
Induction and Maintenance Treatment of Lupus Nephritis: A Comprehensive Review of Meta-Analyses

 , , , , , , , , , , and add
Show full author list
, , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
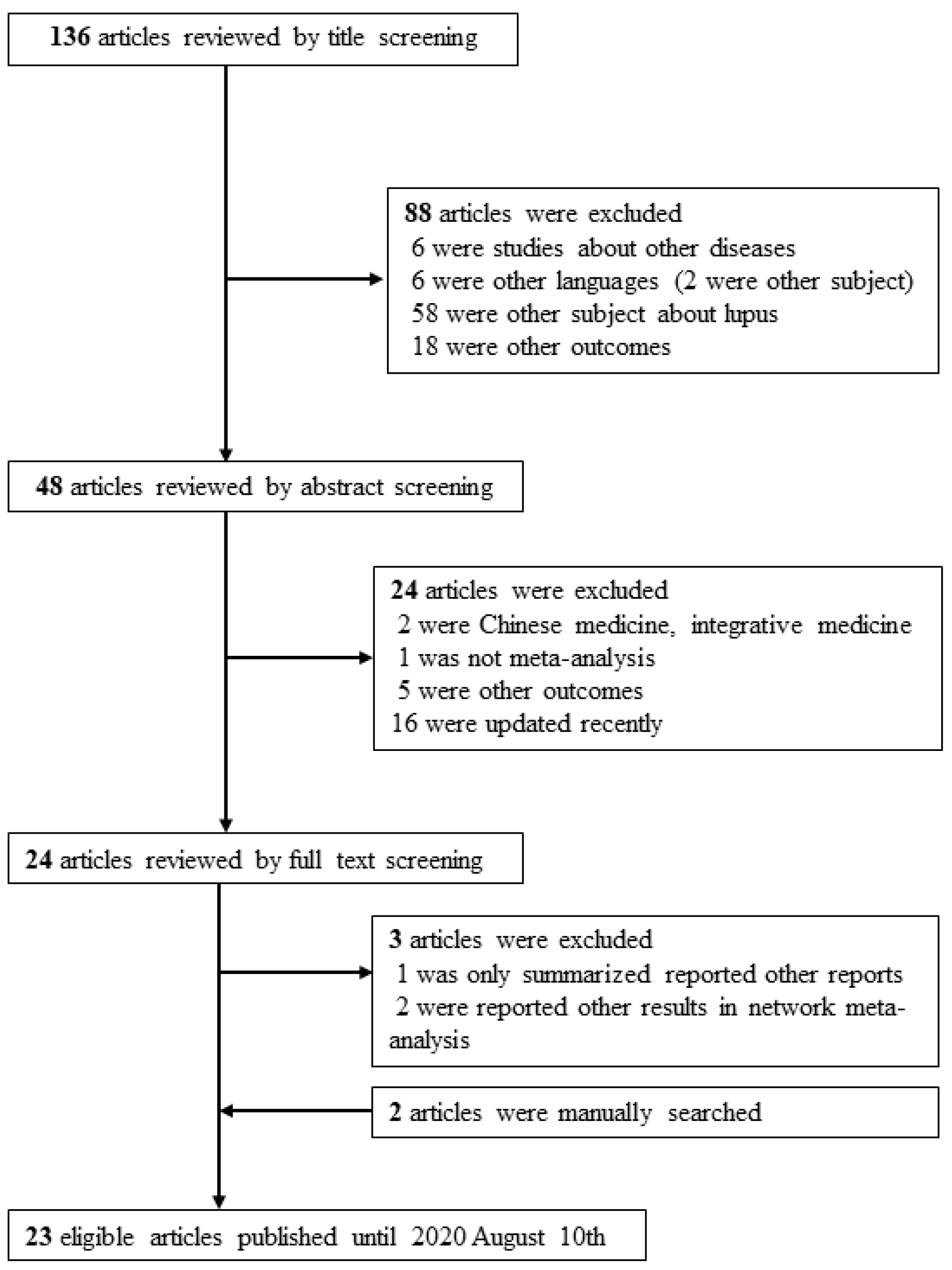
2.2. Search Strategy and Data Extraction
3. Results
3.1. Characteristics of Meta-Analysis
3.2. Complete and Partial Remission Rates during Induction Therapy in Lupus Nephritis
3.3. Relapse during Maintenance Therapy in Lupus Nephritis
3.4. Mortality during Induction Therapy in Lupus Nephritis
3.5. Progression to ESKD during Induction Therapy in Lupus Nephritis
3.6. Infection during Induction Therapy in Lupus Nephritis
3.7. Relapse during Maintenance Therapy in Lupus Nephritis
3.8. Mortality during Maintenance Therapy in Lupus Nephritis
3.9. Progression to ESKD during Maintenance Therapy in Lupus Nephritis
3.10. Infection during Maintenance Therapy in Lupus Nephritis
3.11. Malignancy during Induction and Maintenance Therapy in Lupus Nephritis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anders, H.J.; Saxena, R.; Zhao, M.H.; Parodis, I.; Salmon, J.E.; Mohan, C. Lupus nephritis. Nat. Rev. Dis. Primers 2020, 6, 7. [Google Scholar] [CrossRef]
- Cervera, R.; Khamashta, M.A.; Hughes, G.R. The Euro-lupus project: Epidemiology of systemic lupus erythematosus in Europe. Lupus 2009, 18, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.S.; Nie, Y.K.; Jin, X.M.; Yu, H.M.; Li, Y.N.; Sun, Y. The efficacy and safety of leflunomide therapy in lupus nephritis by repeat kidney biopsy. Rheumatol. Int. 2009, 29, 1331–1335. [Google Scholar] [CrossRef]
- Singh, J.A.; Hossain, A.; Kotb, A.; Wells, G.A. Comparative effectiveness of immunosuppressive drugs and corticosteroids for lupus nephritis: A systematic review and network meta-analysis. Syst. Rev. 2016, 5, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunnicliffe, D.J.; Palmer, S.C.; Henderson, L.; Masson, P.; Craig, J.C.; Tong, A.; Singh-Grewal, D.; Flanc, R.S.; Roberts, M.A.; Webster, A.C.; et al. Immunosuppressive treatment for proliferative lupus nephritis. Cochrane Database Syst. Rev. 2018, 6, Cd002922. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [Green Version]
- Croca, S.C.; Rodrigues, T.; Isenberg, D.A. Assessment of a lupus nephritis cohort over a 30-year period. Rheumatology (Oxford) 2011, 50, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Tektonidou, M.G.; Dasgupta, A.; Ward, M.M. Risk of End-Stage Renal Disease in Patients With Lupus Nephritis, 1971-2015: A Systematic Review and Bayesian Meta-Analysis. Arthritis Rheumatol. 2016, 68, 1432–1441. [Google Scholar] [CrossRef]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Palmer, S.C.; Tunnicliffe, D.J.; Singh-Grewal, D.; Mavridis, D.; Tonelli, M.; Johnson, D.W.; Craig, J.C.; Tong, A.; Strippoli, G.F.M. Induction and Maintenance Immunosuppression Treatment of Proliferative Lupus Nephritis: A Network Meta-analysis of Randomized Trials. Am. J. Kidney Dis. 2017, 70, 324–336. [Google Scholar] [CrossRef] [Green Version]
- Zhou, T.; Lin, S.; Yang, S.; Lin, W. Efficacy and safety of tacrolimus in induction therapy of patients with lupus nephritis. Drug Des. Dev. Ther. 2019, 13, 857–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Song, G.G. Relative efficacy and safety of tacrolimus, mycophenolate mofetil, and cyclophosphamide as induction therapy for lupus nephritis: A Bayesian network meta-analysis of randomized controlled trials. Lupus 2015, 24, 1520–1528. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ji, L.; Yang, L.; Tang, X.; Qin, W. The effect of calcineurin inhibitors in the induction and maintenance treatment of lupus nephritis: A systematic review and meta-analysis. Int. Urol. Nephrol. 2016, 48, 731–743. [Google Scholar] [CrossRef]
- Bae, S.C.; Lee, Y.H. Comparative efficacy and safety of low-dose and high-dose cyclophosphamide as induction therapy for lupus nephritis: A network meta-analysis. Z. Rheumatol. 2019, 78, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.K.; Masson, P.; Craig, J.C.; Roberts, M.A.; Flanc, R.S.; Strippoli, G.F.; Webster, A.C. Induction and maintenance treatment of proliferative lupus nephritis: A meta-analysis of randomized controlled trials. Am. J. Kidney Dis. 2013, 61, 74–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, J.A.; Hossain, A.; Kotb, A.; Oliveira, A.; Mudano, A.S.; Grossman, J.; Winthrop, K.; Wells, G.A. Treatments for Lupus Nephritis: A Systematic Review and Network Metaanalysis. J. Rheumatol. 2016, 43, 1801–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, M.; Song, X.; Dong, L.; Xin, X.; Dong, J. Systematic evaluation of different doses of cyclophosphamide induction therapy for lupus nephritis. Medicine 2017, 96, e9408. [Google Scholar] [CrossRef]
