
Could Total Neoadjuvant Therapy Followed by Surgical Resection Be the New Standard of Care in Pancreatic Cancer? A Systematic Review and Meta-Analysis

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection Criteria and Outcome Measures
2.4. Data Extraction
2.5. Quality Assessment of Retrieved Articles
2.6. Statistical Analysis
3. Results
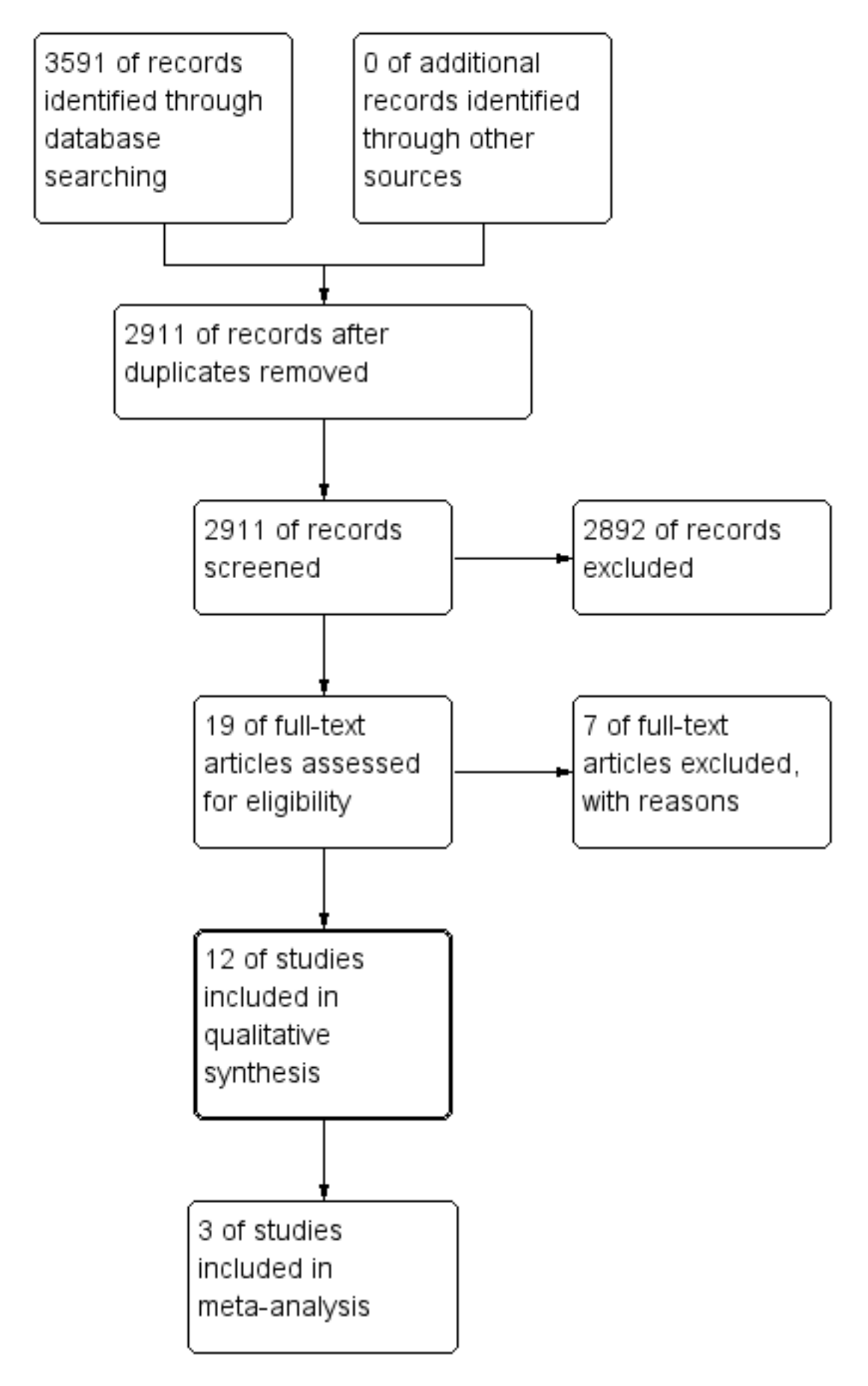
3.1. Study Selection
3.2. Study Characteristics and Patients Characteristics
3.3. Response and Tolerance to TNT
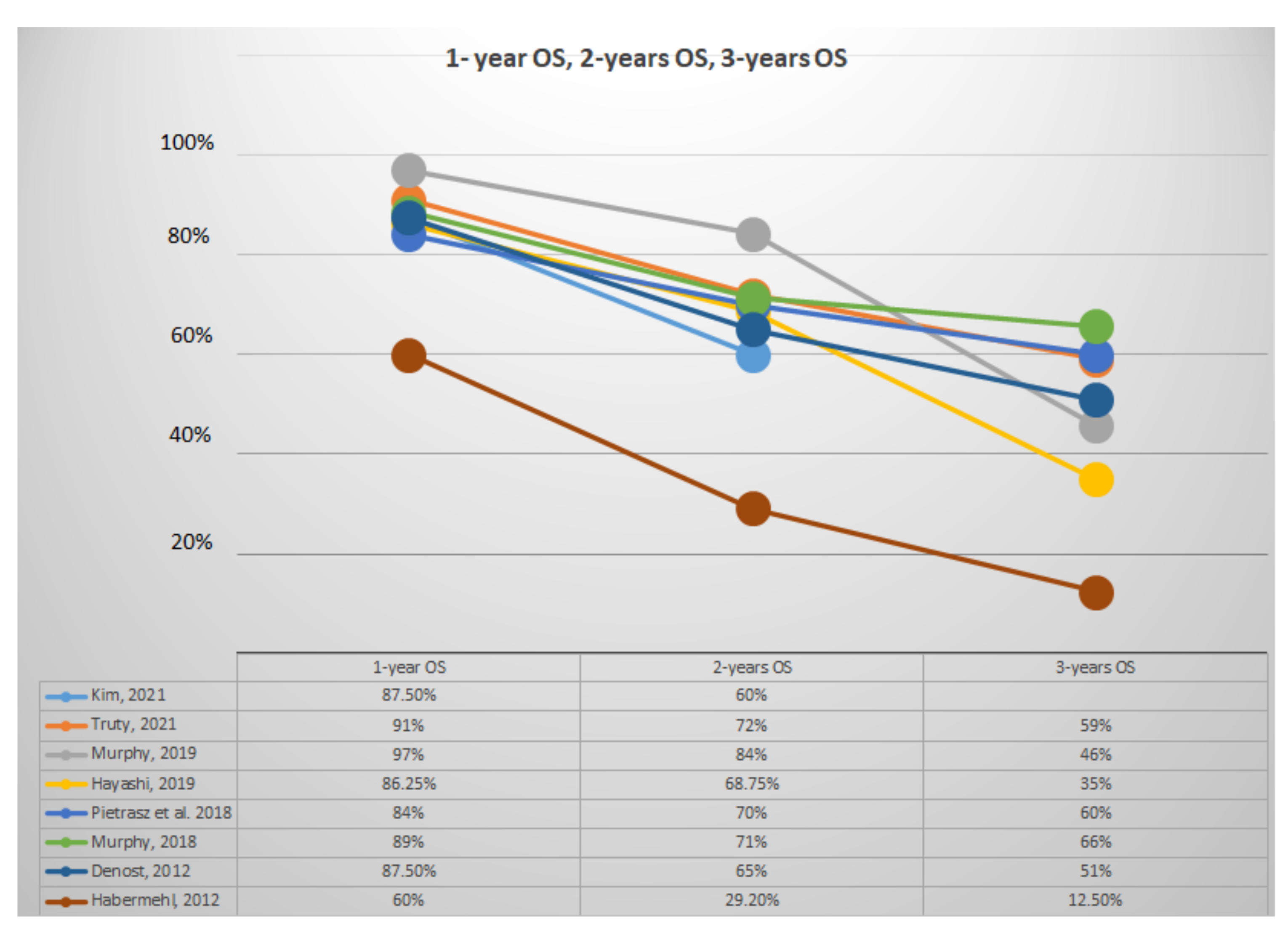
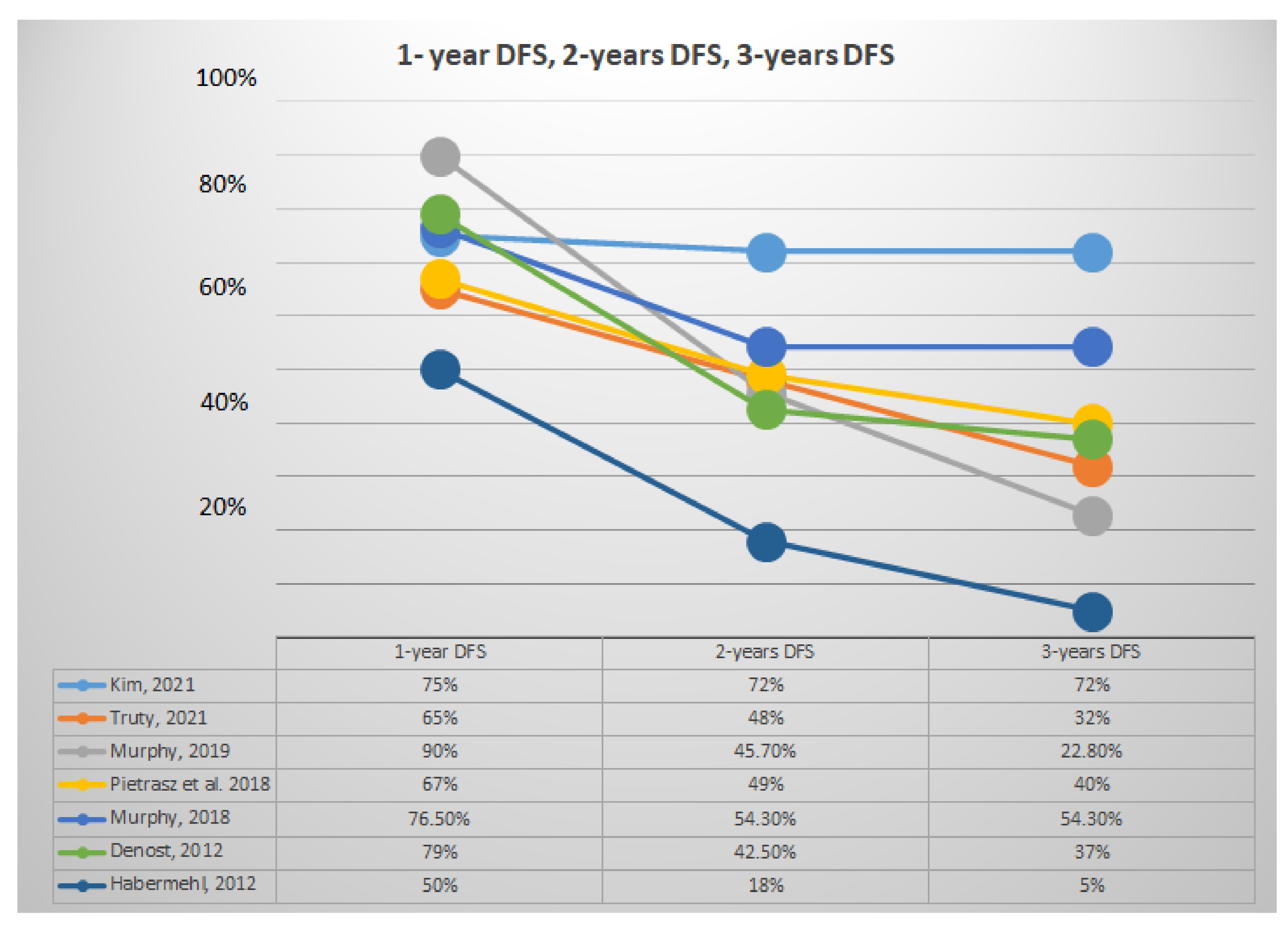
3.4. Pathological, Surgical and Survival Outcomes
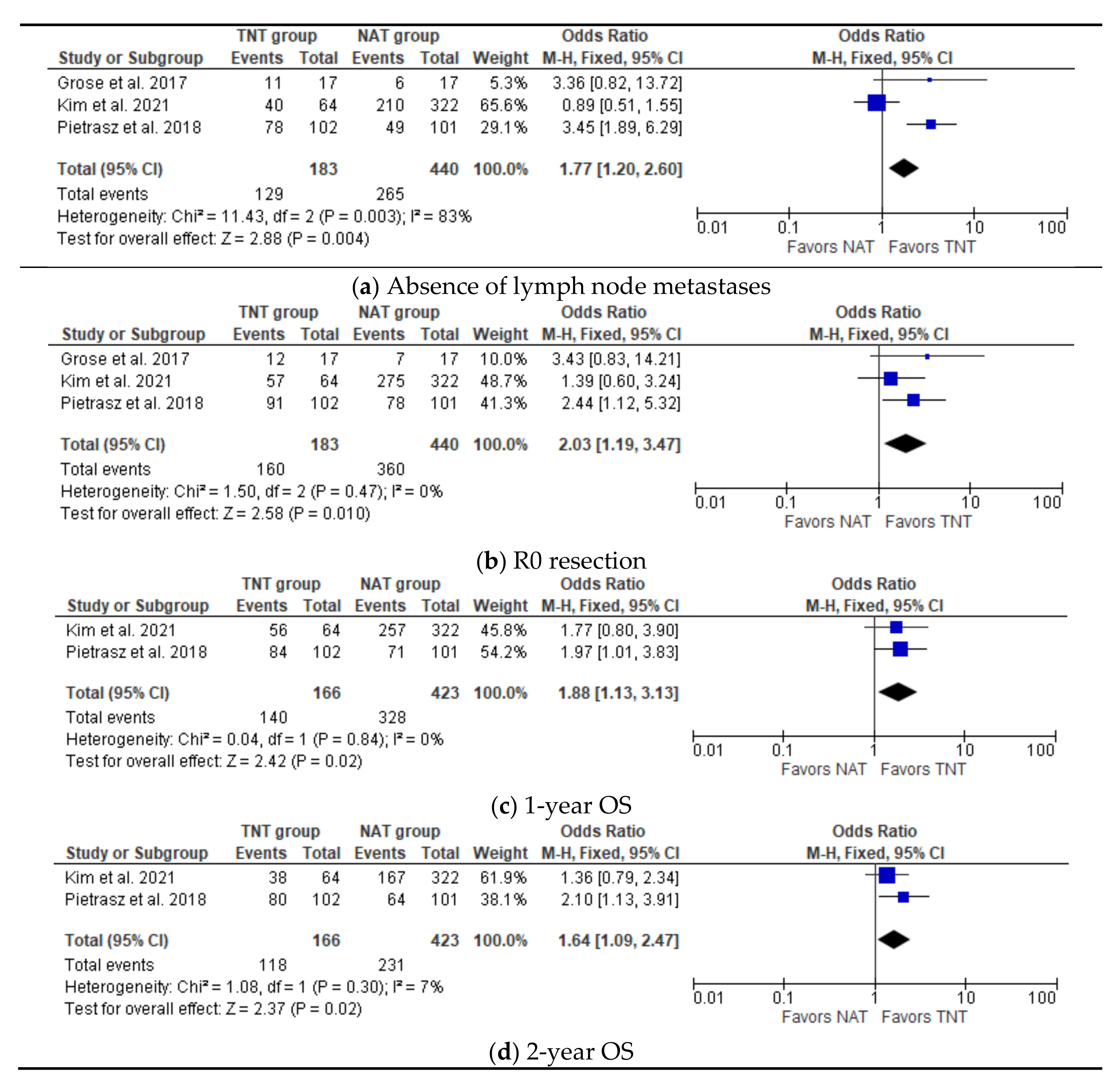
3.5. Meta-Analysis: Pathological and Survival outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review, 1975–2013; National Cancer Institute: Bethesda, MD, USA, 2016. [Google Scholar]
- Hartwig, W.; Werner, J.; Jäger, D.; Debus, J.; Büchler, M.W. Improvement of Surgical Results for Pancreatic Cancer. Lancet Oncol. 2013, 14, e476–e485. [Google Scholar] [CrossRef]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic Cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef] [PubMed]
