1. Introduction
The novel Coronavirus Disease 2019 (COVID-19), which was officially announced as a pandemic more than one year ago (11 March 2020), remains a huge challenge, particularly for frontline workers, having a significant impact not only on the physical, but also on the mental health of the entire population [
1]. According to current global statistics, there are more than 233 million confirmed cases, along with a total number of more than 4 million deaths worldwide, while in Poland there are more than 2 million confirmed cases and more than 75 thousand deaths confirmed (as of 3 October 2021, the World Health Organization (WHO)) [
2]. The very wide spectrum of clinical manifestations, as well as the long-term effects associated with the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection, has continually aroused concern and anxiety among the public [
3].
Like many countries [
4,
5,
6,
7], Poland has implemented certain relatively effective restrictions to gain control of the pandemic. A sudden outbreak of COVID-19 has forced the government to introduce certain restrictions to prevent viral transmission and minimize the risk of potential infections. In Poland, the lockdown was announced on 10 March 2020, and the restrictions have been continually changing depending on the ongoing situation, and especially on the number of new and confirmed cases, as well as fatal cases. Such quick implementation of strict restrictions, limited information about the virus and disease itself, uncertainty about further recommendations and potential restrictions introduced by the government, continuous need to stay at home, limited contact with family members/friends, fear about future education, as well as limited medical assistance (primarily limited to those with SARS-CoV-2-positive infection or emergency) are only a few of the major issues that significantly changed the way of living of the general population in Poland. These, in consequence, have had a significant impact on mental health and daily well-being.
The pandemic affects all individuals regardless of age or gender; however, young adults remain one of the most susceptible to the negative consequences of the pandemic in the general population as they represent the lowest levels of psychological health during the ongoing situation [
8,
9]. Students were reported to be the most vulnerable to emotional distress, and this group is characterized by some of the highest depression, anxiety, and stress levels because of the COVID-19 pandemic [
10,
11,
12,
13,
14]. The ongoing pandemic might either induce psychological/psychiatric disorders or exaggerate already existing ones [
14,
15]. Even without the COVID-19 pandemic, suicide and depression rates amongst students are reported to be increasing alarmingly nowadays [
16,
17]. Generally, university studies might constitute a stressful period in students’ lives since they remain in a transition period leading to independent, adult life. Factors associated with the COVID-19 pandemic (fear of infection, insufficient knowledge about the SARS-CoV-2 virus at the beginning of the pandemic, implementation of the strict restrictions by the governments, social isolation, etc.) constitute additional factors that could trigger emotional disturbances for students during the ongoing pandemic.
According to the transactional model of stress and coping by Lazarus and Folkman (1984), psychological stress is closely associated with the person and the environment; the model includes two major phases: (1) cognitive appraisal and (2) coping [
18]. Therefore, the stress-coping adjustment process is crucial in this group to alleviate symptoms and provide better general well-being. Lazarus’ classic transactional approach emphasizes the importance of analyzing individuals or subjectively evaluating stressful events that take place in their environment. Thus, it can be assumed that an individual’s interpretation of the environment is the main determinant in triggering a stress response in response to a stressor [
19,
20]. A crucial matter regarding Lazarus’ approach is taking into account two elements: the question of evaluation (i.e., what will be a burden for a given person) and the type of effort put in to deal with the requirements. In the last version of the understanding theory of stress by Lazarus and Folkman (1986), comprehending stress as a clearly relational concept is proposed [
21]. This means that stress is not defined as a specific type of external stimulation or a specific pattern of physiological, behavioral, or subjective responses, but rather as a kind of relationship between individuals and their environment. It is this relationship that will determine whether the available resources prove to be sufficient and effective in coping by activating various types of activities and organizing them into coping strategies [
18]. Certain types of stress are embedded in various types of so-called basic emotions [
22]. We assumed, following Lazarus [
22], that depression can be treated as one of the underlying distress emotions. Previous studies suggest that depression is one of the main psychopathological responses in a pandemic situation [
3,
23,
24,
25,
26,
27,
28].
The number of coping strategies for lifestyle changes due to the pandemic and lockdown is significant, and they are mainly dependent on one’s personality traits. Besides, different coping styles are in close relationship with the severity of mental and emotional distress [
29,
30]. It is assumed that coping strategies might be predicted based on the combination of psychological factors, factors experienced during the pandemic and lockdown specifically, as well as demographic factors of the population [
31]; they are also determined by gender, age, education, physical and mental health, and nature of the stressor [
32,
33]. Even though, during the pandemic, students most prevalently presented increased depression and/or anxiety and/or stress levels, they also tended to use approach coping strategies (such as acceptance, planning, and seeking emotional support) rather than avoidant coping strategies (such as denial, substance use, behavioral disengagement) [
34,
35].
The aim of this cross-sectional study that involves more than two thousand Polish students was to present the most frequently applied coping strategies amongst students during the ‘first wave’ of the COVID-19 pandemic. In addition, we aimed to present the effects of the pandemic on mental health, with an emphasis on emotional distress, as well as the severity of depression, anxiety, and stress symptoms. Lastly, we wanted to indicate adaptive coping strategies, which might be related to the reduction of emotional distress, acting as potential protective factors against the negative consequences of the pandemic, while at the same time presenting maladaptive coping strategies, leading to extremely high levels of anxiety, depression, and stress.
