
Acupuncture Treatment Associated with Functional Connectivity Changes in Primary Dysmenorrhea: A Resting State fMRI Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Acupuncture Intervention
2.4. Menstrual Pain Experience and Psychological Assessments
2.5. Measurement of Blood Gonadal Hormone Level
2.6. Image Acquisition
2.7. Image Preprocessing
2.8. Statistical Analysis
3. Results
3.1. Demographic Data and General PDM Experience
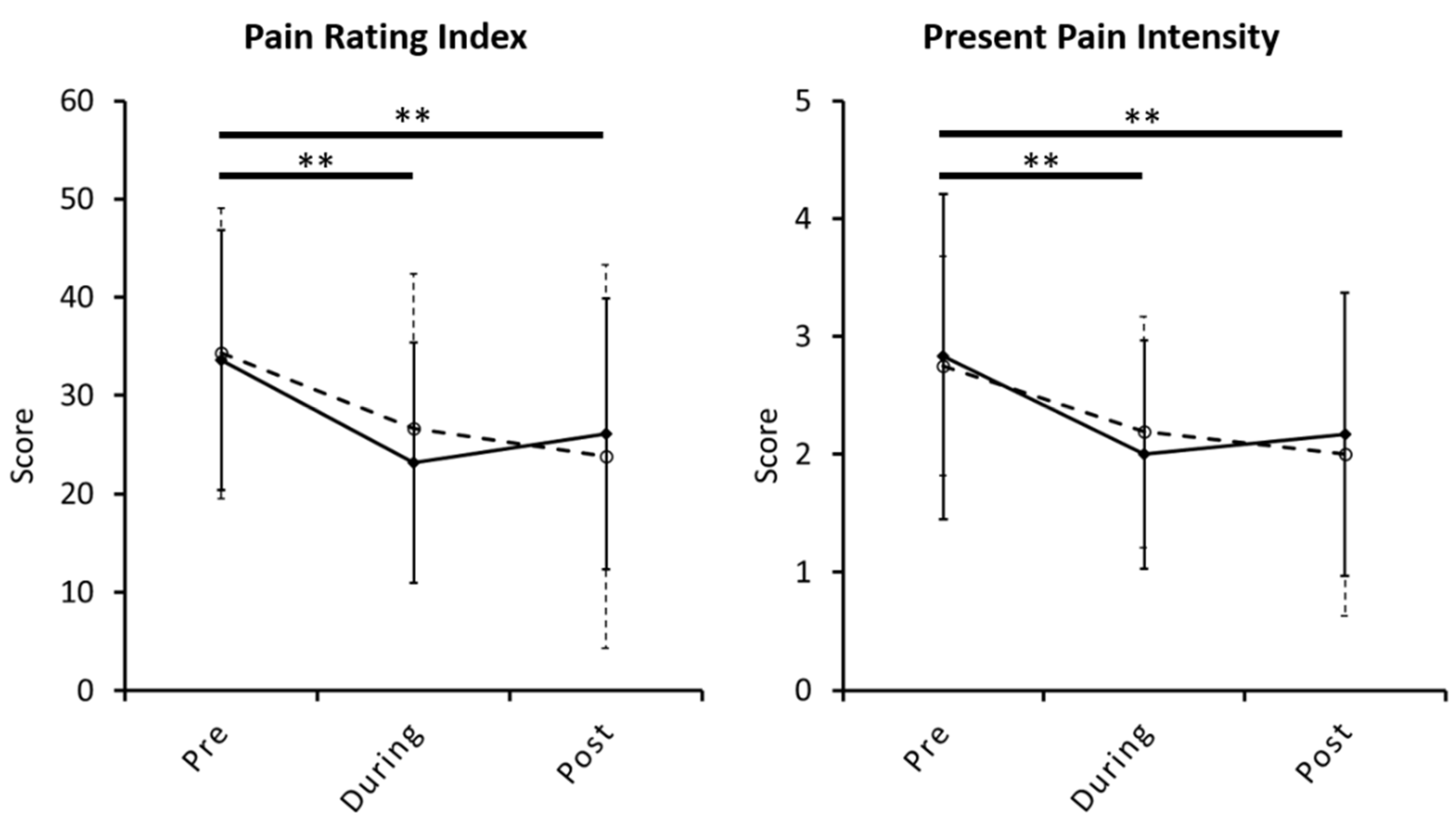
3.2. Changes in Menstrual Pain Experience, Psychological Assessment, and Gonadal Hormone Level across Acupuncture Intervention
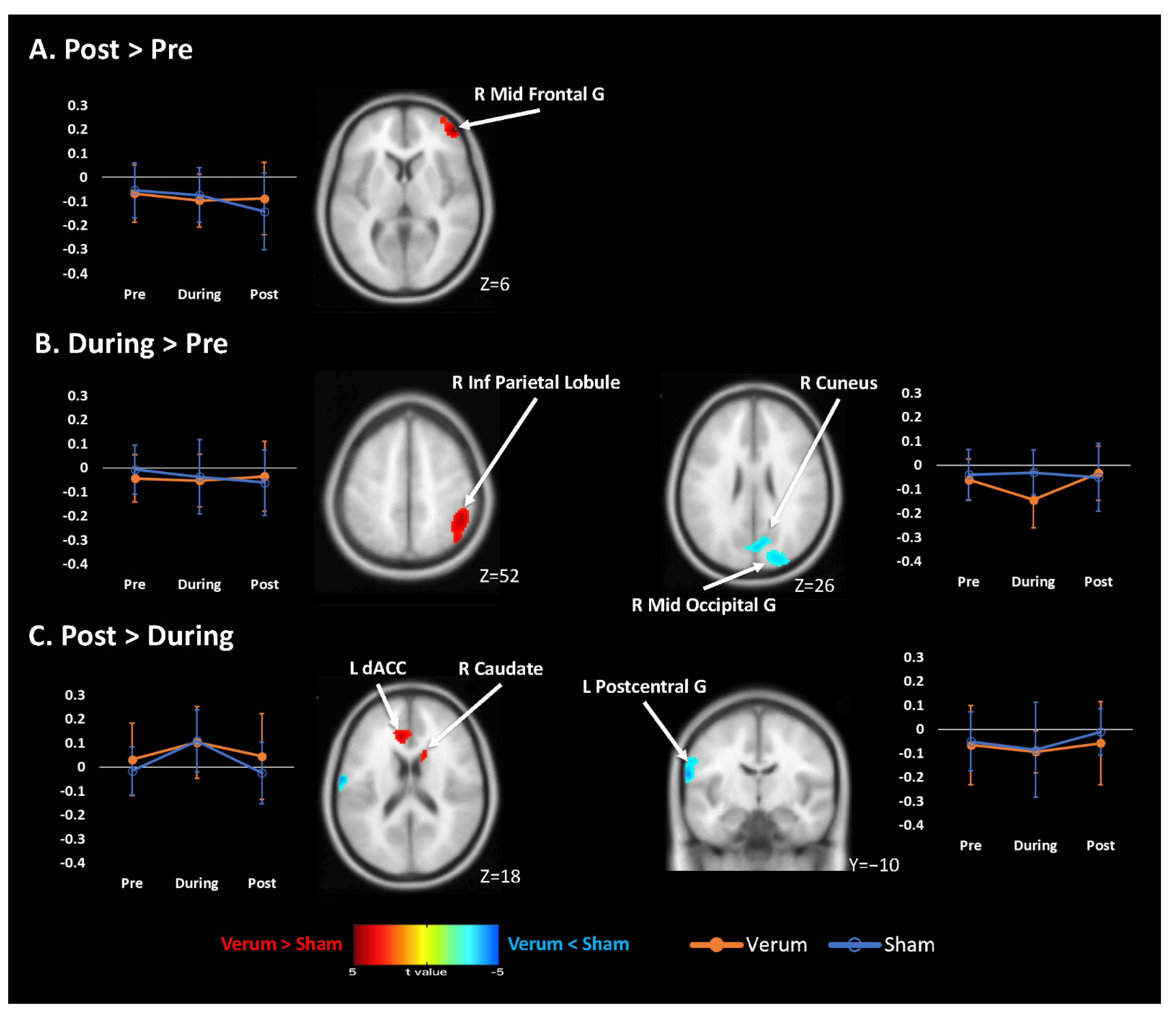
3.3. Changes in FC Maps across Acupuncture Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- French, L. Dysmenorrhea. Am. Fam. Physicians 2005, 71, 285–291. [Google Scholar]
- Dawood, M.Y. Primary dysmenorrhea: Advances in pathogenesis and management. Obstet. Gynecol. 2006, 108, 428–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajaj, P.; Madsen, H.; Arendt-Nielsen, L. A comparison of modality-specific somatosensory changes during menstruation in dysmenorrheic and nondysmenorrheic women. Clin. J. Pain 2002, 18, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Granot, M.; Yarnitsky, D.; Itskovitz-Eldor, J.; Granovsky, Y.; Peer, E.; Zimmer, E.Z. Pain perception in women with dysmenorrhea. Obstet. Gynecol 2001, 98, 407–411. [Google Scholar]
- Tu, C.H.; Niddam, D.M.; Chao, H.T.; Chen, L.F.; Chen, Y.S.; Wu, Y.T.; Yeh, T.C.; Lirng, J.F.; Hsieh, J.C. Brain morphological changes associated with cyclic menstrual pain. Pain 2010, 150, 462–468. [Google Scholar] [CrossRef]
- Tu, C.H.; Niddam, D.M.; Chao, H.T.; Liu, R.S.; Hwang, R.J.; Yeh, T.C.; Hsieh, J.C. Abnormal cerebral metabolism during menstrual pain in primary dysmenorrhea. Neuroimage 2009, 47, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Y.; Chao, H.T.; Tu, C.H.; Li, W.C.; Low, I.; Chuang, C.Y.; Chen, L.F.; Hsieh, J.C. Changes in functional connectivity of pain modulatory systems in women with primary dysmenorrhea. Pain 2016, 157, 92–102. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Acupuncture: Review and Analysis of Reports on Controlled Clinical Trials; World Health Organization: Geneva, Switzerland, 2003; p. 81. [Google Scholar]
