
The Impact of the COVID-19 Outbreak on Patients’ Adherence to PCSK9 Inhibitors Therapy

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
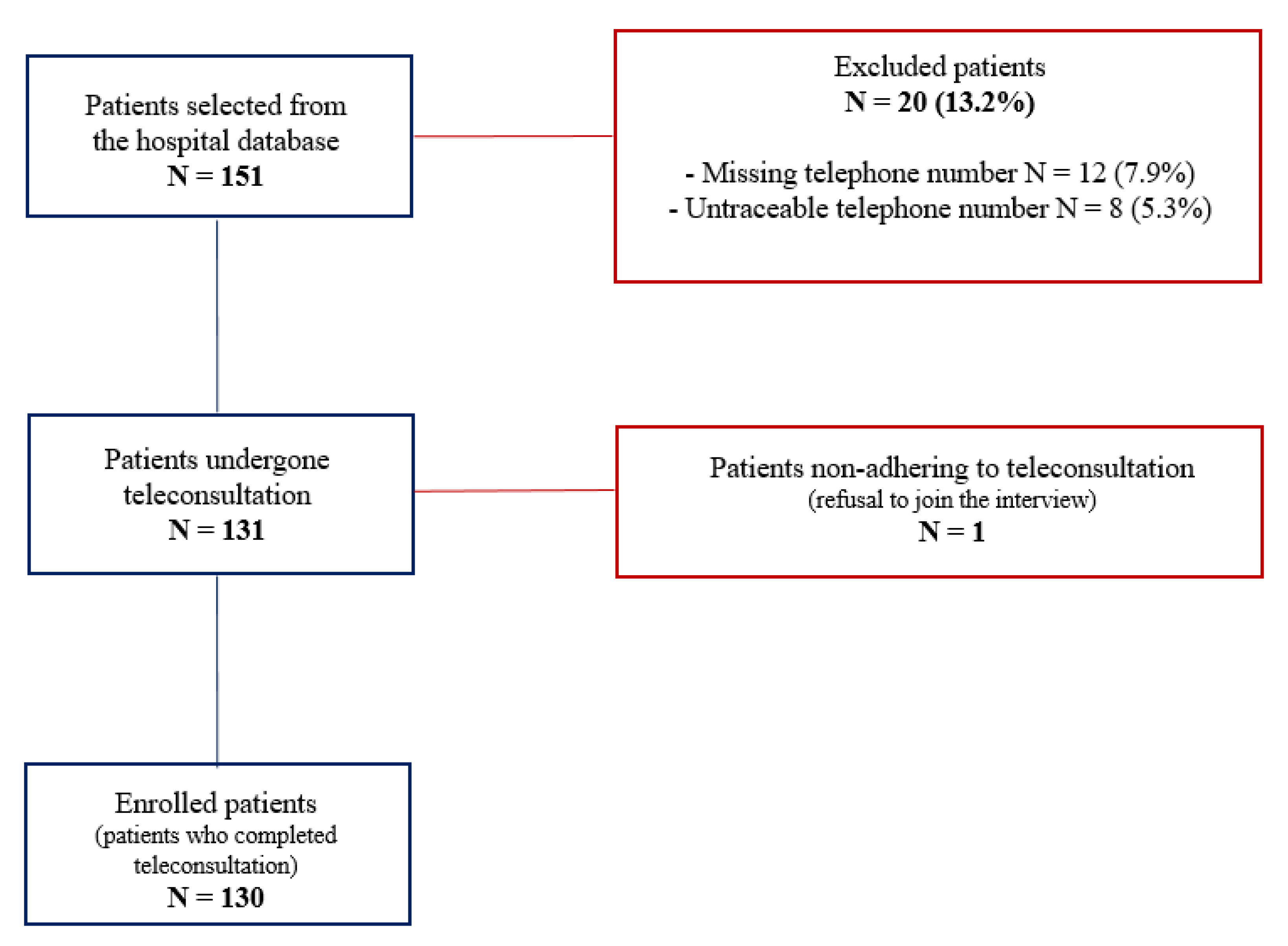
2.1. Study Design and Study Population
2.2. Teleconsultation and Data Collection
2.3. Primary and Secondary Outcomes
2.4. Satistical Analysis
2.5. Ethics Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Concomitant Lipid Lowering Drugs | N (%) |
|---|---|
| Ezetimibe 10 mg, n (%) | 15 (11.5) |
| Atorvastatin 40 mg, n (%) | 14 (10.8) |
| Rosuvastatin 40 mg, n (%) | 6 (4.6) |
| Rosuvastatin 20 mg, n (%) | 15 (11.5) |
| Rosuvastatin 10 mg, n (%) | 2 (1.5) |
| Atorvastatin 20 mg + Ezetimibe 10 mg, n (%) | 10 (7.7) |
| Atorvastatin 40 mg + Ezetimibe 10 mg, n (%) | 20 (15.4) |
| Simvastatin 20 mg + Ezetimibe 10 mg, n (%) | 8 (6.2) |
| Simvastatin 40 mg + Ezetimibe 10 mg, n (%) | 12 (9.2) |
| Rosuvastatin 10 mg + Ezetimibe 10 mg, n (%) | 5 (3.8) |
| Rosuvastatin 20 mg + Ezetimibe 10 mg, n (%) | 8 (6.2) |
| Concomitant Drugs | N (%) |
|---|---|
| Beta-blockers | |
| - Bisoprolol | 53 (40.8) |
| - Nebivolol | 7 (5.4) |
| - Metoprolol | 6 (4.6) |
| - Carvedilol | 5 (3.8) |
| - Atenolol | 3 (2.3) |
| Antiplatelet agents | |
| - Acetylsalicylic acid | 49 (37.7) |
| - Clopidogrel | 9 (6.9) |
| - Ticagrerol | 13 (10) |
| - Clopidogrel + acetylsalicylic acid | 19 (14.6) |
| ACE- inhibitors | |
| - Ramipril | 30 (23.1) |
| - Lisinopril | 6 (4.6) |
| - Enalapril | 5 (3.8) |
| Angiotensin II receptor-blockers | |
| - Losartan | 9 (6.9) |
| - Olmesartan | 11 (8.5) |
| - Telmisartan | 7 (5.4) |
| - Valsartan | 6 (4.6) |
| Calcium channel-blockers | |
| - Amlodipine | 14 (10.8) |
| - Lercandipine | 1 (0.8) |
| Diuretics | |
| - Thiazide diuretics | 17 (13) |
