
Arterial Remodelling in Chronic Kidney Disease: Impact of Uraemic Toxins and New Pharmacological Approaches


Abstract
:1. Chronic Kidney Disease, Definition and Epidemiology
2. Cardiovascular Risk and Chronic Kidney Disease
3. Arterial Remodelling Associated with CKD
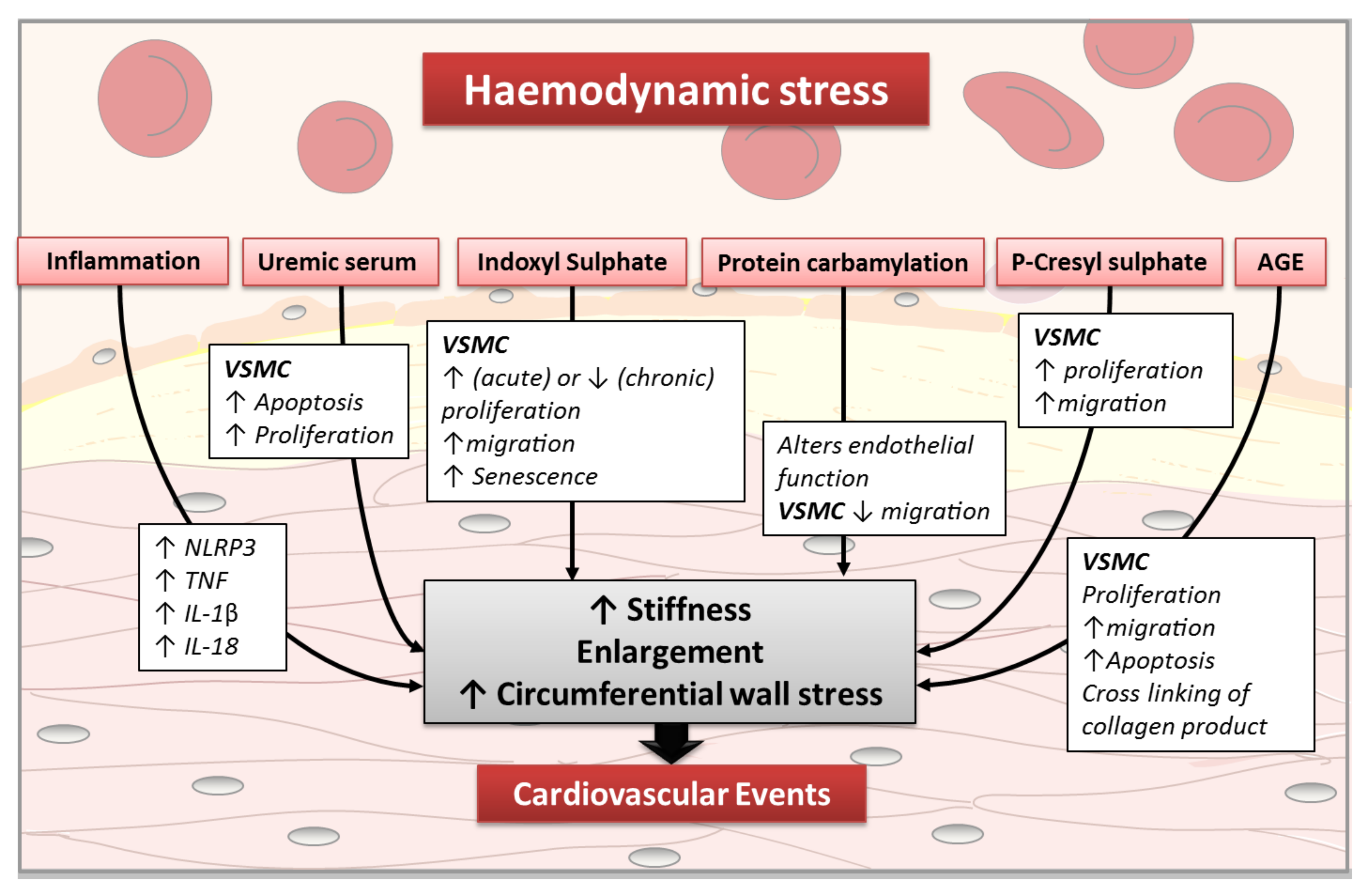
4. Impact of Uraemic Toxins on Arterial Remodelling
5. Uraemic Toxin Definition and Classification
6. Impact of Uraemic Toxins on Vascular Smooth Muscle Cell Functions
6.1. Effect of Uraemic Serum on VSMC Functions
6.2. Effect of Indoxyl Sulphate (IS)
6.3. Effect of P-Cresyl Sulphate (PCS)
6.4. Impact of Protein Carbamylation on Vascular Function
6.5. Effect of Advanced Glycation End Products (AGEs) on VSMC Functions
7. Inflammation and Arterial Remodelling in the Context of CKD
8. Pharmacological Approaches of Uraemia-Linked Arterial Remodelling
Author Contributions
Funding
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Richard Hobbs, F.D. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Brück, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Völzke, H.; Ärnlöv, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Pop-ulation. J. Am. Soc. Nephrol. 2016, 27, 2135–2147. [Google Scholar] [CrossRef] [PubMed]
- GBD. Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Available online: https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf (accessed on 18 August 2021).
