
Prevalence of Neural Autoantibodies in Paired Serum and Cerebrospinal Fluid in Adult Patients with Drug-Resistant Temporal Lobe Epilepsy of Unknown Etiology

 ,
,  ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Patients
2.3. Protocol
2.4. Prevalence of Neural Autoantibodies
2.5. Baseline Characteristics
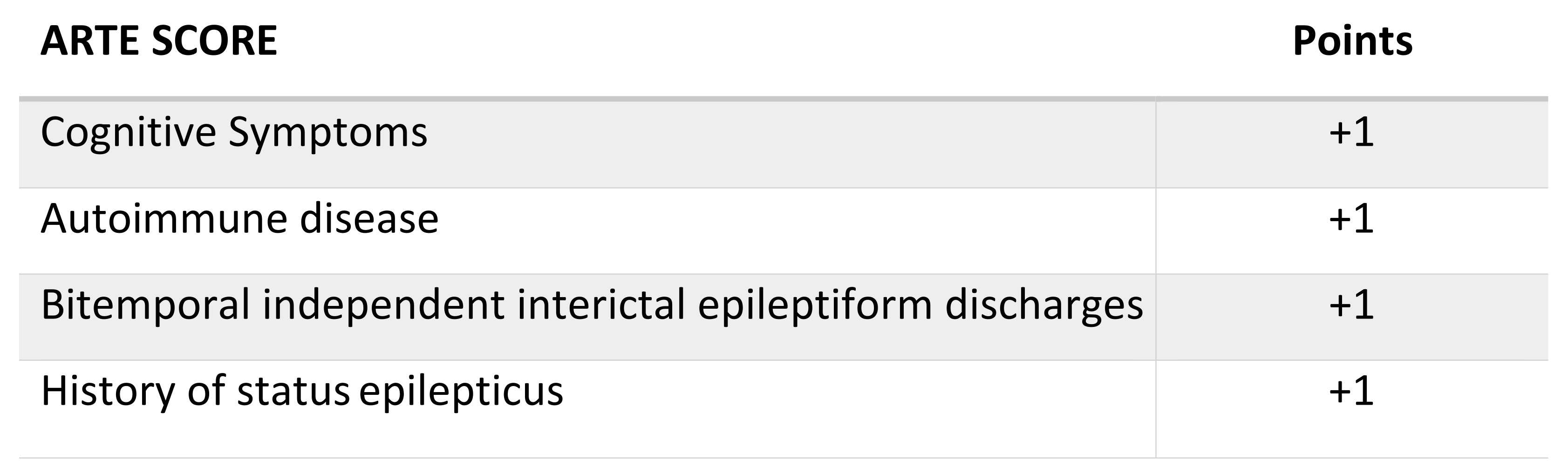
2.6. Antibody Prevalence Scores
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics and the Frequency of Neural Autoantibodies
3.2. Neural Autoantibodies Profile
3.3. Sensitivity and Specificity of Antibody Predictive Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshé, S.L.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [Green Version]
- Geis, C.; Planagumà, J.; Carreño, M.; Graus, F.; Dalmau, J. Autoimmune seizures and epilepsy. J. Clin. Investig. 2019, 129, 926–940. [Google Scholar] [CrossRef] [Green Version]
- Steriade, C.; Britton, J.; Dale, R.C.; Gadoth, A.; Irani, S.R.; Linnoila, J.; McKeon, A.; Shao, X.-Q.; Venegas, V.; Bien, C.G.; et al. Acute symptomatic seizures secondary to autoimmune encephalitis and autoimmune-associated epilepsy: Conceptual definitions. Epilepsia 2020, 61, 1341–1351. [Google Scholar] [CrossRef]
- Kuehn, J.C.; Meschede, C.; Helmstaedter, C.; Surges, R.; von Wrede, R.; Hattingen, E.; Vatter, H.; Elger, C.E.; Schoch, S.; Becker, A.J.; et al. Adult-onset temporal lobe epilepsy suspicious for autoimmune pathogenesis: Autoantibody prevalence and clinical correlates. PLoS ONE 2020, 15, e0241289. [Google Scholar] [CrossRef]
- Zhang, W.; Bu, H.; Li, Y.; Han, X.; He, J.; Jia, L.; Wang, W. Development and validation of a predictive model for the diagnosis of neural antibody-mediated epilepsy/ seizure in patients with new-onset seizure or established epilepsy. Seizure 2020, 83, 5–12. [Google Scholar] [CrossRef]
- Cabezudo-García, P.; Mena-Vázquez, N.; Ciano-Petersen, N.L.; García-Martín, G.; Estivill-Torrús, G.; Serrano-Castro, P.J. Prevalence of neural autoantibodies in epilepsy of unknown etiology: Systematic review and meta-analysis. Brain Sci. 2021, 11, 392. [Google Scholar] [CrossRef]
- Graus, F.; Titulaer, M.J.; Balu, R.; Benseler, S.; Bien, C.G.; Cellucci, T.; Cortese, I.; Dale, R.C.; Gelfand, J.M.; Geschwind, M.; et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016, 15, 391–404. [Google Scholar] [CrossRef] [Green Version]
- Dubey, D.; Pittock, S.J.; McKeon, A. Antibody Prevalence in Epilepsy and Encephalopathy score: Increased specificity and applicability. Epilepsia 2019, 60, 367–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Tymchuk, S.; Barry, J.; Muppidi, S.; Le, S. Antibody Prevalence in Epilepsy before Surgery (APES) in drug-resistant focal epilepsy. Epilepsia 2021, 62, 720–728. [Google Scholar] [CrossRef] [PubMed]
- de Bruijn, M.A.A.M.; Bastiaansen, A.E.M.; Mojzisova, H.; van Sonderen, A.; Thijs, R.D.; Majoie, M.J.M.; Rouhl, R.P.W.; van Coevorden-Hameete, M.H.; de Vries, J.M.; Lopetegi, A.M.; et al. Antibodies Contributing to Focal Epilepsy Signs and Symptoms Score. Ann. Neurol. 2021, 89, 698–710. [Google Scholar] [CrossRef] [PubMed]
