
The Beneficial Effects of Eccentric Exercise in the Management of Lateral Elbow Tendinopathy: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
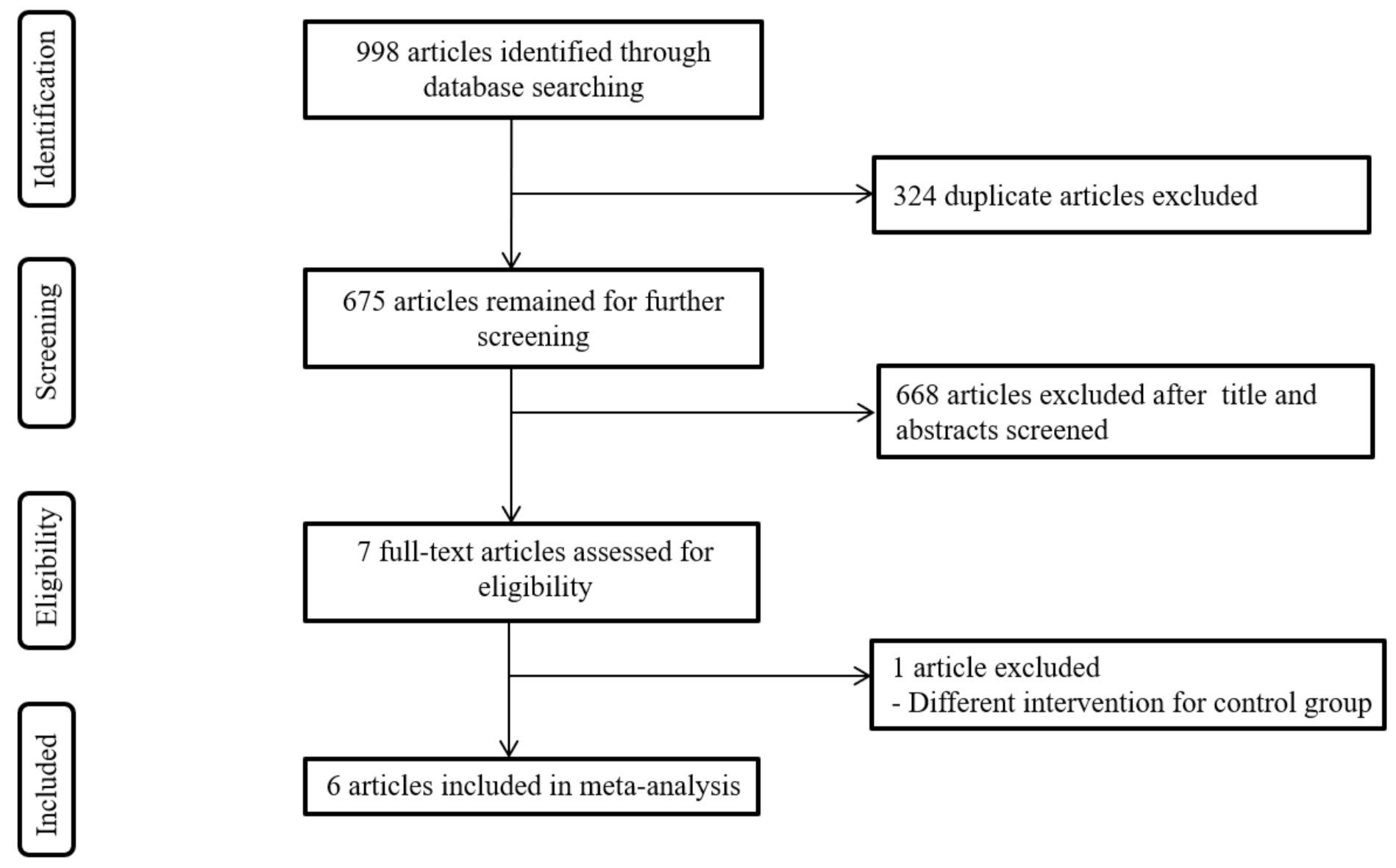
2.1. Search Strategy and Study Selection
2.2. Data Extraction and Quality Assessment
2.3. Data Synthesis and Statistical Analysis
3. Results
3.1. Description of the Selected Studies
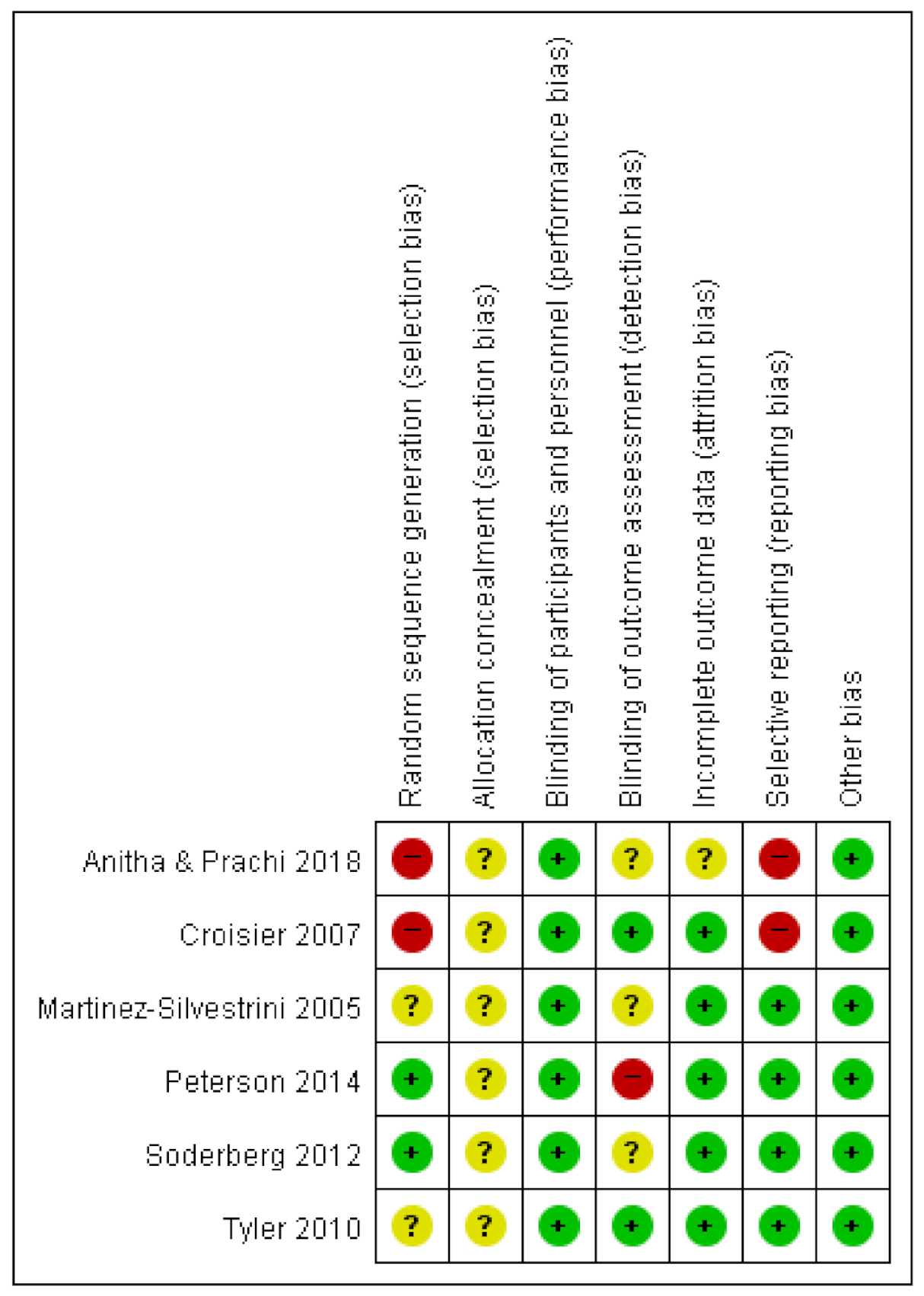
3.2. Risk of Bias
3.3. Study Characteristics
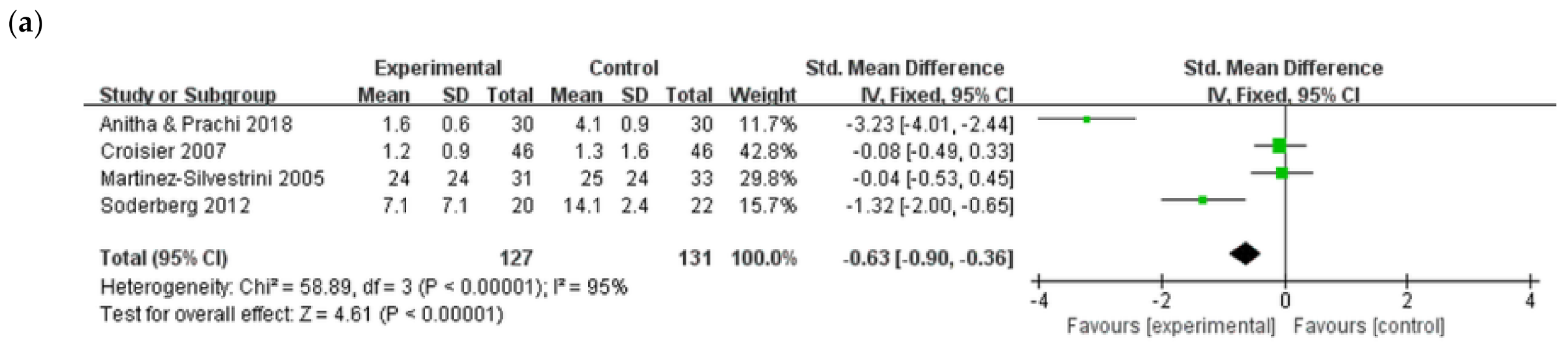
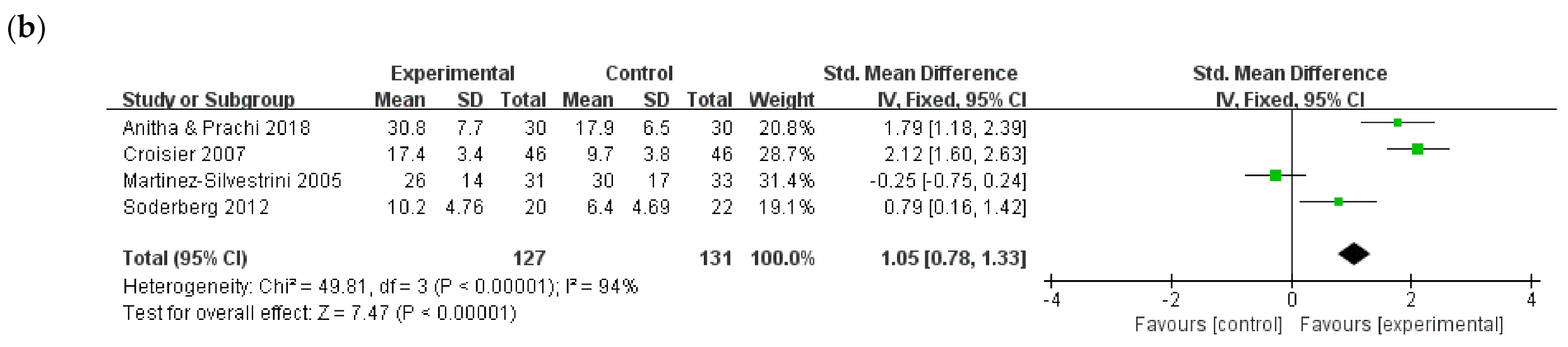
3.4. Add-on Effects of Eccentric Exercise with Adjuvant Therapy for LET
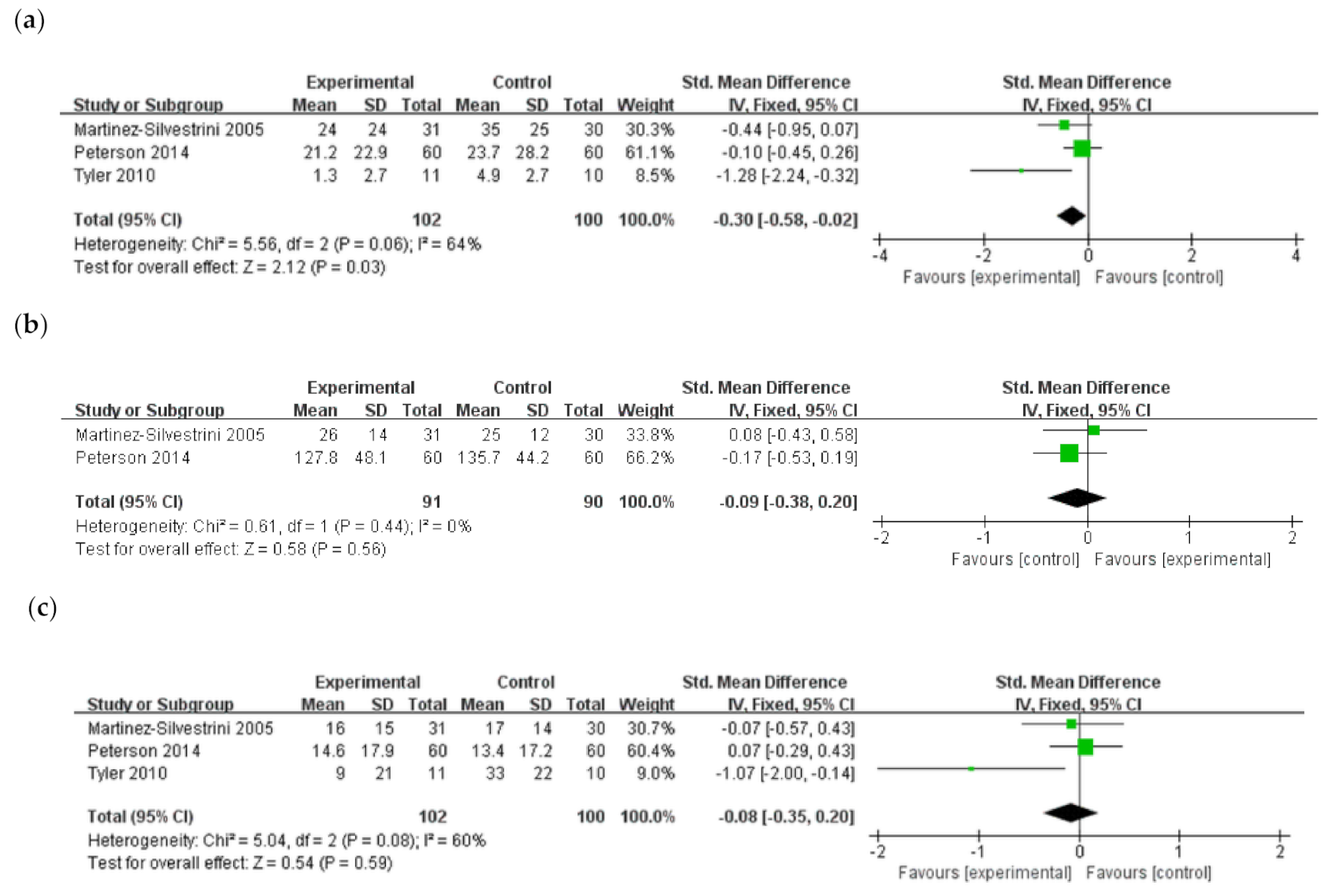
3.5. Comparison between Eccentric Exercise and Other Exercises (Concentric or Isotonic) in LET
3.6. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stasinopoulos, D.; Stasinopoulos, I. Comparison of effects of eccentric training, eccentric-concentric training, and eccentric-concentric training combined with isometric contraction in the treatment of lateral elbow tendinopathy. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 2017, 30, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Bisset, L.M.; Vicenzino, B. Physiotherapy management of lateral epicondylalgia. J. Physiother. 2015, 61, 174–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coombes, B.K.; Bisset, L.; Vicenzino, B. Management of lateral elbow tendinopathy: One size does not fit all. J. Orthop. Sports Phys. Ther. 2015, 45, 938–949. [Google Scholar] [CrossRef] [Green Version]
- Kraushaar, B.S.; Nirschl, R.P. Tendinosis of the elbow (tennis elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J. Bone Jt. Surg. Am. Vol. 1999, 81, 259–278. [Google Scholar] [CrossRef]
- Waugh, E.J.; Jaglal, S.B.; Davis, A.M.; Tomlinson, G.; Verrier, M.C. Factors associated with prognosis of lateral epicondylitis after 8 weeks of physical therapy. Arch. Phys. Med. Rehabil. 2004, 85, 308–318. [Google Scholar] [CrossRef]