- Conlon, K.C.; Klimstra, D.S.; Brennan, M.F. Long-Term Survival after Curative Resection for Pancreatic Ductal Adenocarcinoma. Clinicopathologic Analysis of 5-Year Survivors. Ann. Surg. 1996, 223, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Chua, Y.J.; Cunningham, D. Adjuvant Treatment for Resectable Pancreatic Cancer. J. Clin. Oncol. 2005, 23, 4532–4537. [Google Scholar] [CrossRef] [PubMed]
- Gillen, S.; Schuster, T.; Meyer zum Büschenfelde, C.; Friess, H.; Kleeff, J. Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-Analysis of Response and Resection Percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gemenetzis, G.; Groot, V.P.; Blair, A.B.; Laheru, D.A.; Zheng, L.; Narang, A.K.; Fishman, E.K.; Hruban, R.H.; Yu, J.; Burkhart, R.A.; et al. Survival in Locally Advanced Pancreatic Cancer After Neoadjuvant Therapy and Surgical Resection. Ann. Surg. 2019, 270, 340–347. [Google Scholar] [CrossRef]
- Hackert, T.; Sachsenmaier, M.; Hinz, U.; Schneider, L.; Michalski, C.W.; Springfeld, C.; Strobel, O.; Jäger, D.; Ulrich, A.; Büchler, M.W. Locally Advanced Pancreatic Cancer: Neoadjuvant Therapy with Folfirinox Results in Resectability in 60% of the Patients. Ann. Surg. 2016, 264, 457–463. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Marchegiani, G.; Hong, T.S.; Ryan, D.P.; Deshpande, V.; McDonnell, E.I.; Sabbatino, F.; Santos, D.D.; Allen, J.N.; Blaszkowsky, L.S.; et al. Radiological and Surgical Implications of Neoadjuvant Treatment with FOLFIRINOX for Locally Advanced and Borderline Resectable Pancreatic Cancer. Ann. Surg. 2015, 261, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Miyasaka, Y.; Ohtsuka, T.; Kimura, R.; Matsuda, R.; Mori, Y.; Nakata, K.; Kakihara, D.; Fujimori, N.; Ohno, T.; Oda, Y.; et al. Neoadjuvant Chemotherapy with Gemcitabine Plus Nab-Paclitaxel for Borderline Resectable Pancreatic Cancer Potentially Improves Survival and Facilitates Surgery. Ann. Surg. Oncol. 2019, 26, 1528–1534. [Google Scholar] [CrossRef]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.-J.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Tang, K.; Lu, W.; Qin, W.; Wu, Y. Neoadjuvant Therapy for Patients with Borderline Resectable Pancreatic Cancer: A Systematic Review and Meta-Analysis of Response and Resection Percentages. Pancreatology 2016, 16, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Turpin, A.; El Amrani, M.; Bachet, J.-B.; Pietrasz, D.; Schwarz, L.; Hammel, P. Adjuvant Pancreatic Cancer Management: Towards New Perspectives in 2021. Cancers 2020, 12, E3866. [Google Scholar] [CrossRef] [PubMed]