- GBD. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Jha, V.; Garcia, G.G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.-M.; Yang, C.-W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Thomas, B.; Matsushita, K.; Abate, K.H.; Al-Aly, Z.; Ärnlöv, J.; Asayama, K.; Atkins, R.; Badawi, A.; Ballew, S.; Banerjee, A.; et al. Global Cardiovascular and Renal Outcomes of Reduced GFR. J. Am. Soc. Nephrol. 2017, 28, 2167–2179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am. J. Kidney Dis. 1998, 32, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Chronic Kidney Disease Prognosis Consortium. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef] [Green Version]
- Hajhosseiny, R.; Khavandi, K.; Goldsmith, D.J. Cardiovascular disease in chronic kidney disease: Untying the Gordian knot. Int. J. Clin. Pr. 2012, 67, 14–31. [Google Scholar] [CrossRef]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and car-diovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 27, 339–352. [Google Scholar] [CrossRef]
- Fox, C.S.; Matsushita, K.; Woodward, M.; Bilo, H.J.; Chalmers, J.; Heerspink, H.J.L.; Lee, B.J.; Perkins, R.M.; Rossing, P.; Sairenchi, T.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet 2012, 380, 1662–1673. [Google Scholar] [CrossRef] [Green Version]
- Mahmoodi, B.K.; Matsushita, K.; Woodward, M.; Blankestijn, P.J.; Cirillo, M.; Ohkubo, T.; Rossing, P.; Sarnak, M.J.; Stengel, B.; Yamagishi, K.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: A meta-analysis. Lancet 2012, 380, 1649–1661. [Google Scholar] [CrossRef] [Green Version]
- Foley, R.N.; Murray, A.M.; Li, S.; Herzog, C.A.; McBean, A.M.; Eggers, P.W.; Collins, A.J. Chronic Kidney Disease and the Risk for Cardiovascular Disease, Renal Replacement, and Death in the United States Medicare Population, 1998 to 1999. J. Am. Soc. Nephrol. 2004, 16, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Bethesda, M.D.; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. USRDS 2007 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2007. [Google Scholar]
- Wanner, C.; Krane, V.; Marz, W.; Olschewski, M.; Mann, J.F.; Ruf, G.; Ritz, E.; German, D. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N. Engl. J. Med. 2005, 353, 238–248. [Google Scholar] [CrossRef]
- Weiner, D.E.; Tighiouart, H.; Elsayed, E.F.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. The Framingham Predictive Instrument in Chronic Kidney Disease. J. Am. Coll. Cardiol. 2007, 50, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fellström, B.C.; Jardine, A.G.; Schmieder, R.E.; Holdaas, H.; Bannister, K.; Beutler, J.; Chae, D.W.; Chevaile, A.; Cobbe, S.M.; Grönhagen-Riska, C.; et al. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N. Engl. J. Med. 2009, 360, 1395–1407. [Google Scholar] [CrossRef] [Green Version]
- EVOLVE Trial Investigators. Effect of cinacalcet on car-diovascular disease in patients undergoing dialysis. N. Engl. J. Med. 2012, 367, 2482–2494. [Google Scholar] [CrossRef] [Green Version]
- De Zeeuw, D.; Akizawa, T.; Audhya, P.; Bakris, G.L.; Chin, M.; Christ-Schmidt, H.; Goldsberry, A.; Houser, M.; Krauth, M.; Heerspink, H.J.L.; et al. Bardoxolone methyl in type 2 diabetes and stage 4 chronic kidney disease. N. Engl. J. Med. 2013, 369, 2492–2503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, G.M.; Marchais, S.J.; Safar, M.E.; Genest, A.F.; Guerin, A.P.; Metivier, F.; Chedid, K.; London, A.M. Aortic and large artery compliance in end-stage renal failure. Kidney Int. 1990, 37, 137–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blacher, J.; Guerin, A.P.; Pannier, B.; Marchais, S.J.; Safar, M.E.; London, G.M. Impact of Aortic Stiffness on Survival in End-Stage Renal Disease. Circulation 1999, 99, 2434–2439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utescu, M.S.; Couture, V.; Mac-Way, F.; De Serres, S.A.; Marquis, K.; Larivière, R.; Desmeules, S.; Lebel, M.; Boutouyrie, P.; Agharazii, M. Determinants of progression of aortic stiffness in hemodialysis patients: A prospective longitudinal study. Hypertension 2013, 62, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.