
The Influence of Psychotherapy on Peripheral Brain-Derived Neurotrophic Factor Concentration Levels and Gene Methylation Status: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Inclusion Criteria
2.3. Data Extraction and Variables Investigated
2.4. Data Synthesis
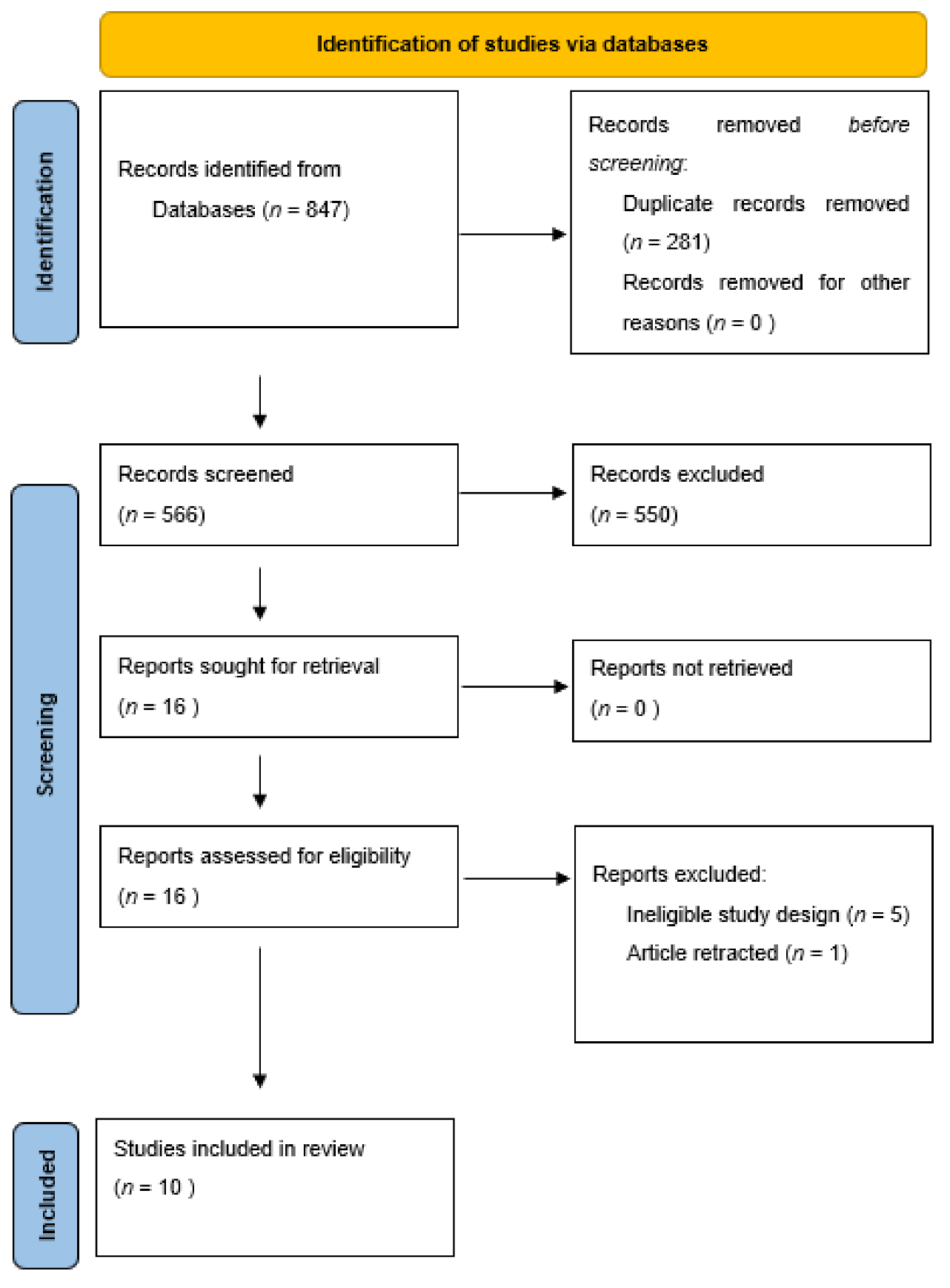
2.5. Studies Retrieved
3. Results
3.1. Peripheral BDNF Concentration Levels
3.2. BDNF Promoter Gene Methylation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Weingarten, C.P.; Strauman, T.J. Neuroimaging for psychotherapy research: Current trends. Psychother. Res. 2015, 25, 185–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binder, D.K.; Scharfman, H.E. Brain-derived neurotrophic factor. Growth Factors 2004, 22, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Lee, S.; Park, H.; Suzuki, T. A large, cross-sectional observational study of serum BDNF, cognitive function, and mild cognitive impairment in the elderly. Front. Aging Neurosci. 2014, 6, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, M.; Morici, J.F.; Zanoni, M.B.; Bekinschtein, P. Brain-Derived Neurotrophic Factor: A Key Molecule for Memory in the Healthy and the Pathological Brain. Front. Cell. Neurosci. 2019, 13, 363. [Google Scholar] [CrossRef]
- Mizoguchi, Y.; Yao, H.; Imamura, Y.; Hashimoto, M.; Monji, A. Lower brain-derived neurotrophic factor levels are associated with age-related memory impairment in community-dwelling older adults: The Sefuri study. Sci. Rep. 2020, 10, 16442. [Google Scholar] [CrossRef]
- Hariri, A.R.; Goldberg, T.E.; Mattay, V.S.; Kolachana, B.S.; Callicott, J.H.; Egan, M.F.; Weinberger, D.R. Brain-derived neurotrophic factor val66met polymorphism affects human memory-related hippocampal activity and predicts memory performance. J. Neurosci. Off. J. Soc. Neurosci. 2003, 23, 6690–6694. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, T.E.; Iudicello, J.; Russo, C.; Elvevåg, B.; Straub, R.; Egan, M.F.; Weinberger, D.R. BDNF Val66Met polymorphism significantly affects d’ in verbal recognition memory at short and long delays. Biol. Psychol. 2008, 77, 20–24. [Google Scholar] [CrossRef]
- Egan, M.F.; Kojima, M.; Callicott, J.H.; Goldberg, T.E.; Kolachana, B.S.; Bertolino, A.; Zaitsev, E.; Gold, B.; Goldman, D.; Dean, M.; et al. The BDNF val66met Polymorphism Affects Activity-Dependent Secretion of BDNF and Human Memory and Hippocampal Function. Cell 2003, 112, 257–269. [Google Scholar] [CrossRef] [Green Version]
- Autry, A.E.; Monteggia, L.M. Brain-derived neurotrophic factor and neuropsychiatric disorders. Pharm. Rev. 2012, 64, 238–258. [Google Scholar] [CrossRef] [Green Version]
- Youssef, M.M.; Underwood, M.D.; Huang, Y.-Y.; Hsiung, S.-C.; Liu, Y.; Simpson, N.R.; Bakalian, M.J.; Rosoklija, G.B.; Dwork, A.J.; Arango, V.; et al. Association of BDNF Val66Met Polymorphism and Brain BDNF Levels with Major Depression and Suicide. Int. J. Neuropsychopharmacol. 2018, 21, 528–538. [Google Scholar] [CrossRef]
