
Predictive Value of Comorbid Conditions for COVID-19 Mortality


 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Building the Prediction Model
2.2. Outcome
2.3. Predictors
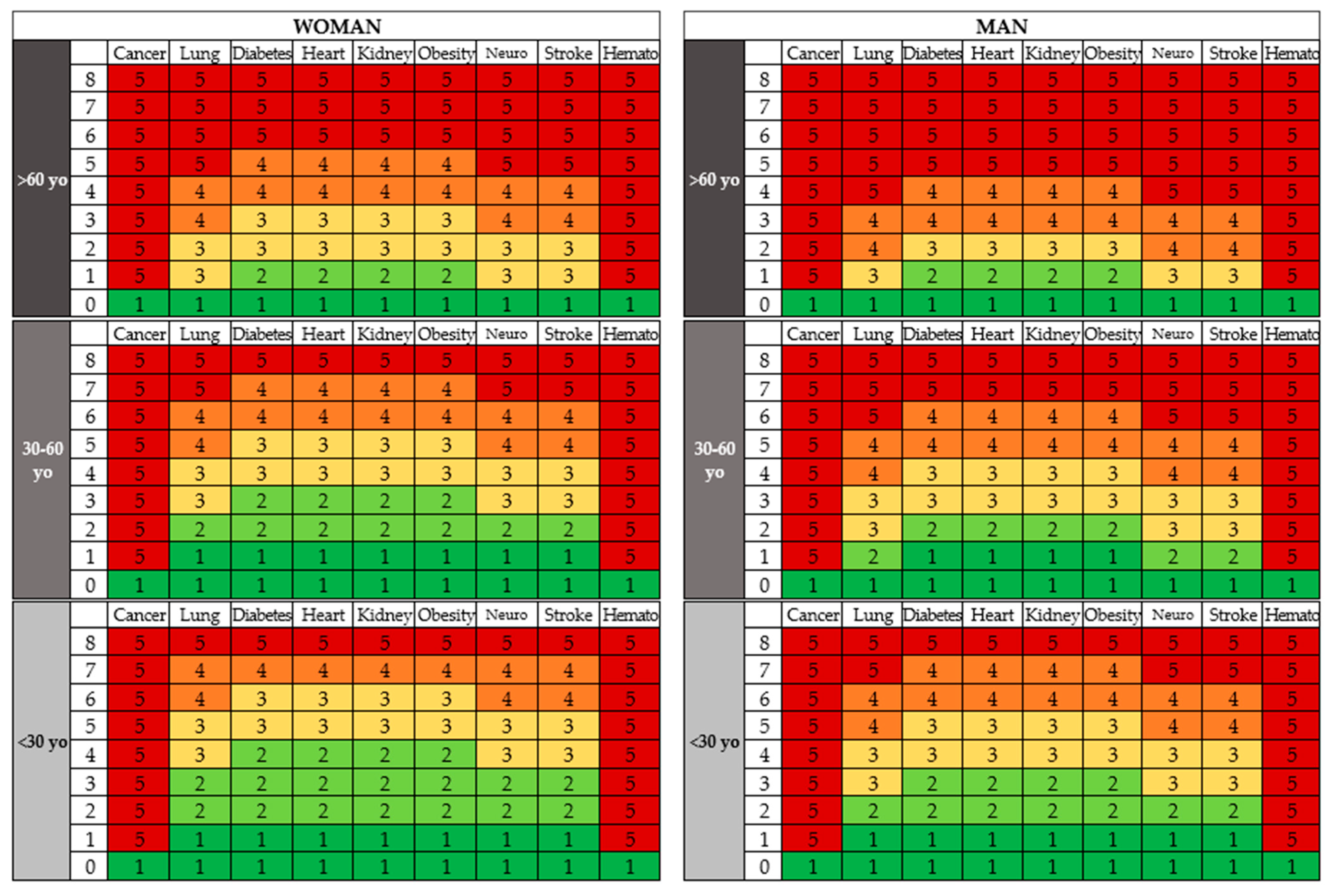
2.4. Risk Groups
2.5. Statistical Analysis Methods
