
Short- and Mid-Term Outcomes in Patients Deemed Inoperable Undergoing Transapical and Transfemoral TAVR with an STS-PROM below Four Percent

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
3.2. General Procedural Characteristics
3.3. Thirty-Day Outcome and Functional Status
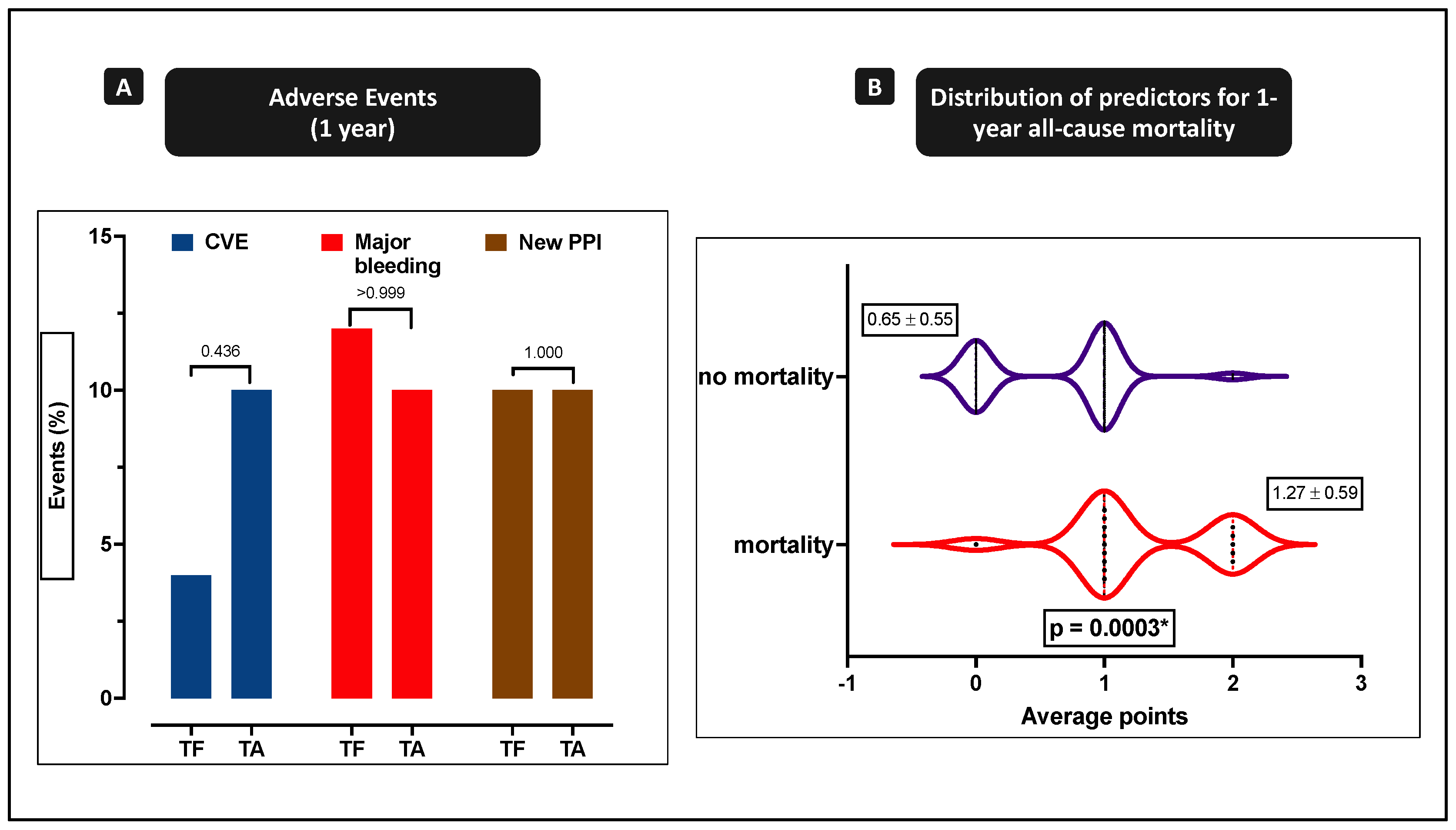
3.4. One-Year Clinical Outcome
4. Discussion
- Mortality after 30 days was only mildly enhanced in TA patients and twice as high after one year.
- Cerebrovascular events, major bleeding, and even pacemaker need were nearly similar during a one-year follow-up in TF and TA patients.
- Other factors besides transapical access were identified as independent predictors for one-year mortality in low-risk patients (hemoglobin < 12 g/dL at admission and use of dual antiplatelet therapy).