- Ritz, B.R. Humeral epicondylitis among gas- and waterworks employees. Scand. J. Work Environ. Health 1995, 21, 478–486. [Google Scholar] [CrossRef]
- Babaei-Ghazani, A.; Shahrami, B.; Fallah, E.; Ahadi, T.; Forough, B.; Ebadi, S. Continuous shortwave diathermy with exercise reduces pain and improves function in lateral epicondylitis more than sham diathermy: A randomized controlled trial. J. Bodyw. Mov. Ther. 2020, 24, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, P.W.; Renstrom, P. Tendinopathy in sport. Sports Health 2012, 4, 193–201. [Google Scholar] [CrossRef]
- Murtaugh, B.; Ihm, J.M. Eccentric training for the treatment of tendinopathies. Curr. Sports Med. Rep. 2013, 12, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Kaux, J.F.; Forthomme, B.; Goff, C.L.; Crielaard, J.M.; Croisier, J.L. Current opinions on tendinopathy. J. Sports Sci. Med. 2011, 10, 238–253. [Google Scholar]
- Orchard, J.; Kountouris, A. The management of tennis elbow. Br. Med. J. (Clin. Res. Ed.) 2011, 342, d2687. [Google Scholar] [CrossRef] [Green Version]
- Maffulli, N.; Longo, U.G.; Denaro, V. Novel approaches for the management of tendinopathy. J. Bone Jt. Surg. Am. Vol. 2010, 92, 2604–2613. [Google Scholar] [CrossRef]
- O’Neill, S.; Watson, P.J.; Barry, S. Why are eccentric exercises effective for Achilles’ tendinopathy? Int. J. Sports Phys. Ther. 2015, 10, 552–562. [Google Scholar]
- Alfredson, H.; Pietila, T.; Jonsson, P.; Lorentzon, R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am. J. Sports Med. 1998, 26, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Stanish, W.D.; Rubinovich, R.M.; Curwin, S. Eccentric exercise in chronic tendinitis. Clin. Orthop. Relat. Res. 1986, 208, 65–68. [Google Scholar] [CrossRef]
