
The Spectrum of Central Choriocapillaris Abnormalities on Swept-Source Optical Coherence Tomography Angiography in the Fellow Eye of Unilateral Exudative Age-Related Macular Degeneration Patients: From Flow Deficits to Subclinical Non-Exudative Neovascularization

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Imaging
2.2. Image Processing
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinical Characteristics
3.2. OCTA Spectrum of Choriocapillaris Abnormalities
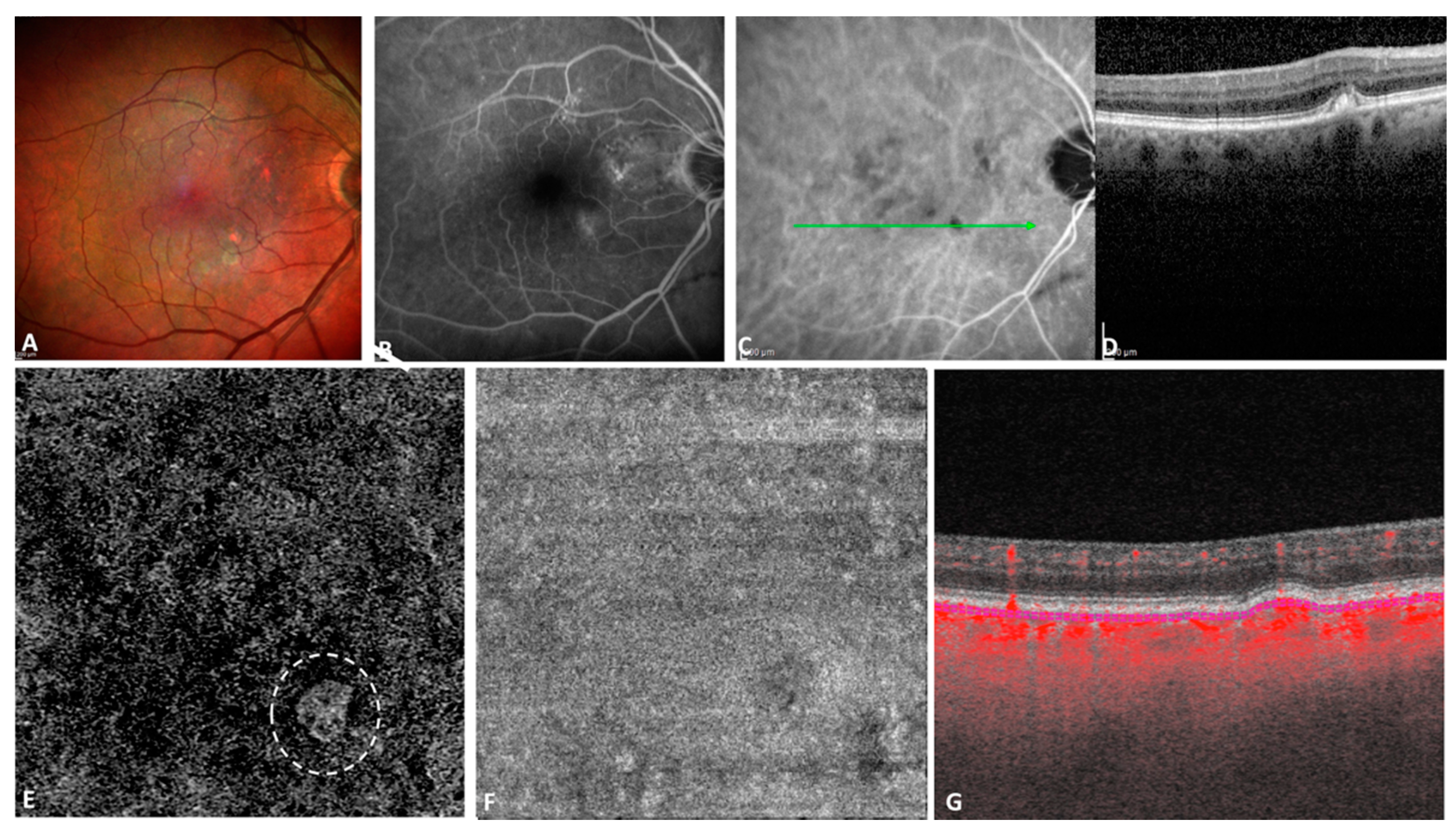
3.2.1. Neovascularization: Subclinical Non-Exudative MNV
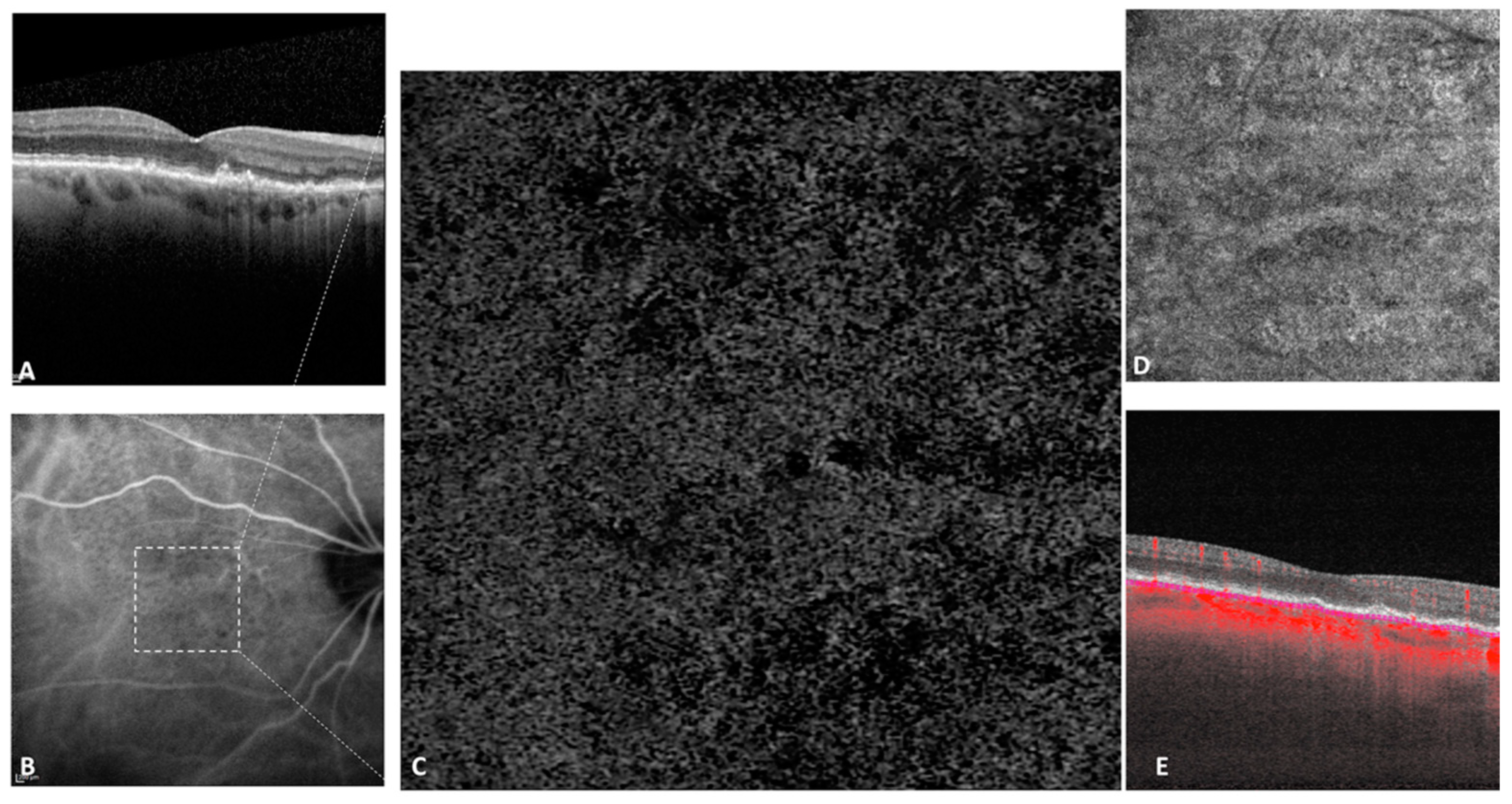
3.2.2. Choriocapillaris Flow Deficits in Non-Neovascular Fellow Eyes
3.2.3. Sensitivity Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bressler, N.M. Age-related macular degeneration is the leading cause of blindness. JAMA 2004, 291, 1900–1901. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.J.; Agrón, E.; Clemons, T.E.; Domalpally, A.; van Asten, F.; Keenan, T.D.; Cukras, C.; Chew, E.Y.; Age-Related Eye Disease Study 2 Research Group. Natural History of Drusenoid Pigment Epithelial Detachment Associated with Age-Related Macular Degeneration: Age-Related Eye Disease Study 2 Report No. 17. Ophthalmology 2019, 126, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Uji, A.; Sarraf, D.; Sadda, S.R. Alterations in the Choriocapillaris in Intermediate Age-Related Macular Degeneration. Investig. Ophthalmol. Vis. Sci. 2017, 58, 4792–4798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramrattan, R.S.; van der Schaft, T.L.; Mooy, C.M.; de Bruijn, W.C.; Mulder, P.G.; de Jong, P.T. Morphometric analysis of Bruch’s membrane, the choriocapillaris, and the choroid in aging. Investig. Ophthalmol. Vis. Sci. 1994, 35, 2857–2864. [Google Scholar]
- Grunwald, J.E.; Metelitsina, T.I.; Dupont, J.C.; Ying, G.S.; Maguire, M.G. Reduced foveolar choroidal blood flow in eyes with increasing AMD severity. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1033–1038. [Google Scholar] [CrossRef] [Green Version]
- Bhutto, I.; Lutty, G. Understanding age-related macular degeneration (AMD): Relationships between the photoreceptor/retinal pigment epithelium/Bruch’s membrane/choriocapillaris complex. Mol. Asp. Med. 2012, 33, 295–317. [Google Scholar] [CrossRef] [Green Version]
