
The Aggregate Index of Systemic Inflammation (AISI): A Novel Prognostic Biomarker in Idiopathic Pulmonary Fibrosis

 , , ,
, , ,  , , , , and
, , , , and
Abstract
:1. Background
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. ATS/ERS/JRS/ALAT Committee on Idiopathic Pulmonary Fibrosis. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed]
- King, T.E., Jr.; Pardo, A.; Selman, M. Idiopathic pulmonary fibrosis. Lancet 2011, 378, 1949–1961. [Google Scholar] [CrossRef]
- Khalil, W.; Xia, H.; Bodempudi, V.; Kahm, J.; Hergert, P.; Smith, K.; Peterson, M.; Parker, M.; Herrera, J.; Bitterman, P.B.; et al. Pathologic Regulation of Collagen I by an Aberrant Protein Phos-phatase 2A/Histone Deacetylase C4/MicroRNA-29 Signal Axis in Idiopathic Pulmonary Fibrosis Fibroblasts. Am. J. Respir. Cell. Mol. Biol. 2015, 53, 391–399. [Google Scholar] [CrossRef]
- De Vries, J.; Kessels, B.L.J.; Drent, M. Quality of life of idiopathic pulmonary fibrosis patients. Eur. Respir. J. 2001, 17, 954–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomioka, H.; Imanaka, K.; Hashimoto, K.; Iwasaki, H. Health-related Quality of Life in Patients with Idiopathic Pulmonary Fibrosis -Cross-sectional and Longitudinal Study. Intern. Med. 2007, 46, 1533–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, T.E., Jr.; Tooze, J.A.; Schwarz, M.I.; Brown, K.R.; Cherniack, R.M. Predicting survival in id-iopathic pulmonary fibrosis: Scoring system and survival model. Am. J. Respir. Crit. Care. Med. 2001, 164, 1171–1181. [Google Scholar] [CrossRef]
- Wells, A.U.; Desai, S.R.; Rubens, M.B.; Goh, N.S.; Cramer, D.; Nicholson, A.G.; Colby, T.V.; du Bois, R.M.; Hansell, D.M. Idiopathic pulmonary fibrosis: A composite physiologic index derived from disease extent observed by computed tomography. Am. J. Respir. Crit. Care Med. 2003, 167, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Collard, H.R.; King, T.E., Jr.; Bartelson, B.B.; Vourlekis, J.S.; Schwarz, M.I.; Brown, K.K. Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2003, 168, 538–542. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, K.R.; Mumford, J.A.; Murray, S.; Kazerooni, E.A.; Gross, B.H.; Colby, T.V.; Travis, W.D.; Flint, A.; Toews, G.B.; Lynch, J.P., 3rd; et al. Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia. Am. J. Respir. Crit. Care Med. 2003, 168, 543–548. [Google Scholar] [CrossRef]
- Nathan, S.D.; Reffett, T.; Brown, A.W.; Fischer, C.P.; Shlobin, O.A.; Ahmad, S.; Weir, N.; Sheridan, M.J. The Red Cell Distribution Width as a Prognostic Indicator in Idiopathic Pulmonary Fibrosis. Chest 2013, 143, 1692–1698. [Google Scholar] [CrossRef]