-C.; Tsai, W.-C.; Chen, J.-Y.; Huang, J.-J. Stepwise increase in arterial stiffness corresponding with the stages of chronic kidney disease. Am. J. Kidney Dis. 2005, 45, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Briet, M.; Bozec, E.; Laurent, S.; Fassot, C.; London, G.; Jacquot, C.; Froissart, M.; Houillier, P.; Boutouyrie, P. Arterial stiffness and enlargement in mild-to-moderate chronic kidney disease. Kidney Int. 2006, 69, 350–357. [Google Scholar] [CrossRef] [Green Version]
- Townsend, R.R.; Anderson, A.H.; Chirinos, J.A.; Feldman, H.I.; Grunwald, J.E.; Nessel, L.; Roy, J.; Weir, M.R.; Wright, J.T., Jr.; Bansal, N.; et al. Association of Pulse Wave Velocity with Chronic Kidney Disease Progression and Mortality. Hypertension 2018, 71, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Townsend, R.R.; Wimmer, N.J.; Chirinos, J.A.; Parsa, A.; Weir, M.; Perumal, K.; Lash, J.P.; Chen, J.; Steigerwalt, S.P.; Flack, J.; et al. Aortic PWV in Chronic Kidney Disease: A CRIC Ancillary Study. Am. J. Hypertens. 2010, 23, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, J.A.; Khan, A.; Bansal, N.; Dries, D.L.; Feldman, H.I.; Ford, V.; Anderson, A.H.; Kallem, R.; Lash, J.P.; Ojo, A.; et al. Arterial Stiffness, Central Pressures, and Incident Hospitalized Heart Failure in the Chronic Renal Insufficiency Cohort Study. Circ. Heart Fail. 2014, 7, 709–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briet, M.; Collin, C.; Karras, A.; Laurent, S.; Bozec, E.; Jacquot, C.; Stengel, B.; Houillier, P.; Froissart, M.; Boutouyrie, P.; et al. Arterial Remodeling Associates with CKD Progression. J. Am. Soc. Nephrol. 2011, 22, 967–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karras, A.; Haymann, J.P.; Bozec, E.; Metzger, M.; Jacquot, C.; Maruani, G.; Houillier, P.; Froissart, M.; Stengel, B.; Guardiola, P.; et al. Large artery stiffening and remodeling are inde-pendently associated with all-cause mortality and cardiovascular events in chronic kidney disease. Hypertension 2012, 60, 1451–1457. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Zhao, X.; Wu, H. Arterial Stiffness: A Focus on Vascular Calcification and Its Link to Bone Mineralization. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1078–1093. [Google Scholar] [CrossRef]
- Moe, S.M. Calcium as a cardiovascular toxin in CKD-MBD. Bone 2016, 100, 94–99. [Google Scholar] [CrossRef]
- Block, G.; Port, F.K. Calcium phosphate metabolism and cardiovascular disease in patients with chronic kidney disease. Semin Dial. 2003, 16, 140–147. [Google Scholar] [CrossRef]
- Raggi, P.; Kleerekoper, M. Contribution of Bone and Mineral Abnormalities to Cardiovascular Disease in Patients with Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 836–843. [Google Scholar] [CrossRef] [Green Version]
- Vanholder, R.; De Smet, R.; Glorieux, G.; Argilés, A.; Baurmeister, U.; Brunet, P.; Clark, W.F.; Cohen, G.M.; De Deyn, P.P.; Deppisch, R.; et al. Review on uremic toxins: Classification, concentration, and interindividual variability. Kidney Int. 2003, 63, 1934–1943. [Google Scholar] [CrossRef] [Green Version]