| - Loop diuretics | 14 (10.8) |
| - Potassium sparing diuretics | 2 (1.5) |
| - Carbonic anhydrase inhibitors | 1 (0.8) |
| - Osmotic diuretics | 9 (6.9) |
| Non-vitamin K oral anticoagulants | |
| - Apixaban | 3 (2.3) |
| - Rivaroxaban | 2 (1.5) |
| - Dabigatran | 1 (0.8) |
| Class III antiarrhythmics | |
| - Amiodarone | 6 (4.6) |
| Oral antidiabetics | |
| - Biguanide | 8 (6.1) |
| - Sulfonylureas | 2 (1.5) |
| Insulin | 6 (4.6) |
| Alpha-blockers | |
| - Doxazosine | 5 (3.8) |
| Antianginal agents | |
| - Ranolazine | 7 (5.4) |
| Antigout drugs | |
| - Febuxostat | 5 (3.8) |
| Glucocorticoids | |
| - Prednisolone | 1 (0.8) |
| Levothyroxine | 6 (4.6) |
| Heparin | 1 (0.8) |
| Antiepileptic drugs | 1 (0.8) |
| Proton pump inhibitors | |
| - Omeprazole | 14 (10.8) |
| - Pantoprazole | 44 (33.8) |
| - Esomeprazole | 3 (2.3) |
| - Lansoprazole | 1 (0.8) |
| - Rabeprazole | 2 (1.5) |
References
- Hui, D.; Azhar, E.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; McHugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [Green Version]
- Russo, V.; Bottino, R.; Carbone, A.; Rago, A.; Papa, A.A.; Golino, P.; Nigro, G. COVID-19 and Heart: From Clinical Features to Pharmacological Implications. J. Clin. Med. 2020, 9, 1944. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Piccinocchi, G.; Mandaliti, V.; Annunziata, S.; Cimmino, G.; Attena, E.; Moio, N.; Di Micco, P.; Severino, S.; Trotta, R.; et al. Cardiovascular Comorbidities and Pharmacological Treatments of COVID-19 Patients Not Requiring Hospitalization. Int. J. Environ. Res. Public Health 2020, 18, 102. [Google Scholar] [CrossRef]
- Available online: www.gazzettaufficiale.it/eli/id/2020/03/09/20A01558/sg (accessed on 15 November 2021).