- Woo, H.L.; Ji, H.R.; Pak, Y.K.; Lee, H.; Heo, S.J.; Lee, J.M.; Park, K.S. The efficacy and safety of acupuncture in women with primary dysmenorrhea: A systematic review and meta-analysis. Medicine (Baltimore) 2018, 97, e11007. [Google Scholar] [CrossRef]
- Yu, Y.P.; Ma, L.X.; Ma, Y.X.; Ma, Y.X.; Liu, Y.Q.; Liu, C.Z.; Xie, J.P.; Gao, S.Z.; Zhu, J. Immediate effect of acupuncture at Sanyinjiao (SP6) and Xuanzhong (GB39) on uterine arterial blood flow in primary dysmenorrhea. J. Altern. Complement. Med. 2010, 16, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.X.; Liu, C.Z.; Zhu, J.; Guan, L.P.; Wang, D.J.; Wu, M.M. Effects of acupuncture at Sanyinjiao (SP6) on prostaglandin levels in primary dysmenorrhea patients. Clin. J. Pain 2011, 27, 258–261. [Google Scholar] [CrossRef]
- Lin, J.G.; Chen, W.L. Acupuncture analgesia: A review of its mechanisms of actions. Am. J. Chin. Med. 2008, 36, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Raecke, R.; Niemeier, A.; Ihle, K.; Ruether, W.; May, A. Brain gray matter decrease in chronic pain is the consequence and not the cause of pain. J. Neurosci. 2009, 29, 13746–13750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teutsch, S.; Herken, W.; Bingel, U.; Schoell, E.; May, A. Changes in brain gray matter due to repetitive painful stimulation. Neuroimage 2008, 42, 845–849. [Google Scholar] [CrossRef]
- Bingel, U.; Herken, W.; Teutsch, S.; May, A. Habituation to painful stimulation involves the antinociceptive system--a 1-year follow-up of 10 participants. Pain 2008, 140, 393–394. [Google Scholar] [CrossRef]
- Yang, N.; Waddington, G.; Adams, R.; Han, J. Translation, cultural adaption, and test-retest reliability of Chinese versions of the Edinburgh Handedness Inventory and Waterloo Footedness Questionnaire. Laterality 2018, 23, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.C.; Wen, X.Y.; Jiang, L.; Xie, M.J.; Fu, W.B. Validity of the “streitberger” needle in a chinese population with acupuncture: A randomized, single-blinded, and crossover pilot study. Evid. Based Complement. Altern. Med. 2013, 2013, 251603. [Google Scholar] [CrossRef]
- Streitberger, K.; Kleinhenz, J. Introducing a placebo needle into acupuncture research. Lancet 1998, 352, 364–365. [Google Scholar] [CrossRef]
