
Peroral Cholangioscopy-Guided Targeted Biopsy versus Conventional Endoscopic Transpapillary Forceps Biopsy for Biliary Stricture with Suspected Bile Duct Cancer

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Diagnostic Algorithms of Suspected Bile Duct Cancer in Our Institutions
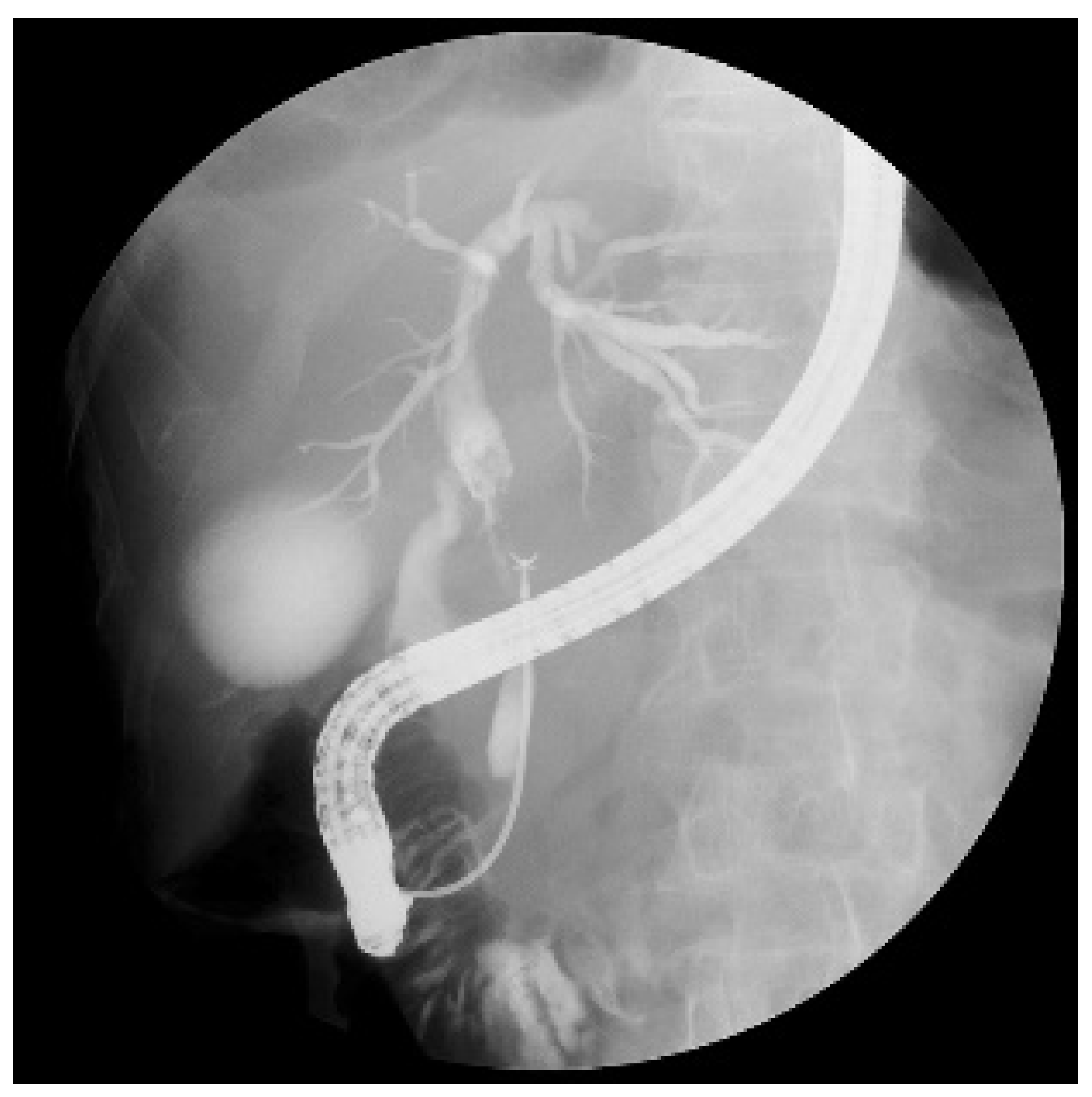
2.4. Endoscopic Procedures
2.5. Final Diagnosis
2.6. Outcome Measurements
2.7. Evaluation of Biopsy Samples
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Sensitivity, Specificity, PPV, NPV, and Accuracy of Fluoroscopy- and POCS-Guided Biopsies
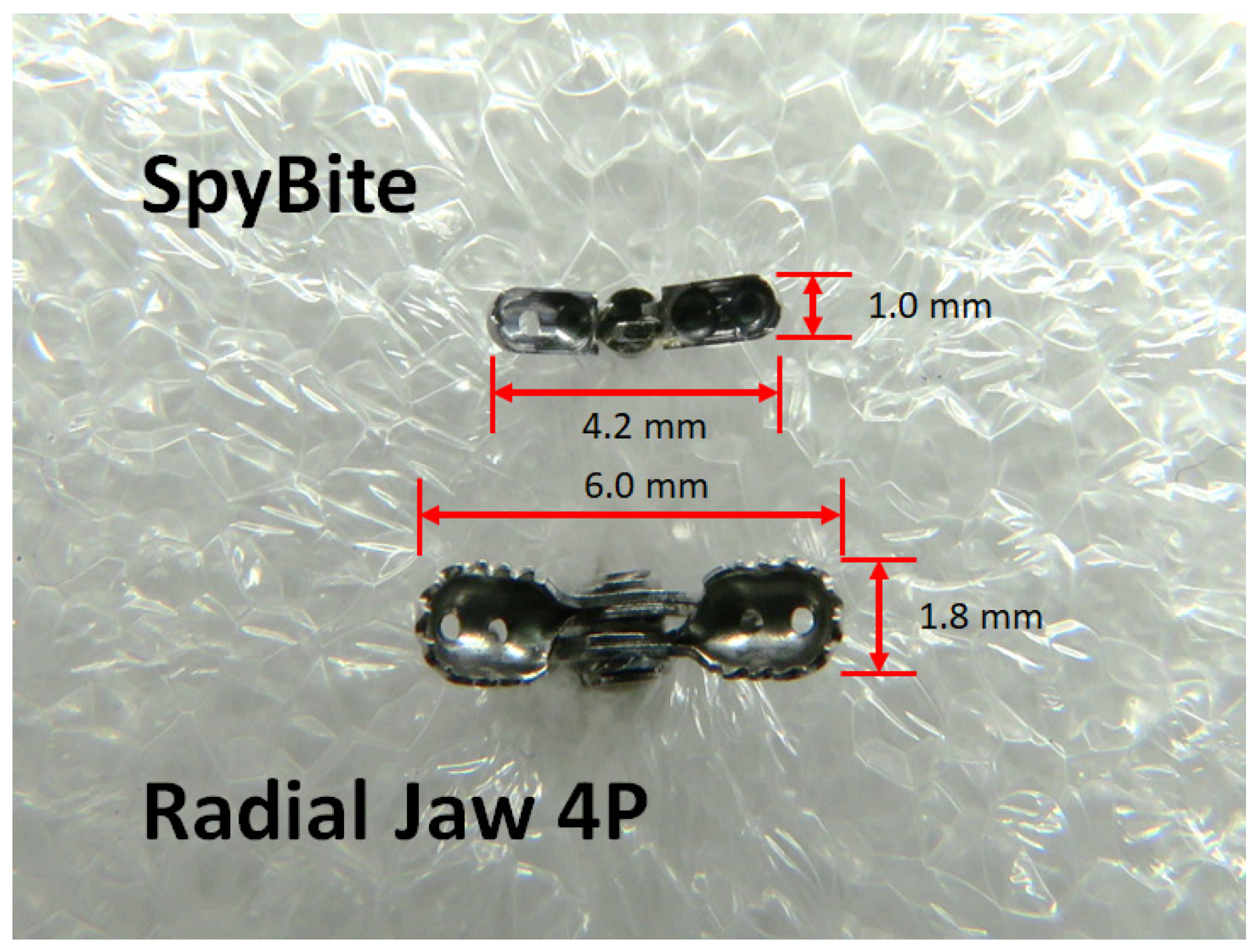
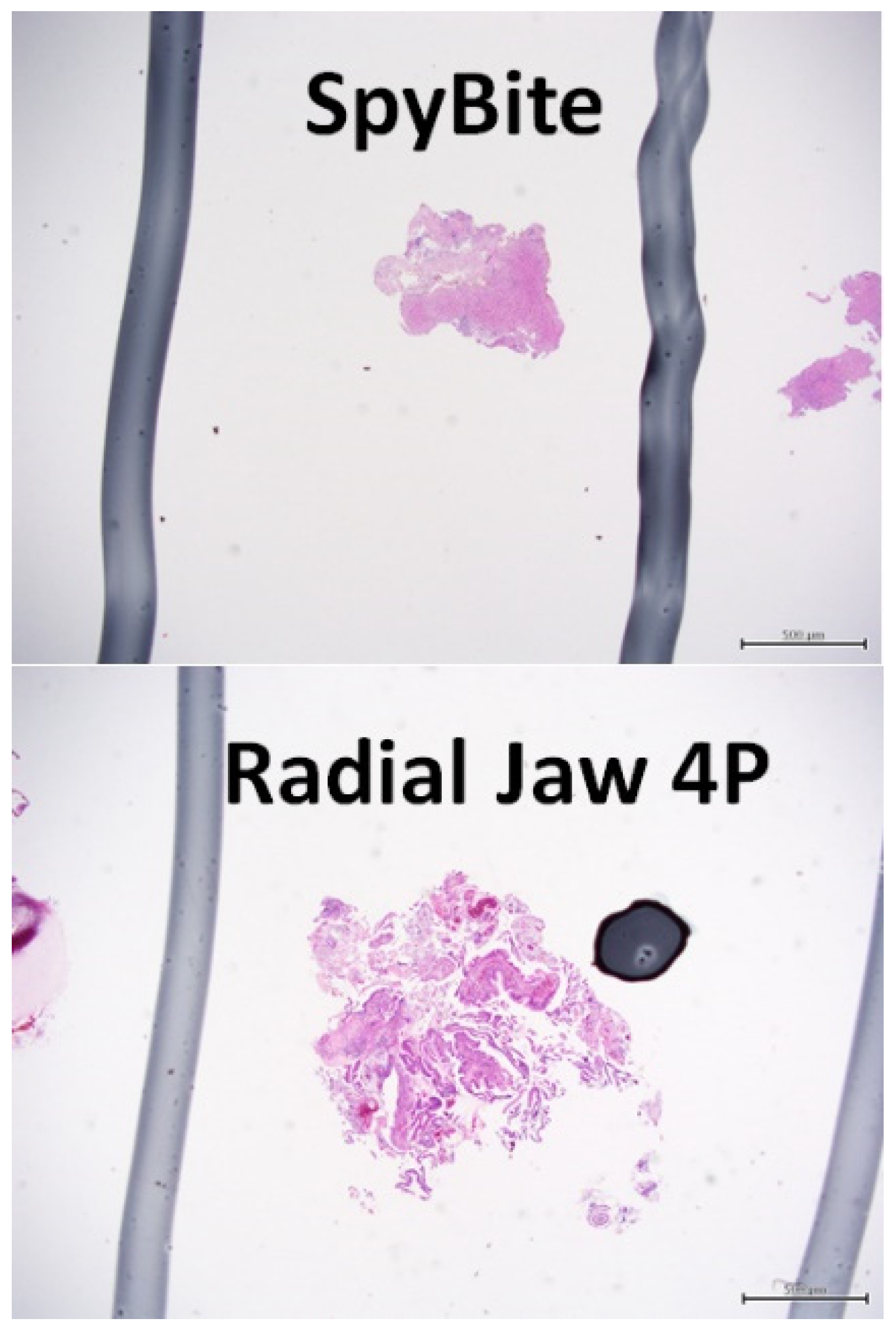
3.3. Comparison of the Size of the Biopsy Samples
3.4. Comparison of the Quality of the Biopsy Samples
3.5. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banales, J.M.; Marin, J.; Lamarca, A.; Rodrigues, P.M.; Gores, G.J. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Brandi, G. Pitfalls, challenges, and updates in adjuvant systemic treatment for resected biliary tract cancer. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Derdeyn, J.; Laleman, W. Current role of endoscopic cholangioscopy. Curr. Opin. Gastroenterol. 2018, 34, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Nakai, Y.; Isayama, H.; Wang, H.; Rerknimitr, R.; Khor, C.; Yasuda, I. International consensus statements for endoscopic management of distal biliary stricture. J. Gastroenterol. Hepatol. 2020, 35, 967–979. [Google Scholar] [CrossRef] [Green Version]
- Tanisaka, Y.; Mizuide, M.; Fujita, A.; Ogawa, T.; Ryozawa, S. Diagnostic Process Using Endoscopy for Biliary Strictures: A Narrative Review. J. Clin. Med. 2021, 10, 1048. [Google Scholar] [CrossRef]
- Navaneethan, U.; Njei, B.; Lourdusamy, V.; Konjeti, R.; Vargo, J.J.; Parsi, M.A. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: A systematic review and meta-analysis. Gastrointest. Endosc. 2015, 81, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.K. Preclinical characterization of the Spyglass peroral cholangiopancreatoscopy system for direct access, visualization, and biopsy. Gastrointest. Endosc. 2007, 65, 303–311. [Google Scholar] [CrossRef]