4. Results
4.1. Sociodemographic Characteristics of the Respondents
The questionnaire was completed by 2172 students from 87 Polish universities, of whom 73% (
n = 1.585) were women and 27% (
n = 587) were men. The mean age of the respondents was 22.1 ± 2.2. The majority of the respondents were medical students (60.5%,
n = 1314), and the remainder were students of the following fields of study: social sciences (19.2%,
n = 416), engineering (10%,
n = 219), arts and humanities (5%,
n = 110), and sciences (4.4%,
n = 96). The highest number of students were in their first year of study (23.5%,
n = 511), and the lowest were completing their sixth year (4.9%,
n = 106). The most common chosen place of residence was the countryside (22.9%,
n = 497). The majority of the respondents were single (65.6%,
n = 1.426) or in an informal relationship (30.7%,
n = 667), while only 2.5% (
n = 54) were married. Most of the students (48.3%,
n = 1049) lived with their parents during the outbreak of the COVID-19 pandemic, while only a small percentage, that is, 1% (
n = 21), lived with a partner and a child (
Table 1).
4.2. Health Status of the Students Enrolled in the Study
According to the results of our questionnaire, the majority of students (97.2%, n = 2112) did not confirm that they were infected by SARS-CoV-2. In addition, 89.5% (n = 1943) replied that neither their relatives nor friends had had COVID-19. Only 1.3% (n = 28) of the students, 2.4% (n = 52) of their family members, and 7.4% (n = 161) of their friends reported that they were infected by the virus. Regarding psychological well-being, 82.9% (n = 1800) of the studied group used the support of neither a psychologist nor a psychiatrist before the outbreak of the pandemic, 7.5% (n = 162) used the help of a psychologist, and 3.7% (n = 80) visited a psychiatrist, while 6.0% (n = 130) used both—psychological and psychiatric support—even before the pandemic started. Taking into account somatic diseases, the majority of students (84.6%, n = 1837) did not report any chronic disease. Thyroid diseases (4.1%, n = 88), asthma (2.5%, n = 54), mental disorders (1.9%, n = 41), allergies (1.5%, n = 32), and diabetes (0.7 %, n = 15) were among the most frequently mentioned by the respondents. Of the total respondents, 69.3% (n = 1506) admitted that they did not use any dietary supplements during the pandemic. Those who wanted to boost their immune system (30.6%, n = 665) used a complex of vitamins (6.2%, n = 134), vitamin C (6.5%, n = 140), vitamin D (7.2%, n = 157), magnesium, omega-3 fatty acids, herbs, and traditional medicine (10.8%, n = 234) habitually. Due to the outbreak of the pandemic, students had to face a vast number of difficulties, the most pronounced being the fear of infection of loved ones (33.5%, n = 728), followed by the fear of changes that awaited the world after the pandemic (20.3%, n = 440), and change of lifestyle (12.2%, n = 265).
4.3. Economic Condition of Students Participating in the Study
Out of all the students, 67.6% (n = 1469) admitted that they did not work during the pandemic; only 30.9% (n = 672) worked either intellectually or physically. During the pandemic, 15.2% (n = 330) of the studied group lost their jobs. Furthermore, we asked respondents how they assessed their economic situation in this difficult time—more than half of them (58.8%, n = 1278) had a stable family income and nothing had changed, while 29.8% (n = 647) had a stable family income but described the situation as worse than before. Only 1% (n = 21) of the students answered that they had to start borrowing money from family or friends during the pandemic outbreak because they were not able to support themselves.
4.4. Total DASS Score
The DASS total score for the whole group of respondents was 38.13 ± 26.51, which is lower than the cut-off score equal to 60, as originally proposed by Lovibond and Lovibond [
39]. Overall emotional distress turned out to be significantly higher (
p < 0.001) in females (M = 40.54 ± 26.65) compared to males (M = 31.60 ± 25.02). There were statistical differences between the DASS total score and the field of study; the lowest DASS total score was observed in the case of medical students (median (Me) = 31.00 ± 25.48), while the highest was in the case of students studying science (Me = 42.00 ± 40.91), followed by arts and humanities (Me = 39.00 ± 28.98), social sciences (Me = 35.00 ± 28.14), and engineering (Me = 32.00 ± 26.79). Based on the Kruskal–Wallis test, the studied groups were statistically different (H = 16.16,
p = 0.0028); the highest difference was noted between the medical and science students (z = 3.312,
p = 0.009) (
Supplementary Tables S1–S12).
4.5. Depression
The respondents presented a moderate level of depression symptoms; the mean score for the depression subscale for the entire group was equal to 14.04 ± 10.44. Depression symptoms were significantly (
p < 0.001) more intensified amongst females (M = 18.41 ± 14.05) compared to males (M = 12.24 ± 14.37). The intensity of depression defined in the DASS-21 subscale concerned the following number of respondents: ‘normal’ depression applied to 43.6% (
n = 948) of the students, ‘mild’ depression applied to 13% (
n = 282), ‘moderate’ depression applied to 19.9% (
n = 432), while ‘severe’ and ‘extremely severe’ applied to 10.2% (
n = 221) and 13.3% (
n = 289) of the students, respectively. A significant difference was found between the severity of depression for students of science and medicine (z = 3.25,
p = 0.012), following the results obtained from the Kruskal–Wallis test (H = 19.82,
p = 0.0005) (
Supplementary Tables S2 and S55).
