
Lifestyle and Pain following Cancer: State-of-the-Art and Future Directions

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
3. State-of-the-Art
3.1. Pain
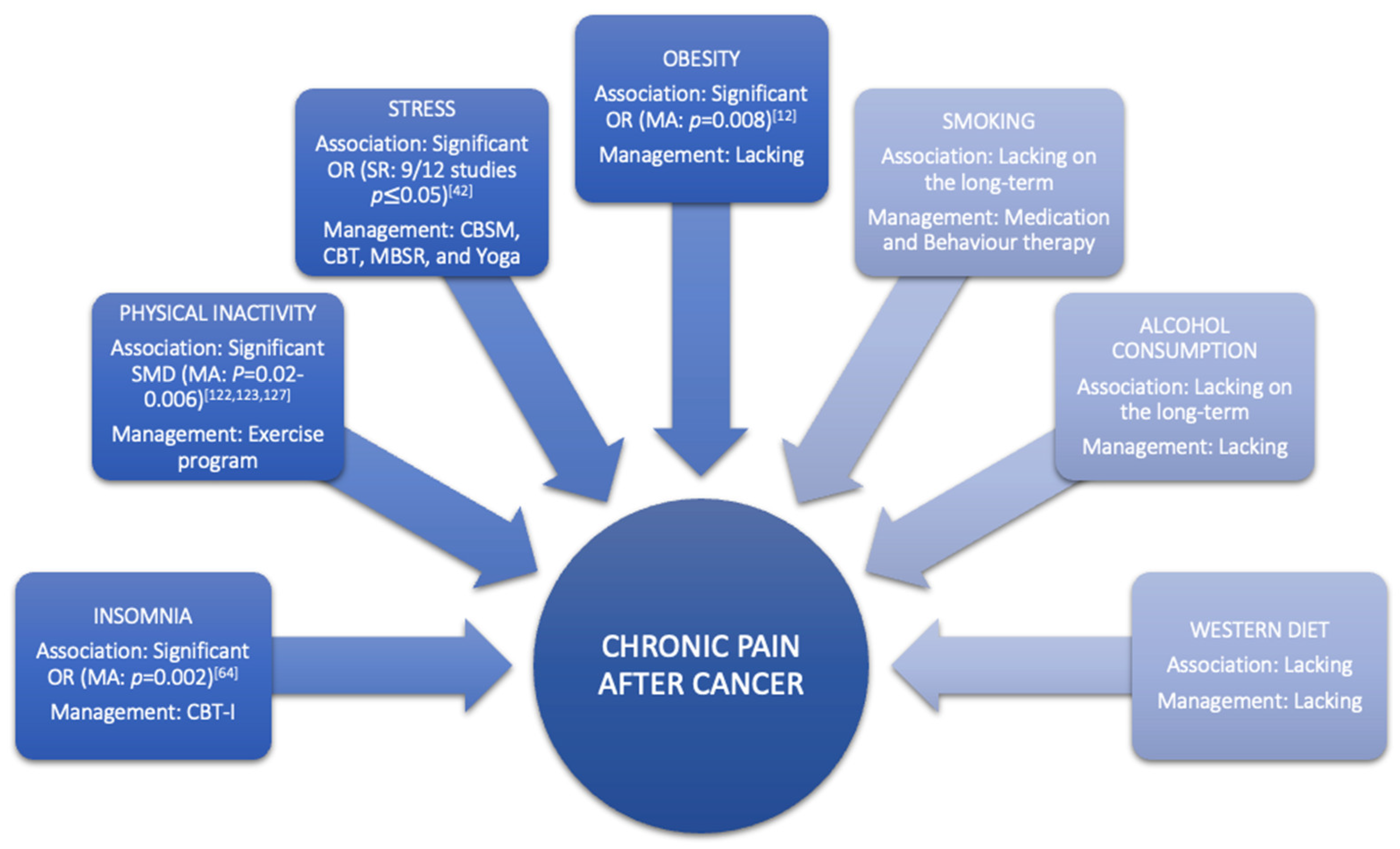
3.2. Lifestyle Behaviour
3.2.1. Stress
3.2.2. Sleep
3.2.3. Diet
Dietary Intake
Obesity
3.2.4. Smoking
3.2.5. Alcohol Consumption
3.2.6. Physical Activity

{kind=link}
{kind=link}
| Lifestyle Factor | First Author, Year Published, Study Type | Included Population | Number of Included Studies (n1) and Participants (n2) | Detail of Lifestyle Factor/Intervention Assessed | Main Results in Context of the Specified State-of-the-Art | Level of Evidence [136] |
|---|---|---|---|---|---|---|
| Alcohol consumption | Leysen et al., 2017, Systematic review with meta-analysis [12] | Breast Cancer Survivors | n1 = 2 (1 CS and 1 C) and n2 = 2519 | Alcohol use | Alcohol (OR 0.94, 95% CI [0.47, 1.89], p = 0.86, I2 = 67%) was not a predictor for pain, Inconsistent and low evidence | 3b |
| Diet | Kim et al., 2018, Systematic review of systematic reviews [81] | Breast Cancer Survivors with AIA | n1 = 3 (systematic review of RCT), and n2_Omega-3 = 817, and n2_VD = 453 | Omega-3 Fatty Acids, and Vitamin D | Significant effects were found for omega-3 fatty acids (MD −2.10, 95% CI [−3.23, −0.97]), and vitamin D (MD 0.63, 95% CI [0.13, 1.13]) on pain, Low evidence | 1a |
| Yilmaz et al., 2021, Systematic review [80] | Cancer Survivors | n1 = 2 (uncontrolled clinical trial) and n2 = 77 | Nutritional supplements: vitamin C, chondroitin, and glucosamine | Lack of evidence | 2a | |
| Obesity | Leysen et al., 2017, Systematic review with meta-analysis [12] | Breast Cancer Survivors | n1 = 7 (4 CS and 3 C) and n2 = 5573 | BMI | BMI > 30 (OR 1.34, 95% CI [1.08, 1.67], p = 0.008, I2 = 33%,) was a predictor for pain, Consistent and low evidence | 3b |
| Timmins et al., 2021, Systematic review [88] | Cancer Survivors | n1 = 16 (3 CS, 11 C, and 2 retrospective chart review) and n2 = 14,033 | Obesity | According to the SORT: the association between obesity and CIPN was good-to-moderate patient-centred evidence | 3b | |
| Physical Activity | Boing et al., 2020, Systematic review with meta-analysis [123] | Breast Cancer Survivors with AIA | n1 = 3 (2 RCT, 1 pilot study), and n2 = 118 | Exercise | Significant effect was found on pain (SMD −0.55, 95 % CI [−1.11, −0.00], p = 0.05 I2 = 80%), Low Evidence | 1b |
| Kim et al., 2018, Systematic review of systematic reviews [81] | Breast Cancer Survivors with AIA | n1 = 2 (systematic review of RCT), and n2 = 262 | Aerobic Exercise | No significant effect was found on pain (MD −0.80, 95% CI [−1.33, 0.016]), Low evidence | 1a | |
| Lavín-Pérez et al., 2021, Systematic review with meta-analysis [127] | Cancer Survivors | n1 = 7 (RCT), and n2 = 355 | Exercise (HIT) | Significant effect was found on pain (SMD −0.18, 95% CI [−0.34, −0.02], p = 0.02, I2 = 4%), Moderate evidence | 1a | |
| Lu et al., 2020, Systematic review with meta-analysis [122] | Breast Cancer Survivors with AIA | n1 = 6 (RCT), and n2 = 416 | Exercise | Significant effect was found on pain (SMD −0.46, 95% CI [−0.79, −0.13], p = 0.006, I2 = 63%), Moderate evidence | 1a | |
| Timmins et al., 2021, Systematic review [88] | Cancer Survivors | n1 = 5 (2 C and 3 CS), and n2 = 3950 | Low physical activity | According to the SORT: the association between physical inactivity and CIPN was of moderate evidence | 3b | |
| Sleep | Leysen et al., 2019, Systematic review with meta-analysis [64] | Breast Cancer Survivors | n1 = 4 (2 CS and 2 C) and n2 = 1907 | Sleep Disturbances | Pain was a predictor for sleep disturbances (OR 1.68, 95% CI [1.19, 2.37], p = 0.05, I2 = 55%, after subgroup analysis OR 2.31, 95% CI [1.36, 3.92], p = 0.002, I2 = 27%) | 3b |
| Smoking | Leysen et al., 2017, Systematic review with meta-analysis [12] | Breast Cancer Survivors | n1 = 2 (1 CS and 1 C) and n2 = 2519 | Smoking status | Smoking (OR 0.75, 95% CI [0.62, 0.92], p = 0.005, I2 = 0%) was not a predictor for pain, Consistent and low evidence | 3b |
| Stress | Syrowatka et al., 2017, Systematic review [42] | Breast Cancer Survivors | n1 = 12 (6 CS and 6 C) and n2 = 7842 | Distress | Pain was significantly associated with distress: 9/12 studies (75%) | 3b |
| Intervention | Chang et al., 2020, Systematic review with meta-analysis [54] | Breast Cancer Survivors | n1 = 5 (RCT) and n2 = 827 | Mindfulness-Based interventions | No significant effect was found on pain (SMD −0.39, 95% CI, [−0.81, 0.03], p = 0.07, I2 = 85%), Moderate evidence | 1a |