- Sklar, P.; Gabriel, S.B.; McInnis, M.G.; Bennett, P.; Lim, Y.; Tsan, G.; Schaffner, S.; Kirov, G.; Jones, I.; Owen, M.; et al. Family-based association study of 76 candidate genes in bipolar disorder: BDNF is a potential risk locus. Brain-derived neutrophic factor. Mol. Psychiatry 2002, 7, 579–593. [Google Scholar] [CrossRef] [Green Version]
- Sarchiapone, M.; Carli, V.; Roy, A.; Iacoviello, L.; Cuomo, C.; Latella, M.C.; di Giannantonio, M.; Janiri, L.; de Gaetano, M.; Janal, M.N. Association of polymorphism (Val66Met) of brain-derived neurotrophic factor with suicide attempts in depressed patients. Neuropsychobiology 2008, 57, 139–145. [Google Scholar] [CrossRef]
- Brandys, M.K.; Kas, M.J.; van Elburg, A.A.; Campbell, I.C.; Adan, R.A. A meta-analysis of circulating BDNF concentrations in anorexia nervosa. World J. Biol. Psychiatry 2011, 12, 444–454. [Google Scholar] [CrossRef]
- Sen, S.; Duman, R.; Sanacora, G. Serum brain-derived neurotrophic factor, depression, and antidepressant medications: Meta-analyses and implications. Biol. Psychiatry 2008, 64, 527–532. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, B.S.; Steiner, J.; Berk, M.; Molendijk, M.L.; Gonzalez-Pinto, A.; Turck, C.W.; Nardin, P.; Gonçalves, C.A. Peripheral brain-derived neurotrophic factor in schizophrenia and the role of antipsychotics: Meta-analysis and implications. Mol. Psychiatry 2015, 20, 1108–1119. [Google Scholar] [CrossRef]
- Ng, T.K.S.; Ho, C.S.H.; Tam, W.W.S.; Kua, E.H.; Ho, R.C.-M. Decreased Serum Brain-Derived Neurotrophic Factor (BDNF) Levels in Patients with Alzheimer’s Disease (AD): A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 257. [Google Scholar] [CrossRef] [Green Version]
- Iughetti, L.; Lucaccioni, L.; Fugetto, F.; Predieri, B.; Berardi, A.; Ferrari, F. Brain-derived neurotrophic factor and epilepsy: A systematic review. Neuropeptides 2018, 72, 23–29. [Google Scholar] [CrossRef]
- Roth, T.L.; Sweatt, J.D. Epigenetic marking of the BDNF gene by early-life adverse experiences. Horm. Behav. 2011, 59, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Miao, Z.; Wang, Y.; Sun, Z. The Relationships between Stress, Mental Disorders, and Epigenetic Regulation of BDNF. Int. J. Mol. Sci. 2020, 21, 1375. [Google Scholar] [CrossRef] [Green Version]
- Moser, D.A.; Paoloni-Giacobino, A.; Stenz, L.; Adouan, W.; Manini, A.; Suardi, F.; Cordero, M.I.; Vital, M.; Sancho Rossignol, A.; Rusconi-Serpa, S.; et al. BDNF Methylation and Maternal Brain Activity in a Violence-Related Sample. PLoS ONE 2015, 10, e0143427. [Google Scholar] [CrossRef]
