
Health-Related Quality of Life Outcomes in Patients with Myelodysplastic Syndromes with Ring Sideroblasts Treated with Luspatercept in the MEDALIST Phase 3 Trial

 , ,
, , 
Abstract
:1. Introduction
2. Methods
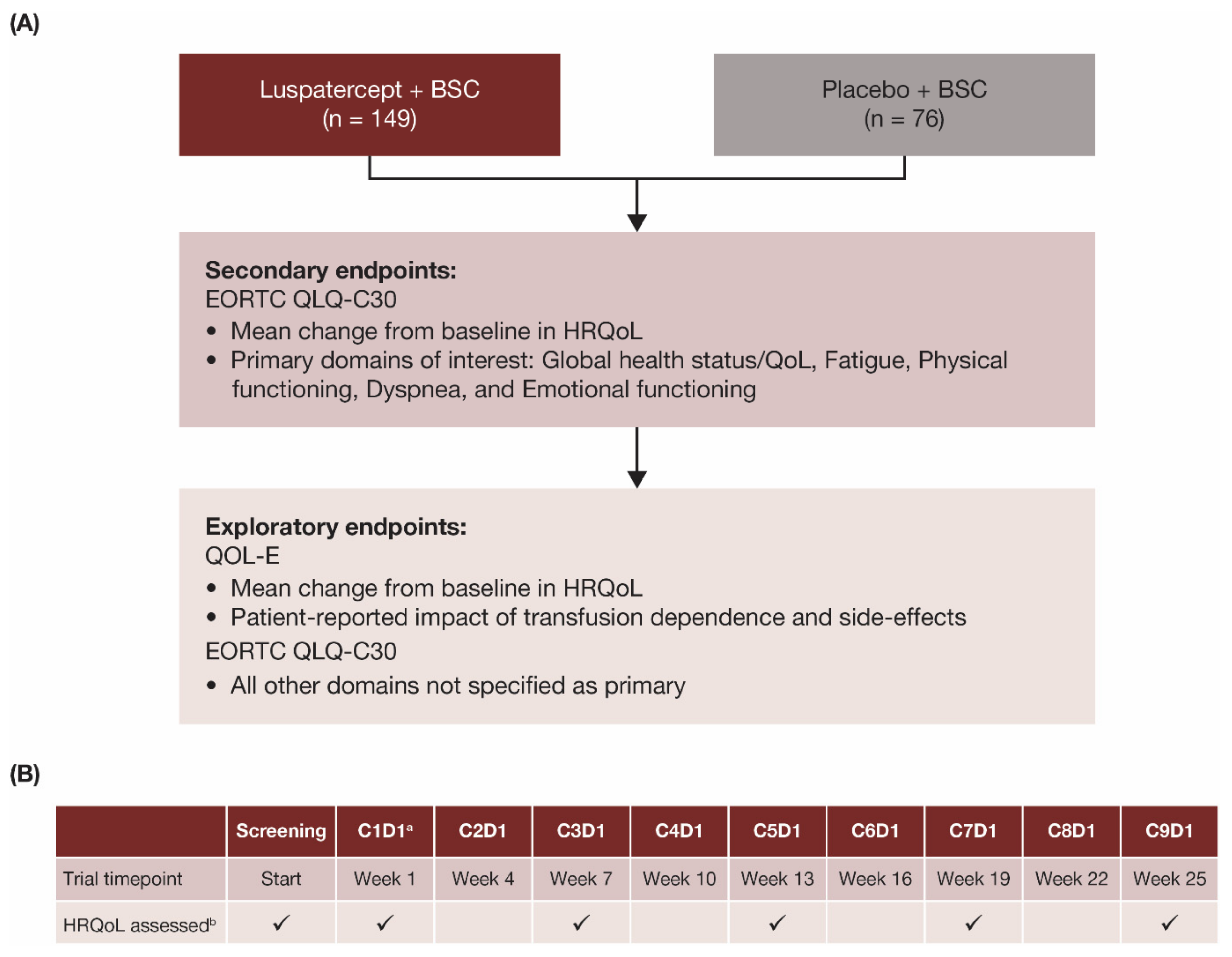
2.1. Study Design
2.2. Patient Selection
2.3. HRQoL Assessments
2.4. Statistical Analyses
3. Results
3.1. Patients
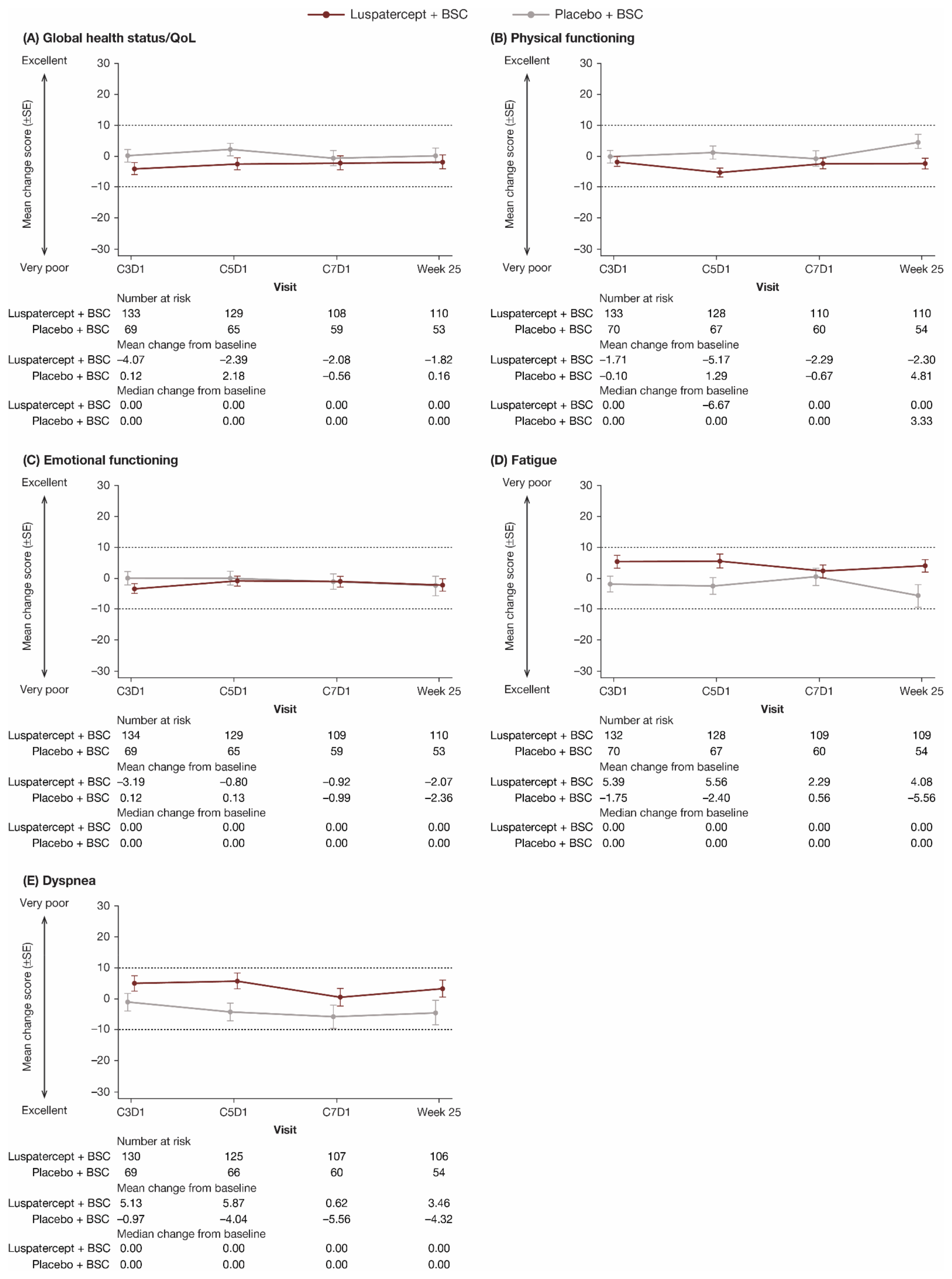
3.2. EORTC QLQ-C30 Assessment
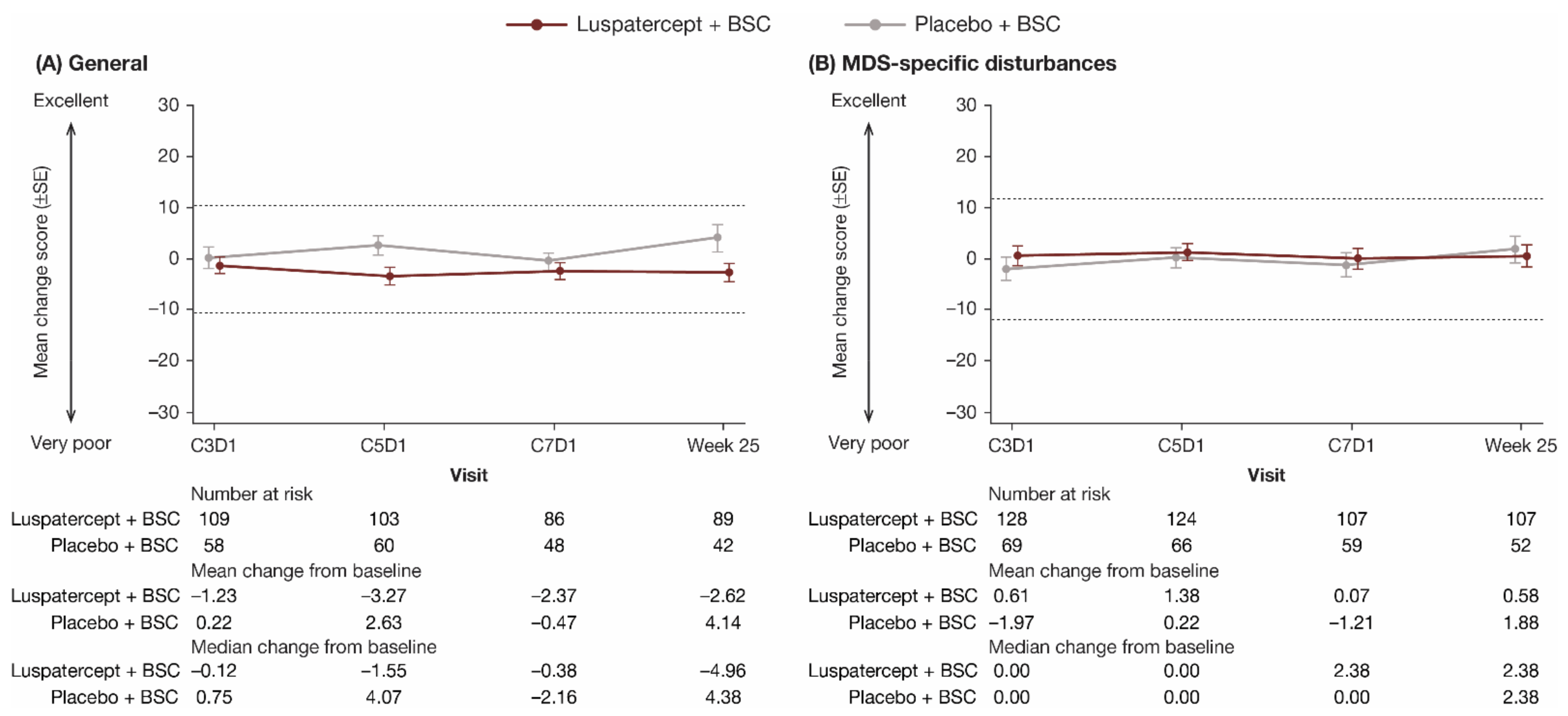
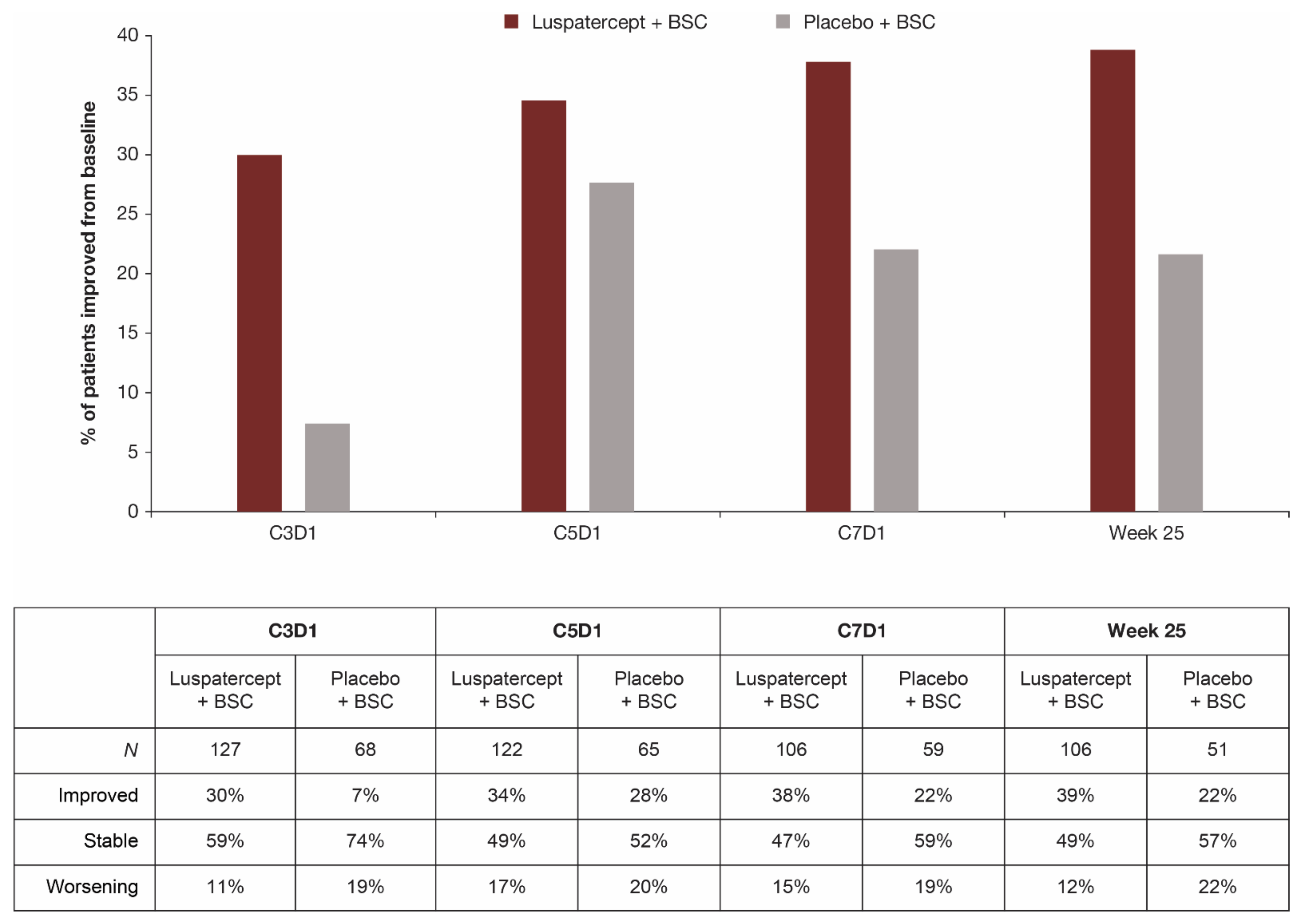
3.3. QOL-E Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeidan, A.M.; Linhares, Y.; Gore, S.D. Current therapy of myelodysplastic syndromes. Blood Rev. 2013, 27, 243–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adès, L.; Itzykson, R.; Fenaux, P. Myelodysplastic syndromes. Lancet 2014, 383, 2239–2252. [Google Scholar] [CrossRef]
- Malcovati, L. Red blood cell transfusion therapy and iron chelation in patients with myelodysplastic syndromes. Clin. Lymphoma Myeloma 2009, 9 (Suppl. 3), S305–S311. [Google Scholar] [CrossRef]
- Steensma, D.P.; Heptinstall, K.V.; Johnson, V.M.; Novotny, P.J.; Sloan, J.A.; Camoriano, J.K.; Niblack, J.; Bennett, J.M.; Mesa, R.A. Common troublesome symptoms and their impact on quality of life in patients with myelodysplastic syndromes (MDS): Results of a large internet-based survey. Leuk. Res. 