- Hui, Y.L.; Chen, A.C. Analysis of headache in a Chinese patient population. Ma Zui Xue Za Zhi 1989, 27, 13–18. [Google Scholar]
- Wu, P.C.; Huang, T.W. Gender-related invariance of the Beck Depression Inventory II for Taiwanese adolescent samples. Assessment 2014, 21, 218–226. [Google Scholar] [CrossRef]
- Ma, W.F.; Liu, Y.C.; Chen, Y.F.; Lane, H.Y.; Lai, T.J.; Huang, L.C. Evaluation of psychometric properties of the Chinese Mandarin version State-Trait Anxiety Inventory Y form in Taiwanese outpatients with anxiety disorders. J. Psychiatr. Ment. Health Nurs. 2013, 20, 499–507. [Google Scholar] [CrossRef]
- Yan, C.G.; Wang, X.D.; Zuo, X.N.; Zang, Y.F. DPABI: Data Processing & Analysis for (Resting-State) Brain Imaging. Neuroinformatics 2016, 14, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Keuken, M.C.; Forstmann, B.U. A probabilistic atlas of the basal ganglia using 7 T MRI. Data Brief 2015, 4, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cremers, H.R.; Wager, T.D.; Yarkoni, T. The relation between statistical power and inference in fMRI. PLoS ONE 2017, 12, e0184923. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Larrea, L.; Peyron, R. Pain matrices and neuropathic pain matrices: A review. Pain 2013, 154, S29–S43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Symonds, L.L.; Gordon, N.S.; Bixby, J.C.; Mande, M.M. Right-lateralized pain processing in the human cortex: An FMRI study. J. Neurophysiol. 2006, 95, 3823–3830. [Google Scholar] [CrossRef]
- Coghill, R.C.; Gilron, I.; Iadarola, M.J. Hemispheric lateralization of somatosensory processing. J. Neurophysiol. 2001, 85, 2602–2612. [Google Scholar] [CrossRef] [PubMed]
- Villemure, C.; Bushnell, M.C. Mood influences supraspinal pain processing separately from attention. J. Neurosci. 2009, 29, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Kong, J.; Kaptchuk, T.J.; Webb, J.M.; Kong, J.T.; Sasaki, Y.; Polich, G.R.; Vangel, M.G.; Kwong, K.; Rosen, B.; Gollub, R.L. Functional neuroanatomical investigation of vision-related acupuncture point specificity—A multisession fMRI study. Hum. Brain Mapp. 2009, 30, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.H.; Cho, S.Y.; Jahng, G.H.; Ryu, C.W.; Park, S.U.; Ko, C.N.; Park, J.M. Differential Localization of Pain-Related and Pain-Unrelated Neural Responses for Acupuncture at BL60 Using BOLD fMRI. Evid.