- Thaler, L.; Gauvin, L.; Joober, R.; Groleau, P.; de Guzman, R.; Ambalavanan, A.; Israel, M.; Wilson, S.; Steiger, H. Methylation of BDNF in women with bulimic eating syndromes: Associations with childhood abuse and borderline personality disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2014, 54, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.Y.; Kim, S.J.; Chung, H.G.; Choi, J.H.; Kim, S.H.; Kang, J.I. Epigenetic alterations of the BDNF gene in combat-related post-traumatic stress disorder. Acta Psychiatr. Scand. 2017, 135, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.K.; McDougall, S.; Thomas, S.; Wiener, J. The Impact of the Brain-Derived Neurotrophic Factor Gene on Trauma and Spatial Processing. J. Clin. Med. 2017, 6, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G.W.Y.; Wolkowitz, O.M.; Reus, V.I.; Kang, J.I.; Elnar, M.; Sarwal, R.; Flory, J.D.; Abu-Amara, D.; Hammanieh, R.; Gautam, A.; et al. Serum brain-derived neurotrophic factor remains elevated after long term follow-up of combat veterans with chronic post-traumatic stress disorder. Psychoneuroendocrinology 2021, 105360. [Google Scholar] [CrossRef]
- Hauck, S.; Kapczinski, F.; Roesler, R.; de Moura Silveira, E., Jr.; Magalhães, P.V.; Kruel, L.R.; Schestatsky, S.S.; Ceitlin, L.H. Serum brain-derived neurotrophic factor in patients with trauma psychopathology. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 459–462. [Google Scholar] [CrossRef]
- Matsuoka, Y.; Nishi, D.; Noguchi, H.; Kim, Y.; Hashimoto, K. Longitudinal changes in serum brain-derived neurotrophic factor in accident survivors with posttraumatic stress disorder. Neuropsychobiology 2013, 68, 44–50. [Google Scholar] [CrossRef]
- Dell’Osso, L.; Carmassi, C.; Del Debbio, A.; Catena Dell’Osso, M.; Bianchi, C.; da Pozzo, E.; Origlia, N.; Domenici, L.; Massimetti, G.; Marazziti, D.; et al. Brain-derived neurotrophic factor plasma levels in patients suffering from post-traumatic stress disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2009, 33, 899–902. [Google Scholar] [CrossRef]
- Angelucci, F.; Ricci, V.; Gelfo, F.; Martinotti, G.; Brunetti, M.; Sepede, G.; Signorelli, M.; Aguglia, E.; Pettorruso, M.; Vellante, F.; et al. BDNF serum levels in subjects developing or not post-traumatic stress disorder after trauma exposure. Brain Cogn. 2014, 84, 118–122. [Google Scholar] [CrossRef]
- Toledo-Rodriguez, M.; Lotfipour, S.; Leonard, G.; Perron, M.; Richer, L.; Veillette, S.; Pausova, Z.; Paus, T. Maternal smoking during pregnancy is associated with epigenetic modifications of the brain-derived neurotrophic factor-6 exon in adolescent offspring. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2010, 153, 1350–1354. [Google Scholar] [CrossRef]
- Zheleznyakova, G.Y.; Cao, H.; Schiöth, H.B. BDNF DNA methylation changes as a biomarker of psychiatric disorders: Literature review and open access database analysis. Behav. Brain Funct. 2016, 12, 17. [Google Scholar] [CrossRef] [Green Version]