2008, 32, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Sobrero, A.; Puglisi, F.; Guglielmi, A.; Belvedere, O.; Aprile, G.; Ramello, M.; Grossi, F. Fatigue: A main component of anemia symptomatology. Semin. Oncol. 2001, 28 (Suppl. 8), 15–18. [Google Scholar] [CrossRef]
- Oliva, E.N.; Dimitrov, B.D.; Benedetto, F.; D’Angelo, A.; Nobile, F. Hemoglobin level threshold for cardiac remodeling and quality of life in myelodysplastic syndrome. Leuk. Res. 2005, 29, 1217–1219. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.L.; Crisp, N.; Campbell, K. The importance of quality of life for patients living with myelodysplastic syndromes. Clin. J. Oncol. Nurs. 2012, 16 (Suppl. 16), 47–57. [Google Scholar] [CrossRef]
- Sekeres, M.A.; Stone, R.M.; Zahrieh, D.; Neuberg, D.; Morrison, V.; De Angelo, D.J.; Galinsky, I.; Lee, S.J. Decision-making and quality of life in older adults with acute myeloid leukemia or advanced myelodysplastic syndrome. Leukemia 2004, 18, 809–816. [Google Scholar] [CrossRef] [Green Version]
- Sekeres, M.A.; Maciejewski, J.P.; List, A.F.; Steensma, D.P.; Artz, A.; Swern, A.S.; Scribner, P.; Huber, J.; Stone, R. Perceptions of disease state, treatment outcomes, and prognosis among patients with myelodysplastic syndromes: Results from an internet-based survey. Oncologist 2011, 16, 904–911. [Google Scholar] [CrossRef] [Green Version]