-Based Complement. Altern. Med. 2013, 2013, 804696. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Zeng, F.; Yin, T.; Lan, L.; Makris, N.; Jorgenson, K.; Guo, T.; Wu, F.; Gao, Y.; Dong, M.; et al. Acupuncture modulates the abnormal brainstem activity in migraine without aura patients. Neuroimage Clin. 2017, 15, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Frangos, E.; Ceko, M.; Wang, B.; Richards, E.A.; Gracely, J.L.; Colloca, L.; Schweinhardt, P.; Bushnell, M.C. Neural effects of placebo analgesia in fibromyalgia patients and healthy individuals. Pain 2021, 162, 641–652. [Google Scholar] [CrossRef]
- Jahn, A.; Nee, D.E.; Alexander, W.H.; Brown, J.W. Distinct Regions within Medial Prefrontal Cortex Process Pain and Cognition. J. Neurosci. 2016, 36, 12385–12392. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, M.D.; Eisenberger, N.I. The dorsal anterior cingulate cortex is selective for pain: Results from large-scale reverse inference. Proc. Natl. Acad. Sci. USA 2015, 112, 15250–15255. [Google Scholar] [CrossRef] [Green Version]
- Shyu, B.C.; Sikes, R.W.; Vogt, L.J.; Vogt, B.A. Nociceptive processing by anterior cingulate pyramidal neurons. J. Neurophysiol. 2010, 103, 3287–3301. [Google Scholar] [CrossRef] [PubMed]
- Wager, T.D.; Scott, D.J.; Zubieta, J.K. Placebo effects on human mu-opioid activity during pain. Proc. Natl. Acad. Sci. USA 2007, 104, 11056–11061. [Google Scholar] [CrossRef] [Green Version]
- Bian, Y.; He, X.; Hu, S.; Li, C.; Xu, C.; Kan, H.; Xue, Q.; Yang, J.; Qiu, B. Functional Connectivity Modulation by Acupuncture in Patients with Bell’s Palsy. Evid.-Based Complement. Altern. Med. 2016, 2016, 5928758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eippert, F.; Bingel, U.; Schoell, E.D.; Yacubian, J.; Klinger, R.; Lorenz, J.; Buchel, C. Activation of the opioidergic descending pain control system underlies placebo analgesia. Neuron 2009, 63, 533–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiech, K.; Kalisch, R.; Weiskopf, N.; Pleger, B.; Stephan, K.E.; Dolan, R.J. Anterolateral prefrontal cortex mediates the analgesic effect of expected and perceived control over pain. J. Neurosci. 2006, 26, 11501–11509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wager, T.D.; Rilling, J.K.; Smith, E.E.; Sokolik, A.; Casey, K.L.; Davidson, R.J.; Kosslyn, S.M.; Rose, R.M.; Cohen, J.D. Placebo-induced changes in FMRI in the anticipation and experience of pain. Science 2004, 303, 1162–1167. [Google Scholar] [CrossRef]
