
Efficacy of Prolonged-Release Melatonin 2 mg (PRM 2 mg) Prescribed for Insomnia in Hospitalized Patients for COVID-19: A Retrospective Observational Study


Abstract
:1. Introduction
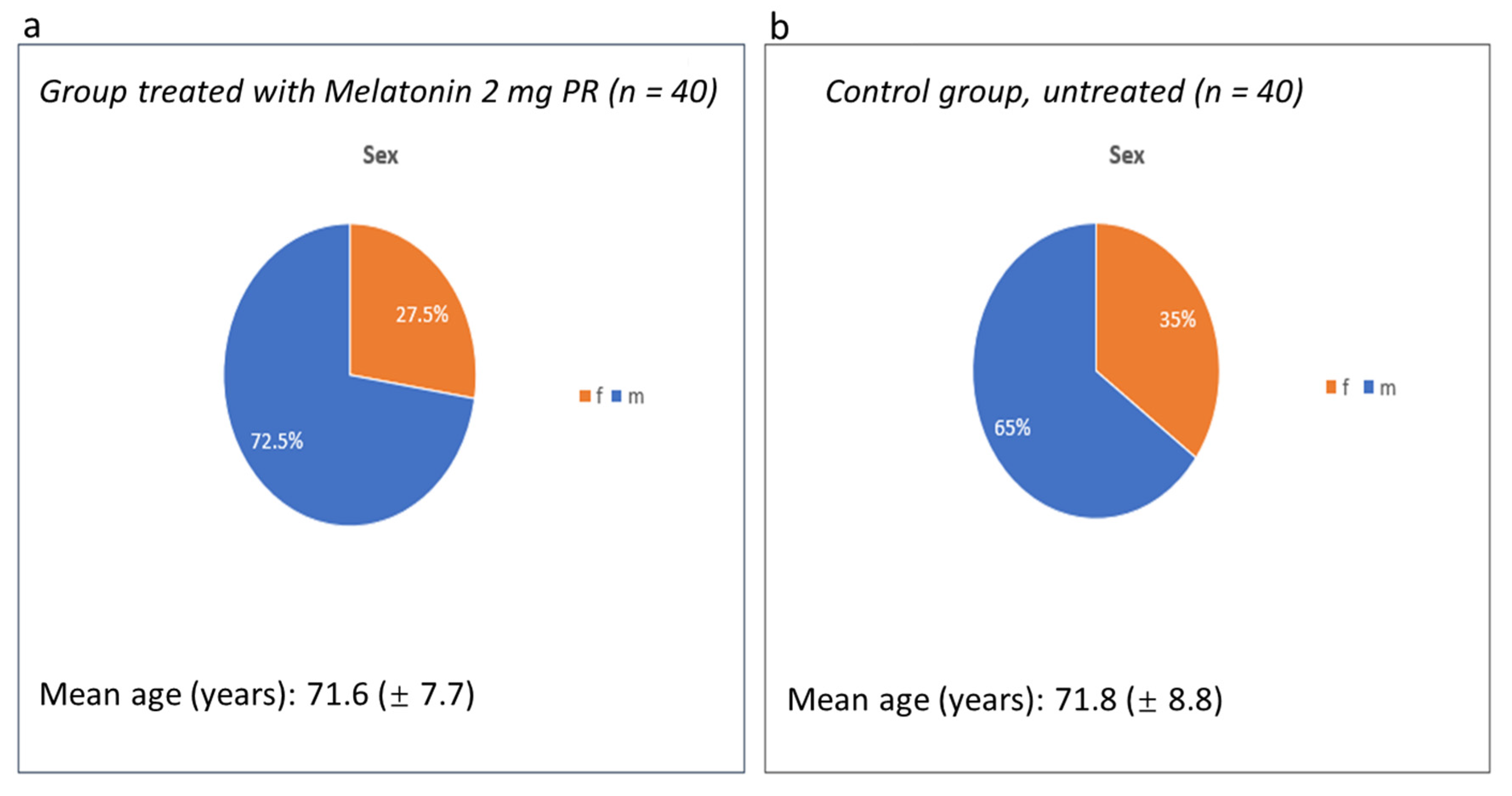
2. Materials and Methods
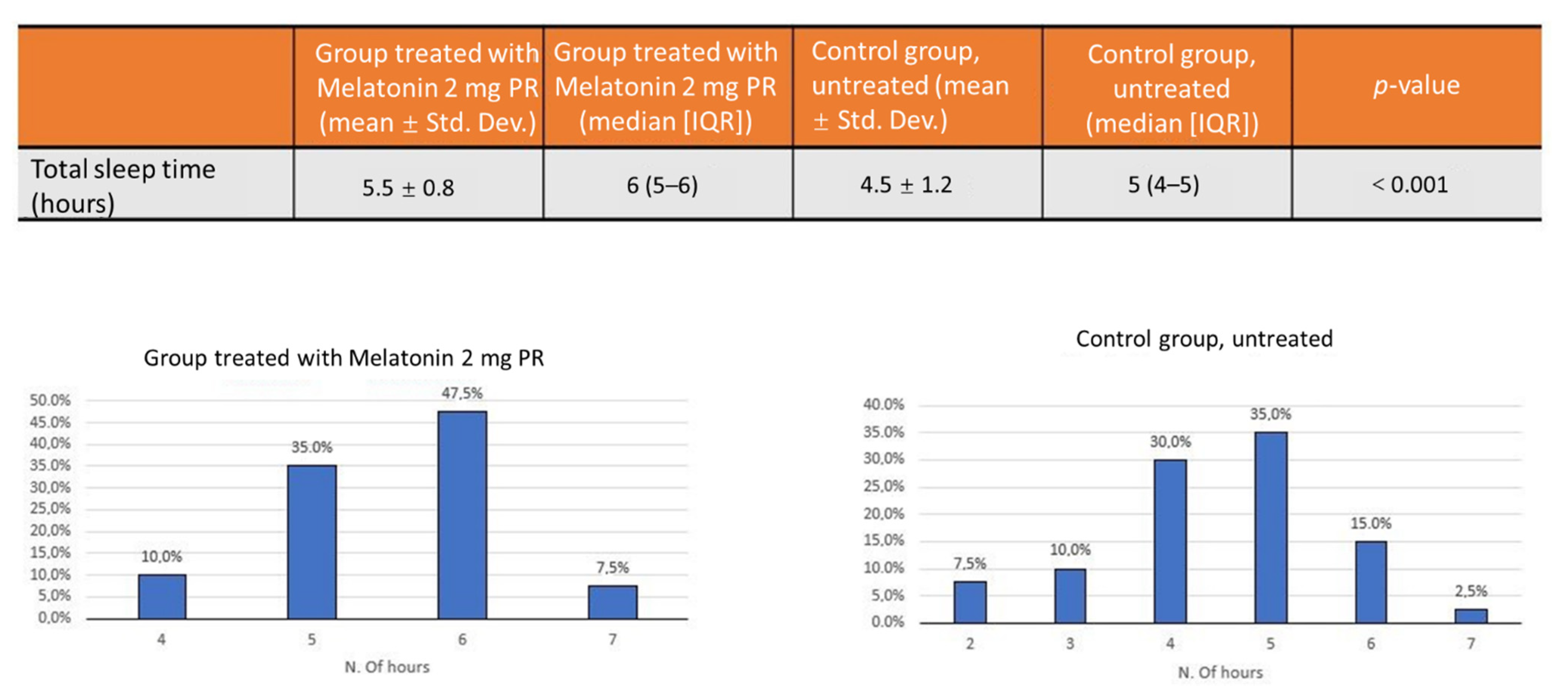
- Total number of hours of sleep ensured for the patient;
- Duration of non-invasive ventilation;
- Duration of the sub-intensive stay;
- Overall hospitalization duration;
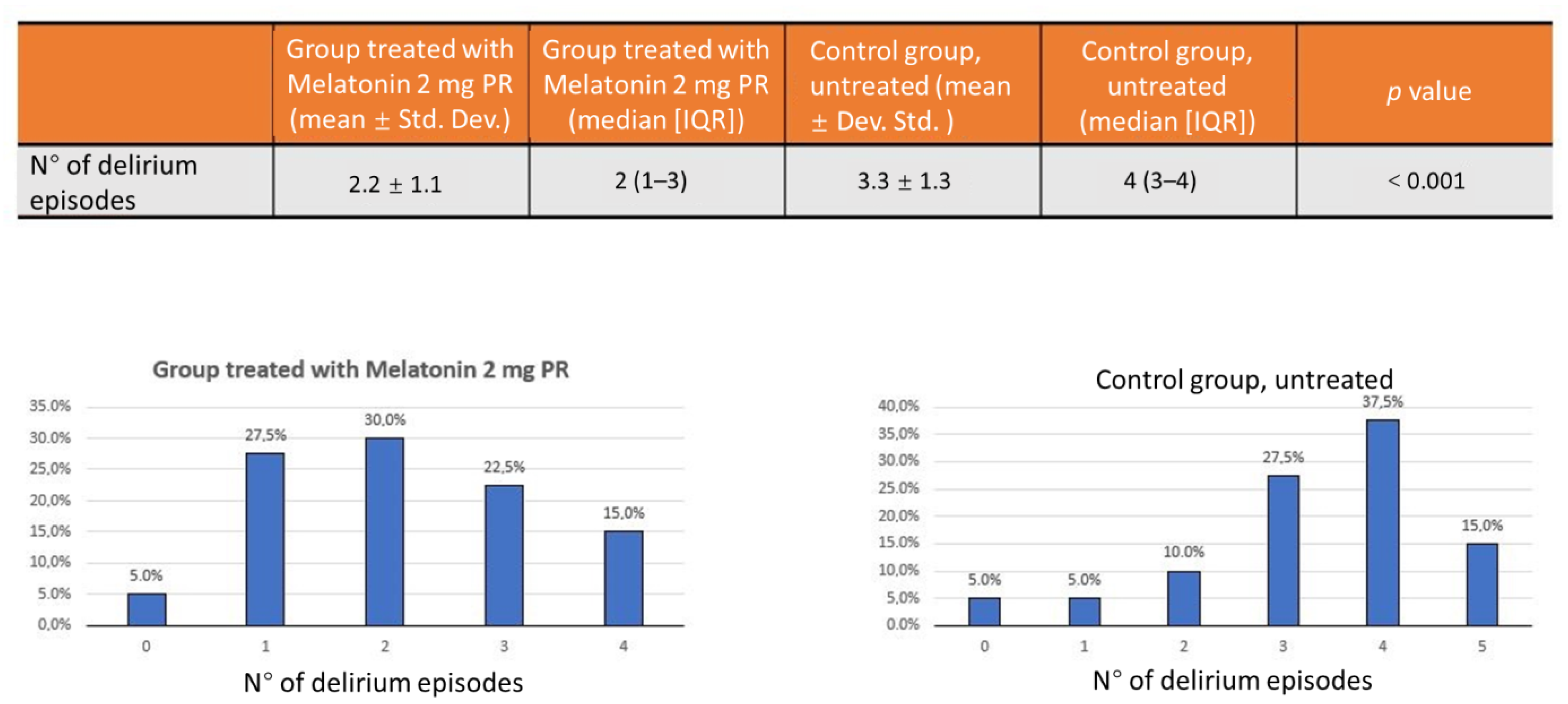
- Incidence of delirium, an acute disturbance of consciousness with inattention accompanied by a change in cognition, or perceptual disturbance that fluctuates over time [9].
Authorization of the Ethics Committee Opinion Expressed in the Session of 28 April 2021 Prot. 275\CE22-2021 ASL Na1
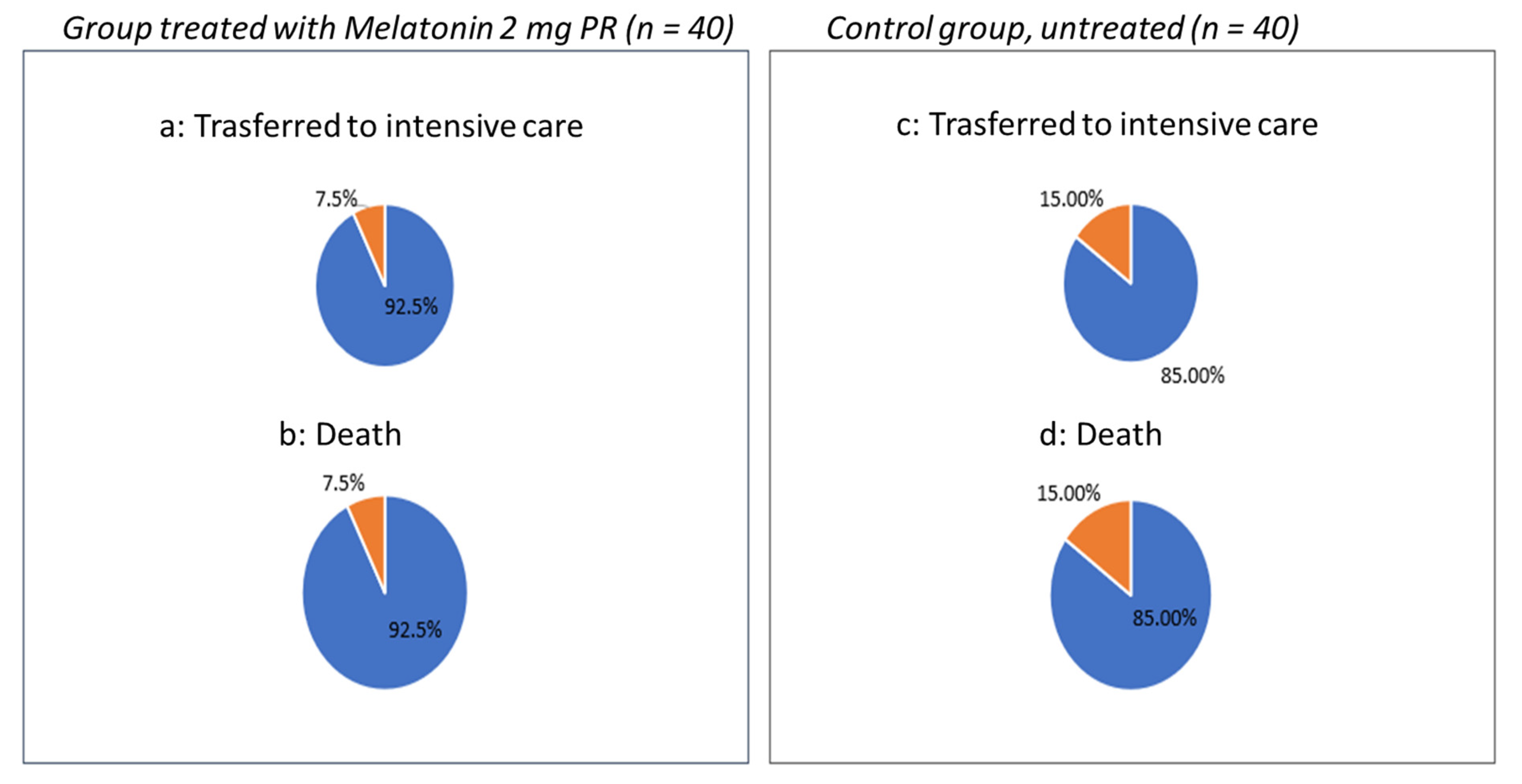
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, R.; Wang, X.; Ni, L.; Di, X.; Ma, B.; Niu, S.; Liu, C.; Reiter, R.J. COVID-19: Melatonin as a potential adjuvant treatment. Life Sci. 2020, 250, 117583. [Google Scholar] [CrossRef]
- Anderson, G. Reiter Melatonin: Roles in influenza, COVID-19, and other viral infections. R. J. Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef]
- Shneider, A.; Kudriavtsev, A.; Vakhrusheva, A. Can melatonin reduce the severity of COVID-19 pandemic? Int. Rev. Immunol. 2020, 39, 153–162. [Google Scholar] [CrossRef]
- Cardinali, D.P.; Brown, G.M.; Pandi-Perumal, S.R. Can Melatonin Be a Potential "Silver Bullet" in Treating COVID-19 Patients? Diseases 2020, 8, 44. [Google Scholar] [CrossRef]