- Spaide, R.F. Choriocapillaris Flow Features Follow a Power Law Distribution: Implications for Characterization and Mechanisms of Disease Progression. Am. J. Ophthalmol. 2016, 170, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Sarraf, D.; Freund, K.B.; Sadda, S.R. OCT angiography and evaluation of the choroid and choroidal vascular disorders. Prog. Retin. Eye Res. 2018, 67, 30–55. [Google Scholar] [CrossRef]
- Zheng, F.; Zhang, Q.; Shi, Y.; Russell, J.F.; Motulsky, E.H.; Banta, J.T.; Chu, Z.; Zhou, H.; Patel, N.A.; de Sisternes, L.; et al. Age-dependent Changes in the Macular Choriocapillaris of Normal Eyes Imaged with Swept-Source Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2019, 200, 110–122. [Google Scholar] [CrossRef]
- Borrelli, E.; Shi, Y.; Uji, A.; Balasubramanian, S.; Nassisi, M.; Sarraf, D.; Sadda, S.R. Topographic Analysis of the Choriocapillaris in Intermediate Age-related Macular Degeneration. Am. J. Ophthalmol. 2018, 196, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Green, W.R.; Key, S.N., 3rd. Senile macular degeneration: A histopathologic study. Trans. Am. Ophthalmol. Soc. 1977, 75, 180–254. [Google Scholar]
- Sarks, S.H. New vessel formation beneath the retinal pigment epithelium in senile eyes. Br. J. Ophthalmol. 1973, 57, 951–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Querques, G.; Srour, M.; Massamba, N.; Georges, A.; Ben Moussa, N.; Rafaeli, O.; Souied, E.H. Functional characterization and multimodal imaging of treatment-naive “quiescent” choroidal neovascularization. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6886–6892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnevali, A.; Cicinelli, M.V.; Capuano, V.; Corvi, F.; Mazzaferro, A.; Querques, L.; Scorcia, V.; Souied, E.H.; Bandello, F.; Querques, G. Optical Coherence Tomography Angiography: A Useful Tool for Diagnosis of Treatment-Naïve Quiescent Choroidal Neovascularization. Am. J. Ophthalmol. 2016, 169, 189–198. [Google Scholar] [CrossRef]