- Wager, T.D.; Atlas, L.Y. The neuroscience of placebo effects: Connecting context, learning and health. Nat. Rev. Neurosci. 2015, 16, 403–418. [Google Scholar] [CrossRef]
- Vachon-Presseau, E.; Berger, S.E.; Abdullah, T.B.; Huang, L.; Cecchi, G.A.; Griffith, J.W.; Schnitzer, T.J.; Apkarian, A.V. Brain and psychological determinants of placebo pill response in chronic pain patients. Nat. Commun. 2018, 9, 3397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, J.C.; Faull, O.K.; Pattinson, K.T.; Jenkinson, M. Physiological noise in brainstem FMRI. Front. Hum. Neurosci. 2013, 7, 623. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Verum (N = 18) | Sham (N = 16) | p-Value | |
|---|---|---|---|
| Age (year) | 24.89 ± 4.59 | 26.13 ± 4.54 | 0.44 |
| Headedness (−1~1) | 0.84 ± 0.16 | 0.91 ± 0.17 | 0.23 |
| The age of menarche (year) | 11.72 ± 1.36 | 11.88 ± 1.36 | 0.75 |
| Gynecologic age (year) | 13.17 ± 4.78 | 14.25 ± 4.81 | 0.52 |
| Length of menstrual cycle (day) | 31.06 ± 2.34 | 30.06 ± 1.95 | 0.19 |
| The age of dysmenorrhea onset (year) | 14.50 ± 2.73 | 14.69 ± 2.77 | 0.84 |
| Dysmenorrhea history (year) | 10.39 ± 5.80 | 11.44 ± 5.46 | 0.59 |
| The duration of menstrual pain per cycle (day) | 1.89 ± 0.68 | 1.63 ± 0.62 | 0.25 |
| MPQ | |||
| PRI (0~78) | 35.83 ± 13.28 | 36.31 ± 12.14 | 0.91 |
| PPI (0~5) | 3.17 ± 1.20 | 3.25 ± 1.00 | 0.83 |
| Verum (N = 18) | Sham (N = 16) | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | During | Post | Pre | During | Post | Interaction | Group | Time | |
| MPQ | |||||||||
| PRI total (0~78) | 33.61 ± 13.22 | 23.17 ± 12.20 | 26.11 ± 13.79 | 34.31 ± 14.78 | 26.69 ± 15.70 | 23.81 ± 19.46 | 0.52 | 0.88 | 0.001 #& |
| PPI (0~5) | 2.83 ± 1.38 | 2.00 ± 0.97 | 2.17 ± 1.20 | 2.75 ± 0.93 | 2.19 ± 0.98 | 2.00 ± 1.37 | 0.77 | 0.94 | 0.009 #& |
| BDI | 8.11 ± 6.33 | 7.89 ± 5.80 | 7.72 ± 9.41 | 10.69 ± 9.51 | 6.38 ± 3.65 | 7.63 ± 5.77 | 0.32 | 0.86 | 0.23 |
| STAI | |||||||||
| State (20~80) | 43.17 ± 8.96 | 41.67 ± 7.30 | 40.78 ± 10.94 | 43.38 ± 9.98 | 43.13 ± 8.88 | 40.81 ± 9.30 | 0.89 | 0.83 | 0.29 |