- Patel, D.; Steinberg, J.; Patel, P. Insomnia in the Elderly: A Review. J. Clin. Sleep Med. 2018, 14, 1017–1024. [Google Scholar] [CrossRef]
- Cerezo, A.; Leal, Á.; Álvarez-Fernández, M.; Hornedo-Ortega, R.; Troncoso, A.; García-Parrilla, M. Quality control and determination of melatonin in food supplements. J. Food Compos. Anal. 2016, 45, 80–86. [Google Scholar] [CrossRef]
- Erland, L.; Saxena, P. Melatonin Natural Health Products and Supplements: Presence of Serotonin and Significant Variability of Melatonin Content. J. Clin. Sleep Med. 2017, 13, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Palagini, L.; Manni, R.; Aguglia, E.; Amore, M.; Brugnoli, R.; Girardi, P.; Grassi, L.; Mencacci, C.; Plazzi, G.; Minervino, A.; et al. Expert Opinions and Consensus Recommendations for the Evaluation and Management of Insomnia in Clinical Practice: Joint Statements of Five Italian Scientific Societies. Front. Psychiatry 2020, 11, 558. [Google Scholar] [CrossRef] [PubMed]
- Zisapel, N. New perspectives on the role of melatonin in human sleep, circadian rhythms and their regulation. Br. J. Pharmacol. 2018, 175, 3190–3199. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.G.; Ford, I.; Crawford, G.; McMahon, A.D.; Nir, T.; Laudon, M.; Zisapel, N. Efficacy of prolonged release melatonin in insomnia patients aged 55–80 years: Quality of sleep and next-day alertness outcomes. Curr. Med. Res. Opin. 2007, 23, 2597–2605. [Google Scholar] [CrossRef] [PubMed]