- Roisman, L.; Zhang, Q.; Wang, R.K.; Gregori, G.; Zhang, A.; Chen, C.L.; Durbin, M.K.; An, L.; Stetson, P.F.; Robbins, G.; et al. Optical Coherence Tomography Angiography of Asymptomatic Neovascularization in Intermediate Age-Related Macular Degeneration. Ophthalmology 2016, 123, 1309–1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Zhang, Q.; Motulsky, E.H.; Thulliez, M.; Shi, Y.; Lyu, C.; de Sisternes, L.; Durbin, M.K.; Feuer, W.; Wang, R.K.; et al. Two-Year Risk of Exudation in Eyes with Nonexudative Age-Related Macular Degeneration and Subclinical Neovascularization Detected with Swept Source Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2019, 208, 1–11. [Google Scholar] [CrossRef]
- García-Layana, A.; Cabrera-López, F.; García-Arumí, J.; Arias-Barquet, L.; Ruiz-Moreno, J.M. Early and intermediate age-related macular degeneration: Update and clinical review. Clin. Interv. Aging 2017, 12, 1579–1587. [Google Scholar] [CrossRef] [Green Version]
- Spaide, R.F. Disease Expression in Nonexudative Age-Related Macular Degeneration Varies with Choroidal Thickness. Retina 2018, 38, 708–716. [Google Scholar] [CrossRef]
- Zhang, Q.; Zheng, F.; Motulsky, E.H.; Gregori, G.; Chu, Z.; Chen, C.L.; Li, C.; de Sisternes, L.; Durbin, M.; Rosenfeld, P.J.; et al. A Novel Strategy for Quantifying Choriocapillaris Flow Voids Using Swept-Source OCT Angiography. Investig. Ophthalmol. Vis. Sci. 2018, 59, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Chu, Z.; Cheng, Y.; Zhang, Q.; Zhou, H.; Dai, Y.; Shi, Y.; Gregori, G.; Rosenfeld, P.J.; Wang, R.K. Quantification of Choriocapillaris with Phansalkar Local Thresholding: Pitfalls to Avoid. Am. J. Ophthalmol. 2020, 213, 161–176. [Google Scholar] [CrossRef]
- Sacconi, R.; Borrelli, E.; Corbelli, E.; Capone, L.; Rabiolo, A.; Carnevali, A.; Casaluci, M.; Gelormini, F.; Querques, L.; Bandello, F.; et al. Quantitative changes in the ageing choriocapillaris as measured by swept source optical coherence tomography angiography. Br. J. Ophthalmol. 2019, 103, 1320–1326. [Google Scholar] [CrossRef]
- Spaide, R.F. Improving the Age-Related Macular Degeneration Construct: A New Classification System. Retina 2018, 38, 891–899. [Google Scholar] [CrossRef]