| Cillessen et al., 2019, Systematic review with meta-analysis [133] | Cancer Patients and Survivors | n1 = 4 (RCT) and n2 = 587 | Mindfulness-Based interventions | Significant effect was found on pain (ES 0.2, 95% CI [0.04, 0.36], p = 0.16, I2 = 0%), Moderate evidence | 1a | |
| Martinez-Miranda [26] | Breast Cancer Survivors | n1 = 2 (RCT) and n2 = 134 | Patient Education | No significant effect was found on pain (SMD −0.05, 95% CI [−0.26, 0.17], p = 0.67, I2 = 0%, Low evidence | 1a | |
| Silva et al., 2019, Systematic review [137] | Cancer Survivors | n1 = 4 (4 quasi-experimental studies), and n2 = 522 | Promoting healthy behaviour by mHealth apps | Effect found on pain was inconsistent and of low quality of evidence | 2b |
4. Future Directions for Scientists
5. Future Directions for Clinicians
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahase, E. Cancer ovet alertakes CVD to become leading cause of death in high income countries. BMJ 2019, 366, l5368. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Viale, P.H. The American Cancer Society’s facts & figures: 2020 edition. J. Adv. Pract. Oncol. 2020, 11, 135. [Google Scholar]
- Marzorati, C.; Riva, S.; Pravettoni, G. Who Is a Cancer Survivor? A Systematic Review of Published Definitions. J. Cancer Educ. 2017, 32, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Pachman, D.R.; Barton, D.L.; Swetz, K.M.; Loprinzi, C.L. Troublesome symptoms in cancer survivors: Fatigue, insomnia, neuropathy, and pain. J. Clin. Oncol. 2012, 30, 3687–3696. [Google Scholar] [CrossRef] [PubMed]
- Van den Beuken-van Everdingen, M.H.; Hochstenbach, L.M.; Joosten, E.A.; Tjan-Heijnen, V.C.; Janssen, D.J. Update on Prevalence of Pain in Patients With Cancer: Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2016, 51, 1070–1090.e9. [Google Scholar] [CrossRef] [Green Version]
- Bennett, M.I.; Kaasa, S.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.D. The IASP classification of chronic pain for ICD-11: Chronic cancer-related pain. Pain 2019, 160, 38–44. [Google Scholar] [CrossRef]
- Tevaarwerk, A.; Denlinger, C.S.; Sanft, T.; Ansbaugh, S.M.; Armenian, S.; Baker, K.S.; Broderick, G.; Day, A.; Demark-Wahnefried, W.; Dickinson, K.; et al. Survivorship, Version 1.2021: Featured Updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2021, 19, 676–685. [Google Scholar] [CrossRef] [PubMed]
- Paice, J.A.; Portenoy, R.; Lacchetti, C.; Campbell, T.; Cheville, A.; Citron, M.; Constine, L.S.; Cooper, A.; Glare, P.; Keefe, F. Management of Chronic Pain in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 3325–3345. [Google Scholar] [CrossRef] [Green Version]
- Moloney, N.A.; Pocovi, N.C.; Dylke, E.S.; Graham, P.L.; De Groef, A. Psychological Factors Are Associated with Pain at All Time Frames After Breast Cancer Surgery: A Systematic Review with Meta-Analyses. Pain Med. 2021, 22, 915–947. [Google Scholar] [CrossRef]
- Wang, L.; Guyatt, G.H.; Kennedy, S.A.; Romerosa, B.; Kwon, H.Y.; Kaushal, A.; Chang, Y.; Craigie, S.; de Almeida, C.P.B.; Courban, R.J.; et al. Predictors of persistent pain after breast cancer surgery: A systematic review and meta-analysis of observational studies. CMAJ 2016, 188, E352–E361. [Google Scholar] [CrossRef] [Green Version]
- Leysen, L.; Beckwée, D.; Nijs, J.; Pas, R.; Bilterys, T.; Vermeir, S.; Adriaenssens, N. Risk factors of pain in breast cancer survivors: A systematic review and meta-analysis. Support. Care Cancer 2017, 25, 3607–3643. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Rogers, L.Q.; Alfano, C.M.; Thomson, C.A.; Courneya, K.S.; Meyerhardt, J.A.; Stout, N.L.; Kvale, E.; Ganzer, H.; Ligibel, J.A. Practical clinical interventions for diet, physical activity, and weight control in cancer survivors. CA Cancer J. Clin. 2015, 65, 167–189. [Google Scholar] [CrossRef]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Ramírez-Vélez, R. Effects of supervised exercise on cancer-related fatigue in breast cancer survivors: A systematic review and meta-analysis. BMC Cancer 2015, 15, 77. [Google Scholar] [CrossRef] [Green Version]
- Kessels, E.; Husson, O.; van der Feltz-Cornelis, C.M. The effect of exercise on cancer-related fatigue in cancer survivors: A systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 2018, 14, 479–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, J.T.; Hartland, M.C.; Maloney, L.T.; Davison, K. Therapeutic effects of aerobic and resistance exercises for cancer survivors: A systematic review of meta-analyses of clinical trials. Br. J. Sports Med. 2018, 52, 1311. [Google Scholar] [CrossRef] [PubMed]