- Hartman, D.J.; Slivka, A.; Giusto, D.A.; Krasinskas, A.M. Tissue yield and diagnostic efficacy of fluoroscopic and cholangioscopic techniques to assess indeterminate biliary strictures. Clin. Gastroenterol. Hepatol. 2012, 10, 1042–1046. [Google Scholar] [CrossRef]
- Woo, Y.S.; Lee, J.K.; Oh, S.H.; Kim, M.J.; Jung, J.G.; Lee, K.H. Role of SpyGlass peroral cholangioscopy in the evaluation of indeterminate biliary lesions. Dig. Dis. Sci. 2014, 59, 2565–2570. [Google Scholar] [CrossRef]
- Kurihara, T.; Yasuda, I.; Isayama, H. Diagnostic and therapeutic single-operator cholangiopancreatoscopy in biliopancreatic diseases: Prospective multicenter study in Japan. World J. Gastroenterol. 2016, 22, 1891–1901. [Google Scholar] [CrossRef]
- Navaneethan, U.; Hasan, M.K.; Kommaraju, K.; Zhu, X.; Herbert-Magee, S.; Hawes, R.H. Digital, single-operator cholangiopancreatoscopy in the diagnosis and management of pancreatobiliary disorders: A multicenter clinical experience (with video). Gastrointest. Endosc. 2016, 84, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Atsushi, O.; Takeshi, O.; Akira, M.; Nobu, N.; Miyuki, I.; Wataru, T. Prospective evaluation of digital single-operator cholangioscope for diagnostic and therapeutic procedures (with videos). Dig. Endosc. 2017, 29, 782–789. [Google Scholar]
- Shah, R.J.; Raijman, I.; Brauer, B. Performance of a fully disposable, digital, single-operator cholangiopancreatoscope. Endoscopy 2017, 49, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Laleman, W.; Verraes, K.; Steenbergen, W.V.; Cassiman, D.; Nevens, F.; Schalk, V. Usefulness of the single-operator cholangioscopy system SpyGlass in biliary disease: A single-center prospective cohort study and aggregated review. Surg. Endosc. 2017, 31, 2223–2232. [Google Scholar] [CrossRef]