- Deng, J.; Xie, H.; Zhu, L.; Luo, L.; Xie, H. Maintenance therapy for lupus nephritis with mycophenolate mofetil or azathioprine. A meta-analysis. Clin. Nephrol. 2019, 91, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Luo, L.; Zhu, L.; Xie, H.; Xie, H. Multitarget therapy versus intravenous cyclophosphamide in the induction treatment of lupus nephritis: A metaanalysis of randomized controlled trials. Turk. J. Med. Sci. 2018, 48, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Rao, Y.; Liu, L.; Lin, J.; Yang, H.; Zhang, X.; Chen, Z. The Efficacy and Safety of Leflunomide for the Treatment of Lupus Nephritis in Chinese Patients: Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0144548. [Google Scholar] [CrossRef] [Green Version]
- Kraaij, T.; Bredewold, O.W.; Trompet, S.; Huizinga, T.W.; Rabelink, T.J.; de Craen, A.J.; Teng, Y.K. TAC-TIC use of tacrolimus-based regimens in lupus nephritis. Lupus Sci. Med. 2016, 3, e000169. [Google Scholar] [CrossRef]
- Zhong, Z.; Li, H.; Zhong, H.; Zhou, T. Clinical efficacy and safety of rituximab in lupus nephritis. Drug Des. Devel. Ther. 2019, 13, 845–856. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Ou, Q.; Tang, Y.; Fu, S.; Liang, P.; Yu, Y.; Xu, Z.; Chen, Y.; Xu, A. Corticosteroids combined with doublet or single-agent immunosuppressive therapy for active proliferative lupus nephritis. Clin. Rheumatol. 2019, 38, 2519–2528. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Huo, D.; Wu, Q.; Yang, Z.; Liao, Y. A meta-analysis of randomized controlled trials comparing tacrolimus with intravenous cyclophosphamide in the induction treatment for lupus nephritis. Tohoku J. Exp. Med. 2012, 227, 281–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, K.T.; Tseng, C.H.; Hsieh, T.Y.; Chen, D.Y. Induction therapy for membranous lupus nephritis: A systematic review and network meta-analysis. Int. J. Rheum. Dis. 2018, 21, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Hannah, J.; Casian, A.; D’Cruz, D. Tacrolimus use in lupus nephritis: A systematic review and meta-analysis. Autoimmun. Rev. 2016, 15, 93–101. [Google Scholar] [CrossRef]
- Kandala, N.B.; Connock, M.; Grove, A.; Sutcliffe, P.; Mohiuddin, S.; Hartley, L.; Court, R.; Cummins, E.; Gordon, C.; Clarke, A. Belimumab: A technological advance for systemic lupus erythematosus patients? Report of a systematic review and meta-analysis. BMJ Open 2013, 3, e002852. [Google Scholar] [CrossRef]
- Flanc, R.S.; Roberts, M.A.; Strippoli, G.F.; Chadban, S.J.; Kerr, P.G.; Atkins, R.C. Treatment of diffuse proliferative lupus nephritis: A meta-analysis of randomized controlled trials. Am. J. Kidney Dis. 2004, 43, 197–208. [Google Scholar] [CrossRef]
- Shamliyan, T.A.; Dospinescu, P. Additional Improvements in Clinical Response From Adjuvant Biologic Response Modifiers in Adults With Moderate to Severe Systemic Lupus Erythematosus Despite Immunosuppressive Agents: A Systematic Review and Meta-analysis. Clin. Ther. 2017, 39, 1479–1506.e1445. [Google Scholar] [CrossRef]
- Borba, H.H.; Wiens, A.; de Souza, T.T.; Correr, C.J.; Pontarolo, R. Efficacy and safety of biologic therapies for systemic lupus erythematosus treatment: Systematic review and meta-analysis. BioDrugs 2014, 28, 211–228. [Google Scholar] [CrossRef]
- Mok, C.C. Calcineurin inhibitors in systemic lupus erythematosus. Best Pract. Res. Clin. Rheumatol. 2017, 31, 429–438. [Google Scholar] [CrossRef]
- Fransen, J.H.; van der Vlag, J.; Ruben, J.; Adema, G.J.; Berden, J.H.; Hilbrands, L.B. The role of dendritic cells in the pathogenesis of systemic lupus erythematosus. Arthritis Res. Ther. 2010, 12, 207. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.H.; Kronbichler, A.; Park, D.D.; Park, Y.; Moon, H.; Kim, H.; Choi, J.H.; Choi, Y.; Shim, S.; Lyu, I.S.; et al. Neutrophil extracellular traps (NETs) in autoimmune diseases: A comprehensive review. Autoimmun. Rev. 2017, 16, 1160–1173. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Okuyama, K.; Konno, O.; Jojima, Y.; Akashi, I.; Nakamura, Y.; Iwamoto, H.; Hama, K.; Iwahori, T.; Uchiyama, M.; et al. Optimal dose and target trough level in cyclosporine and tacrolimus conversion in renal transplantation as evaluated by lymphocyte drug sensitivity and pharmacokinetic parameters. Transplant. Proc. 2005, 37, 1745–1747. [Google Scholar] [CrossRef]
- Rovin, B.H.; Solomons, N.; Pendergraft, W.F., 3rd; Dooley, M.A.; Tumlin, J.; Romero-Diaz, J.; Lysenko, L.; Navarra, S.V.; Huizinga, R.B. A randomized, controlled double-blind study comparing the efficacy and safety of dose-ranging voclosporin with placebo in achieving remission in patients with active lupus nephritis. Kidney Int. 2019, 95, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Rovin, B.H.; Teng, Y.K.O.; Ginzler, E.M.; Arriens, C.; Caster, D.J.; Romero-Diaz, J.; Gibson, K.; Kaplan, J.; Lisk, L.; Navarra, S.; et al. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): A double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2021, 397, 2070–2080. [Google Scholar] [CrossRef]