- Bobyrov, V. Bases of Bioethics and Biosafety: Study Guide for Stud. of Higher Med. Est; Hoва Kнига: Vinnytsia, Ukraine, 2012. [Google Scholar]
- Maindet, C.; Burnod, A.; Minello, C.; George, B.; Allano, G.; Lemaire, A. Strategies of complementary and integrative therapies in cancer-related pain-attaining exhaustive cancer pain management. Support. Care Cancer 2019, 27, 3119–3132. [Google Scholar] [CrossRef] [PubMed]
- Glare, P.A.; Davies, P.S.; Finlay, E.; Gulati, A.; Lemanne, D.; Moryl, N.; Oeffinger, K.C.; Paice, J.A.; Stubblefield, M.D.; Syrjala, K.L. Pain in cancer survivors. J. Clin. Oncol. 2014, 32, 1739. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.R.; Ramirez, J.D.; Farquhar-Smith, P. Pain in cancer survivors. Br. J. Pain 2014, 8, 139–153. [Google Scholar] [CrossRef] [Green Version]
- Sun, V.; <monospace> </monospace>Borneman, T.; Piper, B.; Koczywas, M.; Ferrell, B. Barriers to pain assessment and management in cancer survivorship. J. Cancer Surviv. 2008, 2, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Chow, R.; Saunders, K.; Burke, H.; Belanger, A.; Chow, E. Needs assessment of primary care physicians in the management of chronic pain in cancer survivors. Support. Care Cancer 2017, 25, 3505–3514. [Google Scholar] [CrossRef]
- Oldenmenger, W.H.; Geerling, J.I.; Mostovaya, I.; Vissers, K.C.; de Graeff, A.; Reyners, A.K.; van der Linden, Y.M. A systematic review of the effectiveness of patient-based educational interventions to improve cancer-related pain. Cancer Treat. Rev. 2018, 63, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Binkley, J.M.; Harris, S.R.; Levangie, P.K.; Pearl, M.; Guglielmino, J.; Kraus, V.; Rowden, D. Patient perspectives on breast cancer treatment side effects and the prospective surveillance model for physical rehabilitation for women with breast cancer. Cancer 2012, 118, 2207–2216. [Google Scholar] [CrossRef]
- McGuire, D.B. Occurrence of cancer pain. J. Natl. Cancer Inst. Monogrphs 2004, 2004, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Miranda, P.; Casuso-Holgado, M.J.; Jiménez-Rejano, J.J. Effect of patient education on quality-of-life, pain and fatigue in breast cancer survivors: A systematic review and meta-analysis. Clin. Rehabil. 2021, 35, 1722–1742. [Google Scholar] [CrossRef] [PubMed]
- Boland, E.G.; Ahmedzai, S.H. Persistent pain in cancer survivors. Curr. Opin. Support Palliat. Care 2017, 11, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Ong, W.Y.; Stohler, C.S.; Herr, D.R. Role of the Prefrontal Cortex in Pain Processing. Mol. Neurobiol. 2019, 56, 1137–1166. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.J.; Scott, W.; Trost, Z. Perceived injustice: A risk factor for problematic pain outcomes. Clin. J. Pain. 2012, 28, 484–488. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.J.; Davidson, N.; Garfinkel, B.; Siriapaipant, N.; Scott, W. Perceived injustice is associated with heightened pain behavior and disability in individuals with whiplash injuries. Psychol. Inj. Law 2009, 2, 238–247. [Google Scholar] [CrossRef]
- Carriere, J.S.; Donayre Pimentel, S.; Yakobov, E.; Edwards, R.R. A Systematic Review of the Association Between Perceived Injustice and Pain-Related Outcomes in Individuals with Musculoskeletal Pain. Pain Med. 2020, 21, 1449–1463. [Google Scholar] [CrossRef]
- Leysen, L.; Cools, W.; Nijs, J.; Adriaenssens, N.; Pas, R.; van Wilgen, C.P.; Bults, R.; Roose, E.; Lahousse, A.; Beckwée, D. The mediating effect of pain catastrophizing and perceived injustice in the relationship of pain on health-related quality of life in breast cancer survivors. Support. Care Cancer 2021, 29, 5653–5661. [Google Scholar] [CrossRef] [PubMed]
- Carriere, J.S.; Martel, M.O.; Kao, M.C.; Sullivan, M.J.; Darnall, B.D. Pain behavior mediates the relationship between perceived injustice and opioid prescription for chronic pain: A Collaborative Health Outcomes Information Registry study. J. Pain Res. 2017, 10, 557–566. [Google Scholar] [CrossRef] [Green Version]
- Turk, D.C.; Okifuji, A. What factors affect physicians’ decisions to prescribe opioids for chronic noncancer pain patients? Clin. J. Pain 1997, 13, 330–336. [Google Scholar] [CrossRef]
- Paice, J.A. Chronic treatment-related pain in cancer survivors. Pain 2011, 152, S84–S89. [Google Scholar] [CrossRef]
- Derksen, J.W.G.; Beijer, S.; Koopman, M.; Verkooijen, H.M.; van de Poll-Franse, L.V.; May, A.M. Monitoring potentially modifiable lifestyle factors in cancer survivors: A narrative review on currently available methodologies and innovations for large-scale surveillance. Eur. J. Cancer 2018, 103, 327–340. [Google Scholar] [CrossRef]