- Gerges, C.; Beyna, T.; Tang, R.; Fracp, F.B.; Lau, J.; Geenen, E.V. Digital single-operator peroral cholangioscopy-guided biopsy sampling versus ERCP-guided brushing for indeterminate biliary strictures: A prospective, randomized, multicenter trial (with video). Gastrointest. Endosc. 2020, 91, 1105–1113. [Google Scholar] [CrossRef]
- Bang, J.Y.; Navaneethan, U.; Hasan, M.; Sutton, B.; Hawes, R.; Varadarajulu, S. Optimizing Outcomes of Single-Operator Cholangioscopy-Guided Biopsies Based on a Randomized Trial. Clin. Gastroenterol. Hepatol. 2020, 18, 441–448.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almadi, M.A.; Itoi, T.; Moon, J.H.; Goenka, M.K.; Seo, D.W. Using single-operator cholangioscopy for endoscopic evaluation of indeterminate biliary strictures: Results from a large multinational registry. Endoscopy 2020, 52, 574–582. [Google Scholar] [CrossRef]
- Jang, S.; Stevens, T.; Lei, K.; Vargo, J.J.; Parsi, M.A. Efficacy of digital single-operator cholangioscopy and factors affecting its accuracy in the evaluation of indeterminate biliary stricture. Gastrointest. Endosc. 2020, 91, 385–393.e1. [Google Scholar] [CrossRef] [PubMed]
- Vries, A.D.; Frans, V.; Steege, R.T.; Koornstra, J.J.; Buddingh, K.T.; Gouw, A. Limited diagnostic accuracy and clinical impact of single-operator peroral cholangioscopy for indeterminate biliary strictures. Endoscopy 2020, 52, 107–114. [Google Scholar] [CrossRef]
- Draganov, P.V.; Chauhan, S.; Wagh, M.S.; Gupte, A.R.; Lin, T.; Hou, W. Diagnostic accuracy of conventional and cholangioscopy-guided sampling of indeterminate biliary lesions at the time of ERCP: A prospective, long-term follow-up study. Gastrointest. Endosc. 2012, 75, 347–353. [Google Scholar] [CrossRef]