- Desai, O.; Winkler, J.; Minasyan, M.; Herzog, E.L. The Role of Immune and Inflammatory Cells in Idiopathic Pulmonary Fibrosis. Front. Med. 2018, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Paliogiannis, P.; Ginesu, G.C.; Tanda, C.; Feo, C.F.; Fancellu, A.; Fois, A.G.; Mangoni, A.A.; Sotgia, S.; Carru, C.; Porcu, A.; et al. Inflammatory cell indexes as preoperative predictors of hospital stay in open elective thoracic surgery. ANZ J. Surg. 2018, 88, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Paliogiannis, P.; Satta, R.; Deligia, G.; Farina, G.; Bassu, S.; Mangoni, A.A.; Carru, C.; Zinellu, A. Associations between the neutrophil-to-lymphocyte and the platelet-to-lymphocyte ratios and the presence and severity of psoriasis: A systematic review and meta-analysis. Clin. Exp. Med. 2018, 19, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Erre, G.L.; Paliogiannis, P.; Castagna, F.; Mangoni, A.A.; Carru, C.; Passiu, G.; Zinellu, A. Me-ta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur. J. Clin. Investig. 2019, 49, e13037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinna, A.; Porcu, T.; Ricci, G.D.; Dore, S.; Boscia, F.; Paliogiannis, P.; Carru, C.; Zinellu, A. Complete Blood Cell Count–Derived Inflammation Biomarkers in Men with Age-Related Macular Degeneration. Ocul. Immunol. Inflamm. 2018, 27, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Putzu, C.; Cortinovis, D.; Colonese, F.; Canova, S.; Carru, C.; Zinellu, A.; Paliogiannis, P. Blood cell count indexes as predictors of outcomes in advanced non-small-cell lung cancer patients treated with Nivolumab. Cancer Immunol. Immunother. 2018, 67, 1349–1353. [Google Scholar] [CrossRef]
- Paliogiannis, P.; Fois, A.G.; Sotgia, S.; Mangoni, A.A.; Zinellu, E.; Pirina, P.; Carru, C.; Zinellu, A. The neutrophil-to-lymphocyte ratio as a marker of chronic obstructive pulmonary disease and its exacerbations: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2018, 48, e12984. [Google Scholar] [CrossRef] [Green Version]
- Paliogiannis, P.; Fois, A.G.; Sotgia, S.; Mangoni, A.A.; Zinellu, E.; Pirina, P.; Negri, S.; Carru, C.; Zinellu, A. Neutrophil to lymphocyte ratio and clinical outcomes in COPD: Recent evidence and future perspectives. Eur. Respir. Rev. 2018, 27, 170113. [Google Scholar] [CrossRef] [Green Version]
- Mochimaru, T.; Ueda, S.; Suzuki, Y.; Asano, K.; Fukunaga, K. Neutrophil-to-lymphocyte ratio as a novel independent predictor of severe exacerbation in patients with asthma. Ann. Allergy Asthma Immunol. 2019, 122, 337–339. [Google Scholar] [CrossRef]
- Ruta, V.; Man, A.; Alexescu, T.; Motoc, N.; Tarmure, S.; Ungur, R.; Todea, D.; Coste, S.; Valean, D.; Pop, M. Neutrophil-To-Lymphocyte Ratio and Systemic Immune-Inflammation Index—Biomarkers in Interstitial Lung Disease. Medicina 2020, 56, 381. [Google Scholar] [CrossRef]
- Zinellu, A.; Paliogiannis, P.; Sotgiu, E.; Mellino, S.; Mangoni, A.A.; Zinellu, E.; Negri, S.; Collu, C.; Pintus, G.; Serra, A.; et al. Blood cell count derived in-flammation indexes in patients with idiopathic pulmonary fibrosis. Lung 2020, 198, 821–827. [Google Scholar] [CrossRef]