4.1. Alternative Access Sites
4.2. Procedural Characteristics
4.3. Thirty-Day Outcome
4.4. One-Year Clinical Outcome and Independent Predictors for All-Cause One-Year Mortality
4.5. Current Knowledge on One-Year Mortality in Low-Risk Patients Using Alternative Access Routes
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koifman, E.; Magalhaes, M.; Kiramijyan, S.; Escarcega, R.O.; Didier, R.; Torguson, R.; Ben-Dor, I.; Corso, P.; Shults, C.; Satler, L.; et al. Impact of transfemoral versus transapical access on mortality among patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Cardiovasc. Revasc. Med. 2016, 17, 318–321. [Google Scholar] [CrossRef]
- Elmariah, S.; Fearon, W.F.; Inglessis, I.; Vlahakes, G.J.; Lindman, B.R.; Alu, M.C.; Crowley, A.; Kodali, S.; Leon, M.B.; Svensson, L.; et al. PARTNER Trial Investigators and PARTNER Publications Office. Transapical Transcatheter Aortic Valve Replacement Is Associated with Increased Cardiac Mortality in Patients with Left Ventricular Dysfunction: Insights from the PARTNER I Trial. JACC Cardiovasc. Interv. 2017, 10, 2414–2422. [Google Scholar] [CrossRef]
- Murdock, J.E.; Jensen, H.; Thourani, V. Nontransfemoral approaches to transcatheter aortic valve replacement. Interv. Cardiol. Clin. 2015, 4, 95–105. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Baumgartner, H.; Bax, J.J.; de Bonis, M.; Hamm, C.; Holm, J.; Iung, B.; Lancellotti, P.; Lansac, E.; et al. ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardiothorac. Surg. 2017, 52, 616–664. [Google Scholar]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.-A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. J. Am. Coll. Cardiol. 2012, 60, 1438–1454. [Google Scholar] [CrossRef] [Green Version]
- Gaede, L.; Blumenstein, J.; Husser, O.; Liebetrau, C.; Dörr, O.; Grothusen, C.; Eckel, C.; Al-Terki, H.; Kim, W.K.; Nef, H.; et al. Aortic valve replacement in Germany in 2019. Clin. Res. Cardiol. 2021, 110, 460–465. [Google Scholar] [CrossRef]
- Greason, K.L.; Suri, R.M.; Nkomo, V.T.; Rihal, C.S.; Holmes, D.R.; Mathew, V. Beyond the learning curve. Transapical versus transfemoral transcatheter aortic valve replacement in the treatment of severe aortic valve stenosis. J. Card. Surg. 2014, 29, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Tuzcu, E.M.; Stewart, W.; Bajaj, N.S.; Svensson, L.G.; Kapadia, S.R. Comparison of multicenter registries and randomized control trials for transcatheter aortic valve replacement (TAVR). Indian Heart J. 2013, 65, 400–411. [Google Scholar] [CrossRef] [Green Version]
- Unbehaun, A.; Pasic, M.; Dreysse, S.; Drews, T.; Kukucka, M.; Mladenow, A.; Ivanitskaja-Kühn, E.; Hetzer, R.; Buz, S. Transapical aortic valve implantation: Incidence and predictors of paravalvular leakage and transvalvular regurgitation in a series of 358 patients. J. Am. Coll. Cardiol. 2012, 59, 211–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulos, N.; Wenzel, R.; Thudt, M.; Doss, M.; Wimmer-Greinecker, G.; Seeger, F.; Ahmad, A.-S.; Fichtlscherer, S.; Moritz, A.; Zierer, A. A decade of transapical aortic valve implantation. Ann. Thorac. Surg. 2016, 102, 759–765. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.; Schymik, G.; Walther, T.; Himbert, D.; Lefevre, T.; Treede, H.; Eggebrecht, H.; Rubino, P.; Michev, I.; Lange, R.; et al. Thirty-day results of the SAPIEN aortic bioprosthesis European outcome (SOURCE) registry: A European registry of transcatheter aortic valve implantation using the Edwards SAPIEN valve. Circulation 2010, 122, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Greco, A.; Capodanno, D. Anticoagulation after Transcatheter Aortic Valve Implantation: Current Status. Interv. Cardiol. 2020, 15, e02. [Google Scholar] [CrossRef]
