
The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery


Abstract
:1. Introduction
2. Materials and Methods
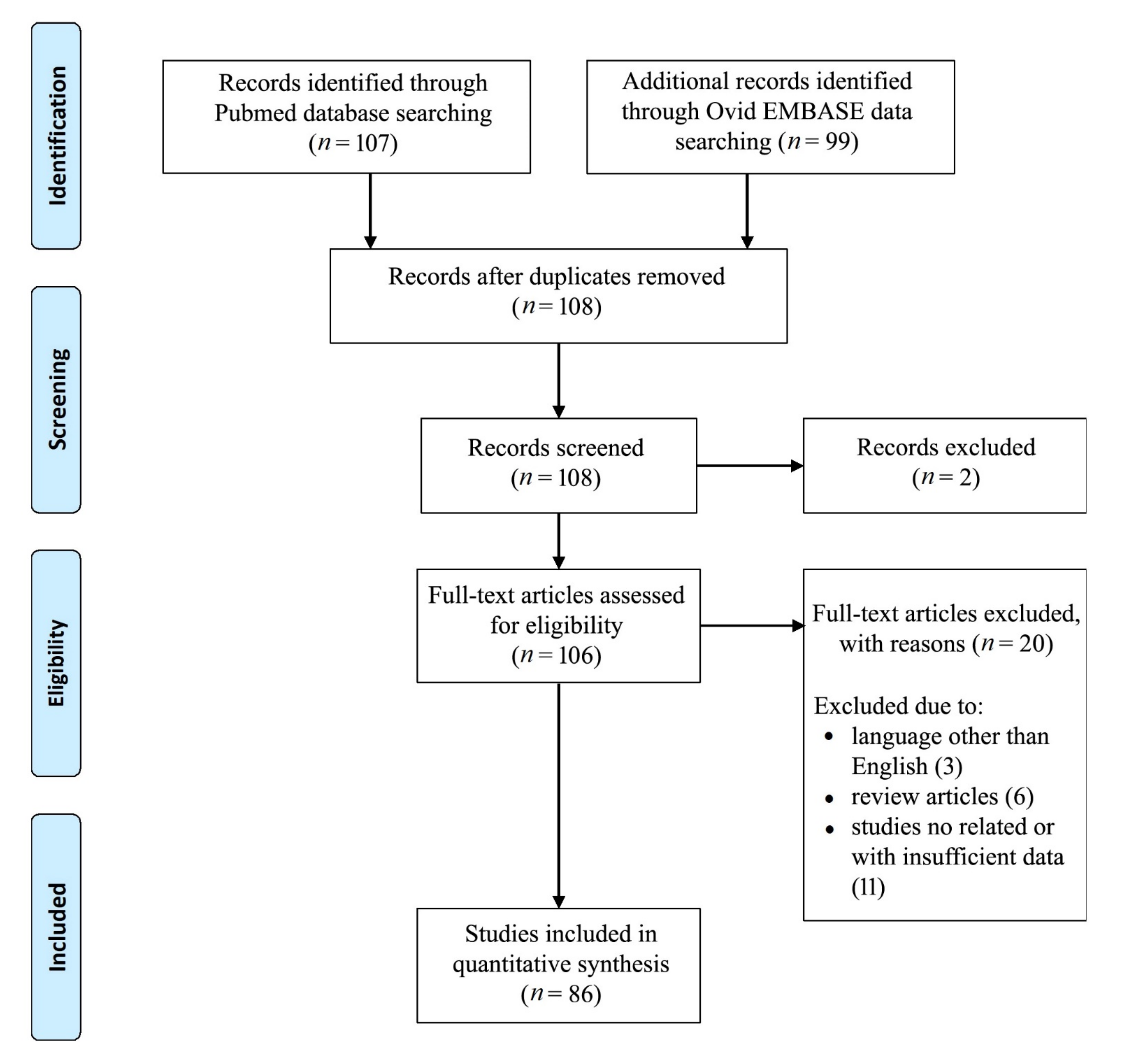
2.1. Literature Search
2.2. Data Collection
2.3. Outcomes
3. Results
3.1. Demographic and Number of Neurosurgical Procedures Performed Using Exoscope
3.2. Evaluation of Exoscopic Surgical Procedures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kriss, T.C.; Kriss, V.M. History of the operating microscope: From magnifying glass to microneurosurgery. Neurosurgery 1998, 42, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Langer, D.J.; White, T.G.; Schulder, M.; Boockvar, J.A.; Labib, M.; Lawton, M.T. Advances in intraoperative optics: A brief review of current exoscope platforms. Oper. Neurosurg. 2020, 19, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Fuse, Y.; Watanabe, T.; Shintai, K.; Kishida, Y.; Nagatani, T.; Seki, Y. Non-brain-exposure exoscopic and endoscopic volume reduction surgery for benign meningioma en plaque in an elderly patient: A case report. NMC Case Rep. J. 2020, 7, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Angileri, F.F.; Esposito, F.; Scibilia, A.; Priola, S.M.; Raffa, G.; German, A. Exoscope-guided (VITOM 3D) single-stage removal of supratentorial cavernous angioma and hemangioblastoma: 3-dimensional operative video. Oper. Neurosurg. 2019, 17, E164–E165. [Google Scholar] [CrossRef]
- Siller, S.; Zoellner, C.; Fuetsch, M.; Trabold, R.; Tonn, J.C.; Zausinger, S. A high-definition 3D exoscope as an alternative to the operating microscope in spinal microsurgery. J. Neurosurg. Spine 2020, 33, 705–714. [Google Scholar] [CrossRef]
- De Divitiis, O.; D’avella, E.; Denaro, L.; Somma, T.; Sacco, M.; D’avella, D. Vitom 3D: Preliminary experience with intradural extramedullary spinal tumors. J. Neurosurg. Sci. 2019, 2, 1–4. [Google Scholar] [CrossRef]
- Muhammad, S.; Lehecka, M.; Niemelä, M. Preliminary experience with a digital robotic exoscope in cranial and spinal surgery: A review of the Synaptive Modus V system. Acta Neurochir. 2019, 161, 2175–2180. [Google Scholar] [CrossRef] [Green Version]
- Sindelar, B.D.; Patel, V.; Chowdhry, S.; Bailes, J.E. A case report in hemorrhagic stroke: A complex disease process and requirement for a multimodal treatment approach. Cureus 2018, 10, e2976. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, F.I.; Mericli, A.F.; DeFazio, M.V.; Chang, E.I.; Hanasono, M.M.; Pederson, W.C.; Kaufman, M.; Selber, J.C. Application of the ORBEYE three-dimensional exoscope for microsurgical procedures. Microsurgery 2020, 40, 468–472. [Google Scholar] [CrossRef]
- Baron, R.B.; Lakomkin, N.; Schupper, A.J.; Nistal, D.; Nael, K.; Price, G.; Hadjipanayis, C.G. Postoperative outcomes following glioblastoma resection using a robot-assisted digital surgical exoscope: A case series. J. Neurooncol. 2020, 148, 519–527. [Google Scholar] [CrossRef]
- Barkun, J.S.; Aronson, J.K.; Feldman, L.S.; Maddern, G.J.; Strasberg, S.M.; Altman, D.G.; Barkun, J.S.; Blazeby, J.M.; Boutron, I.C.; Campbell, W.B.; et al. Evaluation and stages of surgical innovations. Lancet 2009, 374, 1089–1096. [Google Scholar] [CrossRef]
- Raheja, A.; Mishra, S.; Garg, K.; Katiyar, V.; Sharma, R.; Tandon, V.; Goda, R.; Suri, A.; Kale, S.S. Impact of different visualization devices on accuracy, efficiency, and dexterity in neurosurgery: A laboratory investigation. Neurosurg. Focus 2021, 50, E18. [Google Scholar] [CrossRef]
- Sack, J.; Steinberg, J.A.; Rennert, R.C.; Hatefi, D.; Pannell, J.S.; Levy, M.; Khalessi, A.A. Initial experience using a high-definition 3-dimensional exoscope system for microneurosurgery. Oper. Neurosurg. 2018, 14, 395–401. [Google Scholar] [CrossRef]
- Ricciardi, L.; Chaichana, K.L.; Cardia, A.; Stifano, V.; Rossini, Z.; Olivi, A.; Sturiale, C.L. The exoscope in neurosurgery: An innovative “point of view”. A systematic review of the technical, surgical and educational aspects. World Neurosurg. 2019, 124, 136–144. [Google Scholar] [CrossRef]
- Ariffin, M.H.M.; Ibrahim, K.; Baharudin, A.; Tamil, A.M. Early Experience, setup, learning curve, benefits, and complications associated with exoscope and three-dimensional 4K hybrid digital visualizations in minimally invasive spine surgery. Asian Spine J. 2020, 14, 59–65. [Google Scholar] [CrossRef]
- Garneau, J.C.; Laitman, B.M.; Cosetti, M.K.; Hadjipanayis, C.; Wanna, G. The use of the exoscope in lateral skull base surgery: Advantages and limitations. Otol. Neurotol. 2019, 40, 236–240. [Google Scholar] [CrossRef]
- Nishiyama, K. From Exoscope into the next generation. J. Korean Neurosurg. Soc. 2017, 60, 289–293. [Google Scholar] [CrossRef] [Green Version]
- Corsalini, M.; Di Venere, D.; Sportelli, P.; Magazzino, D.; Ripa, C.; Cantatore, F.; Cagnetta, G.; De Rinaldis, C.; Montemurro, N.; De Giacomo, A.; et al. Evaluation of prosthetic quality and masticatory efficiency in patients with total removable prosthesis: Study of 12 cases. Oral Implantol. 2018, 11, 230–240. [Google Scholar]
- Shirzadi, A.; Mukherjee, D.; Drazin, D.G.; Paff, M.; Perri, B.; Mamelak, A.N.; Siddique, K. Use of the video telescope operating monitor (VITOM) as an alternative to the operating microscope in spine surgery. Spine 2012, 37, E1517–E1523. [Google Scholar] [CrossRef]
- Ricciardi, L.; Mattogno, P.P.; Olivi, A.; Sturiale, C.L. Exoscope era: Next technical and educational step in microneurosurgery. World Neurosurg. 2019, 128, 371–373. [Google Scholar] [CrossRef]
- Wali, A.R.; Kang, K.M.; Rennert, R.; Santiago-Dieppa, D.; Khalessi, A.A.; Levy, M. First-in-human clinical experience using high-definition exoscope with intraoperative indocyanine green for clip reconstruction of unruptured large pediatric aneurysm. World Neurosurg. 2021, 151, 52. [Google Scholar] [CrossRef]