- Luthringer, R.; Muzet, M.; Zisapel, N.; Staner, L. The effect of prolonged-release melatonin on sleep measures and psychomotor performance in elderly patients with insomnia. Int. Clin. Psychopharmacol. 2009, 24, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, G.D.; Laudon, M.; Nir, T.; Zisapel, N. Prolonged-release melatonin for insomnia—An open-label long-term study of efficacy, safety, and withdrawal. Ther. Clin. Risk Manag. 2011, 7, 301–311. [Google Scholar] [CrossRef] [Green Version]
- Arbon, E.; Knurowska, M.; Dijk, D. Randomised clinical trial of the effects of prolonged-release melatonin, temazepam and zolpidem on slow-wave activity during sleep in healthy people. J. Psychopharmacol. 2015, 29, 764–776. [Google Scholar] [CrossRef] [Green Version]
- Otmani, S.; Demazieres, A.; Staner, C.; Jacob, N.; Nir, T.; Zisapel, N.; Staner, L. Effects of prolonged-release melatonin, zolpidem, and their combination on psychomotor functions, memory recall, and driving skills in healthy middle aged and elderly volunteers. Hum. Psychopharmacol. Clin. Exp. 2008, 23, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Otmani, S.; Metzger, D.; Guichard, N.; Danjou, P.; Nir, T.; Zisapel, N.; Katz, A. Effects of prolonged-release melatonin and zolpidem on postural stability in older adults. Hum. Psychopharmacol. Clin. Exp. 2012, 27, 270–276. [Google Scholar] [CrossRef]