- Ohberg, L.; Alfredson, H. Effects on neovascularisation behind the good results with eccentric training in chronic mid-portion Achilles tendinosis? Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2004, 12, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Divani, K.; Chan, O.; Padhiar, N.; Twycross-Lewis, R.; Maffulli, N.; Crisp, T.; Morrissey, D. Site of maximum neovascularisation correlates with the site of pain in recalcitrant mid-tendon Achilles tendinopathy. Man. Ther. 2010, 15, 463–468. [Google Scholar] [CrossRef]
- van Snellenberg, W.; Wiley, J.P.; Brunet, G. Achilles tendon pain intensity and level of neovascularization in athletes as determined by color Doppler ultrasound. Scand. J. Med. Sci. Sports 2007, 17, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Danielson, P. Reviving the “biochemical” hypothesis for tendinopathy: New findings suggest the involvement of locally produced signal substances. Br. J. Sports Med. 2009, 43, 265–268. [Google Scholar] [CrossRef]
- Scott, A.; Docking, S.; Vicenzino, B.; Alfredson, H.; Murphy, R.J.; Carr, A.J.; Zwerver, J.; Lundgreen, K.; Finlay, O.; Pollock, N.; et al. Sports and exercise-related tendinopathies: A review of selected topical issues by participants of the second International Scientific Tendinopathy Symposium (ISTS) Vancouver 2012. Br. J. Sports Med. 2013, 47, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Rees, J.D.; Wolman, R.L.; Wilson, A. Eccentric exercises; why do they work, what are the problems and how can we improve them? Br. J. Sports Med. 2009, 43, 242–246. [Google Scholar] [CrossRef]
- Rees, J.D.; Lichtwark, G.A.; Wolman, R.L.; Wilson, A.M. The mechanism for efficacy of eccentric loading in Achilles tendon injury; an in vivo study in humans. Rheumatology 2008, 47, 1493–1497. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, M.; Aaboe, J.; Bliddal, H.; Langberg, H. Biomechanical characteristics of the eccentric Achilles tendon exercise. J. Biomech. 2009, 42, 2702–2707. [Google Scholar] [CrossRef]
- Grigg, N.L.; Wearing, S.C.; O’Toole, J.M.; Smeathers, J.E. The effect of exercise repetition on the frequency characteristics of motor output force: Implications for Achilles tendinopathy rehabilitation. J. Sci. Med. Sport 2014, 17, 13–17. [Google Scholar] [CrossRef]