- Dawley, T.; Schulder, M. Commentary: First-in-man clinical experience using a high-definition 3-dimensional exoscope system for microneurosurgery. Oper. Neurosurg. 2019, 16, E161–E162. [Google Scholar] [CrossRef]
- Hafez, A.; Elsharkawy, A.; Schwartz, C.; Muhammad, S.; Laakso, A.; Niemelä, M.; Lehecka, M. Comparison of conventional microscopic and exoscopic experimental bypass anastomosis: A technical analysis. World Neurosurg. 2020, 135, e293–e299. [Google Scholar] [CrossRef]
- Perrini, P.; Montemurro, N.; Caniglia, M.; Lazzarotti, G.; Benedetto, N. Wrapping of intracranial aneurysms: Single-center series and systematic review of the literature. Br. J. Neurosurg. 2015, 29, 785–791. [Google Scholar] [CrossRef]
- Yoon, W.S.; Lho, H.W.; Chung, D.S. Evaluation of 3-dimensional exoscopes in brain tumor surgery. J. Korean Neurosurg. Soc. 2021, 64, 289–296. [Google Scholar] [CrossRef]
- Rösler, J.; Georgiev, S.; Roethe, A.L.; Chakkalakal, D.; Acker, G.; Dengler, N.F.; Prinz, V.; Hecht, N.; Faust, K.; Schneider, U.; et al. Clinical implementation of a 3D4K-exoscope (Orbeye) in microneurosurgery. Neurosurg. Rev. 2021, 18, 1–9. [Google Scholar] [CrossRef]
- Muscas, G.; Battista, F.; Boschi, A.; Morone, F.; Della Puppa, A. A Single-center experience with the olympus ORBEYE 4K-3D exoscope for microsurgery of complex cranial cases: Technical nuances and learning curve. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2021, 82, 484–489. [Google Scholar] [CrossRef]
- Hafez, A.; Haeren, R.H.L.; Dillmann, J.; Laakso, A.; Niemelä, M.; Lehecka, M. Comparison of operating microscope and exoscope in a highly challenging experimental setting. World Neurosurg. 2021, 147, e468–e475. [Google Scholar] [CrossRef] [PubMed]
- Teo, T.H.L.; Tan, B.J.; Loo, W.L.; Yeo, A.K.S.; Dinesh, S.K. Utility of a high-definition 3D digital exoscope for spinal surgery during the COVID-19 pandemic. Bone Jt. Open 2020, 1, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Eichberg, D.G.; Di, L.; Shah, A.H.; Luther, E.M.; Jackson, C.; Marenco-Hillembrand, L.; Chaichana, K.L.; Ivan, M.E.; Starke, R.M.; Komotar, R.J. Minimally invasive resection of intracranial lesions using tubular retractors: A large, multi-surgeon, multi-institutional series. J. Neurooncol. 2020, 149, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Gildenberg, P.L.; Labuz, J. Stereotactic craniotomy with the exoscope. Stereotact. Funct. Neurosurg. 1997, 68, 64–71. [Google Scholar] [CrossRef]
- Mamelak, A.N.; Danielpour, M.; Black, K.L.; Hagike, M.; Berci, G. A high-definition exoscope system for neurosurgery and other microsurgical disciplines: Preliminary report. Surg. Innov. 2008, 15, 38–46. [Google Scholar] [CrossRef]
- Mamelak, A.N.; Nobuto, T.; Berci, G. Initial clinical experience with a high-definition exoscope system for microneurosurgery. Neurosurgery 2010, 67, 476–483. [Google Scholar] [CrossRef]
- Di Ieva, A.; Komatsu, M.; Komatsu, F.; Tschabitscher, M. Endoscopic telovelar approach to the fourth ventricle: Anatomic study. Neurosurg. Rev. 2012, 35, 341–348. [Google Scholar] [CrossRef]
- Mamelak, A.N.; Drazin, D.; Shirzadi, A.; Black, K.L.; Berci, G. Infratentorial supracerebellar resection of a pineal tumor using a high definition video exoscope (VITOM®). J. Clin. Neurosci. 2012, 19, 306–309. [Google Scholar] [CrossRef]
- Belloch, J.P.; Rovira, V.; Llácer, J.L.; Riesgo, P.A.; Cremades, A. Fluorescence-guided surgery in high grade gliomas using an exoscope system. Acta Neurochir. 2014, 156, 653–660. [Google Scholar] [CrossRef]
- Birch, K.; Drazin, D.; Black, K.L.; Williams, J.; Berci, G.; Mamelak, A.N. Clinical experience with a high definition exoscope system for surgery of pineal region lesions. J. Clin. Neurosci. 2014, 21, 1245–1249. [Google Scholar] [CrossRef]
- Piquer, J.; Llácer, J.L.; Rovira, V.; Riesgo, P.; Rodriguez, R.; Cremades, A. Fluorescence-guided surgery and biopsy in gliomas with an exoscope system. Biomed Res. Int. 2014, 2014, 207974. [Google Scholar] [CrossRef]
- Ritsma, B.; Kassam, A.; Dowlatshahi, D.; Nguyen, T.; Stotts, G. Minimally Invasive Subcortical Parafascicular Transsulcal Access for Clot Evacuation (Mi SPACE) for Intracerebral Hemorrhage. Case Rep. Neurol. Med. 2014, 2014, 102307. [Google Scholar] [CrossRef]
- Parihar, V.; Yadav, Y.R.; Kher, Y.; Ratre, S.; Sethi, A.; Sharma, D. Learning neuroendoscopy with an exoscope system (video telescopic operating monitor): Early clinical results. Asian J. Neurosurg. 2016, 11, 421–426. [Google Scholar] [CrossRef] [Green Version]
- Scranton, R.A.; Fung, S.H.; Britz, G.W. Transulcal parafascicular minimally invasive approach to deep and subcortical cavernomas: Technical note. J. Neurosurg. 2016, 125, 1360–1366. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.M.; Rasmussen, P.A.; Bain, M.D. Initial single-center technical experience with the brainpath system for acute intracerebral hemorrhage evacuation. Oper. Neurosurg. 2017, 13, 69–76. [Google Scholar] [CrossRef]
- Day, J.D. Transsulcal parafascicular surgery using brain path® for subcortical lesions. Neurosurgery 2017, 64, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Gonen, L.; Chakravarthi, S.S.; Monroy-Sosa, A.; Celix, J.M.; Kojis, N.; Singh, M.; Jennings, J.; Fukui, M.B.; Rovin, R.A.; Kassam, A.B. Initial experience with a robotically operated video optical telescopic-microscope in cranial neurosurgery: Feasibility, safety, and clinical applications. Neurosurg. Focus 2017, 42, E9. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C.; Gallia, G.L.; Chaichana, K.L. Minimally invasive biopsies of deep-seated brain lesions using tubular retractors under exoscopic visualization. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2017, 78, 588–594. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, K.G.; Schöller, K.; Uhl, E. Application of a compact high-definition exoscope for illumination and magnification in high-precision surgical procedures. World Neurosurg. 2017, 97, 652–660. [Google Scholar] [CrossRef]