- Wilson, S.; Anderson, K. British Association for Psycopharmacology consensus statement on evidence based treatment of insomnia, parasomnias and citrcadian rhythm disorders: An update. J. Psychopharmacol. 2019, 33, 923–947. [Google Scholar] [CrossRef]
- Pinto, R.D.; Ferri, C.; Pengo, F.M.; Lombardi, C.; Pucci, C.; Salvetti, M.; Parati, G.; The Italian Society of Hypertension. Diagnostic and Therapeutic Approach to Sleep Disorders, High Blood Pressure and Cardiovascular Diseases: A Consensus Document by the Italian Society of Hypertension (SIIA). High Blood Press Cardiovasc. Prev. 2021, 28, 85–102. [Google Scholar] [CrossRef] [PubMed]
- Baller, E.B.; Hogan, C.S.; Fusunyan, M.A.; Ivkovic, A.; Luccarelli, J.W.; Madva, E.; Nisavic, M.; Praschan, N.; Quijije, N.V.; Beach, S.R.; et al. Neurocovid: Pharmacological Recommendations for Delirium Associated With COVID-19. Psychosomatics 2020, 61, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Duggan, M.C.; Van, J.; Ely, E.W. Assessment in Critically Ill Older Adults: Considerations During the COVID-19 Pandemic. Crit. Care Clin. 2021, 37, 175–190. [Google Scholar] [CrossRef]
- Martín Giménez, V.M.; Inserra, F.; Tajer, C.D.; Mariani, J.; Ferder, L.; Reiter, R.J.; Manucha, W. Lungs as target of COVID-19 infection: Protective common molecular mechanisms of vitamin D and melatonin as a new potential synergistic treatment. Life Sci. 2020, 254, 117808. [Google Scholar] [CrossRef] [PubMed]
- Bahrampour Juybari, K.; Pourhanifeh, M.H.; Hosseinzadeh, A.; Hemati, K.; Mehrzadi, S. Melatonin potentials against viral infections including COVID-19: Current evidence and new findings. Virus Res. 2020, 287, 198108. [Google Scholar] [CrossRef]