| Trait (20~80) | 47.33 ± 7.22 | 45.61 ± 4.05 | 45.72 ± 10.01 | 46.94 ± 9.77 | 45.06 ± 8.95 | 43.56 ± 9.63 | 0.76 | 0.68 | 0.15 |
| Hormones | |||||||||
| Estradiol (pg/mL) | 87.89 ± 73.90 | 63.44 ± 30.63 | 116.28 ± 108.75 | 77.69 ± 57.44 | 94.63 ± 63.10 | 117.44 ± 81.97 | 0.45 | 0.65 | 0.05 |
| Progesterone (ng/mL) | 2.77 ± 4.47 | 0.75 ± 1.29 | 2.67 ± 5.11 | 1.23 ± 2.61 | 2.26 ± 4.70 | 2.77 ± 4.12 | 0.24 | 0.98 | 0.40 |
| Testosterone (ng/mL) | 0.52 ± 0.28 | 0.58 ± 0.28 | 0.64 ± 0.27 | 0.51 ± 0.15 | 0.49 ± 0.15 | 0.51 ± 0.41 | 0.05 | 0.32 | 0.05 |
| Verum > Sham | Verum < Sham | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coordinate | Coordinate | ||||||||||||
| Anatomical Area | BA | Size | t-max | x | y | z | Anatomical Area | BA | Size | t-max | x | y | z |
| Post > Pre | |||||||||||||
| R Mid Frontal G | 46/10 | 622 | 4.71 | 50 | 50 | 6 | n.s. | ||||||
| During > Pre | |||||||||||||
| R Inf Parietal Lob | 40/39/7 | 1030 | 4.12 | 48 | −46 | 52 | R Mid Occipital G | 19 | 1153 | 4.23 | 32 | −88 | 14 |
| R Cuneus | 18 | 3.55 | 4 | −76 | 26 | ||||||||
| Post > During | |||||||||||||
| L dACC | 24 | 433 | 3.92 | −8 | 32 | 16 | L Postcentral G | 43 | 483 | 4.16 | −64 | −8 | 20 |
| R Caudate N | 3.22 | 14 | 16 | 18 | L Precentral G | 6 | 3.86 | −60 | −4 | 30 | |||
| L Sup Temporal G | 42 | 3.42 | −68 | −22 | 10 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tu, C.-H.; Lee, Y.-C.; Chen, Y.-Y.; Chen, C.-M.; Lu, W.-C.; Chen, Y.-H.; Yang, S.-T. Acupuncture Treatment Associated with Functional Connectivity Changes in Primary Dysmenorrhea: A Resting State fMRI Study. J. Clin. Med. 2021, 10, 4731. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204731
Tu C-H, Lee Y-C, Chen Y-Y, Chen C-M, Lu W-C, Chen Y-H, Yang S-T. Acupuncture Treatment Associated with Functional Connectivity Changes in Primary Dysmenorrhea: A Resting State fMRI Study. Journal of Clinical Medicine. 2021; 10(20):4731. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204731
Chicago/Turabian StyleTu, Cheng-Hao, Yu-Chen Lee, Ying-Yu Chen, Chun-Ming Chen, Wen-Chi Lu, Yi-Hung Chen, and Su-Tso Yang. 2021. "Acupuncture Treatment Associated with Functional Connectivity Changes in Primary Dysmenorrhea: A Resting State fMRI Study" Journal of Clinical Medicine 10, no. 20: 4731. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204731