- Kronbichler, A.; Neumann, I.; Mayer, G. Moderator’s view: The use of calcineurin inhibitors in the treatment of lupus nephritis. Nephrol. Dial. Transplant. 2016, 31, 1572–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, C.C. Pro: The use of calcineurin inhibitors in the treatment of lupus nephritis. Nephrol. Dial. Transplant. 2016, 31, 1561–1566. [Google Scholar] [CrossRef]
- Fernandez Nieto, M.; Jayne, D.R. Opponent’s comments. Nephrol. Dial. Transplant. 2016, 31, 1566–1567. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C. Con: Cyclophosphamide for the treatment of lupus nephritis. Nephrol. Dial. Transplant. 2016, 31, 1053–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dooley, M.A.; Jayne, D.; Ginzler, E.M.; Isenberg, D.; Olsen, N.J.; Wofsy, D.; Eitner, F.; Appel, G.B.; Contreras, G.; Lisk, L.; et al. Mycophenolate versus azathioprine as maintenance therapy for lupus nephritis. N. Engl. J. Med. 2011, 365, 1886–1895. [Google Scholar] [CrossRef] [Green Version]
- Houssiau, F.A.; D’Cruz, D.; Sangle, S.; Remy, P.; Vasconcelos, C.; Petrovic, R.; Fiehn, C.; de Ramon Garrido, E.; Gilboe, I.M.; Tektonidou, M.; et al. Azathioprine versus mycophenolate mofetil for long-term immunosuppression in lupus nephritis: Results from the MAINTAIN Nephritis Trial. Ann. Rheum. Dis. 2010, 69, 2083–2089. [Google Scholar] [CrossRef] [PubMed]
- Dörner, T. Hydroxychloroquine in SLE: Old drug, new perspectives. Nat. Rev. Rheumatol. 2010, 6, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, C.B.; Pedrosa, T.; Kupa, L.d.V.K.; Aikawa, N.E.; Borba, E.F.; Vendramini, M.B.G.; Silva, C.A.; Pasoto, S.G.; Bonfa, E. Hydroxychloroquine blood levels in stable lupus nephritis under low dose (2–3 mg/kg/day): 12-month prospective randomized controlled trial. Clin. Rheumatol. 2021, 40, 2745–2751. [Google Scholar] [CrossRef] [PubMed]
- Timlin, H.; Magder, L.; Petri, M. Clinical Outcomes Observed among Biopsy Proven Lupus Nephritis Patients Treated with Mycophenolate Mofetil as First-line Therapy. Cureus 2017, 9, e1907. [Google Scholar] [CrossRef] [Green Version]
- Furie, R.; Rovin, B.H.; Houssiau, F.; Malvar, A.; Teng, Y.K.O.; Contreras, G.; Amoura, Z.; Yu, X.; Mok, C.C.; Santiago, M.B.; et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N. Engl. J. Med. 2020, 383, 1117–1128. [Google Scholar] [CrossRef]
- Acharya, N. Glucocorticoid withdrawal in lupus—to do or not to do? Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Houssiau, F.A.; Vasconcelos, C.; D’Cruz, D.; Sebastiani, G.D.; de Ramon Garrido, R.; Danieli, M.G.; Abramovicz, D.; Blockmans, D.; Mathieu, A.; Direskeneli, H.; et al. Immunosuppressive therapy in lupus nephritis: The Euro-Lupus Nephritis Trial, a randomized trial of low-dose versus high-dose intravenous cyclophosphamide. Arthritis Rheum. 2002, 46, 2121–2131. [Google Scholar] [CrossRef]
- Binda, V.; Trezzi, B.; Del Papa, N.; Beretta, L.; Frontini, G.; Porata, G.; Fabbrini, P.; Pozzi, M.R.; Messa, P.; Sinico, R.A.; et al. Belimumab may decrease flare rate and allow glucocorticoid withdrawal in lupus nephritis (including dialysis and transplanted patient). J. Nephrol. 2020, 33, 1019–1025. [Google Scholar] [CrossRef]
- Rovin, B.H.; Furie, R.; Latinis, K.; Looney, R.J.; Fervenza, F.C.; Sanchez-Guerrero, J.; Maciuca, R.; Zhang, D.; Garg, J.P.; Brunetta, P.; et al. Efficacy and safety of rituximab in patients with active proliferative lupus nephritis: The Lupus Nephritis Assessment with Rituximab study. Arthritis Rheum. 2012, 64, 1215–1226. [Google Scholar] [CrossRef]
- Kronbichler, A.; Brezina, B.; Gauckler, P.; Quintana, L.F.; Jayne, D.R.W. Refractory lupus nephritis: When, why and how to treat. Autoimmun. Rev. 2019, 18, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Puhan, M.A.; Vedula, S.S.; Singh, S.; Dickersin, K.; The Ad Hoc Network Meta-analysis Methods Meeting Working Group. Network meta-analysis-highly attractive but more methodological research is needed. BMC Med. 2011, 9, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Comparison | Author, Year | M | T | Reported Summary Effect (95% CI) | NMA Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) | NMA Author, Year |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MMF + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.17 (0.97–1.42) | 1.44 (1.00–2.06) | 0.11 | 0% (0.46) | 1/10 | 868/441 | 1.07 (0.54–2.09) | - | Palmer, et al., 2017 [10] |
| MMF + CPA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.22 (0.78–1.89) | 1.48 (0.62–3.53) | 0.38 | - | 0//1 | 82/40 | 1.22 (0.78–1.89) | 0.38 | Palmer, et al., 2017 [10] |
| TAC + GC vs. CPA + GC | Zhou, et al., 2019 [11] | F | RR | 2.41 (1.8–3.99) | 2.35 (1.03–5.45) | 0.0006 | 0% (0.93) | 0/7 | 276/135 | 1.64 (0.65–4.14) | 0.20 | Lee, et al., 2015 [12] |