3. Results
3.1. Participants
3.2. Model Development
3.3. Model Specification
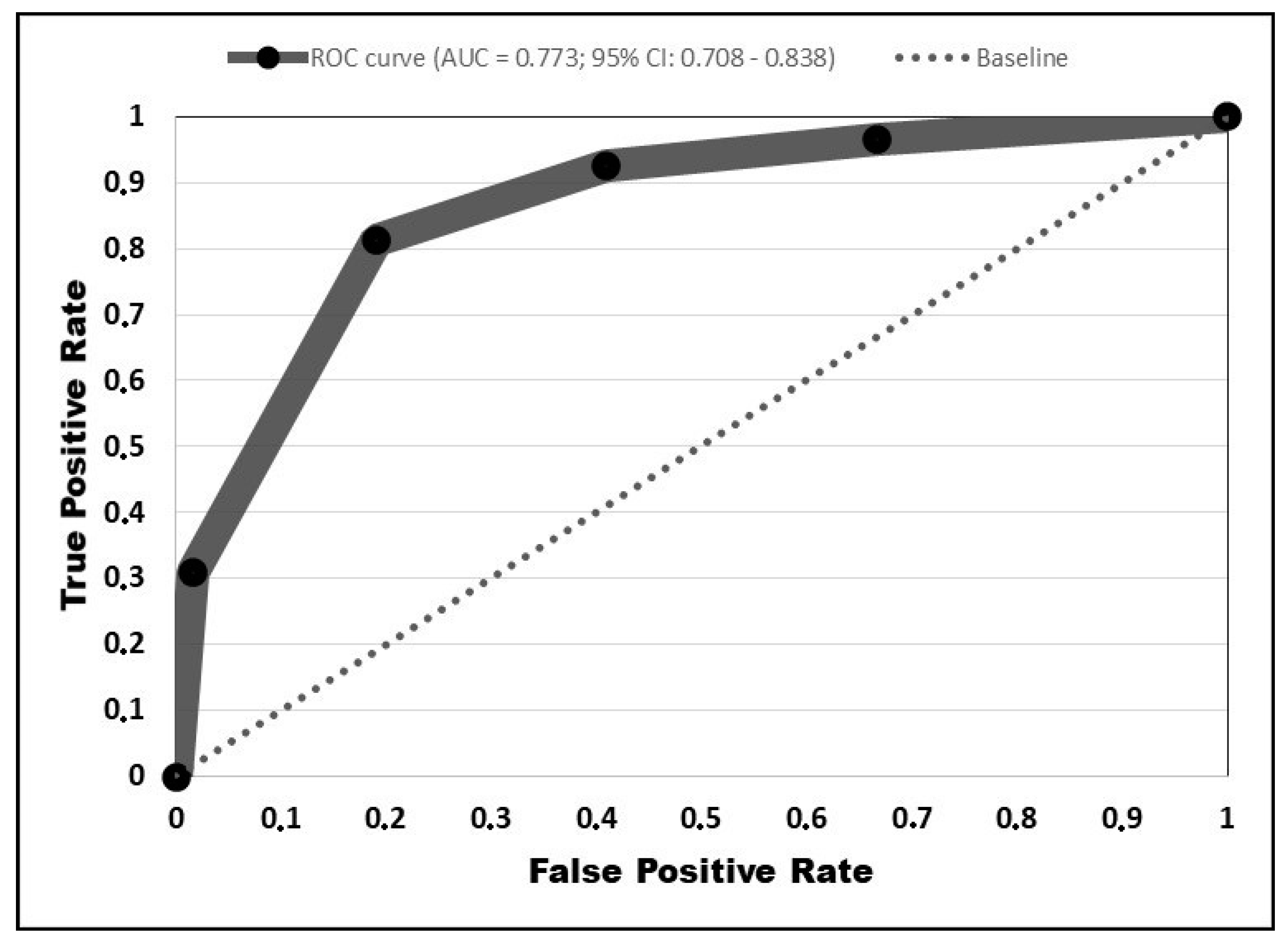
3.4. Model Performance
4. Discussion
4.1. Interpretation
4.2. Implications
4.3. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 10 January 2021).