- Platzbecker, U. Treatment of MDS. Blood 2019, 133, 1096–1107. [Google Scholar] [CrossRef] [Green Version]
- Pinchon, D.J.; Stanworth, S.J.; Dorée, C.; Brunskill, S.; Norfolk, D.R. Quality of life and use of red cell transfusion in patients with myelodysplastic syndromes. A systematic review. Am. J. Hematol. 2009, 84, 671–677. [Google Scholar] [CrossRef]
- Koutsavlis, I. Transfusion thresholds, quality of life, and current approaches in myelodysplastic syndromes. Anemia 2016, 2016, 8494738. [Google Scholar] [CrossRef] [Green Version]
- Malcovati, L.; Germing, U.; Kuendgen, A.; Della Porta, M.G.; Pascutto, C.; Invernizzi, R.; Giagounidis, A.; Hildebrandt, B.; Bernasconi, P.; Knipp, S.; et al. Time-dependent prognostic scoring system for predicting survival and leukemic evolution in myelodysplastic syndromes. J. Clin. Oncol. 2007, 25, 3503–3510. [Google Scholar] [CrossRef]
- Hellström-Lindberg, E.; Gulbrandsen, N.; Lindberg, G.; Ahlgren, T.; Dahl, I.M.; Dybedal, I.; Grimfors, G.; Hesse-Sundin, E.; Hjorth, M.; Kanter-Lewensohn, L.; et al. A validated decision model for treating the anaemia of myelodysplastic syndromes with erythropoietin + granulocyte colony-stimulating factor: Significant effects on quality of life. Br. J. Haematol. 2003, 120, 1037–1046. [Google Scholar] [CrossRef]