| CNI + GC vs. CPA + GC | Zhang, et al., 2016 [13] | F | RR | 1.33 (0.93–1.90) | 1.74 (1.09–2.79) | 0.12 | 0% (0.97) | 0/4 | 188/95 | 1.36 (0.83–2.22) | 0.20 | Palmer, et al., 2017 [10] |
| CPA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | F | RR | 2.63 (0.13–54.64) | 0.57 (0.23–1.40) * | 0.53 | - | 0/1 | 13/7 | 2.63 (0.13–54.64) | 0.53 | Palmer, et al., 2017 [10] |
| AZA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 2.03 (0.64–6.46) | 1.53 (1.53–2.39) † | 0.23 | - | 0/1 | 59/38 | 2.03 (0.64–6.46) | 0.23 | Singh, et al., 2016 [4] |
| Low CPA vs. High CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 1.09 (0.63–1.86) | 1.46 (0.83–2.86) | 0.76 | 67% (0.05) | 0/3 | 267/117 | 1.37 (0.75–2.50) | 0.29 | Bae, et al., 2019 [14] |
| TAC + GC vs. MMF + GC | Zhou, et al., 2019 [11] | F | RR | 0.95 (0.54–1.64) | 1.60 (0.70–3.57) | 0.84 | 42% (0.18) | 0/3 | 206/103 | 1.13 (0.59–2.18) | 0.71 | Lee, et al., 2015 [12] |
| Comparison | Author, Year | M | Type of Metrics | Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|
| Complete Remission | ||||||||||
| CPA vs. Others | ||||||||||
| MMF + TAC + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 2.38 (1.07–5.30) | 0.034 | 57% (0.13) | 2/2 | 402/201 | 1.80 (1.34–2.42) | <0.001 |
| MMF + TAC + GC vs. CPA + GC | Zhou, et al., 2019 [11] | R | RR | 5.13 (0.75–35.02) | 0.10 | 69% (0.07) | 1/2 | 402/201 | 2.49 (1.59–3.88) | <0.001 |
| MMF + GC vs. Oral CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.98 (0.74–1.30) | 0.88 | - | 0/1 | 62/30 | 0.98 (0.74–1.30) | 0.88 |
| Multi target vs. CPA | Deng, et al., 2018 [18] | F | RR | 1.94 (1.61–2.33) | <0.001 | 0% (0.48) | 6/8 | 801/406 | 1.80 (1.34–2.42) | <0.001 |
| Leflunomide +GC vs. CPA + GC | Cao, et al., 2015 [20] | F | RR | 1.41 (1.10–1.82) | 0.007 | 0% (0.94) | 1/9 | 442/220 | 1.63 (1.03–2.56) | - |
| AZA + CPA+ GC vs. GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.21 (0.04–1.02) | 0.054 | - | 0/1 | 29/7 | 0.21 (0.04–1.02) | - |
| CIs vs. Others | ||||||||||
| MMF + CPA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.22 (0.78–1.89) | 0.38 | - | 0//1 | 82/40 | 1.22 (0.78–1.89) | 0.38 |
| TAC vs. Others | Karaaij, et al., 2016 [21] | F | RR | 1.48 (1.23–1.77) | <0.05 | 65% (0.021) | 2/5 | 693/- | 1.77 (1.31–2.38) | <0.001 |
| MMF + GC vs. TAC + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.02 (0.83–1.26) | 0.85 | 0% (0.59) | 0/3 | 273/135 | 0.95 (0.74–1.23) | 0.71 |
| TAC + GC vs. CPA + GC | Zhou, et al., 2019 [11] | F | RR | 2.41 (1.46–3.99) | 0.0006 | 0% (0.93) | 0/7 | 276/135 | 1.64 (0.65–4.14) | 0.20 |
| Biologic agents | ||||||||||
| Rituximab vs. Others | Zhong, et al., 2019 [22] | R | RR | 1.98 (0.90–4.39) | 0.09 | 68% (0.02) | 1/5 | 548/378 | 1.40 (0.53–3.75) | 0.16 |
| Rituximab + CPA vs. Rituximab | Tunnicliffe, et al., 2018 [5] | F | RR | 0.90 (0.16–5.13) | 0.91 | - | 0/1 | 19/9 | 0.90 (0.16–5.13) | 0.91 |
| Rituximab + MMF vs. MMF | Tunnicliffe, et al., 2018 [5] | F | RR | 0.86 (0.51–1.45) | 0.58 | - | 0/1 | 144/72 | 0.86 (0.51–1.45) | 0.58 |
| Abatacept + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | R | RR | 1.13 (0.74–1.71) | 0.57 | 0% (0.74) | 0/2 | 432/168 | 1.08 (0.66–1.77) | - |
| Laquinimod + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 1.55 (0.73–3.42) | 0.28 | - | 0/1 | 46/15 | 1.55 (0.70–3.42) | 0.28 |
| Orcrelizumab + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 1.07 (0.74–1.56) | 0.72 | - | 0/1 | 223/75 | 1.07 (0.74–1.56) | 0.72 |
| Sirukumab + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 0.93 (0.66–1.32) | 0.70 | - | 0/1 | 25/4 | 0.93 (0.66–1.32) | 0.70 |
| Others | ||||||||||
| GC vs. reduced GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.93 (0.39–2.23) | 0.87 | - | 0/1 | 81/39 | 0.93 (0.39–2.23) | 0.87 |
| GC + 2 IS vs. GC + 1 IS | Liu, et al., 2019 [23] | RR | 1.22 (1.09–1.35) | <0.001 | 30.5% (0.17) | 3/10 | 1432/622 | 1.32 (1.16–1.51) | <0.001 | |
| AZA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.95 (0.54–1.69) | 0.87 | 2% (0.31) | 0/2 | 37/19 | 0.91 (0.56–1.46) | - |
| Partial Remission | ||||||||||
| CPA vs. Others | ||||||||||
| MMF + TAC + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.00 (0.78–1.28) | 1.00 | 0% (1.00) | 0/2 | 402/201 | 1.00 (0.77–1.30) | - |
| AZA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.80 (0.67–4.81) | 0.24 | - | 0/1 | 59/38 | 1.80 (0.67–1.81) | 0.24 |
| MMF + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.02 (0.89–1.18) | 0.74 | 0% (0.96) | 0/9 | 868/441 | 1.06 (0.85–1.32) | - |
| TAC + GC vs. CPA + GC | Deng, et al., 2012 [24] | F | RR | 0.95 (0.68–1.33) | 0.78 | 0% (0.63) | 0/5 | 219/111 | 0.87 (0.52–1.48) | 0.20 |
| CNI + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.86 (0.61–1.26) | 0.48 | 0% (0.76) | 0/4 | 178/87 | 0.82 (0.50–1.36) | - |