- Cullinane, F.L.; Boocock, M.G.; Trevelyan, F.C. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clin. Rehabil. 2014, 28, 3–19. [Google Scholar] [CrossRef]
- Malliaras, P.; Maffulli, N.; Garau, G. Eccentric training programmes in the management of lateral elbow tendinopathy. Disabil. Rehabil. 2008, 30, 1590–1596. [Google Scholar] [CrossRef]
- Wen, D.Y.; Schultz, B.J.; Schaal, B.; Graham, S.T.; Kim, B.S. Eccentric strengthening for chronic lateral epicondylosis: A prospective randomized study. Sports Health 2011, 3, 500–503. [Google Scholar] [CrossRef] [Green Version]
- Nagrale, A.V.; Herd, C.R.; Ganvir, S.; Ramteke, G. Cyriax physiotherapy versus phonophoresis with supervised exercise in subjects with lateral epicondylalgia: A randomized clinical trial. J. Man. Manip. Ther. 2009, 17, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Stasinopoulos, D.; Stasinopoulos, I. Comparison of effects of Cyriax physiotherapy, a supervised exercise programme and polarized polychromatic non-coherent light (Bioptron light) for the treatment of lateral epicondylitis. Clin. Rehabil. 2006, 20, 12–23. [Google Scholar] [CrossRef]
- Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1. 0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews ansd Meta-Analyses: The PRISMA statement. Br. Med. J. (Clin. Res. Ed.) 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Huedo-Medina, T.B.; Sanchez-Meca, J.; Marin-Martinez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anitha, A.; Prachi, G. Effectiveness of eccentric strengthening of wrist extensors along with conventional therapy in patients with lateral epicondylitis. Res. J. Pharm. Technol. 2018, 11, 5340. [Google Scholar] [CrossRef]