- Jansen, A.J.G.; Essink-Bot, M.-L.; Beckers, E.A.; Hop, W.C.; Schipperus, M.R.; Van Rhenen, D.J. Quality of life measurement in patients with transfusion-dependent myelodysplastic syndromes. Br. J. Haematol. 2003, 121, 270–274. [Google Scholar] [CrossRef]
- Thomas, M.L. Strategies for achieving transfusion independence in myelodysplastic syndromes. Eur. J. Oncol. Nurs. 2007, 11, 151–158. [Google Scholar] [CrossRef]
- Efficace, F.; Cottone, F.; Abel, G.; Niscola, P.; Gaidano, G.; Bonnetain, F.; Anota, A.; Caocci, G.; Cronin, A.; Fianchi, L.; et al. Patient-reported outcomes enhance the survival prediction of traditional disease risk classifications: An international study in patients with myelodysplastic syndromes. Cancer 2018, 124, 1251–1259. [Google Scholar] [CrossRef]
- Fenaux, P.; Platzbecker, U.; Mufti, G.J.; Garcia-Manero, G.; Buckstein, R.; Santini, V.; Díez-Campelo, M.; Finelli, C.; Cazzola, M.; Ilhan, O.; et al. Luspatercept in patients with lower-risk myelodysplastic syndromes. N. Engl. J. Med. 2020, 382, 140–151. [Google Scholar] [CrossRef]
- Kubasch, A.S.; Fenaux, P.; Platzbecker, U. Development of luspatercept to treat ineffective erythropoiesis. Blood Adv. 2021, 5, 1565–1575. [Google Scholar] [CrossRef]
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001; Available online: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf (accessed on 21 December 2021).