- Gopalakrishna, A.; Longo, T.A.; Fantony, J.J.; Van Noord, M.; Inman, B.A. Lifestyle factors and health-related quality of life in bladder cancer survivors: A systematic review. J Cancer Surviv. 2016, 10, 874–882. [Google Scholar] [CrossRef] [Green Version]
- Fink, G. Stress: Concepts, Cognition, Emotion, and Behavior; Academic Press Elsevier: Cambridge, MA, USA, 2007. [Google Scholar]
- Tsigos, C.; Kyrou, I.; Kassi, E.; Chrousos, G.P. Stress: Endocrine Physiology and Pathophysiology. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com: South Dartmouth, MA, USA, 2000. [Google Scholar]
- National Research Council Committee on, R. and A. Alleviation of Distress in Laboratory, The National Academies Collection: Reports funded by National Institutes of Health. In Recognition and Alleviation of Distress in Laboratory Animals; National Academies Press: Washington, DC, USA, 2008. [Google Scholar]
- Abbey, G.; Thompson, S.B.N.; Hickish, T.; Heathcote, D. A meta-analysis of prevalence rates and moderating factors for cancer-related post-traumatic stress disorder. Psychooncology 2015, 24, 371–381. [Google Scholar] [CrossRef]
- Syrowatka, A.; Motulsky, A.; Kurteva, S.; Hanley, J.A.; Dixon, W.G.; Meguerditchian, A.N.; Tamblyn, R. Predictors of distress in female breast cancer survivors: A systematic review. Breast Cancer Res. Treat 2017, 165, 229–245. [Google Scholar] [CrossRef]
- Riba, M.B.; Donovan, K.A.; Andersen, B.; Braun, I.; Breitbart, W.S.; Brewer, B.W.; Buchmann, L.O.; Clark, M.M.; Collins, M.; Corbett, C.; et al. NCCN Clinical Practice Guidelines in Oncology: Distress Management, v3.2019. Natl. Compr. Cancer Network. 2019, 17, 1229–1249. Available online: https://www.nccn.org/professionals/physician_gls/pdf/distress.pdf (accessed on 14 December 2021). [CrossRef] [PubMed]
- Fagundes, C.; LeRoy, A.; Karuga, M. Behavioral Symptoms after Breast Cancer Treatment: A Biobehavioral Approach. J. Pers. Med. 2015, 5, 280–295. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Z.; Wang, Y.X.; Jiang, C.L. Inflammation: The Common Pathway of Stress-Related Diseases. Front. Hum. Neurosci. 2017, 11, 316. [Google Scholar] [CrossRef]
- Reis, J.C.; Antoni, M.H.; Travado, L. Emotional distress, brain functioning, and biobehavioral processes in cancer patients: A neuroimaging review and future directions. CNS Spectr. 2020, 25, 79–100. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Netwerk. Survivorship 2021 (Version 3. 2021). 2021. Available online: https://www.nccn.org/login?ReturnURL=https://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf (accessed on 8 September 2021).
- Thornton, L.M.; Andersen, B.L.; Blakely, W.P. The pain, depression, and fatigue symptom cluster in advanced breast cancer: Covariation with the hypothalamic-pituitary-adrenal axis and the sympathetic nervous system. Health Psychol. 2010, 29, 333–337. [Google Scholar] [CrossRef] [Green Version]
- Addison, S.; Shirima, D.; Aboagye-Mensah, E.B.; Dunovan, S.G.; Pascal, E.Y.; Lustberg, M.B.; Arthur, E.K.; Nolan, T.S. Effects of tandem cognitive behavioral therapy and healthy lifestyle interventions on health-related outcomes in cancer survivors: A systematic review. J. Cancer Surviv. 2021, 1–24. [Google Scholar] [CrossRef]
- Traeger, L.; Penedo, F.J.; Benedict, C.; Dahn, J.R.; Lechner, S.C.; Schneiderman, N.; Antoni, M.H. Identifying how and for whom cognitive-behavioral stress management improves emotional well-being among recent prostate cancer survivors. Psychooncology 2013, 22, 250–259. [Google Scholar] [CrossRef]
- Tang, M.; Liu, X.; Wu, Q.; Shi, Y. The Effects of Cognitive-Behavioral Stress Management for Breast Cancer Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Cancer Nurs. 2020, 43, 222–237. [Google Scholar] [CrossRef]
- Danhauer, S.C.; Addington, E.L.; Cohen, L.; Sohl, S.J.; Van Puymbroeck, M.; Albinati, N.K.; Culos-Reed, S.N. Yoga for symptom management in oncology: A review of the evidence base and future directions for research. Cancer 2019, 125, 1979–1989. [Google Scholar] [CrossRef]
- Matchim, Y.; Armer, J.M.; Stewart, B.R. Mindfulness-based stress reduction among breast cancer survivors: A literature review and discussion. Oncol. Nurs. Forum 2011, 38, E61–E71. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.C.; Yeh, T.L.; Chang, Y.M.; Hu, W.Y. Short-term Effects of Randomized Mindfulness-Based Intervention in Female Breast Cancer Survivors: A Systematic Review and Meta-analysis. Cancer. Nurs. 2021, 44, E703–E714. [Google Scholar] [CrossRef]