| Low vs. High CPA | Tian, et al., 2017 [17] | F | RR | 1.08 (0.89–1.32) | 0.43 | 0% (0.92) | 0/3 | 411/220 | 1.12 (0.85–1.48) | 0.41 |
| MMF + GC vs. oral CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.07 (0.44–2.59) | 0.88 | - | 0/1 | 62/30 | 1.07 (0.44–2.59_ | 0.88 |
| Others | ||||||||||
| MMF + CPA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.03 (0.55–1.90) | 0.94 | - | 0/1 | 82/40 | 1.03 (0.55–1.90) | 0.94 |
| MMF + GC vs. TAC + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.83 (0.51–1.36) | 0.47 | 0% (0.66) | 0/2 | 190/94 | 0.78 (0.44–1.33) | - |
| MMF + Rituximab vs. MMF | Tunnicliffe, et al., 2018 [5] | F | RR | 2.00 (1.05–3.82) | 0.035 | - | 1/1 | 144/72 | 2.00 (1.05–3.82) | 0.035 |
| Rituximab + CPA vs. Rituximab | Tunnicliffe, et al., 2018 [5] | F | RR | 0.75 (0.35–1.62) | 0.47 | - | 0/1 | 19/9 | 0.75 (0.35–1.62) | 0.47 |
| Abatacept + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | R | RR | 0.88 (0.58–1.33) | 0.54 | 0% (0.80) | 0/2 | 432/168 | 0.92 (0.53–1.61) | - |
| Orcrelizumab + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 1.49 (0.82–2.49) | 0.13 | - | 0/1 | 223/75 | 1.49 (0.89–2.49) | 0.13 |
| GC vs. reduced GC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.33 (0.78–2.24) | 0.29 | - | 0/1 | 81/39 | 1.33 (0.78–2.24) | 0.29 |
| Comparison | Author, Year | Reported Summary Effect (95% CI) |
|---|---|---|
| CPA vs. Others | ||
| MMF + GC vs. Low CPA + GC | Bae, et al., 2019 [14] | 1.02 (0.51–2.02) * |
| MMF + GC vs. High CPA + GC | Bae, et al., 2019 [14] | 1.48 (0.99–2.44) * |
| MMF + CIs + GC vs. CPA + GC | Palmer, et al., 2017 [10] | 2.69 (1.74–4.76) |
| Low CPA + GC vs. CSA + GC | Singh, et al., 2016 [4] | 0.38 (0.38–0.76) *,† |
| High CPA + GC vs. CSA + GC | Singh, et al., 2016 [4] | 0.55 (0.55–0.87) *,† |
| Low CPA vs. TAC | Singh, et al., 2016 [4] | 0.50 (0.50–0.95) * |
| Low CPA vs. CPA | Singh, et al., 2016 [4] | 0.51 (0.51–0.95) |
| Oral CPA vs. CPA | Palmer, et al., 2017 [10] | 0.57 (0.23–1.40) |
| Mizoribine + GC vs. CPA + GC | Palmer, et al., 2017 [10] | 0.29 (0.08–1.11) |
| Other | ||
| CNI + GC vs. MMF + GC | Tang, et al., 2018 [25] | 1.0 (0.3–3.6) |
| Plasma exchange vs. CSA | Singh, et al., 2016 [4] | 0.49 (0.49–0.97) * |
| MMF +GC vs. GC | Tang, et al., 2018 [25] | 8.6 (1.4–51.6) |
| CNI + GC vs. GC | Tang, et al., 2018 [25] | 8.8 (1.6–48.2) |
| Comparison | Author, Year | M | Type of Metrics | Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|
| AZA vs. CSA | Tunnicliffe, et al., 2018 [5] | F | RR | 1.25 (0.51–3.06) | 0.63 | - | 0/1 | 69/36 | 1.25 (0.51–3.06) | 0.63 |
| AZA vs. TAC | Tunnicliffe, et al., 2018 [5] | F | RR | 6.62 (0.35–123.63) | 0.21 | - | 0/1 | 70/34 | 6.62 (0.35–123.63) | 0.21 |
| MMF + GC vs. oral CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.15 (0.55–2.37) | 0.71 | - | 0/1 | 62/30 | 1.15 (0.55–2.37) | 0.71 |
| GC withdrawal vs. GC continuous | Tunnicliffe, et al., 2018 [5] | R | RR | 0.38 (0.05–2.88) | 0.35 | - | 0/1 | 15/8 | 0.38 (0.05–2.88) | 0.35 |
| Comparison | Author, Year | Reported Summary Effect (95% CI) |
|---|---|---|
| MMF vs. AZA | Palmer, et al., 2017 [10] | 0.53 (0.31–0.90) |
| CPA vs. GC | Singh, et al., 2016 [4] | 0.31 (0.11–0.71) |
| Comparison | Author, Year | M | Ta | Reported Summary Effect (95% CI) | NMA Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) | NMA Author, Year |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MMF + CPA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.95 (0.06–14.72) | 0.92 (0.06–15.3) | 0.97 | - | 0//1 | 82/40 | 0.96 (0.06–14.72) | 0.97 | Palmer, et al., 2017 [10] |
| CNI + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.41 (0.06–2.69) | 0.83 (0.27–2.56) | 0.36 | 0% (0.79) | 0/3 | 153/75 | 0.29 (0.01–6.93) | 0.50 | Palmer, et al., 2017 [10] |
| CPA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.98 (0.53–1.82) | 2.03 (0.72–5.77) * | 0.94 | 10% (0.35) | 0/4 | 226/88 | 4.91 (0.66–36.40) | - | Palmer, et al., 2017 [10] |
| AZA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.39 (0.25–7.77) | 1.52 (0.52–4.46) | 0.71 | 67% (0.08) | 0/2 | 146/75 | 0.49 (0.09–2.81) | - | Palmer, et al., 2017 [10] |
| MMF + GC vs. CPA + GC | Henderson, et al., 2013 [15] | R | RR | 1.02 (0.52–1.98) | 4.20 (0.59–2.44) | 0.96 | 0% (0.54) | 0/4 | 710/349 | 1.02 (0.61–5.27) | 0.24 | Palmer, et al., 2017 [10] |
| Oral CPA vs. IV CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.80 (0.20–3.24) | 2.86 (0.82–10.0) | 0.76 | 34% (0.22) | 0/2 | 67/34 | 0.51 (0.18–1.47) | - | Palmer, et al., 2017 [10] |
| Comparison | Author, Year | M | Type of Metrics | Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|
| Induction therapy | ||||||||||
| CPA vs. Others | ||||||||||
| Low CPA vs. High CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.97 (0.14–6.56) | 0.98 | - | 0/2 | 121/63 | 0.97 (0.14–6.56) | - |