- Matrisciano, F.; Bonaccorso, S.; Ricciardi, A.; Scaccianoce, S.; Panaccione, I.; Wang, L.; Ruberto, A.; Tatarelli, R.; Nicoletti, F.; Girardi, P.; et al. Changes in BDNF serum levels in patients with major depression disorder (MDD) after 6 months treatment with sertraline, escitalopram, or venlafaxine. J. Psychiatr. Res 2009, 43, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, R.; Mitoma, M.; Sugita, A.; Hori, H.; Okamoto, T.; Umene, W.; Ueda, N.; Nakamura, J. Effects of paroxetine or milnacipran on serum brain-derived neurotrophic factor in depressed patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2007, 31, 1034–1037. [Google Scholar] [CrossRef]
- Hellweg, R.; Ziegenhorn, A.; Heuser, I.; Deuschle, M. Serum concentrations of nerve growth factor and brain-derived neurotrophic factor in depressed patients before and after antidepressant treatment. Pharmacopsychiatry 2008, 41, 66–71. [Google Scholar] [CrossRef]
- Molendijk, M.L.; Bus, B.A.; Spinhoven, P.; Penninx, B.W.; Kenis, G.; Prickaerts, J.; Voshaar, R.C.; Elzinga, B.M. Serum levels of brain-derived neurotrophic factor in major depressive disorder: State-trait issues, clinical features and pharmacological treatment. Mol. Psychiatry 2011, 16, 1088–1095. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Zhang, J.; Sun, D.; Fan, Y.; Zhou, H.; Fu, B. Effects of fluoxetine on brain-derived neurotrophic factor serum concentration and cognition in patients with vascular dementia. Clin. Interv. Aging 2014, 9, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Castrén, E.; Monteggia, L.M. Brain-Derived Neurotrophic Factor Signaling in Depression and Antidepressant Action. Biol. Psychiatry 2021, 90, 128–136. [Google Scholar] [CrossRef]
- Zheng, F.; Wang, H. NMDA-mediated and self-induced bdnf exon IV transcriptions are differentially regulated in cultured cortical neurons. Neurochem. Int. 2009, 54, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Vanicek, T.; Kranz, G.S.; Vyssoki, B.; Komorowski, A.; Fugger, G.; Höflich, A.; Micskei, Z.; Milovic, S.; Lanzenberger, R.; Eckert, A.; et al. Repetitive enhancement of serum BDNF subsequent to continuation ECT. Acta Psychiatr. Scand. 2019, 140, 426–434. [Google Scholar] [CrossRef] [Green Version]
- Rocha, R.B.; Dondossola, E.R.; Grande, A.J.; Colonetti, T.; Ceretta, L.B.; Passos, I.C.; Quevedo, J.; da Rosa, M.I. Increased BDNF levels after electroconvulsive therapy in patients with major depressive disorder: A meta-analysis study. J. Psychiatr. Res. 2016, 83, 47–53. [Google Scholar] [CrossRef]
- Gomutbutra, P.; Yingchankul, N.; Chattipakorn, N.; Chattipakorn, S.; Srisurapanont, M. The Effect of Mindfulness-Based Intervention on Brain-Derived Neurotrophic Factor (BDNF): A Systematic Review and Meta-Analysis of Controlled Trials. Front. Psychol. 2020, 11, 2209. [Google Scholar] [CrossRef]