- Roth, T. Insomnia: Definition, prevalence, etiology, and consequences. J. Clin. Sleep Med. 2007, 3, S7–S10. [Google Scholar] [CrossRef] [Green Version]
- Savard, J.; Ivers, H.; Villa, J.; Caplette-Gingras, A.; Morin, C.M. Natural course of insomnia comorbid with cancer: An 18-month longitudinal study. J. Clin. Oncol. 2011, 29, 3580–3586. [Google Scholar] [CrossRef]
- Johnson, J.A.; Rash, J.A.; Campbell, T.S.; Savard, J.; Gehrman, P.R.; Perlis, M.; Carlson, L.E.; Garland, S.N. A systematic review and meta-analysis of randomized controlled trials of cognitive behavior therapy for insomnia (CBT-I) in cancer survivors. Sleep Med. Rev. 2016, 27, 20–28. [Google Scholar] [CrossRef]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [Green Version]
- Hall, D.L.; Mishel, M.H.; Germino, B.B. Living with cancer-related uncertainty: Associations with fatigue, insomnia, and affect in younger breast cancer survivors. Support. Care Cancer 2014, 22, 2489–2495. [Google Scholar] [CrossRef]
- Carpenter, J.S.; Elam, J.L.; Ridner, S.H.; Carney, P.H.; Cherry, G.J.; Cucullu, H.L. Sleep, fatigue, and depressive symptoms in breast cancer survivors and matched healthy women experiencing hot flashes. Oncol. Nurs. Forum 2004, 31, 591–5598. [Google Scholar] [CrossRef] [Green Version]
- Savard, J.; Davidson, J.R.; Ivers, H.; Quesnel, C.; Rioux, D.; Dupere, V.; Lasnier, M.; Simard, S.; Morin, C.M. The association between nocturnal hot flashes and sleep in breast cancer survivors. J. Pain Symptom Manag. 2004, 27, 513–522. [Google Scholar] [CrossRef]
- Gupta, P.; Sturdee, D.W.; Palin, S.L.; Majumder, K.; Fear, R.; Marshall, T.; Paterson, I. Menopausal symptoms in women treated for breast cancer: The prevalence and severity of symptoms and their perceived effects on quality of life. Climacteric 2006, 9, 49–58. [Google Scholar] [CrossRef]
- Desai, K.; Mao, J.J.; Su, I.; Demichele, A.; Li, Q.; Xie, S.X.; Gehrman, P.R. Prevalence and risk factors for insomnia among breast cancer patients on aromatase inhibitors. Support. Care Cancer 2013, 21, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Leysen, L.; Lahousse, A.; Nijs, J.; Adriaenssens, N.; Mairesse, O.; Ivakhnov, S.; Bilterys, T.; Van Looveren, E.; Pas, R.; Beckwée, D. Prevalence and risk factors of sleep disturbances in breast cancersurvivors: Systematic review and meta-analyses. Support. Care Cancer 2019, 27, 4401–4433. [Google Scholar] [CrossRef]
- Finan, P.H.; Goodin, B.R.; Smith, M.T. The association of sleep and pain: An update and a path forward. J. Pain 2013, 14, 1539–1552. [Google Scholar] [CrossRef] [Green Version]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Perlis, M.L.; Jungquist, C.; Smith, M.T.; Posner, D. Cognitive Behavioral Treatment of Insomnia: A Session-by-Session Guide; Springer Science and Business Media: New York, NY, USA, 2008. [Google Scholar]
- Ma, Y.; Hall, D.L.; Ngo, L.H.; Liu, Q.; Bain, P.A.; Yeh, G.Y. Efficacy of cognitive behavioral therapy for insomnia in breast cancer: A meta-analysis. Sleep Med. Rev. 2021, 55, 101376. [Google Scholar] [CrossRef]
- Zhou, E.S.; Partridge, A.H.; Syrjala, K.L.; Michaud, A.L.; Recklitis, C.J. Evaluation and treatment of insomnia in adult cancer survivorship programs. J. Cancer Surviv. 2017, 11, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Mindell, J.A.; Bartle, A.; Wahab, N.A.; Ahn, Y.; Ramamurthy, M.B.; Huong, H.T.; Kohyama, J.; Ruangdaraganon, N.; Sekartini, R.; Teng, A.; et al. Sleep education in medical school curriculum: A glimpse across countries. Sleep Med. 2011, 12, 928–931. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.; Grandner, M.; Nowakowski, S.; Nesom, G.; Corbitt, C.; Perlis, M.L. Where are the Behavioral Sleep Medicine Providers and Where are They Needed? A Geographic Assessment. Behav. Sleep Med. 2016, 14, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Stinson, K.; Tang, N.K.; Harvey, A.G. Barriers to treatment seeking in primary insomnia in the United Kingdom: A cross-sectional perspective. Sleep 2006, 29, 1643–1646. [Google Scholar] [CrossRef]
- Matthews, E.E.; Arnedt, J.T.; McCarthy, M.S.; Cuddihy, L.J.; Aloia, M.S. Adherence to cognitive behavioral therapy for insomnia: A systematic review. Sleep Med. Rev. 2013, 17, 453–464. [Google Scholar] [CrossRef] [Green Version]
- American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2019–2021; American Cancer Society: Atlanta, GA, USA, 2019; Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-treatment-and-survivorship-facts-and-figures/cancer-treatment-and-survivorship-facts-and-figures-2019-2021.pdf (accessed on 20 September 2021).