- Bosmans, J.M.; Kefer, J.; De Bruyne, B. Belgian TAVI registry participants procedural, 30-day and one year outcome following CoreValve or Edwards transcatheter aortic valve implantation: Results of the Belgian national registry. Interact Cardiovasc. Thorac. Surg. 2011, 12, 762–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ussia, G.P.; Barbanti, M.; Petronio, A. CoreValve Italian registry investigators transcatheter aortic valve implantation: 3-year outcomes of self-expanding CoreValve prosthesis. Eur. Heart J. 2012, 33, 969–976. [Google Scholar] [CrossRef] [Green Version]
- Vahanian, A.; Alfieri, O.; Al-Attar, N. European Association of Cardio-Thoracic Surgery; European Society of Cardiology; European Association of Percutaneous Cardiovascular Interventions. Transcatheter valve implantation for patients with aortic stenosis: A position statement from the European Association of Cardio-Thoracic Surgery (EACTS) and the European Society of Cardiology (ESC), in collaboration with the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2008, 29, 1463–1470. [Google Scholar]
- Panchal, H.B.; Ladia, V.; Amin, P.; Patel, P.; Veeranki, S.P.; Albalbissi, K.; Paul, T. A meta-analysis of mortality and major adverse cardiovascular and cerebrovascular events in patients undergoing transfemoral versus transapical transcatheter aortic valve implantation using Edwards valve for severe aortic stenosis. Am. J. Cardiol. 2014, 114, 1882–1890. [Google Scholar] [CrossRef] [PubMed]
- Athappan, G.; Gajulapalli, R.D.; Sengodan, P.; Bhardwaj, A.; Ellis, S.G.; Svensson, L.; Tuzcu, E.M.; Kapadia, S.R. Influence of transcatheter aortic valve replacement strategy and valve design on stroke after transcatheter aortic valve replacement: A meta-analysis and systematic review of literature. JACC 2014, 63, 2101–2110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, N.; Khera, R.; Fonarow, G.C.; Bhatt, D.L. Comparison of outcomes of transfemoral versus transapical approach for transcatheter aortic valve implantation. Am. J. Cardiol. 2018, 122, 1520–1526. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisriec, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Thyregod HG, H.; Steinbrüchel, D.A.; Ihlemann, N.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Chang, Y.; Franzen, O.W.; Engstrøm, T.; Clemmensen, P.; et al. Transcatheter versus surgical aortic valve replacement in patients with severe aortic valve stenosis: 1-year results from the all-comers NOTION randomized clinical trial. JACC 2015, 65, 2184–2194. [Google Scholar] [PubMed] [Green Version]
- Beurtheret, S.; Karam, N.; Resseguier, N.; Houel, R.; Modine, T.; Folliguet, T.; Chamandi, C.; Com, O.; Gelisse, R.; Bille, J.; et al. Femoral Versus Nonfemoral Peripheral Access for Transcatheter Aortic Valve Replacement. JACC 2019, 74, 2728–2739. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Data | Overall (n = 100) | TF (n = 50) | TA (n = 50) | p-Value |
|---|---|---|---|---|
| Age, years | 74.5 ± 8.3 | 75.7 ± 8.3 | 73.4 ± 8.3 | 0.180 |
| Gender, male | 68 (68.0) | 27 (54.0) | 41 (82.0) | 0.003 * |
| BMI | 28.0 ± 4.6 | 28.3 ± 4.6 | 27.7 ± 4.6 | 0.556 |