- Szuhany, K.L.; Bugatti, M.; Otto, M.W. A meta-analytic review of the effects of exercise on brain-derived neurotrophic factor. J. Psychiatr. Res. 2015, 60, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Sung, Y.-H.; Seo, J.-H.; Lee, S.-W.; Lim, B.-V.; Lee, C.-Y.; Chung, Y.-R. Effects of treadmill exercise-intensity on short-term memory in the rats born of the lipopolysaccharide-exposed maternal rats. J. Exerc. Rehabil. 2015, 11, 296–302. [Google Scholar] [CrossRef]
- Gomez-Pinilla, F.; Zhuang, Y.; Feng, J.; Ying, Z.; Fan, G. Exercise impacts brain-derived neurotrophic factor plasticity by engaging mechanisms of epigenetic regulation. Eur. J. Neurosci. 2011, 33, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Claudino, F.C.A.; Gonçalves, L.; Schuch, F.B.; Martins, H.R.S.; da Rocha, N.S. The Effects of Individual Psychotherapy in BDNF Levels of Patients with Mental Disorders: A Systematic Review. Front. Psychiatry 2020, 11, 445. [Google Scholar] [CrossRef]
- Koch, J.M.; Hinze-Selch, D.; Stingele, K.; Huchzermeier, C.; Goder, R.; Seeck-Hirschner, M.; Aldenhoff, J.B. Changes in CREB Phosphorylation and BDNF Plasma Levels during Psychotherapy of Depression. Psychother. Psychosom. 2009, 78, 187–192. [Google Scholar] [CrossRef]
- Yamada, H.; Yoshimura, C.; Nakajima, T.; Nagata, T. Recovery of low plasma BDNF over the course of treatment among patients with bulimia nervosa. Psychiatry Res. 2012, 198, 448–451. [Google Scholar] [CrossRef]
- Perroud, N.; Salzmann, A.; Prada, P.; Nicastro, R.; Hoeppli, M.E.; Furrer, S.; Ardu, S.; Krejci, I.; Karege, F.; Malafosse, A. Response to psychotherapy in borderline personality disorder and methylation status of the BDNF gene. Transl. Psychiatry 2013, 3, e207. [Google Scholar] [CrossRef] [Green Version]
- Zwipp, J.; Hass, J.; Schober, I.; Geisler, D.; Ritschel, F.; Seidel, M.; Weiss, J.; Roessner, V.; Hellweg, R.; Ehrlich, S. Serum brain-derived neurotrophic factor and cognitive functioning in underweight, weight-recovered and partially weight-recovered females with anorexia nervosa. Prog. Neuropsychopharmacol. Biol. Psychiatry 2014, 54, 163–169. [Google Scholar] [CrossRef]
- Powers, M.B.; Medina, J.L.; Burns, S.; Kauffman, B.Y.; Monfils, M.; Asmundson, G.J.; Diamond, A.; McIntyre, C.; Smits, J.A. Exercise Augmentation of Exposure Therapy for PTSD: Rationale and Pilot Efficacy Data. Cogn. Behav. Ther. 2015, 44, 314–327. [Google Scholar] [CrossRef] [Green Version]
- Rusch, H.L.; Guardado, P.; Baxter, T.; Mysliwiec, V.; Gill, J.M. Improved Sleep Quality is Associated with Reductions in Depression and PTSD Arousal Symptoms and Increases in IGF-1 Concentrations. J. Clin. Sleep Med. 2015, 11, 615–623. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.; Knoblich, N.; Wallisch, A.; Glowacz, K.; Becker-Sadzio, J.; Gundel, F.; Bruckmann, C.; Nieratschker, V. Increased BDNF methylation in saliva, but not blood, of patients with borderline personality disorder. Clin. Epigenet. 2018, 10, 109. [Google Scholar] [CrossRef] [PubMed]