- Zhang, F.F.; Liu, S.; John, E.M.; Must, A.; Demark-Wahnefried, W. Diet quality of cancer survivors and noncancer individuals: Results from a national survey. Cancer 2015, 121, 4212–4221. [Google Scholar] [CrossRef]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies. Nutr. Rev. 2016, 74, 737–748. [Google Scholar] [CrossRef] [Green Version]
- Jochems, S.H.J.; Van Osch, F.H.M.; Bryan, R.T.; Wesselius, A.; van Schooten, F.J.; Cheng, K.K.; Zeegers, M.P. Impact of dietary patterns and the main food groups on mortality and recurrence in cancer survivors: A systematic review of current epidemiological literature. BMJ Open 2018, 8, e014530. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, S.T.; Elma, Ö.; Deliens, T.; Coppieters, I.; Clarys, P.; Nijs, J.; Malfliet, A. Nutrition/Dietary Supplements and Chronic Pain in Patients with Cancer and Survivors of Cancer: A Systematic Review and Research Agenda. Pain Physician 2021, 24, 335–344. [Google Scholar] [PubMed]
- Kim, T.H.; Kang, J.W.; Lee, T.H. Therapeutic options for aromatase inhibitor-associated arthralgia in breast cancer survivors: A systematic review of systematic reviews, evidence mapping, and network meta-analysis. Maturitas 2018, 118, 29–37. [Google Scholar] [CrossRef]
- Mohammadi, S.; Sulaiman, S.; Koon, P.B.; Amani, R.; Hosseini, S.M. Association of nutritional status with quality of life in breast cancer survivors. Asian Pac. J. Cancer Prev. 2013, 14, 7749–7755. [Google Scholar] [CrossRef] [Green Version]
- Fu, M.R.; Axelrod, D.; Guth, A.; McTernan, M.L.; Qiu, J.M.; Zhou, Z.; Ko, E.; Magny-Normilus, C.; Scagliola, J.; Wang, Y. The Effects of Obesity on Lymphatic Pain and Swelling in Breast Cancer Patients. Biomedicines 2021, 9, 818. [Google Scholar] [CrossRef]
- Blazek, K.; Favre, J.; Asay, J.; Erhart-Hledik, J.; Andriacchi, T. Age and obesity alter the relationship between femoral articular cartilage thickness and ambulatory loads in individuals without osteoarthritis. J. Orthop. Res. 2014, 32, 394–402. [Google Scholar] [CrossRef]
- Rogers, A.H.; Kauffman, B.Y.; Garey, L.; Asmundson, G.J.; Zvolensky, M.J. Pain-Related Anxiety among Adults with Obesity and Chronic Pain: Relations with Pain, Opioid Misuse, and Mental Health. Behav. Med. 2020, 1–9. [Google Scholar] [CrossRef]
- Singh, D.; Park, W.; Hwang, D.; Levy, M.S. Severe obesity effect on low back biomechanical stress of manual load lifting. Work 2015, 51, 337–348. [Google Scholar] [CrossRef]
- Fabris de Souza, S.A.; Faintuch, J.; Valezi, A.C.; Sant’Anna, A.F.; Gama-Rodrigues, J.J.; de Batista Fonseca, I.C.; de Melo, R.D. Postural changes in morbidly obese patients. Obes. Surg. 2005, 15, 1013–1016. [Google Scholar] [CrossRef]
- Timmins, H.C.; Mizrahi, D.; Li, T.; Kiernan, M.C.; Goldstein, D.; Park, S.B. Metabolic and lifestyle risk factors for chemotherapy-induced peripheral neuropathy in taxane and platinum-treated patients: A systematic review. J. Cancer Surviv. 2021, 1–15. [Google Scholar] [CrossRef]
- Parekh, N.; Chandran, U.; Bandera, E.V. Obesity in cancer survival. Annu. Rev. Nutr. 2012, 32, 311–342. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Bracken-Clarke, D.; Kapoor, D.; Baird, A.M.; Buchanan, P.J.; Gately, K.; Cuffe, S.; Finn, S.P. Vaping and lung cancer—A review of current data and recommendations. Lung Cancer 2021, 153, 11–20. [Google Scholar] [CrossRef]
- Strick, K. E-cigarettes: Time to realign our approach? Lancet 2019, 394, 1297. [Google Scholar]
- Lucchiari, C.; Masiero, M.; Botturi, A.; Pravettoni, G. Helping patients to reduce tobacco consumption in oncology: A narrative review. Springerplus 2016, 5, 1136. [Google Scholar] [CrossRef] [Green Version]
- De Moor, J.S.; Elder, K.; Emmons, K.M. Smoking prevention and cessation interventions for cancer survivors. Semin. Oncol. Nurs. 2008, 24, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Santa Mina, D.; Brahmbhatt, P.; Lopez, C.; Baima, J.; Gillis, C.; Trachtenberg, L.; Silver, J.K. The Case for Prehabilitation Prior to Breast Cancer Treatment. PM&R 2017, 9, S305–S316. [Google Scholar]
- Sørensen, L.T.; Hørby, J.; Friis, E.; Pilsgaard, B.; Jørgensen, T. Smoking as a risk factor for wound healing and infection in breast cancer surgery. Eur. J. Surg. Oncol. 2002, 28, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Cancer Trends Progress Report National Cancer Institute. Available online: https://www.progressreport.cancer.gov/after/smoking (accessed on 20 September 2021).
- Aigner, C.J.; Cinciripini, P.M.; Anderson, K.O.; Baum, G.P.; Gritz, E.R.; Lam, C.Y. The Association of Pain With Smoking and Quit Attempts in an Electronic Diary Study of Cancer Patients Trying to Quit. Nicotine Tob. Res. 2016, 18, 1449–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ditre, J.W.; Heckman, B.W.; Zale, E.L.; Kosiba, J.D. Acute analgesic effects of nicotine and tobacco in humans: A meta-analysis. Pain 2016, 157, 1373–1381. [Google Scholar] [CrossRef]
- Davidson, S.M.; Boldt, R.G.; Louie, A.V. How can we better help cancer patients quit smoking? The London Regional Cancer Program experience with smoking cessation. Curr. Oncol. 2018, 25, 226–230. [Google Scholar] [CrossRef] [Green Version]
- Richter, K.P.; Ellerbeck, E.F. It’s time to change the default for tobacco treatment. Addiction 2015, 110, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Willett, W.C.; Rimm, E.B.; Stampfer, M.J.; Giovannucci, E.L. Light to moderate intake of alcohol, drinking patterns, and risk of cancer: Results from two prospective US cohort studies. BMJ 2015, 351, h4238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Light alcohol drinking and cancer: A meta-analysis. Ann. Oncol. 2013, 24, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Myung, S.K. Erroneous conclusions about the association between light alcohol drinking and the risk of cancer: Comments on Bagnardi et al.’s meta-analysis. Ann. Oncol. 2016, 27, 2138. [Google Scholar] [CrossRef]
- Xia, E.Q.; Deng, G.F.; Guo, Y.J.; Li, H.B. Biological activities of polyphenols from grapes. Int. J. Mol. Sci. 2010, 11, 622–646. [Google Scholar] [CrossRef]
- Ali, A.M.; Schmidt, M.K.; Bolla, M.K.; Wang, Q.; Gago-Dominguez, M.; Castelao, J.E.; Carracedo, A.; Garzón, V.M.; Bojesen, S.E.; Nordestgaard, B.G.; et al. Alcohol consumption and survival after a breast cancer diagnosis: A literature-based meta-analysis and collaborative analysis of data for 29,239 cases. Cancer Epidemiol. Biomark. Prev. 2014, 23, 934–945. [Google Scholar] [CrossRef] [Green Version]
- Watts, E.L.; Appleby, P.N.; Perez-Cornago, A.; Bueno-de-Mesquita, H.B.; Chan, J.M.; Chen, C.; Cohn, B.A.; Cook, M.B.; Flicker, L.; Freedman, N.D.; et al. Low Free Testosterone and Prostate Cancer Risk: A Collaborative Analysis of 20 Prospective Studies. Eur. Urol. 2018, 74, 585–594. [Google Scholar] [CrossRef] [Green Version]