- Nassisi, M.; Baghdasaryan, E.; Tepelus, T.; Asanad, S.; Borrelli, E.; Sadda, S.R. Topographic distribution of choriocapillaris flow deficits in healthy eyes. PLoS ONE 2018, 13, e0207638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uji, A.; Balasubramanian, S.; Lei, J.; Baghdasaryan, E.; Al-Sheikh, M.; Sadda, S.R. Choriocapillaris Imaging Using Multiple En Face Optical Coherence Tomography Angiography Image Averaging. JAMA Ophthalmol. 2017, 135, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Byon, I.; Nassisi, M.; Borrelli, E.; Sadda, S.R. Impact of Slab Selection on Quantification of Choriocapillaris Flow Deficits by Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2019, 208, 397–405. [Google Scholar] [CrossRef]
- Chu, Z.; Gregori, G.; Rosenfeld, P.J.; Wang, R.K. Quantification of Choriocapillaris with Optical Coherence Tomography Angiography: A Comparison Study. Am. J. Ophthalmol. 2019, 208, 111–123. [Google Scholar] [CrossRef]
- Nassisi, M.; Baghdasaryan, E.; Borrelli, E.; Ip, M.; Sadda, S.R. Choriocapillaris flow impairment surrounding geographic atrophy correlates with disease progression. PLoS ONE 2019, 14, e0212563. [Google Scholar] [CrossRef] [PubMed]
- Treister, A.D.; Nesper, P.L.; Fayed, A.E.; Gill, M.K.; Mirza, R.G.; Fawzi, A.A. Prevalence of Subclinical CNV and Choriocapillaris Nonperfusion in Fellow Eyes of Unilateral Exudative AMD on OCT Angiography. Transl. Vis. Sci. Technol. 2018, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira Dias, J.R.; Zhang, Q.; Garcia, J.M.B.; Zheng, F.; Motulsky, E.H.; Roisman, L.; Miller, A.; Chen, C.L.; Kubach, S.; de Sisternes, L.; et al. Natural History of Subclinical Neovascularization in Nonexudative Age-Related Macular Degeneration Using Swept-Source OCT Angiography. Ophthalmology 2018, 125, 255–266. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Gender | Age | BCVA (logMAR) | BCVA (Snellen Equivalent) | Small Drusen | Large Drusen | Drusenoid PED | Atrophy | Reticular Pseudodrusen | CMT (µm) | CT (µm) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Female | 72 | 0.1 | 20/25 | 1 | 1 | 1 | 0 | 1 | 252 | 257 |
| 2 | Female | 78 | 0.0 | 20/20 | 0 | 0 | 1 | 0 | 0 | 211 | 139 |
| 3 | Male | 80 | 0.2 | 20/32 | 0 | 0 | 1 | 0 | 0 | 338 | 136 |
| 4 | Male | 82 | 0.1 | 20/25 | 0 | 0 | 0 | 0 | 0 | 249 | 289 |