- Labib, M.A.; Shah, M.; Kassam, A.B.; Young, R.; Zucker, L.; Maioriello, A.; Britz, G.; Agbi, C.; Day, J.D.; Gallia, G.; et al. The safety and feasibility of image-guided brainpath-mediated transsulcul hematoma evacuation: A multicenter study. Neurosurgery 2017, 80, 515–524. [Google Scholar] [CrossRef]
- Moisi, M.D.; Hoang, K.; Tubbs, R.S.; Page, J.; Fisahn, C.; Paulson, D.; Jeyamohan, S.; Delashaw, J.; Hanscom, D.; Oskouian, R.J.; et al. Advancement of surgical visualization methods: Comparison study between traditional microscopic surgery and a novel robotic optoelectronic visualization tool for spinal surgery. World Neurosurg. 2017, 98, 273–277. [Google Scholar] [CrossRef]
- Nagata, Y.; Watanabe, T.; Nagatani, T.; Takeuchi, K.; Chu, J.; Wakabayashi, T. The multiscope technique for microvascular decompression. World Neurosurg. 2017, 103, 310–314. [Google Scholar] [CrossRef]
- Oertel, J.M.; Burkhardt, B.W. Vitom-3D for exoscopic neurosurgery: Initial experience in cranial and spinal procedures. World Neurosurg. 2017, 105, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Rossini, Z.; Cardia, A.; Milani, D.; Lasio, G.B.; Fornari, M.; D’Angelo, V. VITOM 3D: Preliminary experience in cranial surgery. World Neurosurg. 2017, 107, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Weiner, H.L.; Placantonakis, D.G. Resection of a pediatric thalamic juvenile pilocytic astrocytoma with whole brain tractography. Cureus 2017, 9, e1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beez, T.; Munoz-Bendix, C.; Beseoglu, K.; Steiger, H.J.; Ahmadi, S.A. First clinical applications of a high-definition three-dimensional exoscope in pediatric neurosurgery. Cureus 2018, 10, e2108. [Google Scholar] [CrossRef] [Green Version]
- Gassie, K.; Wijesekera, O.; Chaichana, K.L. Minimally invasive tubular retractor-assisted biopsy and resection of subcortical intra-axial gliomas and other neoplasms. J. Neurosurg. Sci. 2018, 62, 682–689. [Google Scholar] [CrossRef]
- Griessenauer, C.; Medin, C.; Goren, O.; Schirmer, C.M. Image-guided, minimally invasive evacuation of intracerebral hematoma: A matched cohort study comparing the endoscopic and tubular exoscopic systems. Cureus 2018, 10, e3569. [Google Scholar] [CrossRef] [Green Version]
- Iyer, R.; Chaichana, K.L. Minimally invasive resection of deep-seated high-grade gliomas using tubular retractors and exoscopic visualization. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2018, 79, 330–336. [Google Scholar] [CrossRef]
- Khalessi, A.A.; Rahme, R.; Rennert, R.C.; Borgas, P.; Steinberg, J.A.; White, T.G.; Santiago-Dieppa, D.R.; Boockvar, J.A.; Hatefi, D.; Pannell, J.S.; et al. First-in-man clinical experience using a high-definition 3-dimensional exoscope system for microneurosurgery. Oper. Neurosurg. 2019, 16, 717–725. [Google Scholar] [CrossRef]
- Klinger, D.R.; Reinard, K.A.; Ajayi, O.O.; Delashaw, J.B., Jr. Microsurgical clipping of an anterior communicating artery aneurysm using a novel robotic visualization tool in lieu of the binocular operating microscope: Operative video. Oper. Neurosurg. 2018, 14, 26–28. [Google Scholar] [CrossRef]
- Mampre, D.; Bechtle, A.; Chaichana, K.L. Minimally invasive resection of intra-axial posterior fossa tumors using tubular retractors. World Neurosurg. 2018, 119, e1016–e1020. [Google Scholar] [CrossRef]
- Takahashi, S.; Toda, M.; Nishimoto, M.; Ishihara, E.; Miwa, T.; Akiyama, T.; Horiguchi, T.; Sasaki, H.; Yoshida, K. Pros and cons of using ORBEYE™ for microneurosurgery. Clin. Neurol. Neurosurg. 2018, 174, 57–62. [Google Scholar] [CrossRef]
- Akbari, S.H.A.; Sylvester, P.T.; Kulwin, C.; Shah, M.V.; Somasundaram, A.; Kamath, A.A.; Beaumont, T.L.; Rich, K.M.; Chicoine, M.R. Initial experience using intraoperative magnetic resonance imaging during a trans-sulcal tubular retractor approach for the resection of deep-seated brain tumors: A case series. Oper. Neurosurg. 2019, 16, 292–301. [Google Scholar] [CrossRef]
- Bakhsheshian, J.; Strickland, B.A.; Jackson, C.; Chaichana, K.L.; Young, R.; Pradilla, G.; Chen, J.W.; Bailes, J.; Zada, G. Multicenter investigation of channel-based subcortical trans-sulcal exoscopic resection of metastatic brain tumors: A retrospective case series. Oper. Neurosurg. 2019, 16, 159–166. [Google Scholar] [CrossRef]
- Herlan, S.; Marquardt, J.S.; Hirt, B.; Tatagiba, M.; Ebner, F.H. 3D exoscope system in neurosurgery-comparison of a standard operating microscope with a new 3d exoscope in the cadaver lab. Oper. Neurosurg. 2019, 17, 518–524. [Google Scholar] [CrossRef]
- Kwan, K.; Schneider, J.R.; Du, V.; Falting, L.; Boockvar, J.A.; Oren, J.; Levine, M.; Langer, D.J. Lessons learned using a high-definition 3-dimensional exoscope for spinal surgery. Oper. Neurosurg. 2019, 16, 619–625. [Google Scholar] [CrossRef]
- Li Ching Ng, A.; Di Ieva, A. How I do it: 3D exoscopic endoscope-assisted microvascular decompression. Acta Neurochir. 2019, 161, 1443–1447. [Google Scholar] [CrossRef]
- Murai, Y.; Sato, S.; Yui, K.; Morimoto, D.; Ozeki, T.; Yamaguchi, M.; Tateyama, K.; Nozaki, T.; Tahara, S.; Yamaguchi, F.; et al. Preliminary clinical microneurosurgical experience with the 4K3-dimensional microvideoscope (ORBEYE) system for microneurological surgery: Observation study. Oper. Neurosurg. 2019, 16, 707–716. [Google Scholar] [CrossRef]