- Sanford, N.N.; Sher, D.J.; Xu, X.; Ahn, C.; D’Amico, A.V.; Aizer, A.A.; Mahal, B.A. Alcohol use among patients with cancer and survivors in the United States 2000–2017. J. Natl. Compr. Cancer Netw. 2020, 18, 69–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashibe, M.; Brennan, P.; Chuang, S.C.; Boccia, S.; Castellsague, X.; Chen, C.; Curado, M.P.; Dal Maso, L.; Daudt, A.W.; Fabianova, E.; et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: Pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol. Biomark. Prev. 2009, 18, 541–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, T.; Oram, C.; Correll, C.U.; Tsermentseli, S.; Stubbs, B. Analgesic effects of alcohol: A systematic review and meta-analysis of controlled experimental studies in healthy participants. J. Pain 2017, 18, 499–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zale, E.L.; Maisto, S.A.; Ditre, J.W. Interrelations between pain and alcohol: An integrative review. Clin. Psychol. Rev. 2015, 37, 57–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boissoneault, J.; Lewis, B.; Nixon, S.J. Characterizing chronic pain and alcohol use trajectory among treatment-seeking alcoholics. Alcohol 2019, 75, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Maleki, N.; Oscar-Berman, M. Chronic Pain in Relation to Depressive Disorders and Alcohol Abuse. Brain Sci. 2020, 10, 826. [Google Scholar] [CrossRef]
- Nieto, S.J.; Green, R.; Grodin, E.N.; Cahill, C.M.; Ray, L.A. Pain catastrophizing predicts alcohol craving in heavy drinkers independent of pain intensity. Drug Alcohol Depend. 2021, 218, 108368. [Google Scholar] [CrossRef]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 243–274. [Google Scholar] [CrossRef] [Green Version]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical Activity and Mortality in Cancer Survivors: A Systematic Review and Meta-Analysis. JNCI Cancer Spectr. 2020, 4, pkz080. [Google Scholar] [CrossRef]
- Turner, R.R.; Steed, L.; Quirk, H.; Greasley, R.U.; Saxton, J.M.; Taylor, S.J.; Rosario, D.J.; Thaha, M.A.; Bourke, L. Interventions for promoting habitual exercise in people living with and beyond cancer. Cochrane Database Syst. Rev. 2018, 9. [Google Scholar] [CrossRef]
- Garcia, D.O.; Thomson, C.A. Physical activity and cancer survivorship. Nutr. Clin. Pract. 2014, 29, 768–779. [Google Scholar] [CrossRef]
- Wolin, K.Y.; Schwartz, A.L.; Matthews, C.E.; Courneya, K.S.; Schmitz, K.H. Implementing the exercise guidelines for cancer survivors. J. Support. Oncol. 2012, 10, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. J. Clin. Oncol. 2016, 34, 611–635. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Zheng, J.; Zhang, L. The effect of exercise on aromatase inhibitor-induced musculoskeletal symptoms in breast cancer survivors: A systematic review and meta-analysis. Support. Care Cancer 2020, 28, 1587–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boing, L.; Vieira, M.C.S.; Moratelli, J.; Bergmann, A.; Guimarães, A.C.A. Effects of exercise on physical outcomes of breast cancer survivors receiving hormone therapy—A systematic review and meta-analysis. Maturitas 2020, 141, 71–81. [Google Scholar] [CrossRef]
- Ballard-Barbash, R.; Friedenreich, C.M.; Courneya, K.S.; Siddiqi, S.M.; McTiernan, A.; Alfano, C.M. Physical activity, biomarkers, and disease outcomes in cancer survivors: A systematic review. J. Natl. Cancer Inst. 2012, 104, 815–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasenoehrl, T.; Palma, S.; Ramazanova, D.; Kölbl, H.; Dorner, T.E.; Keilani, M.; Crevenna, R. Resistance exercise and breast cancer-related lymphedema-a systematic review update and meta-analysis. Support Care Cancer 2020, 28, 3593–3603. [Google Scholar] [CrossRef] [PubMed]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 1, Cd011279. [Google Scholar] [PubMed] [Green Version]
- Lavín-Pérez, A.M.; Collado-Mateo, D.; Mayo, X.; Liguori, G.; Humphreys, L.; Copeland, R.J.; Jiménez, A. Effects of high-intensity training on the quality of life of cancer patients and survivors: A systematic review with meta-analysis. Sci. Rep. 2021, 11, 15089. [Google Scholar] [CrossRef]
- Ijsbrandy, C.; Ottevanger, P.B.; Gerritsen, W.R.; van Harten, W.H.; Hermens, R. Determinants of adherence to physical cancer rehabilitation guidelines among cancer patients and cancer centers: A cross-sectional observational study. J. Cancer Surviv. 2021, 15, 163–177. [Google Scholar] [CrossRef]
- Kampshoff, C.S.; Jansen, F.; van Mechelen, W.; May, A.M.; Brug, J.; Chinapaw, M.J.; Buffart, L.M. Determinants of exercise adherence and maintenance among cancer survivors: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 80. [Google Scholar] [CrossRef] [Green Version]
- Ormel, H.L.; van der Schoot, G.G.F.; Sluiter, W.J.; Jalving, M.; Gietema, J.A.; Walenkamp, A.M.E. Predictors of adherence to exercise interventions during and after cancer treatment: A systematic review. Psychooncology 2018, 27, 713–724. [Google Scholar] [CrossRef]
- Spencer, J.C.; Wheeler, S.B. A systematic review of Motivational Interviewing interventions in cancer patients and survivors. Patient Educ. Couns. 2016, 99, 1099–1105. [Google Scholar] [CrossRef]
- Veenhof, C.; Köke, A.J.; Dekker, J.; Oostendorp, R.A.; Bijlsma, J.W.; van Tulder, M.W.; van den Ende, C.H. Effectiveness of behavioral graded activity in patients with osteoarthritis of the hip and/or knee: A randomized clinical trial. Arthritis Rheum. 2006, 55, 925–934. [Google Scholar] [CrossRef]
- Cillessen, L.; Johannsen, M.; Speckens, A.E.M.; Zachariae, R. Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and survivors: A systematic review and meta-analysis of randomized controlled trials. Psychooncology 2019, 28, 2257–2269. [Google Scholar] [CrossRef] [Green Version]
- Duan, L.; Xu, Y.; Li, M. Effects of Mind-Body Exercise in Cancer Survivors: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2020, 2020, 7607161. [Google Scholar] [CrossRef]
- Mendoza, M.E.; Capafons, A.; Gralow, J.R.; Syrjala, K.L.; Suárez-Rodríguez, J.M.; Fann, J.R.; Jensen, M.P. Randomized controlled trial of the Valencia model of waking hypnosis plus CBT for pain, fatigue, and sleep management in patients with cancer and cancer survivors. Psychooncology 2017, 26, 1832–1838. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute Levels of Evidence and Grades of RecommendationWorking Party Joanna Briggs Institute Levels of Evidence and Grades of Recommendation. 2014. Available online: https://jbi.global/sites/default/files/2019-05/JBI-Levels-of-evidence_2014_0.pdf (accessed on 22 November 2021).