- Oliva, E.; Nobile, F.; Dimitrov, B. Development and validation of QOL-E© instrument for the assessment of health-related quality of life in myelodysplastic syndromes. Cent. Eur. J. Med. 2013, 8, 835–844. [Google Scholar] [CrossRef]
- Osoba, D.; Rodrigues, G.; Myles, J.; Zee, B.; Pater, J. Interpreting the significance of changes in health-related quality-of-life scores. J. Clin. Oncol. 1998, 16, 139–144. [Google Scholar] [CrossRef]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. The truly remarkable universality of half a standard deviation: Confirmation through another look. Expert Rev. Pharmacoecon. Outcomes Res. 2004, 4, 581–585. [Google Scholar] [CrossRef]
- Nolte, S.; Liegl, G.; Patersen, M.A.; Aaronson, N.K.; Costantini, A.; Fayers, P.M.; Groenvold, M.; Holzner, B.; Johnson, C.D.; Kemmler, G.; et al. General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries, Canada and the United States. Eur. J. Cancer 2019, 107, 153–163. [Google Scholar] [CrossRef]
- Scott, N.W.; Fayers, P.M.; Aaronson, N.K.; Bottomley, A.; de Graeff, A.; Groenvold, M.; Gundy, C.; Koller, M.; Petersen, M.A.; Sprangers, M.A.G. EORTC QLQ-C30 Reference Values; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2008; Available online: https://www.eortc.org/app/uploads/sites/2/2018/02/reference_values_manual2008.pdf (accessed on 21 December 2021).