- Brusasco, V.; Crapo, R.; Viegi, G. Coming together: The ATS/ERS consensus on clinical pulmonary function testing. Eur. Respir. J. 2005, 26, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wynn, T.A.; Vannella, K.M. Macrophages in Tissue Repair, Regeneration, and Fibrosis. Immunity 2016, 44, 450–462. [Google Scholar] [CrossRef] [Green Version]
- Evans, T.C.; Jehle, D. The red blood cell distribution width. J. Emerg. Med. 1991, 9, 71–74. [Google Scholar] [CrossRef]
- Tsoutsou, P.G.; Gourgoulianis, K.I.; Petinaki, E.; Germenis, A.; Tsoutsou, A.G.; Mpaka, M.; Efremidou, S.; Molyvdas, P.-A. Cytokine levels in the sera of patients with idiopathic pulmonary fibrosis. Respir. Med. 2006, 100, 938–945. [Google Scholar] [CrossRef] [Green Version]
- Ziegenhagen, M.W.; Zabel, P.; Zissel, G.; Schlaak, M.; Müller-Quernheim, J. Serum level of inter-leukin 8 is elevated in idiopathic pulmonary fibrosis and indicates disease activity. Am. J. Respir. Crit. Care. Med. 1998, 157, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Tsoutsou, P.G.; Gourgoulianis, K.I.; Petinaki, E.; Mpaka, M.; Efremidou, S.; Maniatis, A.; Molyvdas, P.A. ICAM-1, ICAM-2 and ICAM-3 in the Sera of Patients with Idiopathic Pulmonary Fibrosis. Inflammation 2004, 28, 359–364. [Google Scholar] [CrossRef]
- Korthagen, N.M.; van Moorsel, C.H.; Barlo, N.P.; Ruven, H.J.; Kruit, A.; Heron, M.; van den Bosch, J.M.; Grutters, J.C. Serum and BALF YKL-40 levels are predictors of survival in idiopathic pul-monary fibrosis. Respir. Med. 2011, 105, 106–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huszno, J.; Kolosza, Z. Prognostic value of the neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratio in breast cancer patients. Oncol. Lett. 2019, 18, 6275–6283. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.-P.; Liu, J.-P.; Tao, W.-Q.; Li, H.-M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef] [PubMed]
- Ha, R.; Lim, B.W.; Kim, D.H.; Park, J.W.; Cho, C.H.; Lee, J.H. Predictive values of neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and other prognostic factors in pediatric idiopathic sudden sensorineural hearing loss. Int. J. Pediatr. Otorhinolaryngol. 2019, 120, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.-B.; Guo, W.; Cai, S.; Zhang, F.; Shao, F.; Zhang, G.; Liu, T.; Tan, F.; Li, N.; Xue, Q.; et al. Systemic immune-inflammation index (SII) is useful to predict survival outcomes in patients with surgically resected esophageal squamous cell carcinoma. J. Cancer 2019, 10, 3188–3196. [Google Scholar] [CrossRef] [Green Version]
- Dong, G.; Huang, A.; Liu, L. Platelet-to-lymphocyte ratio and prognosis in STEMI: A meta-analysis. Eur. J. Clin. Investig. 2020, 51, e13386. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Chen, P.; Shi, S.; Liu, L.; Lv, J.; Zhu, L.; Zhang, H. Neutrophil-to-lymphocyte ratio as an independent inflammatory indicator of poor prognosis in IgA nephropathy. Int. Immunopharmacol. 2020, 87, 106811. [Google Scholar] [CrossRef] [PubMed]