- Russo, V.; Pafundi, P.C.; Rapacciuolo, A.; D’andrea, A.; de Devitiis, M.; Volpicelli, M.; Ruocco, A.; Nigro, G.; D’onofrio, A. Arrhythmogenic syncope leading to cardiac rhythm management procedures during COVID-19 lockdown. Expert Rev. Med. Devices 2020, 17, 1207–1210. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Pafundi, P.C.; Rapacciuolo, A.; de Divitiis, M.; Volpicelli, M.; Ruocco, A.; Rago, A.; Uran, C.; Nappi, F.; Attena, E.; et al. Cardiac pacing procedures during coronavirus disease 2019 lockdown in Southern Italy. J. Cardiovasc. Med. 2021, 22, 857–859. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- Russo, V.; Boggian, G.; Bolognesi, M.G.; Carretta, D.M.; Cencetti, S.; De Laura, D.; Hrovatin, E.; Pastori, P.; Tomaselli, C.; Parente, E.; et al. The Impact of COVID-19 Outbreak on Syncope Units Activities in Italy: A Report from the Italian Multidisciplinary Working Group on Syncope (GIMSI). Int. J. Environ. Res. Public Health 2021, 18, 9194. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Leiter, L.; Wiviott, S.D.; Giugliano, R.; Deedwania, P.; De Ferrari, G.M.; Murphy, S.; Kuder, J.F.; Gouni-Berthold, I.; Lewis, B.S.; et al. Cardiovascular safety and efficacy of the PCSK9 inhibitor evolocumab in patients with and without diabetes and the effect of evolocumab on glycaemia and risk of new-onset diabetes: A prespecified analysis of the FOURIER randomised controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 941–950. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Mach, F.; Zavitz, K.; Kurtz, C.; Narimon, H.; Kanevsky, E.; Schneider, J.; Wang, H.; Keech, A.; Pedersen, T.R.; et al. Cognitive Function in a Randomized Trial of Evolocumab. N. Engl. J. Med. 2017, 377, 633–643. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170 000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef] [Green Version]
- Hsia, J.; MacFadyen, J.G.; Monyak, J.; Ridker, P.M. Cardiovascular event reduction and adverse events among subjects attaining low-density lipoprotein cholesterol <50 mg/dL with rosuvastatin. The JUPITER trial (Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin). J. Am. Coll. Cardiol. 2011, 57, 1666–1675. [Google Scholar] [CrossRef] [Green Version]
- McCormack, T.; Dent, R.; Blagden, M. Very low LDL-C levels may safely provide additional clinical cardiovascular benefit: The evidence to date. Int. J. Clin. Pract. 2016, 70, 886–897. [Google Scholar] [CrossRef] [Green Version]
- Sperber, C.M.; Samarasinghe, S.R.; Lomax, G.P. An upper and lower bound of the Medication Possession Ratio. Patient Prefer. Adherence 2017, 11, 1469–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef] [Green Version]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective me-ta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 12671278. [Google Scholar]
- Gragnano, F.; Natale, F.; Concilio, C.; Fimiani, F.; Cesaro, A.; Sperlongano, S.; Crisci, M.; Limongelli, G.; Calabrò, R.; Russo, M.; et al. Adherence to proprotein convertase subtilisin/kexin 9 inhibitors in high cardiovascular risk patients. J. Cardiovasc. Med. 2018, 19, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.aifa.gov.it/registri-farmaci-sottoposti-a-monitoraggio (accessed on 15 November 2021).