- Dubey, D.; Alqallaf, A.; Hays, R.; Freeman, M.; Chen, K.; Ding, K.; Agostini, M.; Vernino, S. Neurological autoantibody prevalence in epilepsy of unknown etiology. JAMA Neurol. 2017, 74, 397–402. [Google Scholar] [CrossRef]
- Sultana, B.; Panzini, M.A.; Veilleux Carpentier, A.; Comtois, J.; Rioux, B.; Gore, G.; Bauer, P.R.; Kwon, C.-S.; Jetté, N.; Josephson, C.B.; et al. Incidence and Prevalence of Drug-Resistant Epilepsy: A Systematic Review and Meta-analysis. Neurology 2021, 96, 805–817. [Google Scholar] [CrossRef]
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E.; Engel, J., Jr.; Forsgren, L.; French, J.A.; Glynn, M.; et al. ILAE Official Report: A practical clinical definition of epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Bernasconi, A.; Cendes, F.; Theodore, W.H.; Gill, R.S.; Koepp, M.J.; Hogan, R.E.; Jackson, G.D.; Federico, P.; Labate, A.; Vaudano, A.E.; et al. Recommendations for the use of structural magnetic resonance imaging in the care of patients with epilepsy: A consensus report from the International League Against Epilepsy Neuroimaging Task Force. Epilepsia 2019, 60, 1054–1068. [Google Scholar] [CrossRef] [PubMed]
- Kwan, P.; Arzimanoglou, A.; Berg, A.T.; Brodie, M.J.; Hauser, W.A.; Mathern, G.; Moshé, S.L.; Perucca, E.; Wiebe, S.; French, J.; et al. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 2010, 51, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Bien, C.G.; Elger, C.E. Limbic encephalitis: A cause of temporal lobe epilepsy with onset in adult life. Epilepsy Behav. 2007, 10, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Husari, K.S.; Dubey, D. Autoimmune Epilepsy. Neurotherapeutics 2019, 16, 685–702. [Google Scholar]
- Graus, F.; Saiz, A.; Dalmau, J. GAD antibodies in neurological disorders—Insights and challenges. Nat. Rev. Neurol. 2020, 16, 353–365. [Google Scholar] [CrossRef]
- Trinka, E.; Cock, H.; Hesdorffer, D.; Rossetti, A.O.; Scheffer, I.E.; Shinnar, S.; Shorvon, S.; Lowenstein, D.H. A definition and classification of status epilepticus—Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia 2015, 56, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Cabezudo-García, P.; Mena-Vázquez, N.; Villagrán-García, M.; Serrano-Castro, P.J. Efficacy of antiepileptic drugs in autoimmune epilepsy: A systematic review. Seizure 2018, 59, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Kelley, B.P.; Patel, S.C.; Marin, H.L.; Corrigan, J.J.; Mitsias, P.D.; Griffith, B. Autoimmune encephalitis: Pathophysiology and imaging review of an overlooked diagnosis. Am. J. Neuroradiol. 2017, 38, 1070–1078. [Google Scholar] [CrossRef] [Green Version]
- Steriade, C.; Gillinder, L.; Rickett, K.; Hartel, G.; Higdon, L.; Britton, J.; French, J. Discerning the Role of Autoimmunity and Autoantibodies in Epilepsy: A Review. JAMA Neurol. 2021. [Google Scholar] [CrossRef]