- Platzbecker, U.; Germing, U.; Götze, K.S.; Kiewe, P.; Mayer, K.; Chromik, J.; Radsak, M.; Wolff, T.; Zhang, X.; Laadem, A.; et al. Luspatercept for the treatment of anaemia in patients with lower-risk myelodysplastic syndromes (PACE-MDS): A multicentre, open-label phase 2 dose-finding study with long-term extension study. Lancet Oncol. 2017, 18, 338–1347. [Google Scholar] [CrossRef]
- Kornblith, A.B.; Herndon, J.E.; Silverman, L.R.; Demakos, E.P.; Odchimar-Reissig, R.; Holland, J.F.; Powell, B.L.; DeCastro, C.; Ellerton, J.; Larson, R.A.; et al. Impact of azacytidine on the quality of life of patients with myelodysplastic syndrome treated in a randomized phase III trial: A Cancer and Leukemia Group B study. J. Clin. Oncol. 2002, 20, 2441–2452. [Google Scholar] [CrossRef]
- Bowen, D.; Culligan, D.; Jowitt, S.; Kelsey, S.; Mufti, G.; Oscier, D.; Parker, J. Guidelines for the diagnosis and therapy of adult myelodysplastic syndromes. Br. J. Haematol. 2003, 120, 187–200. [Google Scholar] [CrossRef]
- Lawrence, L.W. Refractory anemia and the myelodysplastic syndromes. Clin. Lab. Sci. 2004, 17, 178–186. [Google Scholar]
- Fenaux, P.; Santini, V.; Spiriti, M.A.A.; Giagounidis, A.; Schlag, R.; Radinoff, A.; Gercheva-Kyuchukova, L.; Anagnostopoulos, A.; Oliva, E.N.; Symeonidis, A.; et al. A phase 3 randomized, placebo-controlled study assessing the efficacy and safety of epoetin-α in anemic patients with low-risk MDS. Leukemia 2018, 32, 2648–2658. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, P.L.; Sun, Z.; Miller, K.B.; Bennett, J.M.; Tallman, M.S.; Dewald, G.; Paietta, E.; van der Jagt, R.; Houston, J.; Thomas, M.L.; et al. Treatment of myelodysplastic syndrome patients with erythropoietin with or without granulocyte colony-stimulating factor: Results of a prospective randomized phase 3 trial by the Eastern Cooperative Oncology Group (E1996). Blood 2009, 114, 2393–2400. [Google Scholar] [CrossRef] [Green Version]
- Spiriti, M.A.; Latagliata, R.; Niscola, P.; Cortelezzi, A.; Francesconi, M.; Ferrari, D.; Volpe, E.; Clavio, M.; Grossi, A.; Reye, M.T.; et al. Impact of a new dosing regimen of epoetin alfa on quality of life and anemia in patients with low-risk myelodysplastic syndrome. Ann. Hematol. 2005, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Kelaidi, C.; Beyne-Rauzy, O.; Braun, T.; Sapena, R.; Cougoul, P.; Adès, L.; Pillard, F.; Lamberto, C.; Charniot, J.C.; Guerci, A.; et al. High response rate and improved exercise capacity and quality of life with a new regimen of darbepoetin alfa with or without filgrastim in lower-risk myelodysplastic syndromes: A phase II study by the GFM. Ann. Hematol. 2013, 92, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Villegas, A.; Arrizabalaga, B.; Fernandez-Lago, C.; Castro, M.; Mayans, J.R.; Gonzalez-Porras, J.R.; Duarte, R.F.; Remacha, A.F.; Luño, E.; Gasquet, J.A. Darbepoetin alfa for anemia in patients with low or intermediate-1 risk myelodysplastic syndromes and positive predictive factors of response. Curr. Med. Res. Opin. 2011, 27, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Gabrilove, J.; Paquette, R.; Lyons, R.M.; Mushtaq, C.; Sekeres, M.A.; Tomita, D.; Dreiling, L. Phase 2, single-arm trial to evaluate the effectiveness of darbepoetin alfa for correcting anaemia in patients with myelodysplastic syndromes. Br. J. Haematol. 2008, 142, 379–393. [Google Scholar] [CrossRef]
- Stasi, R.; Abruzzese, E.; Lanzetta, G.; Terzoli, E.; Amadori, S. Darbepoetin alfa for the treatment of anemic patients with low- and intermediate-1-risk myelodysplastic syndromes. Ann. Oncol. 2005, 16, 1921–1927. [Google Scholar] [CrossRef]