- Nossek, E.; Schneider, J.R.; Kwan, K.; Kulason, K.O.; Du, V.; Chakraborty, S.; Rahme, R.; Faltings, L.; Ellis, J.; Ortiz, R.; et al. Technical aspects and operative nuances using a high-definition 3-dimensional exoscope for cerebral bypass surgery. Oper. Neurosurg. 2019, 17, 157–163. [Google Scholar] [CrossRef]
- Smith, S.; Kozin, E.D.; Kanumuri, V.V.; Barber, S.R.; Backous, D.; Flávio Nogueira, J.; Lee, D.J. Initial experience with 3-dimensional exoscope-assisted transmastoid and lateral skull base surgery. Otolaryngol. Head Neck. Surg. 2019, 160, 364–367. [Google Scholar] [CrossRef]
- Barbagallo, G.M.V.; Certo, F. Three-dimensional, high-definition exoscopic anterior cervical discectomy and fusion: A valid alternative to microscope-assisted surgery. World Neurosurg. 2019, 130, e244–e250. [Google Scholar] [CrossRef]
- Burkhardt, B.W.; Csokonay, A.; Oertel, J.M. 3D-exoscopic visualization using the VITOM-3D in cranial and spinal neurosurgery. What are the limitations? Clin. Neurol. Neurosurg. 2020, 198, 106101. [Google Scholar] [CrossRef]
- Chakravarthi, S.S.; Lyons, L.; Bercu, M.; Singer, J.A. Minimally invasive parafascicular surgical approach for the management of a pediatric third ventricular ependymoma: Case report and review of literature. World Neurosurg. 2020, 141, 311–317. [Google Scholar] [CrossRef]
- Chen, X.; Gao, X.L.; Chai, Y.; Shi, M.M.; Zhang, J.N.; Yue, S.Y. Use of a compact high-definition two-dimensional exoscope in surgical treatment of large vestibular schwannoma. Chin. Med. J. 2020, 133, 1292–1297. [Google Scholar] [CrossRef]
- Crosetti, E.; Arrigoni, G.; Manca, A.; Fantini, M.; Caracciolo, A.; Sardanapoli, F.; Succo, G. VITOM-3D assisted neck dissection via a retroauricular approach (RAND-3D): A preclinical investigation in a cadaver lab. Acta Otorhinolaryngol. Ital. 2020, 40, 343–351. [Google Scholar] [CrossRef]
- D’Ercole, M.; Serchi, E.; Zanello, M.; Tufo, T.; Sturiale, C. Clinical application of a high definition three-dimensional exoscope in anterior lumbar interbody fusion: Technical note. Int. J. Spine Surg. 2020, 14, 1003–1008. [Google Scholar] [CrossRef]
- Doglietto, F.; Belotti, F.; Panciani, P.; Poliani, P.L.; Fontanella, M.M. High-definition 3-dimensional exoscope for 5-ALA glioma surgery: 3-dimensional operative video. Oper. Neurosurg. 2020, 18, E82. [Google Scholar] [CrossRef]
- Garneau, J.C.; Laitman, B.M.; Cosetti, M.K.; Hadjipanayis, C.; Wanna, G.B. Repair of a temporal bone encephalocele with the surgical exoscope. Otol. Neurotol. 2020, 41, 561. [Google Scholar] [CrossRef] [PubMed]
- Khatri, D.; Wagner, K.; Ligas, B.; Higbie, C.; Langer, D. Excision of a retrochiasmatic craniopharyngioma by transcallosal, interforniceal approach with exoscope assistance: 2-dimensional operative video. Oper. Neurosurg. 2020, 19, E411. [Google Scholar] [CrossRef]
- Kleshchova, O.; White, T.G.; Kwan, K.; Chiluwal, A.; Anderson, T.A.; Langer, D.J. Resection of a posterior fossa endodermal cyst with exoscopic assistance: 2-dimensional operative video. Oper. Neurosurg. 2020, 18, E173–E174. [Google Scholar] [CrossRef]
- Ligas, B.; Khatri, D.; Higbie, C.; Wagner, K.; Langer, D. Hemifacial spasm due to bony stenosis of the internal auditory meatus: Look beyond the loop. World Neurosurg. 2020, 137, 179–182. [Google Scholar] [CrossRef]
- Lin, M.; Bakhsheshian, J.; Strickland, B.; Rennert, R.C.; Chu, R.M.; Chaichana, K.L.; Zada, G. Exoscopic resection of atrial intraventricular meningiomas using a navigation-assisted channel-based trans-sulcal approach: Case series and literature review. J. Clin. Neurosci. 2020, 71, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Oren, J.; Kwan, K.; Schneider, J.; Levine, M.; Langer, D. Minimally invasive navigated foraminal discectomy via contralateral approach using a 3-dimensional 4k high-definition exoscope: 2-dimensional operative video. Oper. Neurosurg. 2020, 19, E188. [Google Scholar] [CrossRef] [PubMed]
- Pafitanis, G.; Hadjiandreou, M.; Alamri, A.; Uff, C.; Walsh, D.; Myers, S. The Exoscope versus operating microscope in microvascular surgery: A simulation non-inferiority trial. Arch. Plast. Surg. 2020, 47, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.V.; Ligas, B.; Gandhi, S.; Ellis, J.; Ortiz, R.; Costantino, P.; Qato, K.; Langer, D.J. Internal maxillary to middle cerebral artery bypass using an anterior tibial artery graft, performed using a 3-dimensional exoscope: 2-dimensional operative video. Oper. Neurosurg. 2020, 19, E187. [Google Scholar] [CrossRef]
- Roethe, A.L.; Landgraf, P.; Schröder, T.; Misch, M.; Vajkoczy, P.; Picht, T. Monitor-based exoscopic 3D4k neurosurgical interventions: A two-phase prospective-randomized clinical evaluation of a novel hybrid device. Acta Neurochir. 2020, 162, 2949–2961. [Google Scholar] [CrossRef]
- Rubini, A.; Di Gioia, S.; Marchioni, D. 3D exoscopic surgery of lateral skull base. Eur. Arch. Otorhinolaryngol. 2020, 277, 687–694. [Google Scholar] [CrossRef]
- Silverstein, J.W.; Ellis, J.A.; Langer, D.J. Loss of motor evoked potentials due to carotid artery retraction in an exoscopic clipping of a basilar tip aneurysm. Neurodiagn. J. 2020, 60, 289–299. [Google Scholar] [CrossRef]
- Vetrano, I.G.; Acerbi, F.; Falco, J.; D’Ammando, A.; Devigili, G.; Nazzi, V. High-definition 4K 3D exoscope (ORBEYETM) in peripheral nerve sheath tumor surgery: A preliminary, explorative, pilot study. Oper. Neurosurg. 2020, 19, 480–488. [Google Scholar] [CrossRef]