- Russo, V.; Cassini, R.; Caso, V.; Donno, C.; Laezza, A.; Naddei, M.; Fiorelli, A.; Golino, P.; Nigro, G. Nursing Teleconsultation for the Outpatient Management of Patients with Cardiovascular Disease during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2087. [Google Scholar] [CrossRef]
- Russo, V.; Rapacciuolo, A.; Pafundi, P.C.; de Divitiis, M.; Volpicelli, M.; Ruocco, A.; Rago, A.; Uran, C.; Nappi, F.; Attena, E.; et al. Cardiac implantable electronic devices replacements in patients followed by remote monitoring during COVID-19 lockdown. Eur. Heart J.—Digit. Health 2021, 2, 171–174. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Wang, Y.; Zhang, M.; Gittell, J.H.; Jiang, S.; Chen, B.; Cui, F.; He, X.; Zhao, J.; Wang, X. From isolation to coordination: How can telemedicine help combat the COVID-19 outbreak? MedRxiv 2020. [Google Scholar] [CrossRef]



| Variables | Overall Population (n = 130) | Adherent Group (n = 119) | Non-Adherent Group (n = 11) | p-Value |
|---|---|---|---|---|
| Age (years), mean ± SD | 63.5 ± 9.3 | 68 ± 4.5 | 61.3 ± 5.9 | <0.001 |
| Male, n (%) | 89 (68.5) | 84 (70.6) | 6 (54.5) | 0.3 |
| Smokers, n (%) | 24 (18.5) | 77 (64.7) | 11(100) | 0.01 |
| Hypertension, n (%) | 88 (67.7) | 18 (15.1) | 6 (54.5) | <0.001 |
| Obesity, n (%) | 4 (3.1) | 3 (2.5) | 1 (9.1) | 0.2 |
| Familial hypercholesterolemia, n (%) | 15 (11.5) | 14 (11.8) | 1 (9.1) | 0.8 |
| Diabetes mellitus type 2, n (%) | 21 (16.1) | 1 (0.8) | 0 (0) | 0.8 |
| Coronary artery disease, n (%) | 102 (78.5) | 93 (78.1) | 9 (81.8) | 0.8 |
| Stroke, n (%) | 1 (0.8) | 20 (16.8) | 1 (9.1) | 0.5 |
| Peripheral arterial disease, n (%) | 35 (26.9) | 34 (28.6) | 1 (9.1) | 0.2 |