- Phelan, A.L.; Katz, R.; Gostin, L.O. The novel coronavirus originating in Wuhan, China: Challenges for global health governance. JAMA 2020, 323, 709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef] [PubMed]
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibekwe, T.S.; Fasunla, A.J.; Orimadegun, A. Systematic Review and Meta-analysis of Smell and Taste Disorders in COVID-19. OTO Open 2020, 4. [Google Scholar] [CrossRef] [PubMed]
- Lovato, A.; de Filippis, C. Clinical Presentation of COVID-19: A Systematic Review Focusing on Upper Airway Symptoms. Ear Nose Throat J. 2020, 99, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns Hopkins University of Medicine. Coronavirus Resource Center: Mortality Analyses. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/data/mortality (accessed on 10 January 2021).
- Cao, Y.; Hiyoshi, A.; Montgomery, S. COVID-19 case-fatality rate and demographic and socioeconomic influencers: Worldwide spatial regression analysis based on country-level data. BMJ Open 2020, 10, e043560. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, T.; Yamada, A.; Takahashi, M.; Niikura, R.; Toyama, K.; Ushiku, T.; Kurokawa, M.; Momose, T.; Fukayama, M.; Koike, K. Development and Internal Validation of a Risk Scoring System for Gastrointestinal Events Requiring Surgery in Gastrointestinal Lymphoma Patients. J. Gastroenterol. Hepatol. 2018, 34, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Wu, P.; Lu, W.; Liu, K.; Ma, K.; Huang, L.; Cai, J.; Zhang, H.; Qin, Y.; Sun, H.; et al. Sex-specific clinical characteristics and prognosis of coronavirus disease-19 infection in Wuhan, China: A retrospective study of 168 severe patients. PLoS Pathog. 2020, 16, e1008520. [Google Scholar] [CrossRef] [PubMed]
- Shigui, R. Likelihood of survival of coronavirus disease 2019. Lancet Infect. Dis. 2020, 20, 630–631. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver Operating Characteristic Curve in Diagnostic Test Assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathew, J.G.; Serena, V.R. Remdesivir and COVID-19. Lancet 2020, 396, 953–954. [Google Scholar] [CrossRef]
- Simonis, A.; Theobald, S.J.; Fatkenheuer, G.; Rybniker, J.; Malin, J.J. A comparative analysis of remdesivir and other repurposed antivirals against SARS-CoV-2. EMBO Mol. Med. 2021, 13, e13105. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Shipe, M.E.; Deppen, S.A.; Farjah, F.; Grogan, E.L. Developing prediction models for clinical use using logistic regression: An overview. J. Thorac. Dis. 2019, 11, S574–S584. [Google Scholar] [CrossRef] [PubMed]
- Ghisolfi, S.; Almås, I.; Sandefur, J.C.; Von Carnap, T.; Heitner, J.; Bold, T. Predicted COVID-19 fatality rates based on age, sex, comorbidities and health system capacity. BMJ Glob. Health 2020, 5, e003094. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W. COVID-19 and African Americans. JAMA 2020, 323, 1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahri, K.M.; Hamid, R.N.; Fariba, R. COVID-19 and hematology findings based on the current evidences: A puzzle with many missing pieces. Int. J. Lab. Hematol. 2021, 43, 160–168. [Google Scholar] [CrossRef]
- Słomka, A.; Kowalewski, M.; Żekanowska, E. Coronavirus Disease 2019 (COVID-19): A Short Review on Hematological Manifestations. Pathogens 2020, 9, 493. [Google Scholar] [CrossRef] [PubMed]
- Stoian, A.P.; Pricop-Jeckstadt, M.; Pana, A.; Ileanu, B.-V.; Schitea, R.; Geanta, M.; Catrinoiu, D.; Suceveanu, A.I.; Serafinceanu, C.; Pituru, S.; et al. Death by SARS-CoV 2: A Romanian COVID-19 multi-centre comorbidity study. Sci. Rep. 2020, 10, 21613. [Google Scholar] [CrossRef] [PubMed]
- CDC—Centers for Disease Control and Prevention. People with Certain Medical Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 10 January 2021).