4.6. Anxiety
Regarding the anxiety subscale, the mean result for the entire group was 7.71 ± 8.29, which is equal to the ‘mild’ intensity of anxiety according to the DASS-21 scale. The intensity of anxiety was as follows in a sample of the studied students: ‘normal’ anxiety—60.2% (
n = 1307), ‘mild’ anxiety—12.5% (
n = 273), ‘moderate’ anxiety—9% (
n = 195), ‘severe’ anxiety—6.6% (
n = 144), and ‘extremely severe’—11.7% (
n = 273). Similarly, in the depression subscale, females tended to present statistically higher (
p < 0.001) anxiety levels (M = 13.19 ± 11.54) compared to males (M = 6.90 ± 9.92). Students studying arts and humanities (Me = 6.00 ± 8.63), science (Me = 6.00 ± 9.2), and social sciences (Me = 6.00 ± 8.53) reached the highest levels of anxiety, while in the case of medicine (Me = 4.00 ± 8.0) and engineering (Me = 4.00 ± 8.06), the intensity of anxiety was lower. However, the results did not vary significantly between the fields of studies (
Supplementary Tables S3 and S56).
4.7. Stress
The mean score for the stress subscale was equal to 16.93 ± 10.98, which according to the DASS-21 scale can be classified as ‘mild’ stress. Similarly to the depression and anxiety subscales, females presented significantly (
p < 0.001) higher levels of stress (M = 20.93 ± 15.45) compared to males (M = 12.58 ± 14.70). Stress levels amongst the respondents were of the following degrees of intensity: ‘normal’—47.2% (
n = 1026), ‘mild’—11.8% (
n = 255), ‘moderate’—15.3% (
n = 333), ‘severe’—16.8% (
n = 364), and ‘extremely severe’—8.9% (
n = 194). Regarding stress levels, the highest stress intensity was observed in the case of the students studying science (Me = 20.00 ± 11.12), followed by art and humanities (Me = 19.00 ± 11.62), social sciences (Me = 16.00 ± 11.51), engineering (Me = 16.00 ± 10.82), and medicine (Me = 16.00 ± 10.73). There was no significant difference between stress intensity and the students’ field of study, based on the results obtained from the Kruskal–Wallis test (
Supplementary Tables S4 and S57). The above results are presented in
Table 2.
4.8. Coping Strategies in a General Population of Polish Students
Polish students chose stress coping strategies belonging to the ‘approach’ coping strategies more often (M = 29.60 ± 6.89) compared to ‘avoidant’ coping strategies (M = 22.82 ± 5.78). Amongst the most frequently chosen stress coping strategies were acceptance (M = 2.19 ± 0.71), emotional support (M = 1.58 ± 0.93), planning (M = 1.44 ± 0.84), and positive reframing (M = 1.41 ± 0.90), as well as one strategy belonging to the ‘avoidant’ group, namely self-distraction (M = 1.43 ± 0.80). Further, the three most rarely chosen strategies were denial (M = 0.43 ± 0.64), substance use (M = 0.50 ± 0.80), and behavioral disengagement (M = 0.70 ± 0.76), which also belong to avoidant coping (
Supplementary Tables S13 and S14).
4.9. Sex Differences in the Choice of Coping Strategies between Females and Males
The most frequently chosen stress coping strategy by females was acceptance (M = 2.18 ± 0.71), followed by emotional support (M = 1.67 ± 0.92) and planning (M = 1.46 ± 0.84), while in the case of males, the most prevalent ones also included acceptance (M = 2.22 ± 0.70) and planning (M = 1.38 ± 0.87), as well as humor (M = 1.33 ± 0.74).
Mann–Whitney’s U test showed that among the avoidant coping strategies, women differed from men, choosing self-distraction (M = 1.51 ± 0.79,
p < 0.001), denial (M = 0.47 ± 0.66,
p < 0.001), and venting (M = 1.37 ± 0.76,
p = 0.0001) more often, while men resorted to substance use (M = 0.61 ± 0.85,
p < 0.001). Among the approach strategies, more women chose emotional support (M = 1.67 ± 0.92,
p < 0.001), use of informational support (M = 1.27 ± 0.87,
p < 0.001), and positive reframing (M = 1.45 ± 0.89,
p = 0.001). While women turned to religion (M = 0.84 ± 1.00,
p = 0.001), men dealt with the situation through a sense of humor (M = 1.33 ± 0.74,
p < 0.001) (
Table 3).
4.10. Stress Coping Strategies and Fields of Study
The respondents’ fields of study included medicine, art and humanities, social sciences, engineering, and sciences. The analysis showed a statistically significant differences in the gender distribution of the respondents in the analyzed fields of study (Chi-kw = 109.22, df = 4,
p = 0.00001), which justifies conducting analyses with division into fields of study. Significant differences were noted between medical and social sciences students, which resulted only from differences between women in terms of preferred strategies (
Supplementary Tables S58–S65). Out of 14 Brief-COPE strategies, in five of them (i.e., ‘active coping’, ‘use of informational support’, ‘planning’, ‘humor’, and ‘self-blame’), female medical students achieved significantly higher results than female social sciences students. This is an interesting observation, especially in the context of the lack of any differences between males in this regard.