- Visocchi, M.; Mattogno, P.P.; Ciappetta, P.; Barbagallo, G.; Signorelli, F. Combined transoral exoscope and OArm-assisted approach for craniovertebral junction surgery: Light and shadows in single-center experience with improving technologies. J. Craniovertebr. Junction Spine 2020, 11, 293–299. [Google Scholar]
- Amoo, M.; Henry, J.; Javadpour, M. Beyond magnification and illumination: Preliminary clinical experience with the 4K 3D ORBEYE™ exoscope and a literature review. Acta Neurochir. 2021, 163, 2107–2115. [Google Scholar] [CrossRef]
- Kim, M.; Wainwright, J.; Stein, A.; Hanft, S. Posterior transdural approach for a calcified thoracic intradural disc herniation using a 3-dimensional exoscope: 2-dimensional operative video. Oper. Neurosurg. 2021, 21, E44–E45. [Google Scholar] [CrossRef]
- Marenco-Hillembrand, L.; Suarez-Meade, P.; Chaichana, K.L. Bur hole-based resections of intrinsic brain tumors with exoscopic visualization. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2021, 82, 105–111. [Google Scholar] [CrossRef]
- Muto, J.; Mine, Y.; Nakagawa, Y.; Joko, M.; Kagami, H.; Inaba, M.; Hasegawa, M.; Lee, J.Y.K.; Hirose, Y. Intraoperative real-time near-infrared optical imaging for the identification of metastatic brain tumors via microscope and exoscope. Neurosurg. Focus 2021, 50, E11. [Google Scholar] [CrossRef]
- Rennert, R.C.; Khani, M.; Thomas, K.; Morris, T.W.; Rodriguez, A.; Day, J.D. Transsulcal parafascicular brain path-assisted approach to subcortical lesions: 2-dimensional operative video. Surg. Neurol. Int. 2021, 17, 107. [Google Scholar]
- Rotermund, R.; Regelsberger, J.; Osterhage, K.; Aberle, J.; Flitsch, J. 4K 3-dimensional video microscope system (orbeye) for transsphenoidal pituitary surgery. Acta Neurochir. 2021, 163, 2097–2106. [Google Scholar] [CrossRef]
- Shimizu, T.; Toyota, S.; Nakagawa, K.; Murakami, T.; Mori, K.; Kishima, H.; Taki, T. Retrosigmoid approach in the supine position using ORBEYE: A consecutive series of 14 cases. Neurol. Med. Chir. 2021, 61, 55–61. [Google Scholar] [CrossRef]
- Strickland, B.A.; Brunswick, A.; Zada, G. Exoscopic to endoscopic channel-based trans-sulcal resection of a third ventricular cavernous malformation: Technical case illustration. World Neurosurg. 2021, 148, 66. [Google Scholar] [CrossRef]
- Yaşargil, M.G.; Krayenbühl, H. The use of the binocular microscope in neurosurgery. Bibl. Ophthalmol. 1970, 81, 62–65. [Google Scholar]
- Uluç, K.; Kujoth, G.C.; Başkaya, M.K. Operating microscopes: Past, present, and future. Neurosurg. Focus 2009, 27, E4. [Google Scholar] [CrossRef] [Green Version]
- Perrini, P.; Montemurro, N.; Iannelli, A. The contribution of Carlo Giacomini (1840–1898): The limbus Giacomini and beyond. Neurosurgery 2013, 72, 475–482. [Google Scholar] [CrossRef]
- Hayden, M.G.; Lee, M.; Guzman, R.; Steinberg, G.K. The evolution of cerebral revascularization surgery. Neurosurg. Focus 2009, 26, E17. [Google Scholar] [CrossRef]
- Zebian, B.; Vergani, F.; Lavrador, J.P.; Mukherjee, S.; Kitchen, W.J.; Stagno, V.; Chamilos, C.; Pettorini, B.; Mallucci, C. Recent technological advances in pediatric brain tumor surgery. CNS Oncol. 2017, 6, 71–82. [Google Scholar] [CrossRef]
- Montemurro, N.; Fanelli, G.N.; Scatena, C.; Ortenzi, V.; Pasqualetti, F.; Mazzanti, C.M.; Morganti, R.; Paiar, F.; Naccarato, A.G.; Perrini, P. Surgical outcome and molecular pattern characterization of recurrent glioblastoma multiforme: A single-center retrospective series. Clin. Neurol. Neurosurg. 2021, 207, 106735. [Google Scholar] [CrossRef]
- Rahman, M.; Murad, G.J.; Bova, F.; Friedman, W.A.; Mocco, J. Stereotactic radiosurgery and the linear accelerator: Accelerating electrons in neurosurgery. Neurosurg. Focus 2009, 27, E13. [Google Scholar] [CrossRef]
- Montemurro, N.; Condino, S.; Cattari, N.; D’Amato, R.; Ferrari, V.; Cutolo, F. Augmented reality-assisted craniotomy for parasagittal and convexity en plaque meningiomas and custom-made cranio-plasty: A preliminary laboratory report. Int. J. Environ. Res. Public Health 2021, 18, 9955. [Google Scholar] [CrossRef]
- Shurkhay, V.A.; Goryaynov, S.A.; Aleksandrova, E.V.; Spallone, A.; Potapov, A.A. Navigation systems in neurosurgery. Vopr Neirokhirurgii Im NN Burdenko 2016, 80, 107–114. [Google Scholar] [CrossRef]
- Condino, S.; Montemurro, N.; Cattari, N.; D’Amato, R.; Thomale, U.; Ferrari, V.; Cutolo, F. Evaluation of a wearable AR platform for guiding complex craniotomies in neurosurgery. Ann. Biomed Eng. 2021, 49, 2590–2605. [Google Scholar] [CrossRef]
- Trevisi, G.; Roujeau, T.; Duffau, H. Awake surgery for hemispheric low-grade gliomas: Oncological, functional and methodological differences between pediatric and adult populations. Child’s Nerv. Syst. 2016, 32, 1861–1874. [Google Scholar] [CrossRef]
- Montemurro, N.; Herbet, G.; Duffau, H. Right cortical and axonal structures eliciting ocular deviation during electrical stimulation mapping in awake patients. Brain Topogr. 2016, 29, 561–571. [Google Scholar] [CrossRef]
- Perrini, P.; Gambacciani, C.; Martini, C.; Montemurro, N.; Lepori, P. Anterior cervical corpectomy for cervical spondylotic myelopathy: Reconstruction with expandable cylindrical cage versus iliac crest autograft. A retrospective study. Clin. Neurol. Neurosurg. 2015, 139, 258–263. [Google Scholar] [CrossRef]
- Lavé, A.; Gondar, R.; Demetriades, A.K.; Meling, T.R. Ergonomics and musculoskeletal disorders in neurosurgery: A systematic review. Acta Neurochir. 2020, 162, 2213–2220. [Google Scholar] [CrossRef] [PubMed]