- Wiwanitkit, V. Delirium, sleep, COVID-19 and melatonin. Sleep Med. 2020, 75, 542. [Google Scholar] [CrossRef]
- Missiry, M.A.; El-Missiry, Z.M.A.; Othman, A.I. Melatonin is a potential adjuvant to improve clinical outcomes in individuals with obesity and diabetes with coexistence of COVID-19. J. Pharmacol. 2020, 882, 173329. [Google Scholar] [CrossRef]
- Reiter, R.J.; Abreu-Gonzalez, P.; Marik, P.E.; Dominguez-Rodriguez, A. Therapeutic Algorithm for Use of Melatonin in Patients With COVID-19. Front. Med. 2020, 7, 226. [Google Scholar] [CrossRef]
- Öztürk, G.; Akbulut, K.G.; Güney, Ş. Turk Melatonin, aging, and COVID-19: Could melatonin be beneficial for COVID-19 treatment in the elderly? Med. Sci. 2020, 50, 1504–1512. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group Treated with Melatonin 2 mg PR (n = 40) | Control Group Untreated (n = 40) | ||||
|---|---|---|---|---|---|
| Clinical parameters | Mean | Std. Dev. | Clinical parameters | Mean | Std. Dev. |
| BMI | 29.1 | 2.6 | BMI | 29.8 | 4.0 |
| Creatinine (mg/dL) | 1.4 | 0.4 | Creatinine (mg/dL) | 1.6 | 0.6 |
| Azotemia (mg/dL) | 64.5 | 22.9 | Azotemia (mg/dL) | 87.0 | 42.9 |
| Hemoglobin (mg/dL) | 11.0 | 1.2 | Hemoglobin (mg/dL) | 11.0 | 1.8 |
| Glycemia (mg/dL) | 112.6 | 30.5 | Glycemia (mg/dL) | 142.5 | 58.4 |
| GOT (UI/L) | 48.2 | 32.2 | GOT (UI/L) | 44.8 | 16.0 |
| GPT (UI/L) | 47.8 | 27.8 | GPT (UI/L) | 47.4 | 13.3 |
| PCR (mg/dL) | 19.5 | 15.6 | PCR (mg/dL) | 15.7 | 11.4 |