Students from all fields of study most frequently chose ‘acceptance’ as a coping strategy for stress, except for the engineering students, who most often used ‘positive reframing’. Other frequently chosen coping strategies included emotional support, planning, positive reframing, and self-distraction. Amongst students studying sciences, ‘planning’ was most prevalently replaced by ‘venting’ instead. Based on the results of the Kruskal–Wallis test, students of particular fields of study differed statistically in their chosen coping strategies. Regarding the use of informational support, the individual fields of study were statistically different (H = 20.74,
p = 0.0004), with medicine and engineering presenting the most pronounced difference (z = 3.70,
p = 0.002). The use of the venting strategy also differed significantly between students of different fields of study (H = 18.39,
p = 0.0010); the highest difference was noted between medicine and engineering (z = 3.83,
p = 0.001), followed by sciences and engineering (z = 3.35,
p = 0.008). Planning also showed a statistical difference (H = 25.30,
p < 0.0001), namely between medicine and social sciences (z = 4.16,
p < 0.001). The groups also differed statistically in terms of sense of humor in stressful situations (H = 22.39,
p = 0.0002). The most significant difference was observed between medicine and social sciences (z = 4.38,
p < 0.001), followed by engineering and social sciences (z = 3.40,
p = 0.007). Acceptance showed the biggest difference (H = 37.08,
p < 0.0001) between medical students and social sciences students (z = 5.45,
p = 0.000). The turn to religion also showed a statistical difference (H = 27.07,
p < 0.0001) between the studied groups, particularly in the case of medicine and social sciences (z = 3.95,
p = 0.001), (
Supplementary Tables S15–S19 and S47–S52).
4.11. Coping Strategies of Students who Were Using Support of a Psychologist or Psychiatrist before a Pandemic
The majority of respondents (
n = 1800) used the support of neither a psychologist nor a psychiatrist before the outbreak of the pandemic. The study showed that the three most popular strategies for coping with stress belonged to the approach category and included acceptance (M = 2.19 ± 0.71), emotional support (M = 1.57 ± 0.92), and planning (M = 1.42 ± 0.84). Interestingly, the coping strategies of students who used the support of a psychologist or psychiatrist before the pandemic presented in the same order. Other results were achieved by students who had to use the support of both a psychologist and a psychiatrist—the most common coping strategies in this group were acceptance (M = 2.17 ± 0.71), emotional support (M = 1.52 ± 0.99), and self-distraction (M = 1.52 ± 0.83), (
Supplementary Tables S20–S23).
4.12. Coping Strategies of Students Depending on the Living Situation
Regardless of who the respondents lived with, acceptance was always the most common coping strategy in the cases of living alone (M = 2.26 ± 0.77), with roommates (M = 2.21 ± 0.67), with parents (M = 2.16 ± 0.72), with a partner or spouse (M = 2.24 ± 0.70), and with a partner or spouse and a child (M = 2.12 ± 0.71), (
Supplementary Tables S24–S28).
4.13. The Most Prevalent Difficulties during the Pandemic and Associated Coping Strategies
Regardless of the type of situation that respondents perceived as the most difficult, the most common strategy were acceptance. One of the greatest difficulties pointed out by the students was fear of the infection of their loved ones (n = 730). The three most frequently chosen strategies for coping with stress in this situation included acceptance (M = 2.21 ± 0.67) and emotional support (M = 1.70 ± 0.90), as well as one avoidant coping strategy—self-distraction (M = 1.49 ± 0.80). Quantitatively, the second most frequently chosen difficulty was fear of the changes that awaited the world after the pandemic (n = 446). Those students most often used approach coping strategies: acceptance (M = 2.28 ± 0.68), emotional support (M = 1.66 ± 0.92), and planning (M = 1.59 ± 0.87). The lowest number of people (n = 26) chose the answer that they were not afraid of anything; the strategies most often used by this group were acceptance (M = 2.40 ± 0.84), humor (M = 1.85 ± 0.96), and positive reframing (M = 1.21 ± 1.12).
The use of the approach coping strategy was statistically different (H = 43.75,
p = 0.00001) between those students who felt fear of infection of their loved ones and for those who struggled to cope with loneliness (z = 3.92,
p = 0.003). Another statistical difference was shown by those who felt loneliness the most, and those who were afraid of the changes in a post-pandemic world (avoiding repetition) (z = 3.88,
p = 0.004). Another difference concerned those who were not afraid of anything, and those who were also afraid of the uncertainty of an altered world (z = 3.84,
p = 0.004). Statistical differences were also shown in the use of an avoidant coping strategy by students in the context of the greatest difficulties experienced during lockdown (H = 79.18,
p < 0.0001). The greatest difference was shown between loneliness and those students who were not afraid of anything (z = 7.29,
p < 0.001), followed by the fear of being infected and those who felt no fear (z = 5.91,
p < 0.001), and additionally, between those who had a concern about their education and those who felt lonely (z = 5.48,
p < 0.001), (
Supplementary Tables S29–S37, S53 and S54).
4.14. Coping Strategies of Students Depending on Their Employment Status
Despite their occupation, all students who were not working (M = 2.19 ± 0.70), were working intellectually (M = 2.20 ± 0.73), physically (M = 2.16 ± 0.76), or ran their own business (M = 2.34 ± 0.77) chose acceptance as a major stress coping strategy. Except for acceptance, in all of the aforementioned groups, students most prevalently chose emotional support, planning, self-distraction, and positive reframing (
Supplementary Tables S38–S46).