- Canseco, J.A.; Schroeder, G.D.; Patel, P.D.; Grasso, G.; Chang, M.; Kandziora, F.; Vialle, E.N.; Oner, F.C.; Schnake, K.J.; Dvorak, M.F.; et al. Regional and experiential differences in surgeon preference for the treatment of cervical facet injuries: A case study survey with the AO spine cervical classification validation group. Eur. Spine J. 2021, 30, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Mavrovounis, G.; Meling, T.R.; Lafuente, J.; Fountas, K.N.; Demetriades, A.K. Postural ergonomics and work-related musculoskeletal disorders in neurosurgery: Lessons from an international survey. Acta Neurochir. 2021, 163, 1541–1552. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, G.D.; Canseco, J.A.; Patel, P.D.; Divi, S.N.; Karamian, B.A.; Kandziora, F.; Vialle, E.N.; Oner, F.C.; Schnake, K.J.; Dvorak, M.F.; et al. Establishing the injury severity of subaxial cervical spine trauma: Validating the hierarchical nature of the ao spine subaxial cervical spine injury classification system. Spine 2021, 46, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Santoro, G.; Marani, W.; Petrella, G. Posttraumatic synchronous double acute epidural hematomas: Two craniotomies, single skin incision. Surg. Neurol. Int. 2020, 11, 435. [Google Scholar] [CrossRef] [PubMed]
- Ridge, S.E.; Shetty, K.R.; Lee, D.J. Heads-up surgery: Endoscopes and exoscopes for otology and neurotology in the era of the COVID-19 pandemic. Otolaryngol. Clin. N. Am. 2021, 54, 11–23. [Google Scholar] [CrossRef]
- Montemurro, N. Intracranial hemorrhage and COVID-19, but please do not forget “old diseases” and elective surgery. Brain Behav. Immun. 2021, 92, 207–208. [Google Scholar] [CrossRef]
- Gordon, S.A.; Deep, N.L.; Jethanamest, D. Exoscope and personal protective equipment use for otologic surgery in the era of COVID-19. Otolaryngol. Head Neck Surg. 2020, 163, 179–181. [Google Scholar] [CrossRef]
- Haldeman, S.; Nordin, M.; Tavares, P.; Mullerpatan, R.; Kopansky-Giles, D.; Setlhare, V.; Chou, R.; Hurwitz, E.; Treanor, C.; Hartvigsen, J.; et al. Distance management of spinal disorders during the COVID-19 pandemic and beyond: Evidence-based patient and clinician guides from the global spine care initiative. JMIR Public Health Surveill. 2021, 7, e25484. [Google Scholar] [CrossRef]


{kind=link}
| PubMed Search Accessed on 5 July 2021 (108 Articles) | Embase Search Accessed on 5 July 2021 (106 Articles) |
|---|---|
| (exoscope OR exoscopic visualization) AND (neurosurgery OR brain OR spine OR cadaver lab) | (‘exoscope’ OR ‘exoscopic visualization’) AND (‘neurosurgery’ OR ‘brain’ OR ‘spine’ OR ‘cadaver lab’) |
| Authors | Year | Neurosurgical Procedures | Total | Exoscope Manufacturer and/or Model | Visualization Mode Setting | |
|---|---|---|---|---|---|---|
| Tumor (n°) | Vascular and Others Disease (n°) | |||||
| Gildenberg & Labuz [32] | 1997 | glioma (17), metastasis (1) | - | 18 | N/A | - |
| Mamelak et al. [34] | 2010 | glioma (3), HMG (1), meningioma (3), LGG (1), pituitary adenoma (1) | vagus nerve stimulator (1) | 10 | HDXO-SCOPE, Karl Storz | HD 2D |
| Mamelak et al. [36] | 2012 | germinoma (1) | - | 1 | VITOM® | HD 2D |
| Belloch et al. [37] | 2014 | GBM (15), AA (2), metastasis (3), LGG (3) | - | 23 | HDXO-SCOPE, Karl Storz | HD 2D |
| Birch et al. [38] | 2014 | pineocytoma (3), germinoma (1), lipoma (1) | - | 5 | HDXO-SCOPE, Karl Storz | HD 2D |
| Piquer et al. [39] | 2014 | GBM (23), AA (2), metastasis (3), LGG (2) | - | 30 | VITOM® | HD 2D |
| Ritsma et al. [40] | 2014 | - | ICH (1) | 1 | Mi SPACE | HD 2D |
| Parihar et al. [41] | 2016 | meningioma (5), glioma (4), HMG (1), metastasis (1), schwannoma (3), neurocytoma (1), medulloblastoma (1), craniopharyngioma (1) | ICH (3), colloid cyst (1), arachnoid cyst (1), abscess (2), trigeminal neuralgia (1) | 25 | VITOM® | HD 2D |
| Scranton et al. [42] | 2016 | - | cavernoma (2) | 2 | N/A | HD 2D |
| Bauer et al. [43] | 2017 | - | ICH (18) | 18 | BrainPath® | HD 2D |
| Day [44] | 2017 | GBM (15), AA (4), ependymoma (2), neurocytoma (1), LGG (1), metastasis (20) | ICH (6) | 49 | BrainPath® | HD 2D |
| Gonen et al. [45] | 2017 | astrocytoma (56), meningioma (40), metastasis (33), schwannoma (5), epidermoid/dermoid cyst (3), paraganglioma (2), craniopharyngioma (1), pituitary adenoma (1), miscellaneous (8) | aneurysms (7), AVM (5), dAVF (1), ICH (20), trigeminal neuralgia (7), hemifacial spasm (1), arachnoid cysts (2), Chiari I (1), infection (3), colloid cyst (4) | 200 | ROVOT-m | HD 2D |
| Jackson et al. [46] | 2017 | GBM (3), AA (3), metastasis (1), lymphoma (2) | demyelinating disease (2) | 11 | VITOM® | HD 2D |
| Krishnan et al. [47] | 2017 | - | anastomosis (3), AVF (1), ICH (1) | 3 | VITOM® | HD 2D |
| Labib et al. [48] | 2017 | - | ICH (39) | 39 | Mi SPACE | HD 2D |
| Nagata et al. [50] | 2017 | - | hemifacial spasm (2) | 2 | ORBEYE® | HD 2D |
| Oertel & Burkhardt [51] | 2017 | metastasis (3), lymphoma (1) | trigeminal neuralgia (1) | 5 | VITOM® | HD 3D |
| Rossini et al. [52] | 2017 | meningioma (1) | - | 1 | VITOM® | HD 3D |
| Weiner & Placantonakis [53] | 2017 | JPA (1) | - | 1 | VITOM® | HD 3D |
| Beez et al. [54] | 2018 | astrocytoma (2) | myelomeningocele closure (1) | 3 | VITOM® | HD 3D |
| Gassie et al. [55] | 2018 | GBM (24), AA (6), metastasis (14), lymphoma (2) | cavernoma (2), demyelinating disease (2) | 50 | VITOM® | HD 2D |
| Griessenauer et al. [56] | 2018 | - | ICH (5) | 5 | BrainPath® | HD 2D |
| Iyer & Chaichana [57] | 2018 | GBM (11), AA (3) | - | 14 | VITOM® | HD 2D |
| Khalessi et al. [58] | 2018 | meningioma (1), glioma (1) | clipping (4), cavernoma (3), AVM (2), endarterectomy (1), CSDH (1), cyst (1), Chiari I (1) | 17 | ORBEYE® | HD 3D |
| Klinger et al. [59] | 2018 | - | aneurysm (1) | 1 | Modus V™ | HD 3D |
| Mampre et al. [60] | 2018 | metastasis (11), HMG (2) | cavernoma (2) | 15 | VITOM® | HD 2D |