- Croisier, J.L.; Foidart-Dessalle, M.; Tinant, F.; Crielaard, J.M.; Forthomme, B. An isokinetic eccentric programme for the management of chronic lateral epicondylar tendinopathy. Br. J. Sports Med. 2007, 41, 269–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Silvestrini, J.A.; Newcomer, K.L.; Gay, R.E.; Schaefer, M.P.; Kortebein, P.; Arendt, K.W. Chronic lateral epicondylitis: Comparative effectiveness of a home exercise program including stretching alone versus stretching supplemented with eccentric or concentric strengthening. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 2005, 18, 411–419. [Google Scholar] [CrossRef]
- Peterson, M.; Butler, S.; Eriksson, M.; Svardsudd, K. A randomized controlled trial of eccentric vs. concentric graded exercise in chronic tennis elbow (lateral elbow tendinopathy). Clin. Rehabil. 2014, 28, 862–872. [Google Scholar] [CrossRef]
- Soderberg, J.; Grooten, W.J.; Ang, B.O. Effects of eccentric training on hand strength in subjects with lateral epicondylalgia: A randomized-controlled trial. Scand. J. Med. Sci. Sports 2012, 22, 797–803. [Google Scholar] [CrossRef]
- Tyler, T.F.; Thomas, G.C.; Nicholas, S.J.; McHugh, M.P. Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis: A prospective randomized trial. J. Shoulder Elb. Surg. 2010, 19, 917–922. [Google Scholar] [CrossRef]
- Mafi, N.; Lorentzon, R.; Alfredson, H. Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2001, 9, 42–47. [Google Scholar] [CrossRef]
- Holmgren, T.; Bjornsson Hallgren, H.; Oberg, B.; Adolfsson, L.; Johansson, K. Effect of specific exercise strategy on need for surgery in patients with subacromial impingement syndrome: Randomised controlled study. Br. Med. J. (Clin. Res. Ed.) 2012, 344, e787. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants (E/C) | Eccentric Exercise Group | Comparison Group | Outcome Measures | |
|---|---|---|---|---|
| Eccentric exercise + adjuvant treatment vs. adjuvant treatment | ||||