- da Silva, S.K.; Wiener, C.; Ghisleni, G.; Oses, J.P.; Jansen, K.; Molina, M.L.; Silva, R.; Souza, L.D. Effects of cognitive-behavioral therapy on neurotrophic factors in patients with major depressive disorder. Rev. Bras. Psiquiatr. 2018, 40, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruijniks, S.J.E.; van Grootheest, G.; Cuijpers, P.; de Kluiver, H.; Vinkers, C.H.; Peeters, F.; Penninx, B.; Teunissen, C.E.; Huibers, M.J.H. Working memory moderates the relation between the brain-derived neurotropic factor (BDNF) and psychotherapy outcome for depression. J. Psychiatr. Res. 2020, 130, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Orosz, A.; Federspiel, A.; Eckert, A.; Seeher, C.; Dierks, T.; Tschitsaz, A.; Cattapan, K. Exploring the effectiveness of a specialized therapy programme for burnout using subjective report and biomarkers of stress. Clin. Psychol. Psychother. 2021, 28, 852–861. [Google Scholar] [CrossRef]
- Ehrlich, S.; Salbach-Andrae, H.; Eckart, S.; Merle, J.V.; Burghardt, R.; Pfeiffer, E.; Franke, L.; Uebelhack, R.; Lehmkuhl, U.; Hellweg, R. Serum brain-derived neurotrophic factor and peripheral indicators of the serotonin system in underweight and weight-recovered adolescent girls and women with anorexia nervosa. J. Psychiatry Neurosci. 2009, 34, 323–329. [Google Scholar]
- Phillips, C. Brain-Derived Neurotrophic Factor, Depression, and Physical Activity: Making the Neuroplastic Connection. Neural Plast. 2017, 2017, 7260130. [Google Scholar] [CrossRef]
- Gravesteijn, E.; Mensink, R.P.; Plat, J. Effects of nutritional interventions on BDNF concentrations in humans: A systematic review. Nutr. Neurosci. 2021, 1–12. [Google Scholar] [CrossRef]
- Lopez, J.P.; Mamdani, F.; Labonte, B.; Beaulieu, M.M.; Yang, J.P.; Berlim, M.T.; Ernst, C.; Turecki, G. Epigenetic regulation of BDNF expression according to antidepressant response. Mol. Psychiatry 2013, 18, 398–399. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Dowlatshahi, D.; MacQueen, G.M.; Wang, J.F.; Young, L.T. Increased hippocampal BDNF immunoreactivity in subjects treated with antidepressant medication. Biol. Psychiatry 2001, 50, 260–265. [Google Scholar] [CrossRef]
- Molendijk, M.L.; Spinhoven, P.; Polak, M.; Bus, B.A.; Penninx, B.W.; Elzinga, B.M. Serum BDNF concentrations as peripheral manifestations of depression: Evidence from a systematic review and meta-analyses on 179 associations (N = 9484). Mol. Psychiatry 2014, 19, 791–800. [Google Scholar] [CrossRef]
