 (p = 0.001) |
| SAT | r = 0.78 (p < 0.001) | r = 0.46 (p < 0.001) | r = 0.31 (p = 0.004) | r = 0.17 (p > 0.05) | rs = 0.18, (p > 0.05) |
| BMI | r = 0.42 (p < 0.001) | r = 0.27 (p = 0.002) | r = 0.13 (p > 0.05) | rs = 0.24 (p = 0.005) |
| Study Population | Hepatic Steatosis | p-Value | NASH | p-Value | Hepatic Fibrosis | p-Value | Lobular Inflammation | p-Value | Ballooning | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Absent | Present | Absent | Present | Absent | Present | Absent | Present | Absent | Present | |||||||
| Age (years) | 49.2 ± 11.2 | 47.1 ± 10.5 | 49.8 ± 11.4 | 0.249 * | 47.3 ± 10.9 | 50.8 ± 11.3 | 0.074 * | 48.1 ± 11.5 | 50.1 ± 11 | 0.300 * | 48.5 ± 10 | 49.5 ± 11.8 | 0.622 * | 47.5 ± 10.5 | 50.8 ± 11.7 | 0.086 * |
| BMI (kg/m2) | 42.5 ± 10.1 | 45.7 ± 10.5 | 41.5 ± 9.8 | 0.042 * | 44.1 ± 9.5 | 41.2 ± 10.5 | 0.092 * | 45.7 ± 8.9 | 39.9 ± 10.3 | 0.001 * | 44.74 ± 10.17 | 41.4 ± 10 | 0.068 * | 43.9 ± 10 | 41.2 ± 10.1 | 0.126 * |
| Lvol (mL) | 2492.2 ± 701.5 | 2098.8 ± 505.9 | 2609.8 ± 710.7 | <0.001 * | 2312.4 ± 577.2 | 2645.4 ± 762.9 | 0.005 * | 2285.8 ± 568.3 | 2662.9 ± 756.7 | 0.001 * | 2329.25 ± 590.49 | 2574.1 ± 740.4 | 0.056 * | 2304.3 ± 573.4 | 2672.4 ± 766.9 | 0.002 * |
| Svol (mL) | 381.6 ± 184.4 | 329.8 ± 159.6 | 397.1 ± 189.2 | 0.074 * | 357.3 ± 173 | 402.3 ± 192.4 | 0.159 * | 333.9 ± 137.4 | 421 ± 208.5 | 0.004 * | 355.8 ± 180.5 | 394.6 ± 186 | 0.250 * | 344.7 ± 164.2 | 417 ± 196.7 | 0.022 * |
| VAT (mL) | 120.6 ± 48.6 | 94.3 ± 40.8 | 128.5 ± 48.1 | <0.001 * | 109.2 ± 47.6 | 130.4 ± 47.5 | 0.011 * | 106.6 ± 46.3 | 132.3 ± 47.6 | 0.002 * | 106.8 ± 49.1 | 127.6 ± 47 | 0.019 * | 106.8 ± 44.8 | 134 ± 48.6 | 0.001 * |
| SAT (mL) | 251.6 ± 73.7 | 259.1 ± 70 | 248.5 ± 75.5 | 0.550 * | 248 ± 67.3 | 256.6 ± 82.5 | 0.599 * | 250 ± 68 | 254.4 ± 83.5 | 0.788 * | 249.9 ± 70.2 | 252.9 ± 77 | 0.849 * | 248.2 ± 70.7 | 256.6 ± 78.7 | 0.608 * |
| Liver PDFF (%) | 13.2 ± 8 | 5.5 ± 2 | 16.3 ± 7.4 | <0.001 * | 9.72 ± 6.5 | 18 ± 7.4 | <0.001 * | 10.25 ± 6.7 | 18.11 ± 7.7 | <0.001 * | 9.3 ± 5.6 | 16.1 ± 8.4 | <0.001 * | 91 ± 6.7 | 17.8 ± 7.6 | <0.001 * |
| Pancreas PDFF (%) | 12.7 ± 9.9 | 10.6 ± 10 | 13.3 ± 9.9 | 0.066 ** | 11.4 ± 8.9 | 13.9 ± 10.6 | 0.195 ** | 14 ± 11.4 | 11.6 ± 8.4 | 0.322 ** | 11.8 ± 9.6 | 13.2 ± 10.1 | 0.403 ** | 12.3 ± 10.3 | 13.1 ± 9.7 | 0.350 ** |
| Cut-Off Value | AUC | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|
| Hepatic Steatosis | 101.8 mL | 0.71 (0.60, 0.82) | 0.70 (0.60, 0.78) | 0.68 (0.49, 0.83) | 0.88 (0.78, 0.94) | 0.40 (0.27, 0.55) |
| NASH | 111.8 mL | 0.64 (0.54, 0.73) | 0.61 (0.49, 0.72) | 0.65 (0.51, 0.76) | 0.67 (0.54, 0.78) | 0.59 (0.46, 0.70) |
| Hepatic fibrosis | 111.6 mL | 0.66 (0.57, 0.76) | 0.62 (0.50, 0.73) | 0.64 (0.51, 0.76) | 0.67 (0.55, 0.78) | 0.58 (0.46, 0.70) |
| Parameter | Steatosis Grade | NAS Score | Fibrosis Stage | |||
|---|---|---|---|---|---|---|
| rs | p | rs | p | rs | p | |
| BMI | −0.17 | 0.053 | −0.25 | 0.003 | −0.42 | <0.001 |
| Lvol | 0.31 | <0.001 | 0.27 | 0.001 | 0.22 | 0.011 |
| Svol | 0.14 | 0.100 | 0.13 | 0.127 | 0.25 | 0.003 |
| VAT | 0.31 | <0.001 | 0.28 | 0.001 | 0.26 | 0.003 |
| SAT | 0.04 | 0.704 | 0.00 | 0.977 | 0.01 | 0.951 |
| Liver PDFF (%) | 0.82 | <0.001 | 0.71 | <0.001 | 0.46 | <0.001 |
| Pancreas PDFF (%) | 0.23 | 0.007 | 0.17 | 0.058 | −0.06 | 0.526 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idilman, I.S.; Low, H.M.; Gidener, T.; Philbrick, K.; Mounajjed, T.; Li, J.; Allen, A.M.; Yin, M.; Venkatesh, S.K. Association between Visceral Adipose Tissue and Non-Alcoholic Steatohepatitis Histology in Patients with Known or Suspected Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2021, 10, 2565. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122565
Idilman IS, Low HM, Gidener T, Philbrick K, Mounajjed T, Li J, Allen AM, Yin M, Venkatesh SK. Association between Visceral Adipose Tissue and Non-Alcoholic Steatohepatitis Histology in Patients with Known or Suspected Non-Alcoholic Fatty Liver Disease. Journal of Clinical Medicine. 2021; 10(12):2565. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122565
Chicago/Turabian StyleIdilman, Ilkay S., Hsien Min Low, Tolga Gidener, Kenneth Philbrick, Taofic Mounajjed, Jiahui Li, Alina M. Allen, Meng Yin, and Sudhakar K. Venkatesh. 2021. "Association between Visceral Adipose Tissue and Non-Alcoholic Steatohepatitis Histology in Patients with Known or Suspected Non-Alcoholic Fatty Liver Disease" Journal of Clinical Medicine 10, no. 12: 2565. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122565