4.15. Coping Strategies of Students Suffering from Chronic Diseases
Overall acceptance was the most frequently chosen stress coping strategy for students without chronic disease (
n = 1837), as well as those with thyroid disease (
n = 88), asthma (
n = 54), allergy (
n = 32), diabetes (
n = 15), or mental disorders (
n = 41), as well as students with other chronic diseases (
n = 105), including gastroenterological, neurological, circulatory, endocrine, or autoimmune diseases. The differences between the groups of students suffering from various chronic diseases were related to less frequently used strategies. The second most commonly used strategy for all groups was emotional support, except for asthmatics, who chose planning (M = 1.54 ± 0.82), and those suffering from mental disorders, who used an avoidant strategy of coping with stress—self-distraction (M = 1.78 ± 0.76). Additionally, students suffering from mental disorders most often chose negative ways of coping with stress—the third most prevalently chosen strategy was venting (M = 1.67 ± 0.85). Among the 14 strategies, students of all groups chose substance use and denial least frequently, apart from those suffering from mental disorders, who were least likely to choose religion as a way of coping (M = 0.60 ± 0.87) (
Supplementary Tables S5–S11).
4.16. Correlation between Stress Coping Strategies and Level of Emotional Distress
A strong positive relationship has been observed between avoidant coping mechanisms and scores of DASS Total (r = 0.649), depression (r = 0.588), anxiety (r = 0.556), and stress (r = 0.591). Conversely, approach coping mechanisms show a weak and very weak negative correlation with DASS Total (r = −0.068) and depression (r = −0.159), respectively, both of which were statistically significant (
Table 4).
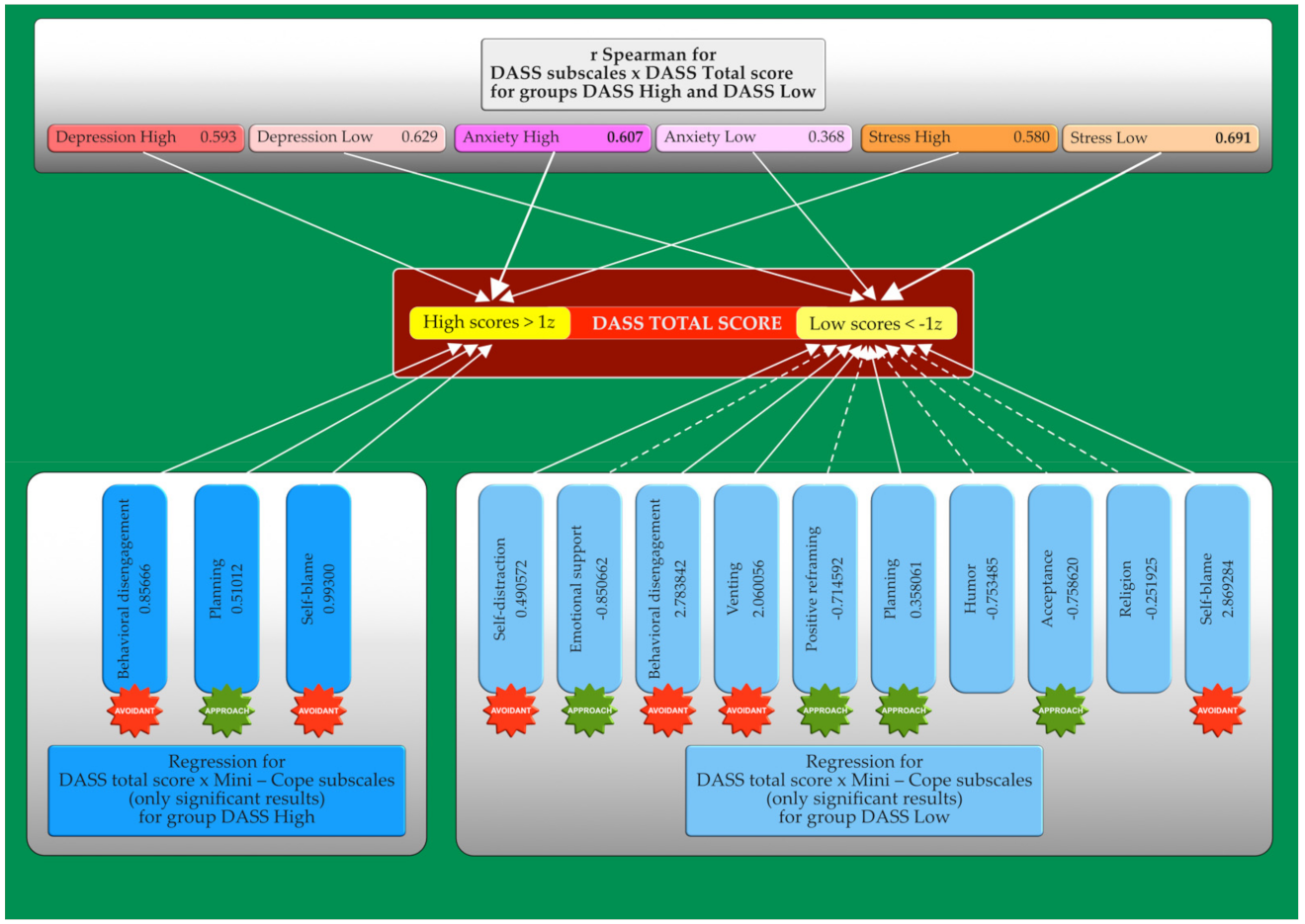
According to the results and statistical significance, the highest positive correlation was found between the scores of DASS Total and the level of depression (D), anxiety (A), and stress (S), and the same three coping mechanisms: self-blame (DASS Total: r = 0.609; D: r = 0.596; A: r = 0.490; S: r = 0.537), behavioral disengagement (DASS Total: r = 0.603; D: r = 0.627; A: r = 0.466; S: r = 0.507), and venting (DASS Total: r = 0.457; D: r = 0.355; A: r = 0.397; S: r = 0.468). As for the highest negative correlation, it was found between acceptance (DASS Total: r = −0.257; D: r = −0.248; A: r = −0.212; S: r = −0.229) and positive reframing (DASS Total: r = −0.159; D: r = −0.201; A: r = −0.057; S: r = −0.141) in all DASS components. On the other hand, for anxiety levels, there were only two coping strategies shown above that were statistically important enough to have negative correlation. For people who used emotional support during the pandemic, there was a decreased level of depression (r = −0.175) and DASS Total scores (r = −0.088). Humor was found to have the third highest negative correlation with level of stress (r = −0.078). Furthermore, religion as a mechanism of stress coping, in addition to a very weak negative correlation with depression (r = −0.093), shows a very weak positive correlation with anxiety (r = 0.057).