- Pietrasz, D.; Turrini, O.; Vendrely, V.; Simon, J.-M.; Hentic, O.; Coriat, R.; Portales, F.; Le Roy, B.; Taieb, J.; Regenet, N.; et al. How Does Chemoradiotherapy Following Induction FOLFIRINOX Improve the Results in Resected Borderline or Locally Advanced Pancreatic Adenocarcinoma? An AGEO-FRENCH Multicentric Cohort. Ann. Surg. Oncol. 2019, 26, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Hammel, P.; Huguet, F.; van Laethem, J.-L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouché, O.; Shannon, J.; André, T.; et al. Effect of Chemoradiotherapy vs Chemotherapy on Survival in Patients with Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine With or Without Erlotinib: The LAP07 Randomized Clinical Trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Kim, R.Y.; Christians, K.K.; Aldakkak, M.; Clarke, C.N.; George, B.; Kamgar, M.; Khan, A.H.; Kulkarni, N.; Hall, W.A.; Erickson, B.A.; et al. Total Neoadjuvant Therapy for Operable Pancreatic Cancer. Ann. Surg. Oncol. 2021, 28, 2246–2256. [Google Scholar] [CrossRef]
- Truty, M.J.; Kendrick, M.L.; Nagorney, D.M.; Smoot, R.L.; Cleary, S.P.; Graham, R.P.; Goenka, A.H.; Hallemeier, C.L.; Haddock, M.G.; Harmsen, W.S.; et al. Factors Predicting Response, Perioperative Outcomes, and Survival Following Total Neoadjuvant Therapy for Borderline/Locally Advanced Pancreatic Cancer. Ann. Surg. 2021, 273, 341–349. [Google Scholar] [CrossRef]
- Hayashi, T.; Nakamura, T.; Kimura, Y.; Yoshida, M.; Someya, M.; Kawakami, H.; Sakuhara, Y.; Katoh, N.; Takahashi, K.; Ambo, Y.; et al. Phase 2 Study of Neoadjuvant Treatment of Sequential S-1-Based Concurrent Chemoradiation Therapy Followed by Systemic Chemotherapy with Gemcitabine for Borderline Resectable Pancreatic Adenocarcinoma (HOPS-BR 01). Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 606–617. [Google Scholar] [CrossRef]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Clark, J.W.; Jiang, W.; Yeap, B.Y.; Drapek, L.C.; Ly, L.; Baglini, C.V.; Blaszkowsky, L.S.; et al. Total Neoadjuvant Therapy with FOLFIRINOX in Combination With Losartan Followed by Chemoradiotherapy for Locally Advanced Pancreatic Cancer: A Phase 2 Clinical Trial. JAMA Oncol. 2019, 5, 1020–1027. [Google Scholar] [CrossRef]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Jiang, W.; Yeap, B.Y.; Drapek, L.C.; Blaszkowsky, L.S.; Kwak, E.L.; Allen, J.N.; Clark, J.W.; et al. Total Neoadjuvant Therapy with FOLFIRINOX Followed by Individualized Chemoradiotherapy for Borderline Resectable Pancreatic Adenocarcinoma: A Phase 2 Clinical Trial. JAMA Oncol. 