| 5 | Female | 91 | 0.3 | 20/40 | 1 | 1 | 1 | 0 | 1 | 264 | 243 |
| 6 | Female | 72 | 0.1 | 20/25 | 1 | 1 | 1 | 0 | 1 | 244 | 382 |
| 7 | Female | 89 | 0.2 | 20/32 | 0 | 0 | 1 | 0 | 1 | 239 | 268 |
| 8 | Female | 88 | 0.0 | 20/20 | 0 | 1 | 1 | 0 | 0 | 204 | 102 |
| Non-Neovascular Study Eyes (n = 89) | Neovascular † Study Eyes (n = 8) | p-Value | |
|---|---|---|---|
| Mean Age (years) | 79 (±7.70) | 82 (±7.41) | 0.41 * |
| BCVA (logMAR) | 0.18 (±0.46) | 0.12 (±0.10) | 0.21 * |
| Small drusen (n,%) | 59 (66.29%) | 3 (37.5%) | 0.13 ** |
| Large drusen (n,%) | 65 (73.03%) | 4 (50%) | 0.22 ** |
| Drusenoid PED (n,%) | 37 (41.57%) | 7 (87.50%) | 0.021 ** |
| Reticular pseudodrusen (n,%) | 50 (56.18%) | 4 (50%) | 1.0 ** |
| Atrophy (n,%) | 19 (21.35%) | 0 (0%) | 0.34 ** |
| CMT (µm) | 231.95 (±43.74) | 250.13 (±40.95) | 0.20 * |
| CT (µm) | 209.09 (±83.04) | 227 (±94.38) | 0.63 * |
| Mean (SD) | |
|---|---|
| Percentage of flow deficits (%) | 45.84 (±11.63) |
| Number of flow deficits | 1964.74 (±1063.19) |
| Size of flow deficits (µm2) | 5076.49 µm2 (±9984.51) |
| Area of flow deficits (mm2) | 4.19 (±1.12) |
| Linear Regression on | Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| Coef. † | Std. Err. | p Value | Coef. † | Std. Err. | p Value | ||
| Percentage of flow deficits * | Age * | 0.77 | 0.26 | 0.004 | 0.62 | 0.26 | 0.02 |
| CMT * | −0.04 | 0.07 | 0.59 | ||||
| CT * | −0.16 | 0.05 | 0.003 | ||||
| Small drusen | 0.03 | 0.05 | 0.55 | −0.13 | 0.05 | 0.017 | |
| Large drusen | 0.12 | 0.06 | 0.03 | ||||
| Drusenoid PED | 0.09 | 0.05 | 0.09 | ||||
| Atrophy | 0.14 | 0.06 | 0.02 | ||||
| RPD | 0.14 | 0.05 | 0.007 | ||||
| Size of flow deficits * | Age * | 3.44 | 1.13 | 0.003 | 2.69 | 1.13 | 0.019 |
| CMT * | −0.15 | 0.32 | 0.64 | ||||
| CT * | −0.81 | 0.23 | 0.001 | −0.68 | 0.23 | 0.005 | |
| Small drusen | 0.16 | 0.24 | 0.49 | ||||
| Large drusen | 0.47 | 0.25 | 0.07 | ||||
| Drusenoid PED | 0.34 | 0.23 | 0.13 | ||||
| Atrophy | 0.61 | 0.27 | 0.029 | ||||
| RPD | 0.53 | 0.22 | 0.02 | ||||
| Number of flow deficits * | Age * | −2.74 | 0.80 | 0.001 | −2.25 | 0.80 | 0.007 |
| CMT * | 0.12 | 0.23 | 0.59 | ||||
| CT * | 0.57 | 0.17 | 0.001 | 0.46 | 0.17 | 0.008 | |