- Vanholder, R.; Pletinck, A.; Schepers, E.; Glorieux, G.L. Biochemical and Clinical Impact of Organic Uremic Retention Solutes: A Comprehensive Update. Toxins 2018, 10, E33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafi, T.; Hostetter, T.H.; Meyer, T.W.; Hwang, S.; Hai, X.; Melamed, M.L.; Banerjee, T.; Coresh, J.; Powe, N.R. Serum Asymmetric and Symmetric Dimethylarginine and Morbidity and Mortality in Hemodialysis Patients. Am. J. Kidney Dis. 2017, 70, 48–58. [Google Scholar] [CrossRef]
- Xia, X.; Luo, Q.; Li, B.; Lin, Z.; Yu, X.; Huang, F. Serum uric acid and mortality in chronic kidney disease: A systematic review and meta-analysis. Metabolism 2016, 65, 1326–1341. [Google Scholar] [CrossRef] [PubMed]
- Koeth, R.A.; Kalantar-Zadeh, K.; Wang, Z.; Fu, X.; Tang, W.W.; Hazen, S.L. Protein Carbamylation Predicts Mortality in ESRD. J. Am. Soc. Nephrol. 2013, 24, 853–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raikou, V.D.; Tentolouris, N.; Kyriaki, D.; Evaggelatou, A.; Tzanatou, H. ?2-Microglobulin, Pulse Pressure and Metabolic Alterations in Hemodialysis Patients. Nephron Clin. Pr. 2011, 117, c237–c245. [Google Scholar] [CrossRef] [PubMed]
- Kohan, D.E.; Inscho, E.W.; Wesson, D.; Pollock, D.M. Physiology of Endothelin and the Kidney. Compr. Physiol. 2011, 1, 883–919. [Google Scholar] [CrossRef] [Green Version]
- Dhaun, N.; Goddard, J.; Webb, D.J. Endothelin Antagonism in Patients with Nondiabetic Chronic Kidney Disease. Contrib. Nephrol. 2011, 172, 243–254. [Google Scholar] [CrossRef]
- Stinghen, A.; Massy, Z.A.; Vlassara, H.; Striker, G.E.; Boullier, A. Uremic Toxicity of Advanced Glycation End Products in CKD. J. Am. Soc. Nephrol. 2015, 27, 354–370. [Google Scholar] [CrossRef] [Green Version]
- Pawlak, K.; Domaniewski, T.; Mysliwiec, M.; Pawlak, D. The kynurenines are associated with oxidative stress, inflammation and the prevalence of cardiovascular disease in patients with end-stage renal disease. Atherosclerosis 2009, 204, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Cazaña-Pérez, V.; Cidad, P.; Donate-Correa, J.; Martin-Nuñez, E.; Lopez-Lopez, J.R.; Perez-Garcia, M.T.; Giraldez, T.; Navarro-González, J.F.; De La Rosa, D.A. Phenotypic Modulation of Cultured Primary Human Aortic Vascular Smooth Muscle Cells by Uremic Serum. Front. Physiol. 2018, 9, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahabi-Layachi, H.; Ourouda, R.; Boullier, A.; Massy, Z.A.; Amant, C. Distinct Effects of Inorganic Phosphate on Cell Cycle and Apoptosis in Human Vascular Smooth Muscle Cells: Inorganic phosphate et smooth muscle cells. J. Cell. Physiol. 2015, 230, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Maciel, R.A.; Rempel, L.C.; Bosquetti, B.; Finco, A.B.; Pecoits-Filho, R.; Souza, W.M.; Stinghen, A.E. p-cresol but not p-cresyl sulfate stimulate MCP-1 production via NF-κB p65 in human vascular smooth muscle cells. J. Bras. Nefrol. 2016, 38, 153–160. [Google Scholar] [CrossRef]
- Monroy, M.A.; Fang, J.; Li, S.; Ferrer, L.; Birkenbach, M.P.; Lee, I.J.; Wang, H.; Yang, X.F.; Choi, E.T. Chronic kidney disease alters vascular smooth muscle cell phenotype. Front. Biosci. 2015, 20, 784–795. [Google Scholar] [CrossRef] [Green Version]
- Kokubo, T.; Ishikawa, N.; Uchida, H.; Chasnoff, S.E.; Xie, X.; Mathew, S.; Hruska, K.A.; Choi, E.T. CKD Accelerates Development of Neointimal Hyperplasia in Arteriovenous Fistulas. J. Am. Soc. Nephrol. 2009, 20, 1236–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangrez, A.Y.; M’Baya-Moutoula, E.; Meuth, V.M.-L.; Hénaut, L.; Djelouat, M.S.E.I.; Benchitrit, J.; Massy, Z.A.; Metzinger, L. Inorganic Phosphate Accelerates the Migration of Vascular Smooth Muscle Cells: Evidence for the Involvement of miR. PLoS ONE 2012, 7, e47807. [Google Scholar] [CrossRef]