| CPA + AZA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.53 (0.17–1.68) | 0.28 | - | 0/1 | 29/7 | 0.53 (0.17–1.68) | 0.28 |
| CNI vs. Others | ||||||||||
| TAC vs. Others | J. Hannah, et al., 2016 [25] | F | RR | 0.39 (0.10–1.42) | 0.15 | 0% (1.00) | 0/5 | 153/75 | 0.29 (0.01–6.93) | 0.5 |
| MMF + GC vs. TAC + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.10 (0.44–2.77) | 0.84 | 0% (0.98) | 0/7 | 273/135 | 1.17 (0.37–3.66) | 1.00 |
| Biologic agents | ||||||||||
| Rituximab + MMF vs. MMF | Tunnicliffe, et al., 2018 [5] | F | RR | 5.00 (0.24–102.35) | 0.30 | - | 0/1 | 144/72 | 5.00 (0.24–102.35) | 0.30 |
| Belimumab vs. placebo | Kandala, et al., 2013 [27] | R | RR | 0.59 (0.16–2.11) | - | - | 0/3 | 2133/675 | - | - |
| Abatacept + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | R | RR | 0.29 (0.10–0.91) | 0.034 | 0% (0.92) | 1/2 | 432/168 | 0.29 (0.09–0.96) | - |
| Laquinimod + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 1.50 (0.06–34.79) | 0.80 | - | 0/1 | 46/15 | 1.50 (0.06–34.79) | 0.80 |
| Orcrelizumab + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 0.66 (0.23–1.85) | 0.43 | - | 0/1 | 379/125 | 0.66 (0.23–1.85) | 0.43 |
| Others | ||||||||||
| GC vs. reduced GC | Tunnicliffe, et al., 2018 [5] | F | RR | 4.65 (0.23–93.95) | 0.32 | - | 0/1 | 81/39 | 4.65 (0.23–93.95) | 0.32 |
| Plasma exchange + IS vs. IS | Tunnicliffe, et al., 2018 [5] | R | RR | 1.62 (0.64–4.09) | 0.31 | - | 0/2 | 125/65 | 1.53 (0.58–4.04) | - |
| AZA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.60 (0.36–0.99) | 0.048 | 0% (0.74) | 1/3 | 78/35 | 0.53 (0.29–0.99) | - |
| Maintenance therapy | ||||||||||
| MMF vs. AZA | Deng, et al., 2019 [18] | F | RR | 0.55 (0.23–1.28) | 0.16 | 0% (0.58) | 0/7 | 601/294 | 0.32 (0.01–7.82) | - |
| AZA vs. CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.12 (0.01–2.03) | 0.14 | - | 0/1 | 39/20 | 0.12 (0.01–2.03) | 0.14 |
| Comparison | Author, Year | M | T | Reported Summary Effect (95% CI) | NMA Author, Year | NMA Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MMF + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.71 (0.27–1.84) | Palmer, et al., 2017 [10] | 2.60 (0.36–18.7) | 0.48 | 0% (0.65) | 0/3 | 231/117 | 0.53 (0.15–1.81) | 0.31 |
| CNI + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.00 (0.07–14.85) | Palmer, et al., 2017 [10] | 2.08 (0.23–18.9) | 1.0 | - | 0/1 | 38/19 | 1.00 (0.07–14.85) | - |
| CPA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.63 (0.39–1.03) | Singh, et al., 2016 [16] | 0.56 (0.33–0.92) | 0.07 | 0% (0.87) | 0/4 | 278/107 | 0.74 (0.29–1.86) | - |
| AZA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.40 (0.15–1.07) | Palmer, et al., 2017 [10] | 1.79 (0.56–5.70) | 0.07 | 0% (0.76) | 0/2 | 144/56 | 0.25 (0.01–5.93) | - |
| Oral CPA vs. IV CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.23 (0.04–1.28) | Palmer, et al., 2017 [10] | 1.34 (0.31–5.88) | 0.09 | 0% (0.97) | 0/2 | 67/34 | 0.23 (0.03–1.83) | - |
| Comparison | Author, Year | M | Type of mETRICS | Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|
| Induction therapy | ||||||||||
| CPA vs. Others | ||||||||||
| MMF + GC vs. oral CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.19 (0.01–3.76) | 0.27 | - | 0/1 | 62/30 | 0.19 (0.01–3.76) | 0.27 |
| CPA + AZA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.21 (0.04–1.02) | 0.054 | - | 0/1 | 29/7 | 0.21 (0.04–1.02) | 0.054 |
| Low vs. High CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.49 (0.05–5.20) | 0.55 | - | 0/2 | 135/64 | 0.49 (0.05–5.20) | 0.55 |
| Long vs. Short CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.40 (0.09–1.83) | 0.24 | - | 0/1 | 40/20 | 0.40 (0.09–1.83) | 0.24 |
| CNs vs. Others | ||||||||||
| MMF + GC vs. TAC + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.22 (0.51–2.91) | 0.66 | - | 0/1 | 150/74 | 1.22 (0.51–2.91) | 0.66 |
| Biologic agents | ||||||||||
| Abatacept + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | R | RR | 0.84 (0.21–3.45) | 0.81 | - | 0/1 | 298/100 | 0.84 (0.21–3.45) | 0.81 |
| Others | ||||||||||
| GC vs. reduced GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.93 (0.39–2.23) | 0.87 | - | 0/1 | 81/39 | 0.93 (0.39–2.23) | 0.87 |
| AZA + GC vs. GC | Flanc, et al., 2004 [28] | R | RR | 0.66 (0.17–2.55) | 0.55 | 49.7% (0.16) | 0/2 | 54/22 | 0.33 (0.08–1.32) | - |
| Plasma exchange + IS vs. IS | Tunnicliffe, et al., 2018 [5] | R | RR | 1.24 (0.60–2.57) | 0.56 | 0% (0.63) | 0/3 | 143/74 | 1.44 (0.63–3.29) | - |
| Plasma exchange vs. IS | Tunnicliffe, et al., 2018 [5] | F | RR | 0.24 (0.01–4.44) | 0.34 | - | 0/1 | 20/11 | 0.24 (0.01–4.44) | 0.34 |
| Maintenance therapy | ||||||||||
| MMF vs. AZA | Deng, et al., 2019 [18] | F | RR | 0.50 (0.18–1.39) | 0.19 | 0% (0.74) | 0/5 | 514/252 | 0.14 (0.01–2.62) | 0.07 |