| Atrial fibrillation, n (%) | 2 (1.5) | 2 (1.7) | 0 (0) | 0.7 |
| Carotid atherosclerosis, n (%) | 10 (7.7) | 9 (7.6) | 1 (9.1) | 0.8 |
| Chronic obstructive pulmonary disease, n (%) | 4 (3.1) | 3 (2.5) | 1 (9.1) | 0.2 |
| High risk, n (%) | 53 (40.8) | 51 (42.8) | 2 (18.1) | 0.11 |
| Very high risk, n (%) | 49 (37.7) | 40 (33.6) | 9 (81.8) | <0.001 |
| Moderate risk, n (%) | 28 (21.5) | 28 (23.5) | 0 | 0.07 |
| Patients on LDL-C target, n (%) | 123 (94.6) | 112 (94.1) | 11 (100) | 0.4 |
| Beta blockers, n (%) | 74 (56.9) | 63 (52.9) | 11 (100) | 0.003 |
| Antiplatelet drugs, n (%) | 90 (69.2) | 80 (67.2) | 10 (90.9) | 0.1 |
| ACE inhibitors, n (%) | 41 (31.5) | 38 (31.9) | 3 (27.3) | 0.7 |
| Angiotensin II receptor blockers, n (%) | 33 (25.4) | 32 (26.9) | 1 (9.1) | 0.2 |
| Calcium channel blockers, n (%) | 15 (11.5) | 14 (11.8) | 1 (9.1) | 0.8 |
| Diuretics, n (%) | 43 (33.1) | 37 (31.1) | 6 (54.5) | 0.1 |
| Non-vitamin K antagonist oral anticoagulants n (%) | 6 (4.6) | 5 (4.2) | 1 (9.1) | 0.5 |
| Class III antiarrhythmics, n (%) | 6 (4.6) | 6 (5.04) | 0 (0) | 0.4 |
| Insulin, n (%) | 6 (4.6) | 6 (5.04) | 0 (0) | 0.4 |
| Alpha blockers, n (%) | 5 (3.8) | 5 (4.2) | 0 (0) | 0.9 |
| Antianginal drugs, n (%) | 7 (5.4) | 6 (5.04) | 1 (9.1) | 0.6 |
| Antigout drugs, n (%) | 5 (3.8) | 5 (4.2) | 0 (0) | 0.5 |
| Glucocorticoids, n (%) | 1 (0.8) | 1(0.8) | 0 (0) | 0.8 |
| Levothyroxine, n (%) | 6 (4.6) | 6 (5.04) | 0 (0) | 0.4 |
| Heparin, n (%) | 1 (0.8) | 1 (0.8) | 0 (0) | 0.8 |
| Antiepileptic drugs, n (%) | 1 (0.8) | 1 (0.8) | 0 (0) | 0.8 |
| Proton pump inhibitors, n (%) | 64 (49.2) | 54 (45.4) | 10 (91) | 0.004 |
| Statins, n (%) | 100 (76.9) | 90 (75.6) | 10 (91) | <0.001 |
| Ezetimibe, n (%) | 78 (60) | 67 (56.3) | 11 (100) | 0.005 |