| Small drusen | −0.05 | 0.17 | 0.76 | ||||
| Large drusen | −0.24 | 0.18 | 0.19 | ||||
| Drusenoid PED | −0.21 | 0.16 | 0.21 | ||||
| Atrophy | −0.43 | 0.19 | 0.03 | ||||
| RPD | −0.33 | 0.16 | 0.048 | ||||
| Mean (SD) Radius 4 | Mean (SD) Radius 8 | Mean (SD) Radius 10 | Mean (SD) Radius 15 Pixel | |
|---|---|---|---|---|
| Percentage of flow deficits (%) | 41.74 (±15.26) | 44.81 (±12.43) | 45.52 (±12.01) | 45.84 (±11.63) |
| Number of flow deficits | 3381.08 (±1735.01) | 2405.87 (±1347.19) | 2151.26 (±1218.96) | 1964.74 (±1063.19) |
| Size of flow deficits (µm2) | 4198.77 (±14,929.13) | 5253.17 (±13,861.42) | 5548.82 (±13,471.32) | 5076.49 (±9984.51) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khorrami Kashi, A.; Souied, E.; Fares, S.; Borrelli, E.; Capuano, V.; Jung, C.; Querques, G.; Mouallem, A.; Miere, A. The Spectrum of Central Choriocapillaris Abnormalities on Swept-Source Optical Coherence Tomography Angiography in the Fellow Eye of Unilateral Exudative Age-Related Macular Degeneration Patients: From Flow Deficits to Subclinical Non-Exudative Neovascularization. J. Clin. Med. 2021, 10, 2658. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122658
Khorrami Kashi A, Souied E, Fares S, Borrelli E, Capuano V, Jung C, Querques G, Mouallem A, Miere A. The Spectrum of Central Choriocapillaris Abnormalities on Swept-Source Optical Coherence Tomography Angiography in the Fellow Eye of Unilateral Exudative Age-Related Macular Degeneration Patients: From Flow Deficits to Subclinical Non-Exudative Neovascularization. Journal of Clinical Medicine. 2021; 10(12):2658. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122658
Chicago/Turabian StyleKhorrami Kashi, Alexis, Eric Souied, Selim Fares, Enrico Borrelli, Vittorio Capuano, Camille Jung, Giuseppe Querques, Alexandra Mouallem, and Alexandra Miere. 2021. "The Spectrum of Central Choriocapillaris Abnormalities on Swept-Source Optical Coherence Tomography Angiography in the Fellow Eye of Unilateral Exudative Age-Related Macular Degeneration Patients: From Flow Deficits to Subclinical Non-Exudative Neovascularization" Journal of Clinical Medicine 10, no. 12: 2658. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122658