- Yamamoto, H.; Tsuruoka, S.; Ioka, T.; Ando, H.; Ito, C.; Akimoto, T.; Fujimura, A.; Asano, Y.; Kusano, E. Indoxyl sulfate stimulates proliferation of rat vascular smooth muscle cells. Kidney Int. 2006, 69, 1780–1785. [Google Scholar] [CrossRef] [Green Version]
- Muteliefu, G.; Enomoto, A.; Niwa, T. Indoxyl Sulfate Promotes Proliferation of Human Aortic Smooth Muscle Cells by Inducing Oxidative Stress. J. Ren. Nutr. 2009, 19, 29–32. [Google Scholar] [CrossRef]
- Mozar, A.; Louvet, L.; Morlière, P.; Godin, C.; Boudot, C.; Kamel, S.; Drüeke, T.B.; Massy, Z.A. Uremic Toxin Indoxyl Sulfate Inhibits Human Vascular Smooth Muscle Cell Proliferation. Ther. Apher. Dial. 2011, 15, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Chen, Y.; Zhu, Z.; Su, X.; Ni, J.; Du, R.; Zhang, R.; Jin, W. p-Cresyl sulfate promotes the formation of atherosclerotic lesions and induces plaque instability by targeting vascular smooth muscle cells. Front. Med. 2016, 10, 320–329. [Google Scholar] [CrossRef]
- Shimizu, H.; Hirose, Y.; Goto, S.; Nishijima, F.; Zrelli, H.; Zghonda, N.; Niwa, T.; Miyazaki, H. Indoxyl sulfate enhances angiotensin II signaling through upregulation of epidermal growth factor receptor expression in vascular smooth muscle cells. Life Sci. 2012, 91, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Takemura, A.; Iijima, K.; Ota, H.; Son, B.-K.; Ito, Y.; Ogawa, S.; Eto, M.; Akishita, M.; Ouchi, Y. Sirtuin 1 Retards Hyperphosphatemia-Induced Calcification of Vascular Smooth Muscle Cells. Arter. Thromb. Vasc. Biol. 2011, 31, 2054–2062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troyano, N.; Del Nogal, M.; Mora, I.; Diaz-Naves, M.; Lopez-Carrillo, N.; Sosa, P.; Rodriguez-Puyol, D.; Olmos, G.; Ruiz-Torres, M.P. Hyperphosphatemia induces cellular senescence in human aorta smooth muscle cells through integrin linked kinase (ILK) up-regulation. Mech. Ageing Dev. 2015, 152, 43–55. [Google Scholar] [CrossRef]
- Muteliefu, G.; Shimizu, H.; Enomoto, A.; Nishijima, F.; Takahashi, M.; Niwa, T. Indoxyl sulfate promotes vascular smooth muscle cell senescence with upregulation of p53, p21, and prelamin A through oxidative stress. Am. J. Physiol. Physiol. 2012, 303, C126–C134. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Jiang, H.; Gao, F.; Liang, S.; Wei, M.; Chen, L. Indoxyl sulfate-induced calcification of vascular smooth muscle cells via the PI3K/Akt/NF-κB signaling pathway. Microsc. Res. Tech. 2019, 82, 2000–2006. [Google Scholar] [CrossRef]
- Gillery, P.; Jaisson, S. Post-translational modification derived products (PTMDPs): Toxins in chronic diseases? Clin. Chem. Lab. Med. 2014, 52, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Apostolov, E.O.; Ray, D.; Savenka, A.V.; Shah, S.V.; Basnakian, A.G. Chronic uremia stimulates LDL carbamylation and atheroscle-rosis. J. Am. Soc. Nephrol. 2010, 21, 1852–1857. [Google Scholar] [CrossRef] [Green Version]
- El-Gamal, D.; Rao, S.P.; Holzer, M.; Hallström, S.; Haybaeck, J.; Gauster, M.; Wadsack, C.; Kozina, A.; Frank, S.; Schicho, R.; et al. The urea decomposition product cyanate promotes endothelial dysfunction. Kidney Int. 2014, 86, 923–931. [Google Scholar] [CrossRef] [Green Version]
- Desmons, A.; Okwieka, A.; Doué, M.; Gorisse, L.; Vuiblet, V.; Pietrement, C.; Gillery, P.; Jaisson, S. Proteasome-dependent degradation of intracellular carbamylated proteins. Aging 2019, 11, 3624–3638. [Google Scholar] [CrossRef] [PubMed]