| Days | Group Treated with Melatonin 2 mg PR (Mean ± Std. Dev.) | Group Treatd with Melatonin 2 mg PR (Median QR) | Control Group Untreated (Mean ± Dev. Std.) | Control Group Untreated (Median IQR) | p-Value |
|---|---|---|---|---|---|
| Hospitalization | 31.3 ± 6.8 | 34.3 ± 6.9 | 0.03 | ||
| In subintensive care | 12.3 ± 3.2 | 20.1 ± 6.1 | <0.001 | ||
| With NIV Non Invasive Ventilation | 5.2 ± 3.0 | 5 (3–7.3) | 12.5 ± 4.2 | 11 (10–15.3) | <0.001 |
| With High flow oxygen ventilation | 7.1 ± 2.5 | 7 (5–8) | 7.7± 3.2 | 7 (5–10) | 0.436 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bologna, C.; Madonna, P.; Pone, E. Efficacy of Prolonged-Release Melatonin 2 mg (PRM 2 mg) Prescribed for Insomnia in Hospitalized Patients for COVID-19: A Retrospective Observational Study. J. Clin. Med. 2021, 10, 5857. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245857
Bologna C, Madonna P, Pone E. Efficacy of Prolonged-Release Melatonin 2 mg (PRM 2 mg) Prescribed for Insomnia in Hospitalized Patients for COVID-19: A Retrospective Observational Study. Journal of Clinical Medicine. 2021; 10(24):5857. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245857
Chicago/Turabian StyleBologna, Carolina, Pasquale Madonna, and Eduardo Pone. 2021. "Efficacy of Prolonged-Release Melatonin 2 mg (PRM 2 mg) Prescribed for Insomnia in Hospitalized Patients for COVID-19: A Retrospective Observational Study" Journal of Clinical Medicine 10, no. 24: 5857. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245857