4.17. The Impact of the Stress Coping Strategies Used by Polish Students on the Emotional Well-Being
According to the results of the multiple regression analysis, the results obtained in the following Brief-COPE scales have a significant impact (R = 0.760, R
2 = 0.578 corrected R
2 = 0.5759; F (14.2157) = 211.64
p < 0.00001, SE of E: 17.265) on the increase of the total DASS score: behavioral disengagement (
p < 0.0001), venting (
p < 0.0001), self-blame (
p < 0.0001), and planning (
p = 0.007); all of them belong to avoidant coping strategies, except for planning, which is an approach coping strategy (
Table 5).
Contrarily, the following Brief-COPE scales have had a statistically significant impact on lowering the total DASS score: emotional support (
p < 0.001), positive reframing (
p < 0.001), acceptance (
p < 0.001), and humor (
p < 0.001). All of these scales belong to the approach coping strategies, except ‘humor’, which is an independent factor. The subscales of anxiety (r = 0.607), depression (r = 0.593), and stress (r = 0.580) correlated with higher DASS total scores, respectively. On the other hand, the stress subscale (r = 0.691) correlated with lower values of the DASS Total score, followed by depression (r = 0.629) and anxiety (r = 0.368) (
Figure 1).
5. Discussion
Research devoted to the mental health of students in the COVID-19 era is currently ongoing all over the world. The uncertainty of returning to schools and universities, as well as changing the forms of teaching and isolation, significantly affected young adults. There are many examples indicating how the mental health of students deteriorated during the pandemic; one of them is a study of more than two thousand American college students, in which 48.14% (
n = 960) showed a moderate-to-severe level of depression, 38.48% (
n = 775) showed a moderate-to-severe level of anxiety, and 18.04% (
n = 366) had suicidal thoughts [
44]. The shift to online learning also had a significant impact on the mental health of students. Research shows that depression and stress levels increased due to e-learning [
45]. A study involving 69,054 students living in France during the COVID-19 quarantine showed a high prevalence of mental health issues among students who experienced quarantine, underlining the need to reinforce prevention, surveillance, and access to care [
46].
In this study, we examined how Polish students manage emotional distress during the COVID-19 pandemic. In our study, students preferred to choose ‘approach’ coping strategies (M = 29.60 ± 6.89), rather than ‘avoidant’ coping strategies for stress (M = 22.82 ± 5.78). Such data indicates that most of the students aimed to approach the problem of the ongoing COVID-19 pandemic in an adaptive way. The implementation of such coping strategies for stress was associated with lower emotional distress as well as lower depression, anxiety, and stress symptoms amongst Polish students. Furthermore, the intensification of distress in women causes a turn to religion (
p = 0.001), while men use substances (
p < 0.001) and a sense of humor (
p < 0.001). The importance of religious practices for the mental condition of adults during the lockdown period in Poland is also confirmed by the results of other authors, especially in relation to private practice [
47]. Acceptance was one of the most frequently chosen coping strategies regardless of gender, age, economic status, or health status of the respondents, followed by emotional support, planning, self-distraction, and positive reframing.
Considering the field of study, it turned out that medical and social sciences students differ in the chosen stress coping strategies. Further analysis showed that these differences are due only to differences between women studying medicine and social sciences. In five of the included Brief-COPE strategies (i.e., ‘active coping’, ‘use of informational support’, ‘planning’, ‘humor’, and ‘self-blame’), female medical students achieved significantly higher results than female social sciences students.
Regarding the results obtained using the DASS-21 scale, the total DASS score for the entire group of the respondents was 38.13 ± 26.51, while the subscales including depression, anxiety, and stress were equal to 14.04 ± 10.44, 7.71 ± 8.29, and 16.93 ± 10.98, respectively. Such results represent a moderate level of depression and mild stress and anxiety. Regarding the DASS Total score, it is lower than the cut-off score proposed by Lovibond and Lovibond [
38]. Le Vigouroux et al. has also indicated that anxiety and depressive symptoms are highlighted amongst French students, but those variables cannot be compared exactly between our studies due to different psychological tools used by their research group (Hospital Anxiety and Depression Scale (HADS)). Regardless, it should be pointed out that similarly to Polish students, emotional distress was also triggered amongst French students during the COVID-19 outbreak. Similarly, in the case of Egyptian students, depression and stress symptoms were mostly enhanced during the outbreak of the pandemic [
48].