- Casciato, S.; Morano, A.; Fattouch, J.; Fanella, M.; Avorio, F.; Albini, M.; Basili, L.M.; Irelli, E.C.; Viganò, A.; Risi, M.D.; et al. Factors underlying the development of chronic temporal lobe epilepsy in autoimmune encephalitis. J. Neurol. Sci. 2019, 396, 102–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruijn, M.A.A.M.; Van Sonderen, A.; Van Coevorden-Hameete, M.H.; Bastiaansen, A.E.M.; Schreurs, M.W.J.; Rouhl, R.P.W.; van Donselaar, C.A.; Majoie, M.H.J.M.; Neuteboom, R.F.; Sillevis Smitt, P.A.E.; et al. Evaluation of seizure treatment in anti-LGI1, anti-NMDAR, and anti-GABABR encephalitis. Neurology 2019, 92, E2185–E2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaspard, N.; Foreman, B.P.; Alvarez, V.; Cabrera Kang, C.; Probasco, J.C.; Jongeling, A.C.; Meyers, E.; Espinera, A.; Haas, K.F.; Schmitt, S.E.; et al. New-onset refractory status epilepticus: Etiology, clinical features, and outcome. Neurology 2015, 85, 1604–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sculier, C.; Gaínza-Lein, M.; Sánchez Fernández, I.; Loddenkemper, T. Long-term outcomes of status epilepticus: A critical assessment. Epilepsia 2018, 59, 155–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armangue, T.; Spatola, M.; Vlagea, A.; Mattozzi, S.; Cárceles-Cordon, M.; Martinez-Heras, E.; Llufriu, S.; Muchart, J.; Erro, M.E.; Abraira, L.; et al. Spanish Herpes Simplex Encephalitis Study Group. Frequency, symptoms, risk factors, and outcomes of autoimmune encephalitis after herpes simplex encephalitis: A prospective observational study and retrospective analysis. Lancet Neurol. 2018, 17, 760–772. [Google Scholar] [PubMed] [Green Version]
- Javidi, E.; Magnus, T. Autoimmunity After Ischemic Stroke and Brain Injury. Front. Immunol. 2019, 10, 686. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | Anti-Neural Positive n = 14 | Anti-Neural Negative n = 13 | p-Value |
|---|---|---|---|
| Female sex, n (%) | 9 (64.3%) | 8 (61.5%) | 0.883 |
| Epilepsy onset age in years, mean (SD) | 34.1 (17.1) | 31.2 (17.7) | 0.672 |
| Age in years, mean (SD) | 51.5 (15.3) | 52.7 (13.5) | 0.829 |
| Epilepsy duration years, mean (SD) | 17.2 (11.2) | 21.3 (14.0) | 0.410 |
| Aseptic meningoencephalitis, n (%) | 1 (7.1%) | 0 (0.0%) | 0.326 |
| Autoimmune disease, n (%) | 6 (42.9%) | 2 (15.4%) | 0.118 |
| Neuropsychiatric changes, n (%) | 7 (50.0%) | 4 (30.8%) | 0.310 |
| Cognitive symptoms, n (%) | 9 (64.3%) | 5 (38.5%) | 0.180 |
| Dysautonomia, n (%) | 1 (7.1%) | 0 (0.0%) | 0.326 |
| Speech problems, n (%) | 2 (14.3%) | 1 (7.7%) | 0.586 |
| Epilepsy Surgery, n (%) | 1 (7.1%) | 1 (7.7%) | 0.957 |
| Status epilepticus, n (%) | 6 (42.9%) | 0 (0.0%) | 0.007 |
| Number of AEDs, mean (SD) | 2.4 (1.0) | 2.4 (0.9) | 0.932 |
| Focal seizures without IA, n (%) | 8 (57.1%) | 5 (38.5%) | 0.332 |
| Focal seizures with IA, n (%) | 12 (85.7%) | 13 (100%) | 0.157 |
| GTC seizures, n (%) | 11 (78.6%) | 8 (68.5%) | 0.333 |