- Hernandez Silva, E.; Lawler, S.; Langbecker, D. The effectiveness of mHealth for self-management in improving pain, psychological distress, fatigue, and sleep in cancer survivors: A systematic review. J. Cancer Surviv. 2019, 13, 97–107. [Google Scholar] [CrossRef]
- Mullan, F. Seasons of survival: Reflections of a physician with cancer. N. Engl. J. Med. 1985, 313, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Paxton, R.J.; Jones, L.A.; Chang, S.; Hernandez, M.; Hajek, R.A.; Flatt, S.W.; Natarajan, L.; Pierce, J.P. Was race a factor in the outcomes of the Women’s Health Eating and Living Study? Cancer 2011, 117, 3805–3813. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, C.M.; Courneya, K.S.; Stein, K. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Bower, P.; Gilbody, S. Stepped care in psychological therapies: Access, effectiveness and efficiency. Narrative literature review. Br. J. Psychiatry 2005, 186, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Zhou, E.S.; Michaud, A.L.; Recklitis, C.J. Developing efficient and effective behavioral treatment for insomnia in cancer survivors: Results of a stepped care trial. Cancer 2020, 126, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Lynch, F.A.; Katona, L.; Jefford, M.; Smith, A.B.; Shaw, J.; Dhillon, H.M.; Ellen, S.; Phipps-Nelson, J.; Lai-Kwon, J.; Milne, D.; et al. Feasibility and Acceptability of Fear-Less: A Stepped-Care Program to Manage Fear of Cancer Recurrence in People with Metastatic Melanoma. J. Clin. Med. 2020, 9, 2969. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.L.; Fisher, A.; Smith, L.; Heinrich, M.; Potts, H.W.W. Digital health behaviour change interventions targeting physical activity and diet in cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2017, 11, 704–719. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Williams, J.H.; Hogan, P.F.; Bruinooge, S.S.; Rodriguez, G.I.; Kosty, M.P.; Bajorin, D.F.; Hanley, A.; Muchow, A.; McMillan, N.; et al. Projected supply of and demand for oncologists and radiation oncologists through 2025: An aging, better-insured population will result in shortage. J. Oncol. Pract. 2014, 10, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Wijma, A.J.; Leysen, L.; Pas, R.; Willaert, W.; Hoelen, W.; Ickmans, K.; Wilgen, C.P.V. Explaining pain following cancer: A practical guide for clinicians. Braz. J. Phys. Ther. 2019, 23, 367–377. [Google Scholar] [CrossRef]
- Lexmond, W.; Jäger, K. Psychomteric Properties of the Dutch Version of the Revised Neurophysiology of Pain Questionnaire; Vrije Universiteit Brussel: Brussels, Belgium, 2019; p. 36. [Google Scholar]
- Bennett, M.I.; Bagnall, A.M.; Closs, S.J. How effective are patient-based educational interventions in the management of cancer pain? Systematic review and meta-analysis. Pain 2009, 143, 192–199. [Google Scholar] [CrossRef]
- Nijs, J.; Roose, E.; Lahousse, A.; Mostaqim, K.; Reynebeau, I.; De Couck, M.; Beckwee, D.; Huysmans, E.; Bults, R.; van Wilgen, P.; et al. Pain and Opioid Use in Cancer Survivors: A Practical Guide to Account for Perceived Injustice. Pain Physician 2021, 24, 309–317. [Google Scholar]
- Levit, L.A.; Balogh, E.; Nass, S.J.; Ganz, P. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Bluethmann, S.M.; Mariotto, A.B.; Rowland, J.H. Anticipating the “Silver Tsunami”: Prevalence Trajectories and Comorbidity Burden among Older Cancer Survivors in the United States. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1029–1036. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lahousse, A.; Roose, E.; Leysen, L.; Yilmaz, S.T.; Mostaqim, K.; Reis, F.; Rheel, E.; Beckwée, D.; Nijs, J. Lifestyle and Pain following Cancer: State-of-the-Art and Future Directions. J. Clin. Med. 2022, 11, 195. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010195
Lahousse A, Roose E, Leysen L, Yilmaz ST, Mostaqim K, Reis F, Rheel E, Beckwée D, Nijs J. Lifestyle and Pain following Cancer: State-of-the-Art and Future Directions. Journal of Clinical Medicine. 2022; 11(1):195. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010195
Chicago/Turabian StyleLahousse, Astrid, Eva Roose, Laurence Leysen, Sevilay Tümkaya Yilmaz, Kenza Mostaqim, Felipe Reis, Emma Rheel, David Beckwée, and Jo Nijs. 2022. "Lifestyle and Pain following Cancer: State-of-the-Art and Future Directions" Journal of Clinical Medicine 11, no. 1: 195. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010195