Our results seem to be in agreement with those obtained by researchers from other countries, which were presented particularly as enhanced anger, insomnia, depression, overall exhaustion, or loss of willingness to conduct everyday tasks. Spanish students presented moderate to extremely severe symptoms of stress (28.14%), anxiety (21.34%), and depression (34.19%) [
49]. The results of one of the Arabic studies indicated that a vast majority of students (92.9%) suffered from the elevation of psychological distress specifically during the outbreak of the COVID-19 pandemic [
50]. It should be noted that there were gender differences regarding the intensity of the emotional distress, which was mostly intensified in females, indicating that they might be more vulnerable to depression, anxiety, and stress symptoms compared to males.
While searching PubMed, Scopus, and Web of Science databases, we found four similar studies conducted in Egypt, France, Nepal, and Pakistan, which we found interesting to compare due to the similarities in materials (population group) and methods used in our studies, along with the time when our studies were conducted [
48,
51,
52,
53]. Comparing the four most frequently chosen stress coping strategies between Polish, French, Egyptian, Nepalese, and Pakistani University students, we can see similarities. In all those countries, acceptance was the most popular strategy, except in Pakistan, where it was in second place and religious/spiritual coping was number one. Only one strategy belonging to the avoidant group was present in the top four strategies in almost all countries (except Egypt), in third or fourth position. Positive reframing was found in three countries, as well as planning, while active coping and religion were found in two countries. Only Polish students selected emotional support as the second most common strategy. Egyptian and Pakistani students were the only ones that had used religious coping mechanisms as one of the most common strategies. These dissimilarities could be due to cultural differences. The main religion of Egypt and Pakistan’s population is Islam, in comparison to Poland and France, where it is mostly Christianity, and in Nepal, where it is Buddhism [
54]. The four most frequently chosen stress coping strategies are shown in
Table 6.
Approach coping strategies were the most common strategies chosen by the students from Poland and were associated with better well-being. The strategies that played a generally protective role against emotional distress symptoms were emotional support, positive reframing, acceptance, and humor, as seen in
Table 4. All other countries have a similar pattern, and show the same effect of approach strategies on the well-being of participants. Interestingly, self-distraction was among the four most frequently chosen coping strategies in all compared countries. In France, acceptance and positive reframing strategies played a generally protective role against anxiety and depressive symptoms. French students who most willingly chose avoidant coping strategies included those who were worried about their future job prospects; those who were worried about their own and their families’/friends’ health statuses; and those whose strategies mostly included behavioral disengagement or denial [
51].
Concerning gender differences in Polish students, women more often chose emotional support (
p < 0.001), use of informational support (
p < 0.001), positive reframing (
p = 0.001), self-distraction (
p < 0.001), denial (
p < 0.001), venting (
p = 0.0001), and religion (
p = 0.001), while men resorted to substance use (
p < 0.001) and humor (
p < 0.001). Significant differences were also observed in Pakistani students—gender was one of the major factors where significant differences were observed regarding the following coping strategies: planning, humor, acceptance, self-distraction, and religious coping. Specifically, females had significantly lower scores for planning (
p = 0.033), as well as humor (
p < 0.001), while males had significantly lower scores for acceptance (
p = 0.019), religious coping (
p < 0.001), and self-distraction (
p < 0.001) [
53]. In a study performed by Skapinakis et al., Greek students mostly used acceptance, humor, and planning as their major coping strategies during the pandemic outbreak, including both females and males, once again indicating that approach coping strategies were more preferable to the students [
55]. Furthermore, the results of this study indicate that active/positive coping strategies were more frequently used compared to supportive strategies. Interestingly, more supportive coping strategies along with religious coping were more likely used by females, while males tended to apply substance use. In another study conducted by Salman et al., the most frequently chosen coping strategies included religious coping, acceptance, and planning, while the lowest prevalence was substance use and self-blame [
53]. Regarding gender differences in this study, females were observed to have significantly greater scores for venting (
p = 0.015), religious/spiritual coping (
p = 0.003), and behavioral disengagement (
p = 0.043), compared to males.
According to current research, the gender differences in coping strategies among medical students appear to be very diverse. For example, Dodek et al. showed that gender does not matter among medical students when choosing a strategy for coping with distress [
56]. This observation is also confirmed by studies conducted on medical students from Canada and Scotland long before the outbreak of the pandemic [
57,
58]. However, some authors, such as Shaikh et al. found significant gender differences in coping. In Pakistan, women studied and slept, while men preferred to play sports, isolate themselves, or spend time with friends [
59]. Additionally, in Pakistan, some studies have shown that it was men who more frequently displayed maladaptive coping strategies, such as substance use, denial, and self-blame [
60]. Since all these observations concern both Western and Eastern countries, further research, especially in an exceptional situation such as increased distress due to pandemic, seems interesting, especially since cultural and environmental factors certainly also play a role.
Regarding gender differences, in a COVID-19 situation, a May 2021 study by Neufeld et al. showed that females reported greater use of behavioral disengagement, while men reported less trust in emotional and instrumental support [
61]. The literature suggests that differences in coping with stress may be due to playing gender roles [
62]. Thus, the study findings that females used more behavioral disengagement while men used less social support may reflect certain stereotypes. Perhaps men will not reach for social support because such behavior is antagonistic to traditional male ideals. On the other hand, women may choose behavioral disengagement more often to show traditional feminine traits such as being submissive. Considering the cultural factor, it is interesting that, as in our study, in South-West Nigeria and Malaysia, women turned to religion more often than men, which may also be associated with the cultivation of stereotypically adopted gender roles [
63,
64].