| CAD | 72 (72.0) | 35 (70) | 37 (74.0) | 0.656 |
| Previous PCI | 31 (31.0) | 16 (32.0) | 15 (30.0) | 0.829 |
| Previous CABG | 23 (23.0) | 10 (20.0) | 13 (26.0) | 0.476 |
| Previous valve | 4 (4.0) | 2 (4.0) | 2 (4.0) | 1.000 |
| Previous PPI | 12 (12.0) | 6 (12.0) | 6 (12.0) | 1.000 |
| Preexisting LBBB/RBBB | 5 (5.0) | 3 (6.0) | 2 (4.0) | 0.646 |
| Preexisting AVB | 2 (2.0) | 1 (2.0) | 1 (2.0) | 1.000 |
| Arterial hypertension | 94 (94.0) | 46 (92.0) | 48 (96.0) | 0.400 |
| PHT | 54 (54.0) | 29 (58.0) | 25 (50.0) | 0.422 |
| Diabetes mellitus | 29 (29.0) | 14 (28.0) | 15 (30.0) | 0.826 |
| PAD | 49 (49.0) | 20 (40.0) | 29 (58.0) | 0.072 |
| CVD | 24 (24.0) | 15 (30.0) | 9 (18.0) | 0.160 |
| Porcelain aorta | 23 (23.0) | 11 (22.0) | 12 (24.0) | 0.812 |
| Hostile Aorta | 14 (14.0) | 6 (12.0) | 8 (16.0) | 0.564 |
| Previous RRT | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| CKD | 36 (36.0) | 21 (42.0) | 15 (30.0) | 0.211 |
| COPD | 23 (23.0) | 10 (20.0) | 13 (26.0) | 0.476 |
| Frailty | 38 (38.0) | 25 (50.0) | 13 (26.0) | 0.013 * |
| Functional Data | ||||
| STS score, % | 2.7 ± 0.8 | 2.8 ± 0.7 | 2.5 ± 0.9 | 0.075 |
| HAS-BLED score | 2.9 ± 1.0 | 2.9 ± 0.9 | 2.8 ± 1.0 | 0.421 |
| LVEF, % | 50.4 ± 11.6 | 46.3 ± 10.7 | 52.7 ± 11.7 | 0.194 |
| AVA, cm2 | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.318 |
| dPmax, mmHg | 63.7 ± 21.1 | 61.9 ± 18.2 | 65.7 ± 23.9 | 0.424 |
| dPmean, mmHg | 39.5 ± 15.5 | 36.2 ± 12.7 | 43.2 ± 17.7 | 0.043 * |
| NYHA III/IV | 64 (64.0) | 31 (62.0) | 33 (66.0) | 0.677 |
| Procedural Data | Overall (n = 100) | TF (n = 50) | TA (n = 50) | p-Value |
|---|---|---|---|---|
| Sapien 3TM | 76 (76.0) | 26 (52.0) | 50 (100.0) | <0.001 * |
| CoreValve Evolut R/ProTM | 24 (24.0) | 24 (48.0) | 0 (0.0) | <0.001 * |
| Valve-in-Valve | 3 (3.0) | 2 (4.0) | 1 (2.0) | 0.558 |
| Bicuspid Valve | 1 (1.0) | 1 (2.0) | 0 (0.0) | 0.315 |
| +MIDCAB | 2 (2.0) | 0 (0.0) | 2 (4.0) | 0.153 |
| +PCI | 1 (1.0) | 1 (2.0) | 1 (2.0) | 0.315 |
| Contrast, mL | 118.0 ± 54.6 | 143.0 ± 62.5 | 93.0 ± 28.9 | <0.001 * |
| Fluoroscopy time, min | 14.3 ± 8.1 | 20.3 ± 5.5 | 8.1 ± 5.0 | <0.001 * |
| Dose Area Product, Gyx, cm2 | 5.289 ± 4.117 | 7.429 ± 4.211 | 3.012 ± 2.491 | <0.001 * |
| Predilatation | 90 (90.0) | 41 (82.0) | 49 (98.0) | 0.008 * |
| Postdilatation | 6 (6.0) | 6 (12.0) | 0 (0) | 0.012 * |
| Intraproced. Complications | ||||
| Immediate stroke | 1 (1.0) | 1 (2.0) | 0 (0) | 0.315 |
| Aortic dissection | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Annulus rupture | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Coronary obstruction | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Vascular complications | 11 (11.0) | 8 (16.0) | 3 (6.0) | 0.110 |
| Valve dislocation | 1 (1.0) | 0 (0) | 1 (2.0) | 0.315 |
| Conversion to surgery | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Need of 2nd valve | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Tamponade | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| CPR | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Immediate procedural death | 1 (1.0) | 0 (0.0) | 1 (2.0) | 0.315 |
| Heart rhythm disturbances | 2 (2.0) | 1 (2.0) | 1 (2.0) | 1.000 |
| Postprocedural Outcome | Overall (n = 100) | TF (n = 50) | TA (n = 50) | p-Value |
|---|---|---|---|---|
| 30-day mortality | 2 (2.0) | 0 (0.0) | 2 (4.0) | 0.153 |
| Disabling bleeding | 7 (7.0) | 3 (6.0) | 4 (8.0) | 0.695 |