| Anitha and Prachi (2018) [36] | N = 30/30 Age (y), NR/NR Sex (M/F), NR/NR Duration (mo), NR/NR | Eccentric exercise + Standardized conventional therapy Device: Rubber bar 3 sets of 15 repetitions 6 session/week Duration, 2 weeks | Standardized conventional therapy (pulsed ultrasonic therapy) | Pain: Numerical pain rating scale (0–10) Grip strength (maximum) |
| Croisier et al. (2007) [37] | N = 46/46 Age (y), 40 (SD, 8)/38 (SD, 8) Sex (M/F), 36/56 Duration (mo), 8 (SD, 4)/8 (SD, 3) | Isokinetic eccentric exercise + Non-strengthening rehabilitation Device: Cybex Norrn dynamometer 2 sets of 10 repetitions for wrist extensors and forearm supinators 3 times/week Duration, 9 weeks | Non-strengthening rehabilitation (e.g., ultrasound, analgesic TENS, ice, deep friction massage, and stretching) | Pain: VAS score (0–10) Eccentric muscle strength Disability questionnaire |
| Martinez-Silvestrini et al. (2005) [38] | N = 31/33 Age (y), 46.6 (SD, NR)/43.1 (SD, NR) Sex (M/F), NR/NR Duration (mo), NR/NR | Eccentric exercise + Self-applied ice massage and stretching of wrist extensors Device: Elastic resistance band 3 sets of 10 repetitions Daily Duration, 6 weeks | Self-applied ice massage and stretching of wrist extensors | Pain: VAS score (0–100) Grip strength (pain-free) DASH PRFEQ SF-36 |
| Soderberg et al. (2012) [40] | N = 20/22 Age (y), 48 (SD, 12.4)/50 (SD, 10.8) Sex (M/F), 24/18 Duration (mo), NR/NR | Eccentric exercise + Forearm band and warm-up exercise Device: Bucket 2→3 sets of 8–12 repetitions Daily → Twice a day Duration, 6 weeks | Forearm band and warm-up exercise for wrist extensors (flexion, extension, abduction, adduction and circumduction for 1 min twice a day) | Pain: VAS score (0–100) Grip strength (pain-free) |
| Eccentric exercise vs. Other exercises (concentric or isotonic) | ||||
| Martinez-Silvestrini et al. (2005) [38] | N = 31/30 Age (y), 46.6 (SD, NR)/47.0 (SD, NR) Sex (M/F), NR/NR Duration (mo), NR/NR | Eccentric exercise + Self-applied ice massage and stretching of wrist extensors Device: Elastic resistance band 3 sets of 10 repetitions Daily Duration, 6 weeks | Concentric exercise + Self-applied ice massage and stretching of wrist extensors Same protocol with eccentric exercise | Pain: VAS score (0–100) Grip strength (pain-free) DASH PRFEQ SF-36 results |