| Sindelar et al. [8] | 2018 | - | ICH (1) | 1 | BrainPath® | HD 2D |
| Takahashi et al. [61] | 2018 | meningioma (5), pituitary adenoma (1), GBM (1), HMG (2), metastasis (1), craniopharyngioma (1) | Moyamoya disease (2), congenital dermal sinus (1) | 14 | ORBEYE® | HD 2D |
| Akbari et al. [62] | 2019 | metastasis (4), GBM (3), LGG (2), AA (1) | - | 10 | VITOM® | HD 2D |
| Angileri et al. [4] | 2019 | - | cavernoma + HMG (1) | 1 | VITOM® | HD 3D |
| Bakhsheshian et al. [63] | 2019 | metastasis (25) | - | 25 | BrainPath® | HD 3D |
| Garneau et al. [16] | 2019 | schwannoma (4) | temporal lobe encephalocele (2) | 6 | Modus V™ | HD 2D |
| Li Ching Ng & Di Ieva [66] | 2019 | - | MVD (1) | 1 | VITOM® | HD 3D |
| Muhammad et al. [7] | 2019 | schwannoma (1), meningioma (3) | - | 4 | Modus V™ | HD 3D |
| Murai et al. [67] | 2019 | meningioma (3), schwannoma (3), pituitary adenoma (1), GBM (1) | clipping (3), bypass (2), carotid endarterectomy (2), ICH (3) | 18 | ORBEYE® | 3D 4K |
| Nossek et al. [68] | 2019 | - | bypass (5) | 5 | ORBEYE® | 3D 4K |
| Smith et al. [69] | 2019 | - | skull base (11) | 11 | ORBEYE® (10), VITOM® (1) | HD 3D |
| Ahmad et al. [9] | 2020 | - | microvascular anastomosis (12) | 12 | ORBEYE® | HD 3D |
| Baron et al. [10] | 2020 | GBM (28) | - | 28 | Modus V™ | HD 3D |
| Burkhardt et al. [71] | 2020 | metastasis (3), LGG (1), AA (1), GBM (2), meningioma (1), subependymoma (1), lymphoma (1) | cavernoma (1), ICH (1), aneurysm (2), CSF leak (1), trigeminal neuralgia (1) | 16 | VITOM® | HD 3D |
| Chakravarthi et al. [72] | 2020 | hypothalamic mass (1) | - | 1 | Kinevo 900 | HD 3D |
| Chen et al. [73] | 2020 | schwannoma (39) | - | 39 | VITOM® | HD 2D |
| Doglietto et al. [76] | 2020 | GBM (1) | - | 1 | ORBEYE® | 3D 4K |
| Eichberg et al. [30] | 2020 | GBM (13), metastasis (19), glioma (8) | cavernoma (7), colloid cyst (4), other (5) | 56 | BrainPath® | HD 2D |
| Fuse et al. [3] | 2020 | meningioma (1) | - | 1 | VITOM® | HD 2D |
| Garneau et al. [77] | 2020 | - | temporal lobe encephalocele (1) | 1 | Modus V™ | HD 3D |
| Khatri et al. [78] | 2020 | craniopharyngioma (1) | - | 1 | N/A | - |
| Kleshchova et al. [79] | 2020 | endodermal cyst (1) | - | 1 | N/A | - |
| Ligas et al. [80] | 2020 | - | hemifacial spasm (1) | 1 | N/A | - |
| Lin et al. [81] | 2020 | meningioma (4) | - | 4 | VITOM® | HD 3D |
| Patel et al. [84] | 2020 | - | bypass (1) | 1 | N/A | - |
| Roethe et al. [85] | 2020 | GBM (9), meningioma (6), LGG (4), metastasis (3), AA (3) | cavernoma (1), trigeminal neuralgia (1), CSF fistula (1) | 28 | Kinevo 900 | 3D 4K |
| Silverstein et al. [87] | 2020 | - | aneurysm (1) | 1 | ORBEYE® | HD 3D |
| Amoo et al. [90] | 2021 | metastasis (5), meningioma (4), GBM (5), schwannoma (1), craniopharyngioma (1) | AVM (1), hemifacial spasm (1) | 18 | ORBEYE® | 3D 4K |
| Marenco-Hillembrand et al. [92] | 2021 | metastasis (8), LGG (4), GBM (3) | - | 15 | N/A | - |
| Muscas et al. [27] | 2021 | meningioma (4), cranial nerve tumors (2), glioma (3), choroid plexus papilloma (1) | aneurysm (1), colloid cyst (1), neurovascular conflict (1), ethmoidal fistula (1) | 14 | ORBEYE® | 3D 4K |
| Muto et al. [93] | 2021 | metastasis (5) | - | 5 | VS3 Iridium | HD 3D |
| Rennert et al. [94] | 2021 | GBM (1) | ICH (1) | 2 | VITOM® | HD 3D |
| Rösler et al. [26] | 2021 | GBM (6), pituitary adenoma (1), meningioma (1), craniopharyngioma (1), LGG (4), lymphoma (1), metastasis (3), HMG (1), hemangioma (1) | ICH (1), epilepsy (6), trigeminal neuralgia (1) | 27 | ORBEYE® | 3D 4K |
| Rotermund et al. [95] | 2021 | pituitary adenoma (239), craniopharyngioma (12), meningioma (7), chordoma (4), metastasis (2) | other (32) | 296 | ORBEYE® | 3D 4K |
| Shimizu et al. [96] | 2021 | meningioma (5), schwannoma (4) | trigeminal neuralgia (2), hemifacial spasm (3) | 14 | ORBEYE® | 3D 4K |
| Strickland et al. [97] | 2021 | - | AVM (1) | 1 | N/A | - |
| Wali et al. [21] | 2021 | - | aneurysm (1) | 1 | ORBEYE® | 3D 4K |
| Yoon et al. [25] | 2021 | metastasis (3), meningioma (3), GBM (4), HMG (1) | - | 11 | VOMS-100 (5), VITOM® (6) | 3D 4K |
| Authors | Year | Neurosurgical Procedures | Total | Exoscope Manufacturer and/or Model | Visualization Mode Setting | |
|---|---|---|---|---|---|---|
| Spine (n°) | Peripheral (n°) | |||||
| Mamelak et al. [34] | 2010 | ACDF (2), epidural abscess (1), lumbar discectomy (3) | - | 6 | HDXO-SCOPE, Karl Storz | HD 2D |
| Shirzadi et al. [19] | 2012 | LPD (11), TLIF (13) | - | 24 | VITOM® | HD 2D |
| Parihar et al. [41] | 2016 | neurofibroma (4), meningioma (1), ACDF (4), corpectomy (2), tuberculosis (1), lumbar discectomy (2) | - | 14 | VITOM® | HD 2D |
| Krishnan et al. [47] | 2017 | LPD (7), cervical foraminotomy (2), ACDF (1) | schwannoma (2), microneurorrhaphy (1) | 13 | VITOM® | HD 2D |
| Oertel & Burkhardt [51] | 2017 | ACDF (2), cervical laminectomies (2), TLIF (2), extradural tumor (1), LPD (1), lumbar discectomy (3) | - | 11 | VITOM® | HD 3D |
| Khalessi et al. [58] | 2018 | ACDF (1), disc herniation (2) | - | 3 | ORBEYE® | HD 3D |
| De Divitiis et al. [6] | 2019 | tumor (5) | - | 5 | VITOM® | HD 3D |
| Kwan et al. [65] | 2019 | ACDF (4), cervical corpectomy (1), cervical laminectomies (3), LPD (2) | - | 10 | ORBEYE® | HD 3D |
| Muhammad et al. [7] | 2019 | CPD (1), ACDF (1), disc herniation (2) | - | 4 | Modus V™ | HD 3D |
| Murai et al. [67] | 2019 | LDP (3) | neurolysis (1) | 4 | ORBEYE® | 3D 4K |
| Ariffin et al. [15] | 2020 | decompression (18), discectomy (17), TLIF (28), OLIF (6) | - | 69 | Kinevo 900 | 3D 4K |
| Barbagallo & Certo [70] | 2020 | ACDF (2) | - | 2 | VITOM® | HD 3D |