- Walter, D.; Peveling-Oberhag, J.; Schulze, F.; Bon, D.; Albert, J.G. Intraductal biopsies in indeterminate biliary stricture: Evaluation of histopathological criteria in fluoroscopy- vs. cholangioscopy guided technique. Dig. Liver Dis. 2016, 48, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Onoyama, T.; Hamamoto, W.; Sakamoto, Y.; Kawahara, S.; Isomoto, H. Peroral cholangioscopy-guided forceps biopsy versus fluoroscopy-guided forceps biopsy for extrahepatic biliary lesions. JGH Open 2020, 4, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, U.; Hasan, M.K.; Lourdusamy, V. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: A systematic review. Gastrointest. Endosc. 2015, 82, 608–614.e2. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, M.; Maetani, I.; Terada, K. Usefulness of endoscopic retrograde biliary biopsy using large-capacity forceps for extrahepatic biliary strictures: A prospective randomized study. Endoscopy 2010, 42, 837–841. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median Age, Years (Range) | 74 (43–89) |
| Male/female | 40/19 |
| Location of the lesion | |
| Hilar | 25 |
| Distal | 34 |
| Median length of biliary stricture, mm (range) | 16 (2–54) |
| Final diagnosis | |
| Bile duct cancer | 48 |
| Gallbladder cancer | 2 |
| Benign stricture | 9 |
| Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | Accuracy (95% CI) | |
|---|---|---|---|---|---|
| POCS-guided biopsy | 54.0% (40.4–67.0) | 100% (70.1–100) | 100% (87.5–100) | 28.1% (15.6–45.4) | 61.0% (48.3–72.4) |
| Fluoroscopy-guided biopsy | 64.0% (50.1–75.9) | 100% (89.3–100) | 100% (89.3–100) | 33.3% (18.6–52.2) | 69.5% (56.9–79.7) |
| Combined cholangioscopy-guided and fluoroscopy-guided biopsy | 80.0% (67.0–88.8) | 100% (70.1–100) | 100% (91.2–100) | 47.4% (27.3–68.3) | 83.1% (71.5–90.5) |
| POCS-Guided Biopsy | Fluoroscopy-Guided Biopsy | p-Value | |
|---|---|---|---|
| Number of biopsy samples | 2.2 ± 0.7 | 2.1 ± 0.6 | 0.163 |
| Size of sample, mm2 | 0.90 ± 1.13 | 1.77 ± 2.00 | <0.001 |
| Excellent | Good | Poor | Inadequate | p-Value | |
|---|---|---|---|---|---|