- Gürün Kaya, A.; Özyürek, B.A.; Şahin Özdemirel, T.; Öz, M.; Erdoğan, Y. Prognostic Significance of Red Cell Distribution Width in Idiopathic Pulmonary Fibrosis and Combined Pulmonary Fibrosis Emphysema. Med. Princ. Pract. 2021, 30, 154–159. [Google Scholar] [CrossRef]
- Bennett, D.; Salvini, M.; Fui, A.; Cillis, G.; Cameli, P.; Mazzei, M.A.; Fossi, A.; Refini, R.M.; Rottoli, P. Calgranulin B and KL-6 in Bronchoalveolar Lavage of Patients with IPF and NSIP. Inflammation 2019, 42, 463–470. [Google Scholar] [CrossRef]
- Kreuter, M.; Lee, J.S.; Tzouvelekis, A.; Oldham, J.M.; Molyneaux, P.L.; Weycker, D.; Atwood, M.; Kirchgaessler, K.U.; Maher, T.M. Monocyte Count as a Prognostic Biomarker in Patients with Idipathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2021, 204, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Fois, A.G.; Paliogiannis, P.; Scano, V.; Cau, S.; Babudieri, S.; Perra, R.; Ruzzittu, G.; Zinellu, E.; Pirina, P.; Carru, C.; et al. The Sytemic Inflammation Index on Admission Predicts In-Hospital Mortality in COVID-19 Patients. Molecules 2020, 25, 5725. [Google Scholar] [CrossRef]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Plata, V.P.; Cabral, H.J. The Body-Mass Index, Airflow Obstruction, Dyspnea, and Exercise Capacity Index in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Prescott, E.; Almdal, T.; Mikkelsen, K.; Tofteng, C.; Vestbo, J.; Lange, P. Prognostic value of weight change in chronic obstructive pulmonary disease: Results from the Copenhagen City Heart Study. Eur. Respir. J. 2002, 20, 539–544. [Google Scholar] [CrossRef] [Green Version]
- Kulkarni, T.; Yuan, K.; Tran-Nguyen, T.K.; Kim, Y.-I.; De Andrade, J.A.; Luckhardt, T.; Valentine, V.G.; Kass, D.J.; Duncan, S.R. Decrements of body mass index are associated with poor outcomes of idiopathic pulmonary fibrosis patients. PLoS ONE 2019, 14, e0221905. [Google Scholar] [CrossRef]
- Alakhras, M.; Decker, P.A.; Nadrous, H.F.; Collazo-Clavell, M.; Ryu, J.H. Body Mass Index and Mortality in Patients with Idiopathic Pulmonary Fibrosis. Chest 2007, 131, 1448–1453. [Google Scholar] [CrossRef]
- Nishiyama, O.; Yamazaki, R.; Sano, H.; Iwanaga, T.; Higashimoto, Y.; Kume, H.; Tohda, Y. Fat-free mass index predicts survival in patients with idiopathic pulmonary fibrosis. Respirology 2016, 22, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Collu, C.; Zinellu, E.; Ahmad, K.; Nasser, M.; Traclet, J.; Sotgiu, E.; Mellino, S.; Mangoni, A.A.; Carru, C.; et al. IC4: A new combined predictive index of mortality in idiopathic pulmonary fibrosis. Panminerva Med. 2021. [Google Scholar] [CrossRef]
- Watters, L.C.; Schwarz, M.I.; Cherniack, R.M.; Waldron, J.A.; Dunn, T.L.; Stanford, R.E.; King, T.E., Jr. Idiopathic pulmonary fibrosis: Pretreatment bronchoalveolar lavage cellular constituents and their relationships with lung histopathology and clinical response to therapy. Am. Rev. Respir. Dis. 1987, 135, 696–704. [Google Scholar] [PubMed]