| Burkhardt et al. [71] | 2020 | ACDF (4), cervical laminectomies (1), metastasis (1), lumbar decompression (4), TLIF (1), disc herniation (5), dAVF (1), angiolipoma (1) | - | 18 | VITOM® | HD 3D |
| D’Ercole et al. [75] | 2020 | ALIF (9) | - | 9 | VITOM® | HD 3D |
| Oren et al. [82] | 2020 | disc herniation (1) | - | 1 | ORBEYE® | 3D 4K |
| Roethe et al. [85] | 2020 | LPD (1) | - | 1 | Kinevo 900 | 3D 4K |
| Siller et al. [5] | 2020 | LDP (40), ACDF (20) | - | 60 | VITOM® | HD 3D |
| Teo et al. [29] | 2020 | fracture (2), meningioma (1), disc herniation (5) | - | 8 | Modus V™ | HD 3D |
| Vetrano et al. [88] | 2020 | - | schwannoma (2) | 2 | ORBEYE® | 3D 4K |
| Visocchi et al. [89] | 2020 | CVJ pathologies (6) | - | 6 | VITOM® (3), ORBEYE® (3) | 3D 4K |
| Kim et al. [91] | 2021 | disc herniation (1) | - | 1 | N/A | - |
| Rösler et al. [26] | 2021 | ACDF (1), metastasis (1), tumor (1), schwannoma (2), LPD (4) | schwannoma (2), peripheral nerve (1) | 12 | ORBEYE® | 3D 4K |
| Authors | Year | Laboratory Neurosurgical Procedures (n°) | Total | Exoscope Manufacturer and/or Model | Visualization Mode Setting |
|---|---|---|---|---|---|
| Mamelak et al. [33] | 2008 | craniotomy (4) | 4 | HDXO-SCOPE, Karl Storz | HD 2D |
| Di Ieva et al. [35] | 2012 | suboccipital approach (20) | 20 | VITOM® | HD 2D |
| Moisi et al. [49] | 2017 | craniotomy (6) | 6 | Modus V™ | HD 2D |
| Sack et al. [13] | 2018 | craniotomy (5) | 5 | ORBEYE® | HD 3D |
| Herlan et al. [64] | 2019 | pterional approach (6) | 6 | FA Aesculap | HD 3D |
| Crosetti et al. [74] | 2020 | dissection (4) | 4 | VITOM® | HD 3D |
| Hafez et al. [23] | 2020 | bypass anastomosis (100) | 100 | VITOM® | HD 3D |
| Pafitanis et al. [83] | 2020 | micro sutures (10), anastomoses (5) | 15 | Modus V™ | HD 3D |
| Rubini et al. [86] | 2020 | skull base (12) | 12 | VITOM® | HD 3D |
| Hafez et al. [28] | 2021 | bypass (5) | 5 | AEOS | 3D 4K |
| Authors | Year | Patients (n°) | Operative complications (%) | Surgical Procedures Switched from Exoscope to OM (%) | Video Image Quality | Surgical Field | Handling | Surgical Ergonomics | Educational Usefulness | Depth Perception | Operative Time and/or Workflow | Operative Team Involvement |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mamelak et al. [34] | 2010 | 16 | 0 | Nd | + | + | + | + | + | |||
| Shirzadi et al. [19] | 2012 | 24 | 0 | Nd | = | = | ||||||
| Belloch et al. [37] | 2014 | 23 | 0 | Nd | + | + | ||||||
| Birch et al. [38] | 2014 | 5 | 20 | Nd | = | = | ||||||
| Piquer et al. [39] | 2014 | 30 | 0 | Nd | + | + | + | |||||
| Parihar et al. [41] | 2016 | 39 | 0 | 0 | = | + | − | |||||
| Bauer et al. [43] | 2017 | 18 | 0 | Nd | = | = | ||||||
| Day [44] | 2017 | 49 | 8.2 | Nd | + | + | ||||||
| Gonen et al. [45] | 2017 | 200 | 0 | 0 | + | + | + | |||||
| Jackson et al. [46] | 2017 | 11 | 0 | 0 | + | + | ||||||
| Krishnan et al. [47] | 2017 | 18 | Nd | 0 | + | + | + | − | − | |||
| Labib et al. [48] | 2017 | 39 | 7.7 | Nd | + | + | ||||||
| Oertel & Burkhardt [51] | 2017 | 16 | 0 | 0 | = | = | + | + | = | + | ||
| Iyer & Chaichana [57] | 2018 | 14 | 0 | Nd | + | + | + | |||||
| Khalessi et al. [58] | 2018 | 18 | 0 | Nd | + | + | + | + | = | + | ||
| Mampre et al. [60] | 2018 | 15 | 0 | Nd | + | + | ||||||
| Bakhsheshian et al. [63] | 2019 | 25 | 4 | 0 | + | + | ||||||
| Garneau et al. [16] | 2019 | 6 | 0 | 0 | + | + | + | − | − | + | ||
| Herlan et al. [64] | 2019 | 6 | NA | Nd | + | = | + | = | ||||
| Kwan et al. [65] | 2019 | 10 | 0 | Nd | + | + | + | + | + | + | ||
| Muhammad et al. [7] | 2019 | 8 | 0 | 0 | + | + | + | − | ||||
| Murai et al. [67] | 2019 | 22 | 0 | 18.2% | + | + | + | |||||
| Smith et al. [69] | 2019 | 11 | 0 | 36.4% | = | = | + | + | + | |||
| Ahmad et al. [9] | 2020 | 22 | 0 | Nd | + | + | + | + | = | |||
| Ariffin et al. [15] | 2020 | 69 | 5.8 | Nd | + | + | + | + | + | + | + | |
| Baron et al. [10] | 2020 | 28 | 3.6 | Nd | + | + | ||||||
| Burkhardt et al. [71] | 2020 | 34 | Nd | 17.6% | =/+ | =/+ | − | |||||
| Chen et al. [73] | 2020 | 39 | 30.8 | Nd | = | + | = | + | ||||
| Eichberg et al. [30] | 2020 | 56 | 8.9 | Nd | = | = | = | |||||
| Hafez et al. [23] | 2020 | 100 | NA | Nd | = | + | + | |||||
| Pafitanis et al. [83] | 2020 | 15 | NA | Nd | = | = | ||||||
| Roethe et al. [85] | 2020 | 29 | 6.9 | 3.4% | − | = | = | + | = | |||
| Siller et al. [5] | 2020 | 60 | 0 | 0 | − | = | = | + | + | − | = | + |
| Teo et al. [29] | 2020 | 8 | 0 | Nd | =/+ | =/+ | =/+ | |||||
| Visocchi et al. [89] | 2020 | 6 | 0 | Nd | + | + | ||||||
| Amoo et al. [90] | 2021 | 18 | 0 | 0 | = | + | + | + | ||||
| Muscas et al. [27] | 2021 | 14 | 0 | 57.1% | + | + | + | + | ||||
| Muto et al. [93] | 2021 | 5 | 0 | 0 | = | = | ||||||
| Rösler et al. [26] | 2021 | 39 | 0 | 69.2% | + | + | − | |||||
| Rotermund et al. [95] | 2021 | 296 | 0 | 0 | + | + | + | + | = | |||
| Shimizu et al. [96] | 2021 | 14 | 0 | 0 | + | + | ||||||
| Yoon et al. [25] | 2021 | 11 | 9.1 | 18.2% | = | + | + | + | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montemurro, N.; Scerrati, A.; Ricciardi, L.; Trevisi, G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. J. Clin. Med. 2022, 11, 223. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010223
Montemurro N, Scerrati A, Ricciardi L, Trevisi G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. Journal of Clinical Medicine. 2022; 11(1):223. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010223
Chicago/Turabian StyleMontemurro, Nicola, Alba Scerrati, Luca Ricciardi, and Gianluca Trevisi. 2022. "The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery" Journal of Clinical Medicine 11, no. 1: 223. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010223