- Hocine, A.; Belmokhtar, K.; Bauley, K.; Jaisson, S.; Gaha, K.; Oubaya, N.; Lesaffre, F.; Lavaud, S.; Halin, P.; Gillery, P.; et al. Serum and Tissue Accumulation of Advanced Glycation End-Products Correlates with Vascular Changes. Perit. Dial. Int. 2015, 35, 592–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, H.; Koyama, H.; Tanaka, S.; Fukumoto, S.; Shinohara, K.; Shoji, T.; Emoto, M.; Tahara, H.; Kakiya, R.; Tabata, T.; et al. Skin autofluorescence, a marker for advanced glycation end product accumulation, is associated with arterial stiffness in patients with end-stage renal disease. Metabolism 2008, 57, 1452–1457. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Yu, Z.; Jia, H.; Sun, F.; Ma, L.; Guo, R.; Peng, L.; Cui, T. Association of Serum Pentosidine With Arterial Stiffness in Hemodialysis Patients. Artif. Organs 2010, 34, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Satoh, H.; Togo, M.; Hara, M.; Miyata, T.; Han, K.; Maekawa, H.; Ohno, M.; Hashimoto, Y.; Kurokawa, K.; Watanabe, T. Advanced Glycation Endproducts Stimulate Mitogen-Activated Protein Kinase and Proliferation in Rabbit Vascular Smooth Muscle Cells. Biochem. Biophys. Res. Commun. 1997, 239, 111–115. [Google Scholar] [CrossRef]
- Xiang, M.; Yang, R.; Zhang, Y.; Wu, P.; Wang, L.; Gao, Z.; Wang, J. Effect of crocetin on vascular smooth muscle cells migration induced by advanced glycosylation end products. Microvasc. Res. 2017, 112, 30–36. [Google Scholar] [CrossRef]
- Koike, S.; Yano, S.; Tanaka, S.; Sheikh, A.M.; Nagai, A.; Sugimoto, T. Advanced Glycation End-Products Induce Apoptosis of Vascular Smooth Muscle Cells: A Mechanism for Vascular Calcification. Int. J. Mol. Sci. 2016, 17, 1567. [Google Scholar] [CrossRef] [Green Version]
- Aronson, D. Cross-linking of glycated collagen in the pathogenesis of arterial and myocardial stiffening of aging and diabetes. J. Hypertens. 2003, 21, 3–12. [Google Scholar] [CrossRef]
- Barreto, D.V.; Barreto, F.C.; Liabeuf, S.; Temmar, M.; Lemke, H.D.; Tribouilloy, C.; Choukroun, G.; Vanholder, R.; Massy, Z.A. Plasma interleukin-6 is independently associ-ated with mortality in both hemodialysis and pre-dialysis patients with chronic kidney disease. Kidney Int. 2010, 77, 550–556. [Google Scholar] [CrossRef]
- Lee, J.-W.; Cho, E.; Kim, M.-G.; Jo, S.-K.; Cho, W.Y.; Kim, H.K. Proinflammatory CD14(+)CD16(+) monocytes are associated with vas-cular stiffness in predialysis patients with chronic kidney disease. Kidney Res. Clin. Pract. 2013, 32, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Kataoka, H.; Murakami, R.; Numaguchi, Y.; Okumura, K.; Murohara, T. Angiotensin II type 1 receptor blockers prevent tumor necrosis factor-α-mediated endothelial nitric oxide synthase reduction and superoxide production in human umbilical vein endothelial cells. Eur. J. Pharmacol. 2010, 636, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Zanoli, L.; Lentini, P.; Briet, M.; Castellino, P.; House, A.A.; London, G.M.; Malatino, L.; McCullough, P.A.; Mikhailidis, D.P.; Boutouyrie, P. Arterial Stiffness in the Heart Disease of CKD. J. Am. Soc. Nephrol. 2019, 30, 918–928. [Google Scholar] [CrossRef]
- Desjardins, M.-P.; Sidibé, A.; Fortier, C.; Mac-Way, F.; Marquis, K.; De Serres, S.; Larivière, R.; Agharazii, M. Association of interleukin-6 with aortic stiffness in end-stage renal disease. J. Am. Soc. Hypertens. 2018, 12, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Krzanowski, M.; Janda, K.; Dumnicka, P.; Dubiel, M.; Stompór, M.; Kuśnierz-Cabala, B.; Grodzicki, T.; Sułowicz, W. Relationship between aortic pulse wave velocity, selected proinflammatory cytokines, and vascular calcification parameters in peritoneal dialysis patients. J. Hypertens. 2014, 32, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Gravos, A.; Georgiopoulos, G.; Terentes-Printzios, D.; Ioakeimidis, N.; Vassilopoulos, D.; Stamatelopoulos, K.; Tousoulis, D. The effect of TNF-a antagonists on aortic stiffness and wave reflections: A meta-analysis. Clin. Rheumatol. 2017, 37, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Klimczak-Tomaniak, D.; Pilecki, T.; Żochowska, D.; Sieńko, D.; Janiszewski, M.; Pączek, L.; Kuch, M. CXCL12 in Patients with Chronic Kidney Disease and Healthy Controls: Relationships to Ambulatory 24-Hour Blood Pressure and Echocardiographic Measures. Cardiorenal Med. 2018, 8, 249–258. [Google Scholar] [CrossRef]