- Schwartz, D.A.; Helmers, R.A.; Galvin, J.R.; Van Fossen, D.S.; Frees, K.L.; Dayton, C.S.; Burmeister, L.F.; Hunninghake, G.W. Determinants of survival in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 1994, 149, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Johnston, I.D.; Prescott, R.J.; Chalmers, J.C.; Rudd, R.M. British Thoracic Society study of cryptogenic fibrosing alveolitis: Current presentation and initial management. Fibrosing Alveolitis Subcommittee of the Research Committee of the British Thoracic Society. Thorax 1997, 52, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, K.B.; Samet, J.M.; Stidley, C.A.; Colby, T.V.; Waldron, J.A. Cigarette smoking: A risk factor for idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 1997, 155, 242–248. [Google Scholar] [CrossRef]
- Zubairi, A.B.S.; Ahmad, R.; Hassan, M.; Sarwar, S.; Abbas, A.; Shahzad, T.; Irfan, M.; Muhammad, I. Clinical characteristics and factors associated with mortality in idiopathic pulmonary fibrosis: An experience from a tertiary care center in Pakistan. Clin. Respir. J. 2018, 12, 1191–1196. [Google Scholar] [CrossRef]
- Kishaba, T.; Nagano, H.; Nei, Y.; Yamashiro, S. Clinical characteristics of idiopathic pulmonary fibrosis patients according to their smoking status. J. Thorac. Dis. 2016, 8, 1112–1120. [Google Scholar] [CrossRef] [Green Version]
- King, T.E., Jr.; Schwarz, M.I.; Brown, K.; Tooze, J.A.; Colby, T.V.; Waldron, J.A., Jr.; Flint, A.; Thurlbeck, W.; Cherniack, R.M. Idiopathic pulmonary fibrosis: Relationship between histopathologic features and mortality. Am. J. Respir. Crit. Care Med. 2001, 164, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, K.M.; Hansell, D.M.; Rubens, M.B.; Marten, K.; Desai, S.R.; Siafakas, N.M.; Nicholson, A.G.; du Bois, R.M.; Wells, A.U. Idiopathic pulmonary fibrosis: Outcome in relation to smoking status. Am. J. Respir. Crit. Care Med. 2008, 177, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Guenther, A.; Krauss, E.; Tello, S.; Wagner, J.; Paul, B.; Kuhn, S.; Maurer, O.; Heinemann, S.; Costabel, U.; Barbero, M.A.N.; et al. The European IPF registry (eurIPFreg): Baseline characteristics and survival of patients with idiopathic pulmonary fi-brosis. Respir. Res. 2018, 19, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behr, J.; Kreuter, M.; Hoeper, M.M.; Wirtz, H.; Klotsche, J.; Koschel, D.; Andreas, S.; Claussen, M.; Grohe, C.; Wilkens, H.; et al. Management of patients with idiopathic pulmonary fibrosis in clinical practice: The INSIGHTS-IPF registry. Eur. Respir. J. 2015, 46, 186–196. [Google Scholar] [CrossRef] [Green Version]
- Jo, H.E.; Glaspole, I.; Grainge, C.; Goh, N.; Hopkins, P.M.; Moodley, Y.; Reynolds, P.N.; Chapman, S.; Walters, E.H.; Zappala, C.; et al. Baseline characteristics of idiopathic pulmonary fibrosis: Analysis from the Australian Idiopathic Pulmonary Fibrosis Registry. Eur. Respir. J. 2017, 49, 1601592. [Google Scholar] [CrossRef] [Green Version]
- Richeldi, L.; du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pul-monary fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef] [Green Version]