| Peterson et al. (2014) [39] | N = 60/60 Age (y), 48.8 (SD, 6.7)/47.0 (SD, 9.4) Sex (M/F), 63/57 Duration (mo), NR/NR | Eccentric exercise Device: Dumbbell (using a specified amount of water in a plastic container) 3 sets of 15 repetitions DailyDuration, 3 months | Concentric exercise Same protocol with eccentric exercise | Pain: VAS score (0–100) Forearm extensor muscles strength DASH Gothenburg Quality of Life instrument questionnaire |
| Tyler et al. (2010) [41] | N = 11/10 Age (y), 47 (SD, 2)/51 (SD, 4) Sex (M/F), 10/11 Duration (wk), 6 (SD, 2)/8 (SD, 3) | Eccentric exercise + Wrist extensor stretching, ultrasound, cross-friction massage, heat, and ice Device: Rubber bar 3 sets of 15 repetitions Daily Duration, 7 weeks | Isotonic exercise + Wrist extensor stretching, ultrasound, cross-friction massage, heat, and ice | Pain: VAS score (0–10) DASH |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, S.Y.; Kim, Y.W.; Shin, I.S.; Kang, S.; Moon, H.I.; Lee, S.C. The Beneficial Effects of Eccentric Exercise in the Management of Lateral Elbow Tendinopathy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3968. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10173968
Yoon SY, Kim YW, Shin IS, Kang S, Moon HI, Lee SC. The Beneficial Effects of Eccentric Exercise in the Management of Lateral Elbow Tendinopathy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(17):3968. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10173968
Chicago/Turabian StyleYoon, Seo Yeon, Yong Wook Kim, In Soo Shin, Seok Kang, Hyun Im Moon, and Sang Chul Lee. 2021. "The Beneficial Effects of Eccentric Exercise in the Management of Lateral Elbow Tendinopathy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 17: 3968. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10173968