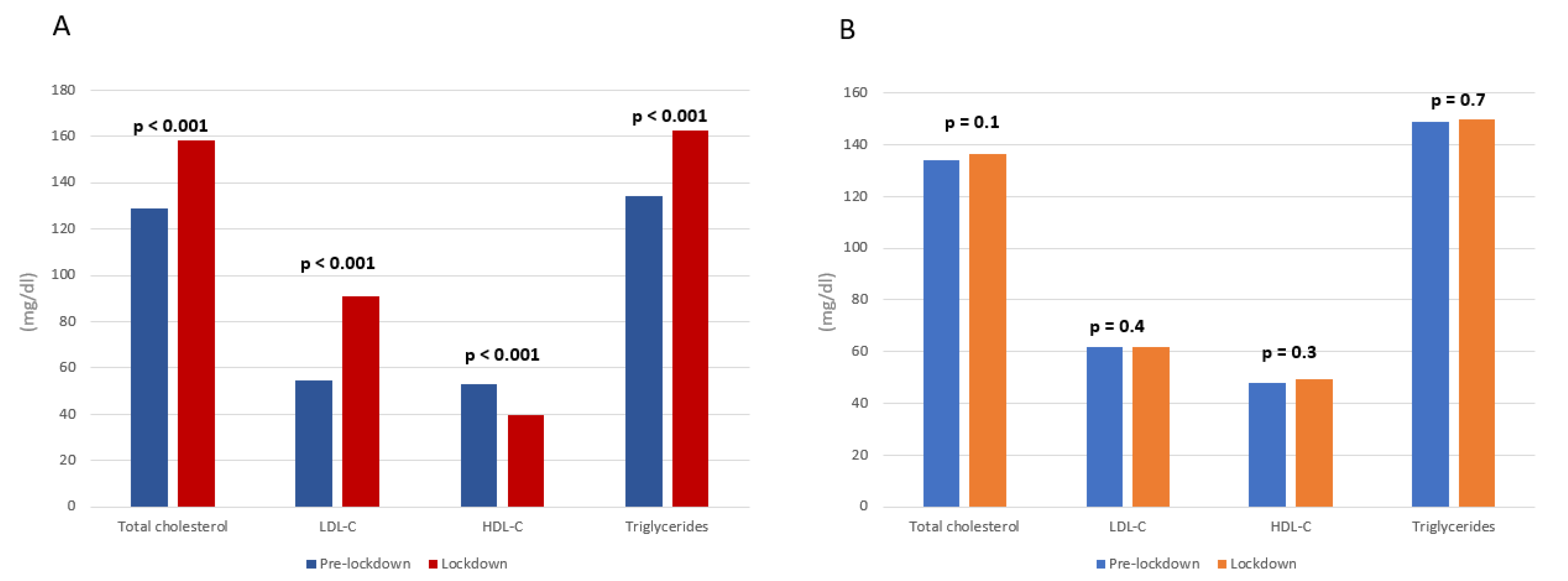
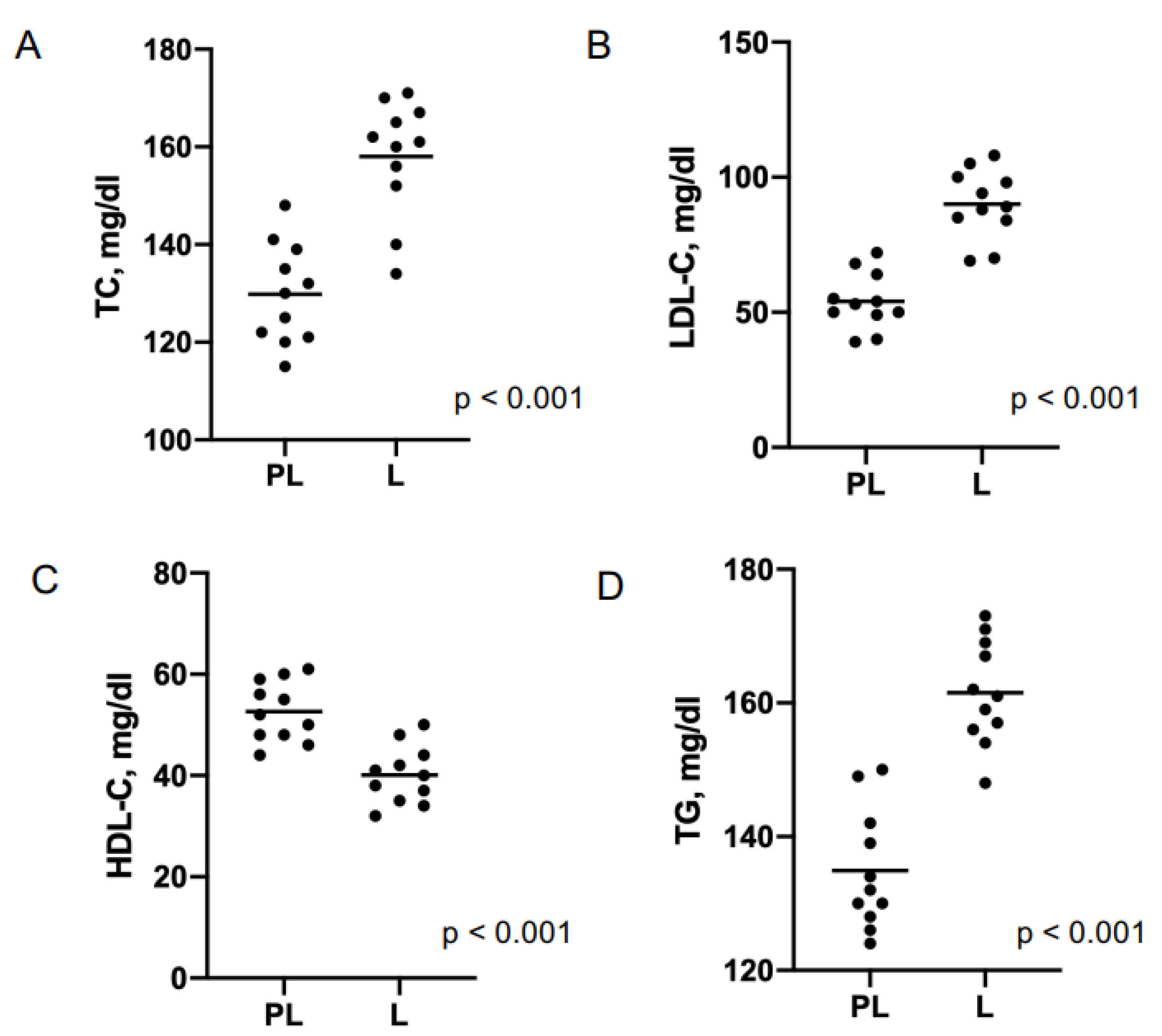
| Lipid, mg/dL | Pre-Lockdown | Lockdown | p-Value | |
|---|---|---|---|---|
| Adherent group (n = 119) | Total cholesterol | 134 ± 12 | 136.5 ± 14 | 0.1 |
| LDL-cholesterol | 61.6. ± 3.2 | 62 ± 3.6 | 0.4 | |
| HDL-cholesterol | 47.8 ± 12.1 | 49.3 ± 12.4 | 0.3 | |
| Triglycerides | 149 ± 21.9 | 150 ± 22 | 0.7 | |
| Non-adherent group (n = 11) | Total cholesterol | 129 ± 9.8 | 158.2 ± 11.4 | <0.0001 |
| LDL-cholesterol | 54.4 ± 7.7 | 90.8 ± 6.02 | <0.0001 | |
| HDL-cholesterol | 52.8 ± 5 | 39.8 ± 4.7 | <0.0001 | |
| Triglycerides | 134 ± 8.8 | 162.3 ± 7 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caso, V.M.; Sperlongano, S.; Liccardo, B.; Romeo, E.; Padula, S.; Arenga, F.; D’Andrea, A.; Caso, P.; Golino, P.; Nigro, G.; et al. The Impact of the COVID-19 Outbreak on Patients’ Adherence to PCSK9 Inhibitors Therapy. J. Clin. Med. 2022, 11, 475. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030475
Caso VM, Sperlongano S, Liccardo B, Romeo E, Padula S, Arenga F, D’Andrea A, Caso P, Golino P, Nigro G, et al. The Impact of the COVID-19 Outbreak on Patients’ Adherence to PCSK9 Inhibitors Therapy. Journal of Clinical Medicine. 2022; 11(3):475. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030475
Chicago/Turabian StyleCaso, Valentina Maria, Simona Sperlongano, Biagio Liccardo, Emanuele Romeo, Sergio Padula, Fortunato Arenga, Antonello D’Andrea, Pio Caso, Paolo Golino, Gerardo Nigro, and et al. 2022. "The Impact of the COVID-19 Outbreak on Patients’ Adherence to PCSK9 Inhibitors Therapy" Journal of Clinical Medicine 11, no. 3: 475. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030475