- King, T.E., Jr.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [Green Version]
- Kolb, M.; Raghu, G.; Wells, A.U.; Behr, J.; Richeldi, L.; Schinzel, B.; Quaresma, M.; Stowasser, S.; Martinez, F.J.; INSTAGE Investigators. Nintedanib plus Sildenafil in Patients with Idiopathic Pul-monary Fibrosis. N. Engl. J. Med. 2018, 379, 1722–1731. [Google Scholar] [CrossRef]
- Sesé, L.; Nunes, H.; Cottin, V.; Israel-Biet, D.; Crestani, B.; Guillot-Dudoret, S.; Cadranel, J.; Wal-laert, B.; Tazi, A.; Maître, B.; et al. Gender Differences in Idiopathic Pulmonary Fibrosis: Are Men and Women Equal? Front. Med. 2021, 8, 713698. [Google Scholar] [CrossRef]
- Durheim, M.T.; Judy, J.; Bender, S.; Neely, M.L.; Baumer, D.; Robinson, S.B.; Conoscenti, C.S.; Leonard, T.B.; Lazarus, H.M.; Palmer, S.M. A retrospective study of in-hospital mortality in patients with idiopathic pulmonary fibrosis between 2015 and 2018. Medicine 2020, 99, e23143. [Google Scholar] [CrossRef]
- Marcon, A.; Schievano, E.; Fedeli, U. Mortality Associated with Idiopathic Pulmonary Fibrosis in Northeastern Italy, 2008–2020: A Multiple Cause of Death Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7249. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Perlman, D.; Tomic, R. Natural history of idiopathic pulmonary fibrosis. Respir. Med. 2015, 109, 661–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Muñiz Ballesteros, B.; López-Herranz, M.; Lopez-de-Andrés, A.; Hernandez-Barrera, V.; Jiménez-García, R.; Carabantes-Alarcon, D.; Jiménez-Trujillo, I.; de Miguel-Diez, J. Sex Differ-ences in the Incidence and Outcomes of Patients Hospitalized by Idiopathic Pulmonary Fibrosis (IPF) in Spain from 2016 to 2019. J. Clin. Med. 2021, 10, 3474. [Google Scholar] [CrossRef]
- Nadrous, H.F.; Ryu, J.H.; Douglas, W.W.; Decker, P.A.; Olson, E.J. Impact of Angiotensin-Converting Enzyme Inhibitors and Statins on Survival in Idiopathic Pulmonary Fibrosis. Chest 2004, 126, 438–446. [Google Scholar] [CrossRef]
- Song, H.; Sun, D.; Ban, C.; Liu, Y.; Zhu, M.; Ye, Q.; Yan, W.; Ren, Y.; Dai, H. Independent Clinical Factors Relevant to Prognosis of Patients with Idiopathic Pulmonary Fibrosis. Med. Sci. Monit. 2019, 25, 4193–4201. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| IPF (n = 82) | |
|---|---|
| Age (years) | 72 ± 7 |
| Gender (F/M) | 9/73 |
| BMI (kg/m2) | 26.8 ± 4.0 |
| Smokers (current/former/no) | 2/61/19 |
| FEV1 (% predicted) | 79.1 ± 20.9 |
| FVC (% predicted) | 77.0 ± 19.2 |
| TLC (% predicted) | 70.0 ± 21.4 |
| DLCO (% predicted) | 45.7 ± 18.3 |
| 6MWT (meters) | 412 ± 138 |
| Disease stage (I/II/III) | 33/41/8 |
| Arterial hypertension (yes/no) | 43/39 |
| Ischemic cardiopathy or cerebrovascular disease (yes/no %) | 16/66 |
| Gastroesophageal reflux disease (yes/no) | 25/57 |
| Pulmonary hypertension (yes/no) | 16/66 |
| COPD or emphysema (yes/no) | 13/69 |
| OSAS (yes/no) | 7/74 |
| Antifibrotic drugs (none/Pirf/Nin) | 30/46/6 |