{kind=link}
{kind=link}
| Characteristic | Non-Survivors (n = 310) | Survivors (n = 200) | p-Value |
|---|---|---|---|
| Mean age (range) * | 67 (27–98) | 49 (18–90) | <0.00001 |
| Male | 192 (61.9) | 91 (45.5) | - |
| Female | 118 (38) | 109 (51.9) | - |
| Malignancy | 24 (7.7) | 0 (0.0) | 0.00005 |
| Lung disease | 57 (18.3) | 7 (3.5) | <0.00001 |
| Hypertension | 113 (36.4) | 57 (28.5) | 0.063 |
| Diabetes | 106 (34.2) | 37 (18.5) | 0.0001 |
| Heart disease | 121 (39) | 20 (10.0) | <0.00001 |
| Kidney disease | 52 (16.8) | 6 (3.0) | <0.00001 |
| Liver disease | 40 (12.9) | 4 (2.0) | 0.00002 |
| Obesity | 45 (14.5) | 13 (6.5) | 0.005 |
| Autoimmune disease | 13 (4.2) | 5 (2.5) | 0.312 |
| Recent surgery | 13 (4.2) | 1 (0.5) | 0.013 |
| Neurologic disorders | 53 (17) | 5 (2.5) | <0.00001 |
| Stroke | 27 (8.7) | 3 (1.5) | 0.001 |
| Hematological disturbances | 19 (6.1) | 0 (0.0) | 0.0003 |
| Probability | Risk | Score |
|---|---|---|
| <10% | Very Low | 1 |
| 10–30% | Low | 2 |
| 31–50% | Medium | 3 |
| 51–70% | High | 4 |
| >70% | Very High | 5 |
| Comorbid Condition | p-Value | OR (99% CI) |
|---|---|---|
| Malignancy | 0.003 | 7.6 (1.1–19.6) |
| Lung disease | 0.0003 | 5.1 (1.5–16.5) |
| Diabetes mellitus | 0.001 | 2.3 (1.1–4.4) |
| Heart disease | <0.0001 | 5.6 (2.6–11.8) |
| Kidney disease | 0.0004 | 5.5 (1.5–19.4) |
| Liver disease | 0.03 | 3.6 (0.7–16.9) |
| Obesity | 0.003 | 3.1 (1.1–8.0) |
| Neurological disorders | 0.0001 | 7.4 (1.9–27.7) |
| Stroke | 0.002 | 7.9 (1.4–43.3) |
| Hematology disturbances | 0.0001 | 8.4 (1.4–3.3) |
| Predicted | Lives | Dies | Result |
|---|---|---|---|
| <10% | 34 | 3 | 8% |
| 10–30% | 64 | 21 | 24% |
| 31–50% | 78 | 35 | 31% |
| 51–70% | 90 | 97 | 52% |
| >70% | 33 | 86 | 72% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marincu, I.; Bratosin, F.; Vidican, I.; Bostanaru, A.-C.; Frent, S.; Cerbu, B.; Turaiche, M.; Tirnea, L.; Timircan, M. Predictive Value of Comorbid Conditions for COVID-19 Mortality. J. Clin. Med. 2021, 10, 2652. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122652
Marincu I, Bratosin F, Vidican I, Bostanaru A-C, Frent S, Cerbu B, Turaiche M, Tirnea L, Timircan M. Predictive Value of Comorbid Conditions for COVID-19 Mortality. Journal of Clinical Medicine. 2021; 10(12):2652. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122652
Chicago/Turabian StyleMarincu, Iosif, Felix Bratosin, Iulia Vidican, Andra-Cristina Bostanaru, Stefan Frent, Bianca Cerbu, Mirela Turaiche, Livius Tirnea, and Madalina Timircan. 2021. "Predictive Value of Comorbid Conditions for COVID-19 Mortality" Journal of Clinical Medicine 10, no. 12: 2652. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122652