- Santini, V.; Almeida, A.; Giagounidis, A.; Platzbecker, U.; Buckstein, R.; Beach, C.L.; Guo, S.; Altincatal, A.; Wu, C.; Fenaux, P. The effect of lenalidomide on health-related quality of life in patients with lower-risk non-del(5q) myelodysplastic syndromes: Results from the MDS-005 Study. Clin. Lymphoma Myeloma Leuk. 2018, 18, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Oliva, E.N.; Latagliata, R.; Lagana, C.; Breccia, M.; Galimberti, S.; Morabito, F.; Poloni, A.; Balleari, E.; Cortelezzi, A.; Palumbo, G.; et al. Lenalidomide in International Prognostic Scoring System Low and Intermediate-1 risk myelodysplastic syndromes with del(5q): An Italian phase II trial of health-related quality of life, safety and efficacy. Leuk. Lymphoma 2013, 54, 2458–2465. [Google Scholar] [CrossRef]
- Revicki, D.A.; Brandenburg, N.A.; Muus, P.; Yu, R.; Knight, R.; Fenaux, P. Health-related quality of life outcomes of lenalidomide in transfusion-dependent patients with Low- or Intermediate-1-risk myelodysplastic syndromes with a chromosome 5q deletion: Results from a randomized clinical trial. Leuk. Res. 2013, 37, 259–265. [Google Scholar] [CrossRef]
- Fenaux, P.; Giagounidis, A.; Selleslag, D.; Beyne-Rauzy, O.; Mufti, G.; Mittelman, M.; Muus, P.; Te Boekhorst, P.; Sanz, G.; Del Cañizo, C.; et al. A randomized phase 3 study of lenalidomide versus placebo in RBC transfusion-dependent patients with Low-/Intermediate-1-risk myelodysplastic syndromes with del5q. Blood 2011, 118, 3765–3776. [Google Scholar] [CrossRef]
- Lefebvre, P.; Vekeman, F.; Sarokhan, B.; Enny, C.; Provenzano, R.; Cremieux, P.Y. Relationship between hemoglobin level and quality of life in anemic patients with chronic kidney disease receiving epoetin alfa. Curr. Med. Res. Opin. 2006, 22, 1929–1937. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Luspatercept + BSC (n = 149) | Placebo + BSC (n = 76) | Total (N = 225) |
|---|---|---|---|
| Age, years, mean (SD) | 70.5 (8.7) | 70.7 (10.9) | 70.6 (9.4) |
| Age group, years, n (%) | |||
| ≤64 | 28 (18.8) | 16 (21.1) | 44 (19.6) |
| 65–74 | 70 (47.0) | 29 (38.2) | 99 (44.0) |
| ≥75 | 51 (34.2) | 31 (40.8) | 82 (36.4) |
| Sex, n (%) | |||
| Male | 93 (62.4) | 50 (65.8) | 143 (63.6) |
| Race, n (%) | |||
| White | 105 (70.5) | 51 (67.1) | 156 (69.3) |
| Black | 1 (0.7) | 0 (0.0) | 1 (0.4) |
| Not collected | 42 (28.2) | 24 (31.6) | 66 (29.3) |
| Other | 1 (0.7) | 1 (1.3) | 2 (0.9) |
| IPSS-R risk, n (%) | |||
| Very low or low | 123 (82.6) | 63 (82.9) | 186 (82.7) |
| Intermediate | 25 (16.8) | 13 (17.1) | 38 (16.9) |
| Missing | 1 (0.7) | 0 (0.0) | 1 (0.4) |
| Prior ESA use, n (%) | |||
| Yes | 144 (96.6) | 70 (92.1) | 214 (95.1) |
| Transfusion burden, n (%) | |||
| <4 RBCT units/8 weeks | 44 (29.5) | 20 (26.3) | 64 (28.4) |
| 4–5 RBCT units/8 weeks | 40 (26.8) | 23 (30.3) | 63 (28.0) |
| ≥6 RBCT units/8 weeks | 65 (43.6) | 33 (43.4) | 98 (43.6) |
| EORTC QLQ-C30 Domain a | Baseline Score in MEDALIST b Mean (SD) (N = 225) | Mean Score in General Population c (N = 11,343) | Mean Score in Patients with Recurrent/Metastatic Cancer d (N = 4812) |
|---|---|---|---|
| Global health status/QoL | 58.3 (20.1) | 67.1 | 56.3 |
| Physical functioning | 66.3 (21.1) | 82.5 | 75.8 |
| Role functioning | 65.1 (29.5) | 83.8 | 60.7 |
| Cognitive functioning | 82.1 (20.3) | 87.2 | 80.5 |
| Emotional functioning | 76.9 (19.9) | 81.6 | 68.7 |
| Social functioning | 74.3 (27.8) | 89.1 | 70.5 |
| Fatigue | 42.9 (24.6) | 24.9 | 41.8 |
| Nausea/vomiting | 5.0 (12.2) | 2.5 | 13.1 |
| Pain | 18.9 (24.6) | 23.2 | 33.7 |
| Dyspnea | 35.7 (29.5) | 17.0 | 23.4 |
| Insomnia | 27.5 (30.8) | 24.0 | 33.6 |
| Appetite loss | 14.4 (23.9) | 6.8 | 28.2 |
| Constipation | 17.6 (27.0) | 10.7 | 23.2 |
| Diarrhea | 8.9 (18.4) | 6.2 | 10.7 |
| Financial difficulties | 11.0 (22.9) | 7.6 | 16.2 |
| EORTC QLQ-C30 Domain | LS Mean (SE) Difference b at Week 25 |
|---|---|
| Global health status/QoL | −3.76 (2.88) |