| Antiaggregants (yes/no) | 33/49 |
| Anticoagulants (yes/no) | 10/72 |
| WBC (×109 L) | 8.26 (7.21–9.66) |
| Monocytes (×109 L) | 1.83 (1.44–2.29) |
| Lymphocytes (×109 L) | 0.61 (0.50–0.80) |
| Neutrophils (×109 L) | 5.34 (4.36–6.20) |
| Platelets (×109 L) | 237 ± 72 |
| NLR | 3.00 (2.25–4.18) |
| dNLR | 1.95 (1.51–2.55) |
| LMR | 3.17 ± 1.36 |
| PLR | 118 (93–169) |
| SII | 708 (479-969) |
| SIRI | 1.82 (1.29–2.74) |
| AISI | 434 (282–584) |
| DLCO % | FEV1 % | FVC % | TLC % | 6MWT | Disease Stage | Survival | ||
|---|---|---|---|---|---|---|---|---|
| WBC | Correlation coefficient Significance level P | −0.340 0.0040 | −0.284 0.0117 | −0.386 0.0006 | −0.394 0.0007 | −0.062 0.6114 | 0.380 0.0017 | −0.207 0.0651 |
| Lymphocytes | Correlation coefficient Significance level P | 0.094 0.4351 | 0.001 0.9927 | 0.005 0.9643 | −0.164 0.1684 | 0.327 0.0057 | 0.073 0.5588 | −0.003 0.9818 |
| Monocytes | Correlation coefficient Significance level P | −0.070 0.5594 | −0.096 0.3981 | −0.172 0.1376 | −0.175 0.1412 | −0.082 0.4974 | 0.100 0.4187 | −0.247 0.0265 |
| Neutrophils | Correlation coefficient Significance level P | −0.422 0.0002 | −0.332 0.0028 | −0.375 0.0008 | −0.356 0.0021 | −0.176 0.1439 | 0.324 0.0076 | −0.193 0.0850 |
| Platelets | Correlation coefficient Significance level P | −0.041 0.7356 | −0.299 0.0075 | −0.195 0.0922 | −0.231 0.0514 | −0.077 0.5286 | 0.020 0.8708 | −0.231 0.0382 |
| DLCO % | FEV1 % | FVC % | TLC % | 6MWT | Disease Stage | Survival | ||
|---|---|---|---|---|---|---|---|---|
| NLR | Correlation coefficient Significance level P | −0.373 0.0014 | −0.237 0.0358 | −0.242 0.0353 | −0.106 0.3777 | −0.374 0.0014 | 0.212 0.0843 | −0.101 0.3696 |
| dNLR | Correlation coefficient Significance level P | −0.422 0.0003 | −0.240 0.0357 | −0.198 0.0880 | −0.126 0.2978 | −0.303 0.0113 | 0.228 0.0658 | −0.083 0.4671 |
| LMR | Correlation coefficient Significance level P | 0.148 0.2178 | 0.055 0.6312 | 0.106 0.3609 | −0.017 0.8897 | 0.339 0.0041 | −0.026 0.8317 | 0.206 0.0657 |
| PLR | Correlation coefficient Significance level P | −0.128 0.2860 | −0.157 0.1663 | −0.082 0.4802 | −0.001 0.9928 | −0.295 0.0133 | −0.063 0.6116 | −0.188 0.0936 |
| SII | Correlation coefficient Significance level P | −0.365 0.0018 | −0.282 0.0117 | −0.249 0.0301 | −0.200 0.0924 | −0.401 0.0006 | 0.148 0.2328 | −0.250 0.0245 |
| SIRI | Correlation coefficient Significance level P | −0.369 0.0015 | −0.275 0.0140 | −0.337 0.0029 | −0.225 0.0573 | −0.424 0.0003 | 0.260 0.0334 | −0.278 0.0120 |
| AISI | Correlation coefficient Significance level P | −0.324 0.0055 | −0.294 0.0081 | −0.324 0.0043 | −0.265 0.0234 | −0.414 0.0004 | 0.196 0.1118 | −0.344 0.0016 |
| Variable | Median Value | Logrank Test | |
|---|---|---|---|
| Chi-Squared | p-Value | ||
| WBC | 8.26 | 2.08 | 0.15 |
| Lymphocytes | 1.83 | 0.01 | 0.93 |
| Monocytes | 0.61 | 2.68 | 0.10 |
| Neutrophils | 5.34 | 0.82 | 0.36 |
| Platelets | 228 | 1.02 | 0.31 |