- Rowland, T.; Perry, B.I.; Upthegrove, R.; Barnes, N.; Chatterjee, J.; Gallacher, D.; Marwaha, S. Neurotrophins, cytokines, oxidative stress mediators and mood state in bipolar disorder: Systematic review and meta-analyses. Br. J. Psychiatry J. Ment. Sci. 2018, 213, 514–525. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, B.S.; Molendijk, M.L.; Köhler, C.A.; Soares, J.C.; Leite, C.M.G.S.; Machado-Vieira, R.; Ribeiro, T.L.; Silva, J.C.; Sales, P.M.G.; Quevedo, J.; et al. Peripheral brain-derived neurotrophic factor (BDNF) as a biomarker in bipolar disorder: A meta-analysis of 52 studies. BMC Med. 2015, 13, 289. [Google Scholar] [CrossRef] [Green Version]
- Çakici, N.; Sutterland, A.L.; Penninx, B.; Dalm, V.A.; de Haan, L.; van Beveren, N.J.M. Altered peripheral blood compounds in drug-naïve first-episode patients with either schizophrenia or major depressive disorder: A meta-analysis. Brain Behav. Immun. 2020, 88, 547–558. [Google Scholar] [CrossRef]
- Sanada, K.; Zorrilla, I.; Iwata, Y.; Bermúdez-Ampudia, C.; Graff-Guerrero, A.; Martínez-Cengotitabengoa, M.; González-Pinto, A. The Efficacy of Non-Pharmacological Interventions on Brain-Derived Neurotrophic Factor in Schizophrenia: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2016, 17, 1766. [Google Scholar] [CrossRef] [Green Version]
- Yan, G.; Zhang, M.; Liu, Y.; Yin, M. Efficacy of vortioxetine combined cognitive behaviour intervention therapy on brain-derived neurotrophic factor level on depressive patients. Psychogeriatrics 2019, 19, 475–481. [Google Scholar] [CrossRef]
- Retraction. Psychogeriatrics 2021, 21, 146. [CrossRef]
- Ziegler, C.; Richter, J.; Mahr, M.; Gajewska, A.; Schiele, M.A.; Gehrmann, A.; Schmidt, B.; Lesch, K.P.; Lang, T.; Helbig-Lang, S.; et al. MAOA gene hypomethylation in panic disorder-reversibility of an epigenetic risk pattern by psychotherapy. Transl. Psychiatry 2016, 6, e773. [Google Scholar] [CrossRef]
- Roberts, S.; Lester, K.J.; Hudson, J.L.; Rapee, R.M.; Creswell, C.; Cooper, P.J.; Thirlwall, K.J.; Coleman, J.R.; Breen, G.; Wong, C.C.; et al. Serotonin transporter [corrected] methylation and response to cognitive behaviour therapy in children with anxiety disorders. Transl. Psychiatry 2014, 4, e444. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study | Diagnosis | Subjects (N) | Control (N) | Type of Therapy | Length of Therapy | Material Analyzed | Main Findings |
|---|---|---|---|---|---|---|---|
| Koch et al. (2009) [45] | MDD | 30 | N/A | IPT 1 | 12 sessions biweekly | Plasma BDNF | No difference |
| Yamada et al. (2012) [46] | BN | 7 | N/A | Behavioral program and cognitive treatment | 4 weeks | Plasma BDNF | Increased BDNF level without link to BMI or psychological factors, decrease frequency of binge eating and purging behaviors |
| Perroud et al. (2013) [47] | BPD | 115 | N/A | DBT 2 | 4 weeks | Serum BDNF/blood BDNF promoter methylation | Nonsignificant increase in BDNF serum levels in therapy responders |
| Zwipp et al. (2014) [48] | AN | 14 | N/A | behaviorally oriented, nutritional rehabilitation program | unknown | Serum BDNF | Increased BDNF level after weight gain |