| Major bleeding | 6 (6.0) | 2 (4.0) | 4 (8.0) | 0.400 |
| Major vascular complications | 14 (14.0) | 6 (12.0) | 8 (16.0) | 0.564 |
| Stroke/TIA | 4 (4.0) | 2 (4.0) | 2 (4.0) | 1.000 |
| AKI I-III | 15 (15.0) | 7 (14.0) | 8 (16.0) | 0.736 |
| AKI I | 10 (10.0) | 4 (8.0) | 6 (12.0) | 0.505 |
| AKI II | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| AKI III | 5 (5.0) | 3 (6.0) | 2 (4.0) | 0.646 |
| New RRT | 5 (5.0) | 3 (6.0) | 2 (4.0) | 0.646 |
| Sepsis | 2 (2.0) | 2 (4.0) | 0 (0.0) | 0.153 |
| Endocarditis | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| New LBBB/RBBB | 15 (15.0) | 10 (20.0) | 5 (10.0) | 0.262 |
| New AVB | 6 (6.0) | 3 (6.0) | 3 (6.0) | 1.000 |
| New PPI | 5 (5.0) | 2 (4.0) | 3 (6.0) | 0.646 |
| In-hospital stay | 14.8 ± 7.4 | 13.3 ± 7.0 | 16.3 ± 7.5 | 0.042 * |
| ICU stay | 5.2 ± 4.1 | 3.9 ± 4.1 | 6.5 ± 3.6 | 0.001 * |
| Functional Data at Discharge | ||||
| Vmax (m/s) | 2.2 ± 0.4 | 2.2 ± 0.4 | 2.2 ± 0.4 | 0.931 |
| dPmean (mmHg) | 11.1 ± 3.1 | 10.6 ± 3.8 | 11.8 ± 3.3 | 0.184 |
| AR ≥ II° (PVL) | 4 (4.0) | 2 (4.0) | 2 (4.0) | 1.000 |
| MR ≥ II° | 12 (12.0) | 4 (8.0) | 8 (16.0) | 0.218 |
| TR ≥ II° | 7 (7.0) | 1 (2.0) | 6 (12.0) | 0.050 |
| MV disease ≥ II° | 22 (22.0) | 9 (18.0) | 13 (26.0) | 0.334 |
| Medication at Discharge | ||||
| DPT | 53 (53.0) | 31 (62.0) | 22 (44.0) | 0.071 |
| N/OAC mono | 12 (12.0) | 3 (6.0) | 9 (18.0) | 0.065 |
| N/OAC + SPT | 20 (20.0) | 10 (20.0) | 10 (20.0) | 1.000 |
| Triple therapy | 9 (9.0) | 2 (4.0) | 7 (14.0) | 0.081 |
| Univariate Analysis | Multivariate Analysis | ROC | |||||
|---|---|---|---|---|---|---|---|
| (A) Risk Factors | OR (95%-CI) | p-Value | OR (95%-CI) | p-Value | AUC | 95%-CI | p-Value |
| Disabling bleeding | 9.94 (1.96–50.42) | 0.006 * | - | - | 0.75 | 0.61–0.88 | 0.0024 * |
| TR ≥ II | 5.06 (1.01–25.46) | 0.049 * | - | - | |||
| MV disease ≥ II | 2.88 (0.90–9.24) | 0.076 | - | - | |||
| Urgent TAVR | 2.59 (0.85–7.90) | 0.094 | - | - | |||
| Hemoglobin < 12 g/dL | 3.97 (1.28–12.36) | 0.017 * | 8.14 (1.88–35.20) | 0.005 * | |||
| AKI (stage 3) | 10.38 (1.57–68.60) | 0.015 * | |||||
| (B) Protective Factors | |||||||
| DPT | 0.27 (0.08–0.91) | 0.034 * | 0.09 (0.02–0.43) | 0.003 * | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veulemans, V.; Hellhammer, K.; Borhan Azad, A.; Goh, S.; Drake, C.; Maier, O.; Piayda, K.; Polzin, A.; Mehdiani, A.; Jung, C.; et al. Short- and Mid-Term Outcomes in Patients Deemed Inoperable Undergoing Transapical and Transfemoral TAVR with an STS-PROM below Four Percent. J. Clin. Med. 2021, 10, 2993. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10132993
Veulemans V, Hellhammer K, Borhan Azad A, Goh S, Drake C, Maier O, Piayda K, Polzin A, Mehdiani A, Jung C, et al. Short- and Mid-Term Outcomes in Patients Deemed Inoperable Undergoing Transapical and Transfemoral TAVR with an STS-PROM below Four Percent. Journal of Clinical Medicine. 2021; 10(13):2993. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10132993
Chicago/Turabian StyleVeulemans, Verena, Katharina Hellhammer, Armin Borhan Azad, Shouheng Goh, Christian Drake, Oliver Maier, Kerstin Piayda, Amin Polzin, Arash Mehdiani, Christian Jung, and et al. 2021. "Short- and Mid-Term Outcomes in Patients Deemed Inoperable Undergoing Transapical and Transfemoral TAVR with an STS-PROM below Four Percent" Journal of Clinical Medicine 10, no. 13: 2993. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10132993