| POCS-guided biopsy | 21 | 29 | 9 | 0 | 0.006 |
| Fluoroscopy-guided biopsy | 39 | 14 | 6 | 0 |
| Author (Year) | Study Design | Method | N | Sensitivity | p |
|---|---|---|---|---|---|
| Draganov (2012) | Prospective | Fluoroscopy-guided POCS-guided | 26 26 (identical cohort) | 29.4% 76.5% | 0.0215 |
| Walter (2016) | Retrospective | Fluoroscopy-guided POCS-guided | 68 38 | 45.7% 58.3% | 0.674 |
| Onoyama (2020) | Retrospective | Fluoroscopy-guided POCS-guided | 31 31 (propensity score-matched cohort) | 82.4% 83.3% | 1.000 |
| Present study | Retrospective | Fluoroscopy-guided POCS-guided | 59 59 (identical cohort) | 64.0% 54.0% | 0.416 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekine, K.; Yasuda, I.; Doi, S.; Kuniyoshi, N.; Tsujikawa, T.; Takano, Y.; Mabuchi, M.; Takahashi, K.; Kawamoto, M.; Takahashi, M.; et al. Peroral Cholangioscopy-Guided Targeted Biopsy versus Conventional Endoscopic Transpapillary Forceps Biopsy for Biliary Stricture with Suspected Bile Duct Cancer. J. Clin. Med. 2022, 11, 289. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020289
Sekine K, Yasuda I, Doi S, Kuniyoshi N, Tsujikawa T, Takano Y, Mabuchi M, Takahashi K, Kawamoto M, Takahashi M, et al. Peroral Cholangioscopy-Guided Targeted Biopsy versus Conventional Endoscopic Transpapillary Forceps Biopsy for Biliary Stricture with Suspected Bile Duct Cancer. Journal of Clinical Medicine. 2022; 11(2):289. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020289
Chicago/Turabian StyleSekine, Katsunori, Ichiro Yasuda, Shinpei Doi, Noriyuki Kuniyoshi, Takayuki Tsujikawa, Yuichi Takano, Masatoshi Mabuchi, Kosuke Takahashi, Masashi Kawamoto, Mikiko Takahashi, and et al. 2022. "Peroral Cholangioscopy-Guided Targeted Biopsy versus Conventional Endoscopic Transpapillary Forceps Biopsy for Biliary Stricture with Suspected Bile Duct Cancer" Journal of Clinical Medicine 11, no. 2: 289. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020289