- Mehta, N.N.; Matthews, G.J.; Krishnamoorthy, P.; Shah, R.; McLaughlin, C.; Patel, P.; Budoff, M.; Chen, J.; Wolman, M.; Go, A.; et al. Higher plasma CXCL12 levels predict incident myocardial infarction and death in chronic kidney disease: Findings from the Chronic Renal Insufficiency Cohort study. Eur. Hear. J. 2014, 35, 2115–2122. [Google Scholar] [CrossRef] [Green Version]
- Pan, C.-H.; Chen, C.-W.; Sheu, M.-J.; Wu, C.-H. Salvianolic acid B inhibits SDF-1α-stimulated cell proliferation and migration of vascular smooth muscle cells by suppressing CXCR4 receptor. Vasc. Pharmacol. 2012, 56, 98–105. [Google Scholar] [CrossRef]
- Strowig, T.; Henao-Mejia, J.; Elinav, E.; Flavell, R.A. Inflammasomes in health and disease. Nature 2012, 481, 278–286. [Google Scholar] [CrossRef]
- Kimmel, P.L.; Phillips, T.M.; Simmens, S.J.; Peterson, R.A.; Weihs, K.L.; Alleyne, S.; Cruz, I.; Yanovski, J.A.; Veis, J.H. Immunologic function and survival in hemo-dialysis patients. Kidney Int. 1998, 54, 236–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Descamps-Latscha, B.; Herbelin, A.; Nguyen, A.T.; Roux-Lombard, P.; Zingraff, J.; Moynot, A.; Verger, C.; Dahmane, D.; De Groote, D.; Jungers, P. Balance between IL-1 beta, TNF-alpha, and their specific inhibitors in chronic renal failure and maintenance dialysis. Relationships with activation markers of T cells, B cells, and monocytes. J. Immunol. 1995, 154, 882–892. [Google Scholar] [PubMed]
- Ren, X.-S.; Tong, Y.; Ling, L.; Chen, D.; Sun, H.-J.; Zhou, H.; Qi, X.-H.; Chen, Q.; Li, Y.-H.; Kang, Y.-M.; et al. NLRP3 Gene Deletion Attenuates Angiotensin II-Induced Phenotypic Transformation of Vascular Smooth Muscle Cells and Vascular Remodeling. Cell. Physiol. Biochem. 2017, 44, 2269–2280. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.-J.; Ren, X.-S.; Xiong, X.-Q.; Chen, Y.-Z.; Zhao, M.-X.; Wang, J.-J.; Zhou, Y.-B.; Han, Y.; Chen, Q.; Li, Y.-H.; et al. NLRP3 inflammasome activation contributes to VSMC phenotypic transformation and proliferation in hypertension. Cell Death Dis. 2017, 8, e3074. [Google Scholar] [CrossRef] [Green Version]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised pla-cebo-controlled trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef] [Green Version]
- Gregg, L.P.; Hedayati, S.S. Management of Traditional Cardiovascular Risk Factors in CKD: What Are the Data? Am. J. Kidney Dis. 2018, 72, 728–744. [Google Scholar] [CrossRef] [PubMed]
- Nowak, K.L.; Chonchol, M.; Ikizler, T.; Farmer-Bailey, H.; Salas, N.; Chaudhry, R.; Wang, W.; Smits, G.; Tengesdal, I.; Dinarello, C.A.; et al. IL-1 Inhibition and Vascular Function in CKD. J. Am. Soc. Nephrol. 2016, 28, 971–980. [Google Scholar] [CrossRef] [Green Version]
- Hung, A.M.; Ellis, C.D.; Shintani, A.; Booker, C.; Ikizler, T.A. IL-1β Receptor Antagonist Reduces Inflammation in Hemodialysis Patients. J. Am. Soc. Nephrol. 2011, 22, 437–442. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Uraemic Serum | Phosphate | Indoxyl Sulphate Acute Exposure Chronic Exposure | P-Cresyl Sulphate | ||
|---|---|---|---|---|---|
| Viability Primary HASMC | Decrease [45] | Decrease [46] | No effect [47] | ||
| Proliferation Primary HASMC Others | Slight decrease [45] or increase [48] Increase/aortic explants [49] | Decrease [46,50] | Increase [51,52] | Decrease [53] | Increase [54]/rat aortic VSMC |