| AZA vs. CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.35 (0.04–3.09) | 0.35 | - | 0/1 | 39/20 | 0.35 (0.04–3.09) | 0.35 |
| Comparison | Author, Year | Reported Summary Effect (95% CI) |
|---|---|---|
| GC vs. CPA + GC | Palmer, et al., 2017 [10] | 2.40 (1.05–5.48) |
| CPA + AZA vs. GC | Singh, et al., 2016 [16] | 0.23 (0.07–0.64) |
| High GC vs. AZA + GC | Singh, et al., 2016 [16] | 2.15 (1.06–4.10) |
| High GC vs. MMF | Singh, et al., 2016 [16] | 4.54 (1.45–17.31) |
| High CPA + GC vs. High GC | Singh, et al., 2016 [16] | 0.24 (0.06–0.71) |
| Plasma exchange vs. CPA | Palmer, et al., 2017 [10] | 2.92 (0.31–27.8) |
| Comparison | Author, Year | M | Type of Metrics | Reported Summary Effect (95% CI) | NMA Author, Year | NMA Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MMF + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 1.02 (0.67–1.54) | Lee, et al., 2015 [12] | 0.87 (0.54–1.53) | 0.94 | 0% (0.50) | 0/9 | 699/351 | 1.22 (0.68–2.20) | - |
| TAC + GC vs. CPA + GC | Zhou, et al., 2019 [11] | F | OR | 0.77 (0.42–1.43) | Lee, et al., 2015 [12] | 0.49 (0.21–1.23) | 0.41 | - | 0/5 | - | - | - |
| CNI + GC vs. CPA + GC | Zhang, et al., 2016 [13] | F | RR | 0.65 (0.43–0.98) | Palmer, et al., 2017 [10] | 0.57 (0.28–1.16) | 0.04 | 0% (0.53) | 0/5 | 194/97 | 1.09 (0.32–3.73) | 0.9 |
| CPA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.87 (0.50–1.51) | Palmer, et al., 2017 [10] | 0.81 (0.34–1.94) * | 0.61 | 0% (0.59) | 0/6 | 291/113 | 1.12 (0.53–2.40) | - |
| Oral CPA vs. IV CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 1.16 (0.47–2.90) | Palmer, et al., 2017 [10] | 1.12 (0.43–2.94) | 0.75 | 0% (0.35) | 0/2 | 67/34 | 0.60 (0.11–3.19) | - |
| Low CPA vs. High CPA | Tian, et al., 2017 [17] | F | RR | 0.74 (0.56–0.98) | Bae, et al., 2019 [14] | 0.62 (0.29–1.25) | 0.03 | 20% (0.28) | 1/7 | 655/348 | 0.80 (0.47–1.35) | 0.39 |
| TAC + GC vs. MMF + GC | Zhou, et al., 2019 [11] | R | OR | 0.95 (0.06–16.03) | Lee, et al., 2015 [12] | 0.56 (0.24–1.30) | 0.97 | - | - | - | - | - |
| Comparison | Author, Year | M | Type of Metrics | Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|
| Induction therapy | ||||||||||
| CPA vs. Others | ||||||||||
| MMF + TAC + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.80 (0.22–2.94) | 0.74 | 57% (0.13) | 2/2 | 402/201 | 1.80 (1.34–2.42) | <0.001 |
| MMF + GC vs. Oral CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.38 (0.08–1.79) | 0.22 | - | 0/1 | 62/30 | 0.38 (0.08–1.79) | 0.22 |
| Long CPA vs. Short CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 1.00 (0.07–14.90) | 1.0 | - | 0/1 | 40/20 | 1.00 (0.07–14.90) | 1.0 |
| AZA + CPA+ GC vs. GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.48 (0.10–2.30) | 0.36 | - | 0/1 | 29/7 | 0.48 (0.10–2.30) | 0.36 |
| CNI vs. Others | ||||||||||
| TAC vs. Others | Karaaij, et al., 2016 [21] | F | RR | 0.91 (0.69–1.19) | - | 26.9% (0.242) | 0/5 | 693/- | 1.14 (0.81–1.60) | - |
| AZA vs. TAC | Tunnicliffe, et al., 2018 [5] | F | RR | 1.26 (0.30–5.22) | 0.75 | - | 0/1 | 70/34 | 1.26 (0.30–5.22) | 0.75 |
| MMF + GC vs. TAC + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 2.14 (0.93–4.92) | 0.60 | 0% (0.28) | 0/2 | 190/94 | 1.70 (0.52–5.58) | 0.53 |
| Biologic agents | ||||||||||
| Rituximab + CPA vs. Rituximab | Tunnicliffe, et al., 2018 [5] | F | RR | 0.09 (0.07–12.38) | 0.94 | - | 0/1 | 19/9 | 0.09 (0.07–12.38) | 0.94 |
| Rituximab + MMF vs. MMF | Tunnicliffe, et al., 2018 [5] | F | RR | 1.00 (0.48–2.08) | 1.0 | - | 0/1 | 144/72 | 1.0 (0.48–2.08) | 1.0 |
| Rituximab + IS vs. IS | Shamliyan, et al., 2017 [29] | F | RD | 0.03 (−0.03–0.08) | - | 0% (0.78) | 0/1 | - | 0.03 (−0.03–0.08) | - |
| Abatacept + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | R | RR | 1.29 (0.81–2.04) | 0.28 | 0% (0.62) | 0/2 | 432/168 | 1.22 (0.73–2.03) | - |
| Orcrelizumab + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 1.14 (0.95–1.36) | 0.17 | - | 0/1 | 378/125 | 1.14 (0.95–1.36) | 0.17 |
| Sirukumab + IS vs. placebo + IS | Tunnicliffe, et al., 2018 [5] | F | RR | 0.93 (0.66–1.32) | 0.70 | - | 0/1 | 25/4 | 0.93 (0.66–1.32) | 0.70 |
| Belimumab vs. placebo | Kandala, et al., 2013 [27] | R | RR | 0.85 (0.57–1.28) | - | - | 0/3 | 2133/675 | - | - |
| Others | ||||||||||
| MMF + CPA + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 0.37 (0.14–0.93) | 0.035 | - | 1/1 | 82/40 | 0.37 (0.14–0.93) | 0.035 |
| Plasma exchange + IS vs. IS | Tunnicliffe, et al., 2018 [5] | R | RR | 0.69 (0.35–1.37) | 0.29 | 0% (0.36) | 0/2 | 125/65 | 0.65 (0.32–1.30) | - |
| Plasma exchange vs. IS | Tunnicliffe, et al., 2018 [5] | F | RR | 0.40 (0.02–8.78) | 0.56 | - | 0/1 | 20/11 | 0.40 (0.02–8.78) | - |
| GC vs. reduced GC | Tunnicliffe, et al., 2018 [5] | F | RR | 4.64 (0.57–38.00) | 0.15 | - | 0/1 | 81/39 | 4.64 (0.57–38.00) | 0.15 |