| Autonomic seizures, n (%) | 5 (35.71%) | 3 (23.1%) | 0.472 |
| Bitemporal independent interictal discharges, n (%) | 8 (57.1%) | 2 (15.4%) | 0.025 |
| Performed vEEG, n (%) | 6 (42.9%) | 7 (53.8%) | 0.568 |
| CSF inflammation, n (%) | 4 (28.6%) | 1 (7.7%) | 0.163 |
| Specific OGB, n (%) | 1 (7.7%) | 1 (8.3%) | 0.953 |
| Hippocampal sclerosis, n (%) | 0 (0.0%) | 2 (15.4%) | 0.127 |
| Positive Patients | Serum | CSF | APE2 Score | APES Score | ACES Score | ARTE Score |
|---|---|---|---|---|---|---|
| Patient 1 | GAD65 + NMDAR | - | 2 | 4 | 1 | 1 |
| Patient 2 | LGI1 | - | 3 | 5 | 2 | 2 |
| Patient 3 | AMPAR | AMPAR | 2 | 3 | 1 | 1 |
| Patient 4 | CV2 | - | 2 | 4 | 1 | 3 |
| Patient 5 | LGI1 | - | 2 | 3 | 1 | 3 |
| Patient 6 | GAD65 | - | 4 | 3 | 2 | 1 |
| Patient 7 | NMDAR | - | 3 | 3 | 2 | 3 |
| Patient 8 | GABABR | - | 3 | 2 | 3 | 2 |
| Patient 9 | NMDAR | - | 4 | 4 | 3 | 2 |
| Patient 10 | - | DPPX | 2 | 3 | 2 | 3 |
| Patient 11 | - | DPPX | 4 | 4 | 3 | 4 |
| Patient 12 | AMPAR | AMPAR | 3 | 3 | 0 | 1 |
| Patient 13 | NMDAR | - | 3 | 3 | 2 | 2 |
| Patient 14 | LGI1 + DPPX + GABABR | 3 | 2 | 2 | 1 |
| Cutoff | N (%) | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|
| ≥1 points | 21 (77.7) | 100% (76.8–100) | 46.1% (19.2–74.8) | 66.6% (54.7–76.7) | 100% |
| ≥2 points | 11 (40.7) | 64.2% (35.1–87.2) | 84.6% (54.5–98.0) | 81.8% (54.2–94.4) | 68.7% (51.2–82.1) |
| ≥3 points | 5 (18.5) | 35.7% (12.7–64.8) | 100% (75.2–100) | 100% | 66.6% (46.0–83.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabezudo-García, P.; Ciano-Petersen, N.L.; Mena-Vázquez, N.; Ortega-Pinazo, J.; Postigo-Pozo, M.J.; García-Martín, G.; Antolí-Martínez, H.; Sánchez-Sánchez, V.; Quiroga-Subirana, P.; Serrano-Castro, P.J.; et al. Prevalence of Neural Autoantibodies in Paired Serum and Cerebrospinal Fluid in Adult Patients with Drug-Resistant Temporal Lobe Epilepsy of Unknown Etiology. J. Clin. Med. 2021, 10, 4843. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10214843
Cabezudo-García P, Ciano-Petersen NL, Mena-Vázquez N, Ortega-Pinazo J, Postigo-Pozo MJ, García-Martín G, Antolí-Martínez H, Sánchez-Sánchez V, Quiroga-Subirana P, Serrano-Castro PJ, et al. Prevalence of Neural Autoantibodies in Paired Serum and Cerebrospinal Fluid in Adult Patients with Drug-Resistant Temporal Lobe Epilepsy of Unknown Etiology. Journal of Clinical Medicine. 2021; 10(21):4843. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10214843
Chicago/Turabian StyleCabezudo-García, Pablo, Nicolás L. Ciano-Petersen, Natalia Mena-Vázquez, Jesús Ortega-Pinazo, María J. Postigo-Pozo, Guillermina García-Martín, Helena Antolí-Martínez, Violeta Sánchez-Sánchez, Pablo Quiroga-Subirana, Pedro J. Serrano-Castro, and et al. 2021. "Prevalence of Neural Autoantibodies in Paired Serum and Cerebrospinal Fluid in Adult Patients with Drug-Resistant Temporal Lobe Epilepsy of Unknown Etiology" Journal of Clinical Medicine 10, no. 21: 4843. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10214843