| Powers et al. (2015) [49] | PTSD | 9 | N/A | Prolonged exposure therapy | 12 sessions | Plasma BDNF | No difference |
| Rusch et al. (2015) [50] | Insomnia | 44 | N/A | CBT-I 3 | 4–8 sessions | Plasma BDNF | Nonsignificant BDNF increase in responders, significant reductions in depression, posttraumatic arousal symptoms, improvement in emotional well-being and energy/fatigue in responders |
| Thomas et al. (2018) [51] | BPD | 26 | N/A | DBT | 12 weeks | Blood/Saliva BDNF promoter methylation | Decrease in BDNF IV promoter methylation, no differences in methylation change between patients with and without significant improvement |
| Da Silva et al. (2018) [52] | MDD | 55 | N/A | CBT 4 | 16 sessions | Serum BDNF | No difference |
| Bruijniks et al. (2020) [53] | MDD | 82 | N/A | IPT/CBT | once or twice a week for 16–24 weeks, maximum 20 sessions | Serum | No difference |
| Orosz et al. (2020) [54] | MMD, burnout | 71 | N/A | Individual CBT Group therapy | 6 weeks | Serum BDNF | Increase in BDNF levels, improvement in sleep, depressive symptoms, emotional exhaustion, and depersonalization, but not personal efficacy and parasympathetic activity |
| Study | Age | Sex | Physical Activity | Meditation | Pharmacotherapy | Supplements | Comorbidity |
|---|---|---|---|---|---|---|---|
| Koch et al. (2009) [45] | + | + | − | − | + | − | + * |
| Yamada et al. (2012) [46] | + | + | − | − | + | − | + |
| Perroud et al. (2013) [47] | + | + | − | − | + | − | − |
| Zwipp et al. (2014) [48] | + | + | − | − | + | − | + |
| Powers et al. (2015) [49] | − | − | + | − | + | − | + |
| Rusch et al. (2015) [50] | + | + | − | − | + | − | + |
| Da Silva et al. (2018) [52] | + | + | − | − | + | − | + |
| Bruijniks et al. (2020) [53] | + | + | − | − | + | − | + |
| Orosz et al. (2020) [54] | + | + | − | − | + | − | + * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piotrkowicz, M.; Janoska-Jazdzik, M.; Koweszko, T.; Szulc, A. The Influence of Psychotherapy on Peripheral Brain-Derived Neurotrophic Factor Concentration Levels and Gene Methylation Status: A Systematic Review. J. Clin. Med. 2021, 10, 4424. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194424
Piotrkowicz M, Janoska-Jazdzik M, Koweszko T, Szulc A. The Influence of Psychotherapy on Peripheral Brain-Derived Neurotrophic Factor Concentration Levels and Gene Methylation Status: A Systematic Review. Journal of Clinical Medicine. 2021; 10(19):4424. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194424
Chicago/Turabian StylePiotrkowicz, Michal, Marlena Janoska-Jazdzik, Tytus Koweszko, and Agata Szulc. 2021. "The Influence of Psychotherapy on Peripheral Brain-Derived Neurotrophic Factor Concentration Levels and Gene Methylation Status: A Systematic Review" Journal of Clinical Medicine 10, no. 19: 4424. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194424