| Physical functioning | −7.13 (2.50) |
| Role functioning | −5.12 (4.15) |
| Cognitive functioning | 1.62 (2.78) |
| Emotional functioning | −0.51 (2.89) |
| Social functioning | −3.12 (3.89) |
| Fatigue | 6.76 (3.24) |
| Nausea/vomiting | −0.67 (1.96) |
| Pain | −1.07 (3.42) |
| Dyspnea | 5.55 (3.87) |
| Insomnia | −1.04 (3.78) |
| Appetite loss | 0.32 (3.73) |
| Constipation | 3.80 (3.22) |
| Diarrhea | −0.86 (2.62) |
| Financial difficulties | 0.58 (2.48) |
| QOL-E Domain a | Baseline Score in MEDALIST Mean (SD) (N = 225) |
|---|---|
| Physical well-being | 52.9 (21.5) |
| Functional well-being | 53.7 (32.4) |
| Social and family life | 48.4 (37.6) |
| Sexual well-being | 62.4 (36.3) |
| Fatigue | 75.0 (14.1) |
| MDS-specific disturbances | 57.0 (23.7) |
| Treatment outcome index b | 54.7 (20.7) |
| General c | 58.7 (21.1) |
| All d | 58.1 (21.1) |
| QOL-E Domain | LS Mean (SE) Difference b at Week 25 | MCID |
|---|---|---|
| Physical well-being | −5.28 (3.18) | 10.74 |
| Functional well-being | −6.07 (4.63) | 16.16 |
| Social and family life | −8.70 (4.50) | 18.76 |
| Sexual well-being | 0.31 (4.49) | 18.08 |
| Fatigue | −5.10 (2.03) | 7.03 |
| MDS-specific disturbances | −2.03 (3.01) | 11.86 |
| Treatment outcome index c | −4.71 (2.80) | 10.33 |
| General d | −6.30 (2.50) | 10.51 |
| All e | −5.10 (2.70) | 10.55 |
| MDS-Specific Disturbances | Baseline, n/N (%) | Week 25, n/N (%) | ||
|---|---|---|---|---|
| Luspatercept + BSC | Placebo + BSC | Luspatercept + BSC | Placebo + BSC | |
| Patients responding “Not at all” | ||||
| Being dependent on transfusions disturbs your daily life | 22/147 (15.0) | 19/74 (25.7) | 48/108 (44.4) | 11/52 (21.2) |
| Not being able to do housework disturbs your daily life | 57/147 (38.8) | 32/75 (42.7) | 49/109 (45.0) | 26/53 (49.1) |
| Not being able to travel either short or long distances disturbs your daily life | 54/147 (36.7) | 25/75 (33.3) | 40/109 (36.7) | 20/53 (37.7) |
| Being dependent on the hospital, doctors, and/or nurses disturbs your daily life | 56/145 (38.6) | 30/74 (40.5) | 43/108 (39.8) | 16/53 (30.2) |
| Stress and worry because of the illness disturb your daily life | 41/149 (27.5) | 19/75 (25.3) | 33/108 (30.6) | 18/53 (34.0) |
| Side-effects of the treatment disturb your daily life | 91/143 (63.6) | 48/74 (64.9) | 57/106 (53.8) | 32/53 (60.4) |
| Patients responding “Never” | ||||
| During the last week did shortness of breath disturb you? | 36/147 (24.5) | 12/76 (15.8) | 19/107 (17.8) | 11/53 (20.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliva, E.N.; Platzbecker, U.; Garcia-Manero, G.; Mufti, G.J.; Santini, V.; Sekeres, M.A.; Komrokji, R.S.; Shetty, J.K.; Tang, D.; Guo, S.; et al. Health-Related Quality of Life Outcomes in Patients with Myelodysplastic Syndromes with Ring Sideroblasts Treated with Luspatercept in the MEDALIST Phase 3 Trial. J. Clin. Med. 2022, 11, 27. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010027
Oliva EN, Platzbecker U, Garcia-Manero G, Mufti GJ, Santini V, Sekeres MA, Komrokji RS, Shetty JK, Tang D, Guo S, et al. Health-Related Quality of Life Outcomes in Patients with Myelodysplastic Syndromes with Ring Sideroblasts Treated with Luspatercept in the MEDALIST Phase 3 Trial. Journal of Clinical Medicine. 2022; 11(1):27. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010027
Chicago/Turabian StyleOliva, Esther Natalie, Uwe Platzbecker, Guillermo Garcia-Manero, Ghulam J. Mufti, Valeria Santini, Mikkael A. Sekeres, Rami S. Komrokji, Jeevan K. Shetty, Derek Tang, Shien Guo, and et al. 2022. "Health-Related Quality of Life Outcomes in Patients with Myelodysplastic Syndromes with Ring Sideroblasts Treated with Luspatercept in the MEDALIST Phase 3 Trial" Journal of Clinical Medicine 11, no. 1: 27. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010027