| MMF vs. AZA | Deng, et al., 2019 [18] | R | RR | 0.61 (0.29–1.30) | 0.20 | 84% (0.0004) | 1/4 | 255/124 | 1.26 (0.88–1.79) | - |
| AZA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 3.56 (0.46–27.79) | 0.23 | 0% (0.59) | 0/2 | 42/16 | 2.00 (0.11–37.22) | - |
| Maintenance therapy | ||||||||||
| AZA vs. MMF | Tunnicliffe, et al., 2018 [5] | F | RR | 1.08 (0.60–1.96) | 0.79 | 0% (0.87) | 0/3 | 412/209 | 1.22 (0.57–2.62) | - |
| CNI vs. AZA | Zhang, et al., 2016 [13] | F | RR | 0.56 (0.28–1.10) | 0.09 | 0% (0.34) | 0/2 | 139/69 | 1.06 (0.23–4.89) | >0.99 |
| AZA vs. GC | Tunnicliffe, et al., 2018 [5] | F | RR | 2.18 (1.01–4.73) | 0.048 | - | 1/1 | 69/36 | 2.18 (1.01–4.73) | 0.048 |
| GC withdrawal vs. GC continuous | Tunnicliffe, et al., 2018 [5] | R | RR | 0.57 (0.06–5.03) | 0.61 | - | 0/1 | 15/8 | 0.57 (0.06–5.03) | 0.61 |
| Comparison | Author, Year | Reported Summary Effect (95% CI) |
|---|---|---|
| MMF + GC vs. CPA + GC | Palmer, et al., 2017 [10] | 1.23 (0.84–1.77) |
| MMF + CNI + GC vs. CPA + GC | Palmer, et al., 2017 [19] | 3.59 (0.66–19.5) |
| Low CPA + GC vs. MMF + GC | Bae SC, et al., 2019 [14] | 0.73 (0.29–1.66) |
| MMF + GC vs. High CPA + GC | Bae SC, et al., 2019 [14] | 0.85 (0.52–1.39) |
| AZA + GC vs. CPA + GC | Palmer, et al., 2017 [10] | 0.34 (0.10–1.13) |
| MMF + GC vs. GC | Tang, et al., 2018 [25] | 5.50 (1.00–30.1) |
| CNI + GC vs. GC | Tang, et al., 2018 [25] | 5.0 (1.1–22.6) |
| Comparison | Author, Year | M | Type of Metrics | Reported Summary Effect (95% CI) | NMA Author, Year | NMA Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MMF vs. AZA | Deng, et al., 2019 [18] | F | RR | 0.75 (0.54–1.05) | Singh, et al., 2016 [4] | 0.59 (0.38–0.90) | 0.09 | 0% (0.72) | 1/7 | 558/270 | 0.55 (0.31–0.99) | 0.03 |
| CNI vs. AZA | Zhang, et al., 2016 [13] | F | RR | 0.44 (0.10–1.89) | Palmer, et al., 2017 [10] | 0.64 (0.22–1.88) | 0.27 | 0% (0.54) | 0/2 | 139/69 | 0.64 (0.22–1.88) | 0.49 |
| AZA vs. CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 0.79 (0.34–1.85) | Palmer, et al., 2017 [10] | 1.68 (0.51–5.51) * | 0.59 | - | 0/1 | 39/20 | 0.79 (0.34–1.85) | 0.59 |
| Comparison | Author, Year | Reported Summary Effect (95% CI) |
|---|---|---|
| MMF + CNI + GC vs. CPA + GC | Palmer, et al., 2017 [10] | 1.00 (0.02–52.8) |
| Plasma exchange + GC vs. CPA +GC | Palmer, et al., 2017 [10] | 8.21 (0.22–3.04) |
| Comparison | Author, Year | M | Type of Metrics | Reported Summary Effect (95% CI) | Reported p Value | I2 (p Value) | No. of Significant Study/Total Study | No. of Cases/Controls | Largest Effect (95% CI) | p Value (Largest) |
|---|---|---|---|---|---|---|---|---|---|---|
| Induction therapy | ||||||||||
| MMF + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.65 (0.11–3.86) | 0.64 | - | 0/1 | 364/180 | 0.65 (0.11–3.86) | 0.64 |
| CPA + GC vs. GC | Tunnicliffe, et al., 2018 [5] | R | RR | 0.82 (0.07–9.90) | 0.87 | 26% (0.24) | 0/2 | 147/39 | 2.69 (0.15–49.06) | - |
| CNI + GC vs. CPA + GC | Tunnicliffe, et al., 2018 [5] | F | RR | 5.00 (0.26–97.70) | 0.29 | - | 0/1 | 38/19 | 5.00 (0.26–97.70) | - |
| Low vs. High CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 1.44 (0.09–23.31) | 0.80 | 41% (0.19) | 0/2 | 206/88 | 5.47 (0.30–99.28) | - |
| Long vs. Short CPA | Tunnicliffe, et al., 2018 [5] | R | RR | 3.00 (0.13–69.52) | 0.49 | - | 0/1 | 40/20 | 3.00 (0.13–69.52) | 0.49 |
| Belimumab * vs. placebo | Borba, et al., 2014 [30] | R | RR | 1.50 (0.25–9.17) | 0.66 | 0% (0.71) | 0/3 | 1349/674 | 2.01 (0.18–22.09) | - |
| Maintenance therapy | ||||||||||
| AZA vs. MMF | Tunnicliffe, et al., 2018 [5] | F | RR | 4.04 (0.45–36.07) | 0.21 | 0% (0.82) | 0/3 | 370/188 | 3.11 (0.13–75.47) | - |
| Comparison | Author, Year | Reported Summary Effect (95% CI) |
|---|---|---|
| AZA + GC vs. CPA + GC | Palmer, et al., 2017 [10] | 4.67 (0.61–37.7) |
| Oral CPA + GC vs. IV CPA + GC | Palmer, et al., 2017 [10] | 7.77 (0.81–74.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, J.I.; Li, H.; Park, S.; Yang, J.W.; Lee, K.H.; Jo, Y.; Park, S.; Oh, J.; Kim, H.; An, H.J.; et al. Induction and Maintenance Treatment of Lupus Nephritis: A Comprehensive Review of Meta-Analyses. J. Clin. Med. 2022, 11, 343. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020343
Shin JI, Li H, Park S, Yang JW, Lee KH, Jo Y, Park S, Oh J, Kim H, An HJ, et al. Induction and Maintenance Treatment of Lupus Nephritis: A Comprehensive Review of Meta-Analyses. Journal of Clinical Medicine. 2022; 11(2):343. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020343
Chicago/Turabian StyleShin, Jae Il, Han Li, Seoyeon Park, Jae Won Yang, Keum Hwa Lee, Yongsuk Jo, Seongeun Park, Jungmin Oh, Hansol Kim, Hyo Jin An, and et al. 2022. "Induction and Maintenance Treatment of Lupus Nephritis: A Comprehensive Review of Meta-Analyses" Journal of Clinical Medicine 11, no. 2: 343. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020343