In addition, we observed a very interesting phenomenon by studying the literature and comparing the obtained results in terms of the study field. In Poland, medical students coped best with the pandemic, which is a very promising factor in the context of their future professional work. In Pakistan, medical students had significantly lower “self-blame” scores than pharmacy (
p = 0.005), allied health sciences (
p = 0.028), and other university students (
p = 0.002) [
53]. This showed quite a different approach than in Egypt, where medical students chose the most dysfunctional coping strategies compared to colleagues studying engineering, sciences, and humanities, and reached the highest levels of depression, anxiety, and stress [
48]. The results of our study showed a relationship between the field of study and the DASS Total score. The highest intensity of emotional distress was obtained by science students, followed by those who studied arts and humanities, and then social sciences and engineering. Medical students also scored the lowest in the DASS Total score (
Supplementary Table S1).
Searching for factors having the greatest impact on the emotional state of students during the lockdown, isolation and loneliness played a meaningful role. In our study, students who chose “loneliness” as their greatest difficulty during the pandemic were 292 times more likely to experience higher overall emotional stress [
8]. Loneliness is a well-known factor in the development of depression, which can be further intensified by the loss of the ability to use natural coping techniques in a pandemic, which Dawson and Golijani-Moghaddam showed in their research [
65,
66]. In a study conducted in France by Vigouroux et al., it was argued that students found it tough to implement a variety of coping strategies during the lockdown. Even so, they were able to use several effective strategies such as acceptance, planning, and positive reframing. It is possible that students who were not flexible in their choices also showed the highest levels of anxiety and depression symptoms [
51].
Reflecting on the intensity of emotional distress between students of different years of study, in Poland there were no statistical differences between the first-year students and the rest of the respondents in the DASS Total score, nor in any of the DASS subscales. The situation was different in Nepal, where last-year nursing students were the most depressed, stressed, and afraid compared to those in their first, second, or third year [
52]. Nepalese colleagues suggest that it may be related to uncertainty about graduation and their professional future.
Even if the model of stress and coping by Lazarus and Folkman mentioned in our study is somewhat simplified (e.g., due to limitations related to internet research and the nature of brief tools), it indicates a linkage between stress, coping with stress, and basic emotions.
The results of our study can provide an insight into which of the coping strategies could act protectively for students and might possibly alleviate depression, anxiety, and stress symptoms effectively in the era of the COVID-19 pandemic. It is very encouraging to see such results since they indicate that students tend to be rather problem-focused and primarily chose positive coping strategies, indicating that they could probably adapt more easily to the changes associated with the ongoing pandemic. Further, such coping with the pandemic might lead to lower-intensity depression, anxiety, and stress symptoms compared to situations when students would rather use negative coping strategies.
The results of the study also have clinical implications for both preventive and therapeutic interventions, related to: (1) the urgent need to identify students particularly at risk of significant emotional disturbances during the COVID-19 pandemic; (2) designing therapeutic programs for the identified group of distressed students in need, including techniques to change maladaptive to effective and adaptive stress coping strategies; (3) creation of crisis/mental health help centers for students to cope with emotional distress caused by the pandemic; and (4) the necessity of including stress coping training in the curriculum of various fields of study.
6. Limitations of the Study
One of the limitations of this study was that the respondents were only Polish students; therefore, the obtained responses were limited to a very select group of students representing quite narrow cultural, ethnic, and religious groups. In Poland, Christianity is the most prevalently practiced religion, which could eventually affect the responses of the students - particularly their coping strategies—which is also emphasized in our results. Besides, the majority of the respondents (n = 1585) were females, while the field of study was also primarily limited to medical students (n = 1314). The students who were involved in this study included only those who were interested in this topic and wanted to contribute to this project. Therefore, our results cannot be generalized to other cultural, ethnic, or religious groups, and only represent those who were included in this study. In the discussion, we tried to compare our results with those obtained in other countries; however, cultural, ethnic, and religious differences, as well as varying restrictions and lockdown status should be taken into consideration, limiting the possibility of providing a fully reliable comparison.
As shown in our study, students of different fields of studies presented different intensities of overall emotional distress, along with the exacerbation of depression, anxiety, and stress symptoms, which, in some aspects, are associated with the application of various coping strategies. Our data is slightly limited since mostly medical students were the respondents, and they presented significantly lower levels of overall emotional distress compared to students in other fields of studies.
Moreover, the reliability of this study is slightly limited due to the fact that it was an online questionnaire, and we did not have any control over the respondents’ responses. Besides, since the questionnaire was open only from 20 to 26 April 2020, the results reflect only a short period of time, without any insight into the possible changes that could occur because of the implementation of further restrictions by the government. Even though we aimed to show the application of which coping strategies are associated with the lowest overall emotional distress and depression, anxiety, and stress levels, we cannot conclude whether their application will provide long-term results.
Another limitation was the choice of an online questionnaire type, which did not provide us information on what percent of students withdrew from the study and at what stage. This data would give us information about the respondents and the structure of the survey itself. Nevertheless, the conducted study provided great insight into the mental condition of the students, who constituted a group capable of going through the entire questionnaire. Besides, the study was conducted during the ‘first wave’ of the pandemic, and thus coping mechanisms may have changed dynamically to this day. Future studies can certainly give an insight into this issue.


 ,
, 

{kind=link}