| Apoptosis Primary HASMC | Increase [45] or no effect [48] | Increase [46] | Not evaluated | Not evaluated | |
| Migration Primary HASMC Others | Decrease [45,48] Increase [49]/aortic explants | Acceleration [50] | Increase [55] | Increase [54] | |
| Senescence Primary HASMC | Needs to be clarified | Increase [46,56,57]/cell cycle arrest | Promotion [58] | Not evaluated | |
| Study Start | Study Title | Population Studied | Drugs and Procedures | Phase | Locations | NCT # |
|---|---|---|---|---|---|---|
| March 2020 | Oral Absorbent and Probiotics in CKD Patients With PAD on Gut Microbiota, IncRNA, Metabolome, and Vascular Function | CKD all stages | Dietary supplement | NA | Taiwan | 04792320 |
| November 2019 | Nicotinamide Riboside Supplementation for Treating Arterial Stiffness and Elevated Systolic Blood Pressure in Patients with Moderate to Severe CKD | CKD stage 3 to 4 | Drug: nicotinamide riboside Primary outcome: change in aortic stiffness (carotid–femoral PWV) Follow-up: 3 months | Phase 2 | Denver, CO, USA | 04040959 |
| December 2018 | HCQ for the CVD in CKD | CKD stage 3B, 4 | Drug: hydroxychloroquine Outcomes:
| Phase 2 | Gainesville, FL, USA | 03636152 |
| April 2018 | Phase 2b Study of KBP-5074 in Subjects with Uncontrolled Hypertension and Advanced Chronic Kidney Disease | CKD stage 3B, 4, uncontrolled hypertension | Drug: KBP-5074 (mineralocorticoid receptor antagonist) Outcome: systolic blood pressure Follow-up: 84 days | Phase 2 | Princeton, NJ, USA Morrisville, NC, USA | 03574363 |
| September 2017 | Vitamin K to Slow Progression of Cardiovascular Disease Risk in Haemodialysis Patients | Stages 3, 4 and 5 of CKD | Drug: menaquinone-7 Outcomes:
| NA | Augusta, GA, USA | 03311321 |
| July 2017 | Effectiveness and Tolerability of Long-Acting Nifedipine Gastrointestinal Therapeutic System in Chronic Kidney Disease with Uncontrolled Hypertension Patients, a Prospective, Multicentre, Observational Study | CKD, uncontrolled hypertension | Drug: nifedipine controlled-release tablets (Adalat, BAYA1040) Outcome: systolic blood pressure Follow-up: 12 weeks | NA | Multiple locations, China | 03194633 |
| April 2017 | Study Comparing Treatment Effectiveness of Guideline Indicated APT for ACS in Patients with CKD | CKD, acute coronary syndrome | Drug: ticagrelor Drug: clopidogrel Outcome: occurrence of all-cause mortality, non-fatal myocardial infarction, stroke | Phase 4 | Durham, NC, USA Dallas, TX, USA | 03150667 |
| October 2014 | Metformin in Kidney Disease | CKD stage 3 overweight or obese, normal if pre-diabetic or insulin resistant | Drug: metformin Outcome: leptin to adiponectin ratio (an atherosclerotic index) Follow-up: 16 weeks | Phase 2 | Nashville, TN, USA | 02252081 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foudi, N.; Palayer, M.; Briet, M.; Garnier, A.-S. Arterial Remodelling in Chronic Kidney Disease: Impact of Uraemic Toxins and New Pharmacological Approaches. J. Clin. Med. 2021, 10, 3803. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10173803
Foudi N, Palayer M, Briet M, Garnier A-S. Arterial Remodelling in Chronic Kidney Disease: Impact of Uraemic Toxins and New Pharmacological Approaches. Journal of Clinical Medicine. 2021; 10(17):3803. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10173803
Chicago/Turabian StyleFoudi, Nabil, Maeva Palayer, Marie Briet, and Anne-Sophie Garnier. 2021. "Arterial Remodelling in Chronic Kidney Disease: Impact of Uraemic Toxins and New Pharmacological Approaches" Journal of Clinical Medicine 10, no. 17: 3803. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10173803