| NLR | 3.00 | 0.31 | 0.58 |
| dNLR | 1.95 | 0.04 | 0.84 |
| LMR | 3.05 | 0.26 | 0.61 |
| PLR | 118 | 0.50 | 0.48 |
| SII | 708 | 1.60 | 0.21 |
| SIRI | 1.82 | 1.10 | 0.29 |
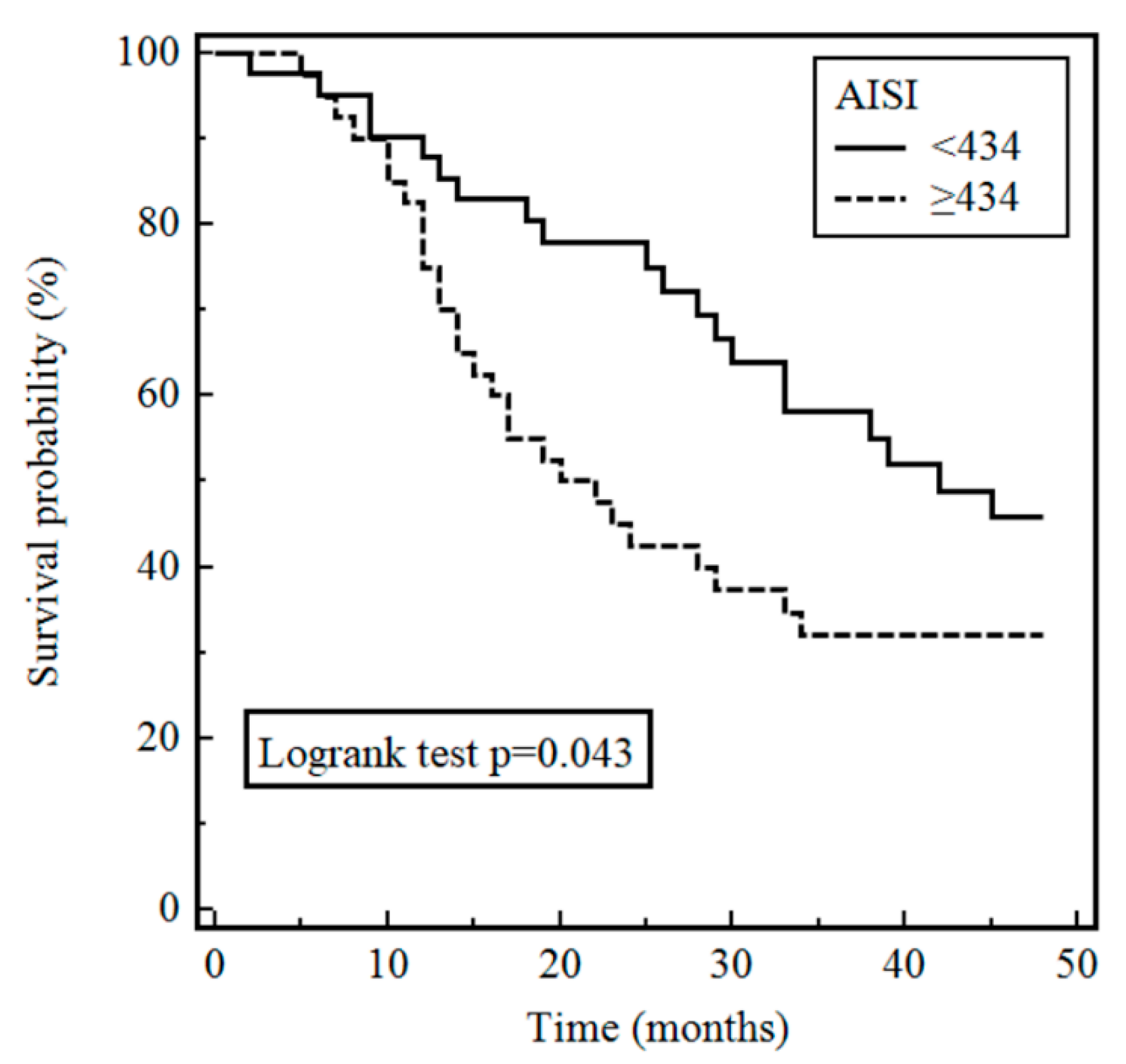
| AISI | 434 | 4.08 | 0.043 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 1.0271 (0.9863–1.0695) | 0.20 | 1.0481 (0.9816–1.1192) | 0.16 |
| Gender | 0.6803 (0.2439–1.8973) | 0.46 | 0.7934 (0.1812–3.4749) | 0.76 |
| BMI | 0.8528 (0.7820–0.9299) | 0.0003 | 0.8589 (0.7685–0.9601) | 0.007 |
| Smoking status | 0.8223 (0.5876–1.1509) | 0.25 | 0.7150 (0.4559–1.1212) | 0.14 |
| Disease stage | 1.5011 (0.9231–2.4411) | 0.10 | 1.2901 (0.7460–2.2311) | 0.36 |
| Antifibrotic drugs | 0.7578 (0.4657–1.2330) | 0.26 | 1.0097 (0.5669–1.7981) | 0.97 |
| AISI | 1.0012 (1.0005–1.0018) | 0.0006 | 1.0017(1.0006–1.0027) | 0.003 |
| AISI < 434 (n = 41) | AISI ≥ 434 (n = 41) | p-Value | |
|---|---|---|---|
| Age (years) | 71 ± 6 | 73 ± 7 | 0.16 |
| Gender (F/M) | 3/38 | 6/35 | 0.29 |
| BMI (kg/m2) | 27.5 ± 4.4 | 26.1 ± 3.6 | 0.13 |
| Smokers (current/former/no) | 0/33/8 | 2/28/11 | 0.23 |
| FEV1 (% predicted) | 84.7 ± 18.3 | 73.8 ± 22.0 | 0.019 |
| FVC (% predicted) | 81.6 ± 18.5 | 72.2 ± 19.1 | 0.033 |
| TLC (% predicted) | 74.4 ± 21.9 | 65.0 ± 19.9 | 0.059 |
| DLCO (% predicted) | 48.2 ± 15.8 | 42.9 ± 20.6 | 0.23 |
| 6MWT (meters) | 458 ± 116 | 363 ± 146 | 0.004 |
| Disease stage (I/II/III) | 18/20/3 | 15/21/5 | 0.67 |
| Dead/alive | 20/21 | 27/14 | 0.12 |
| WBC (×109 L) | 7.58 (7.01–8.84) | 8.59 (7.73–10.87) | 0.006 |
| Monocytes (×109 L) | 0.56 (0.47–0.72) | 0.65 (0.57–0.83) | 0.012 |
| Lymphocytes (×109 L) | 1.94 (1.70–2.59) | 1.56 (1.25–2.17) | 0.007 |
| Neutrophils (×109 L) | 4.63 (4.08–5.45) | 5.74 (5.16–7.34) | <0.001 |
| Platelets (×109 L) | 206 ± 60 | 267 ± 71 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zinellu, A.; Collu, C.; Nasser, M.; Paliogiannis, P.; Mellino, S.; Zinellu, E.; Traclet, J.; Ahmad, K.; Mangoni, A.A.; Carru, C.; et al. The Aggregate Index of Systemic Inflammation (AISI): A Novel Prognostic Biomarker in Idiopathic Pulmonary Fibrosis. J. Clin. Med. 2021, 10, 4134. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184134
Zinellu A, Collu C, Nasser M, Paliogiannis P, Mellino S, Zinellu E, Traclet J, Ahmad K, Mangoni AA, Carru C, et al. The Aggregate Index of Systemic Inflammation (AISI): A Novel Prognostic Biomarker in Idiopathic Pulmonary Fibrosis. Journal of Clinical Medicine. 2021; 10(18):4134. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184134
Chicago/Turabian StyleZinellu, Angelo, Claudia Collu, Mouhamad Nasser, Panagiotis Paliogiannis, Sabrina Mellino, Elisabetta Zinellu, Julie Traclet, Kais Ahmad, Arduino Aleksander Mangoni, Ciriaco Carru, and et al. 2021. "The Aggregate Index of Systemic Inflammation (AISI): A Novel Prognostic Biomarker in Idiopathic Pulmonary Fibrosis" Journal of Clinical Medicine 10, no. 18: 4134. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184134