2018, 4, 963–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, H.; Akita, H.; Ioka, T.; Wada, H.; Tomokoni, A.; Asukai, K.; Ohue, M.; Yano, M.; Ishikawa, O. Phase I Trial Evaluating the Safety of Preoperative Gemcitabine/Nab-Paclitaxel with Concurrent Radiation Therapy for Borderline Resectable Pancreatic Cancer. Pancreas 2018, 47, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Grose, D.; McIntosh, D.; Jamieson, N.; Carter, R.; Dickson, E.; Chang, D.; Marashi, H.; Wilson, C.; Alfayez, M.; Kerr, A.; et al. The Role of Induction Chemotherapy + Chemoradiotherapy in Localised Pancreatic Cancer: Initial Experience in Scotland. J. Gastrointest. Oncol. 2017, 8, 683–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiore, M.; Ramella, S.; Valeri, S.; Caputo, D.; Floreno, B.; Trecca, P.; Trodella, L.E.; Trodella, L.; D’Angelillo, R.M.; Coppola, R. Phase II Study of Induction Chemotherapy Followed by Chemoradiotherapy in Patients with Borderline Resectable and Unresectable Locally Advanced Pancreatic Cancer. Sci. Rep. 2017, 7, 45845. [Google Scholar] [CrossRef] [Green Version]
- Abbott, D.E.; Tzeng, C.-W.D.; Merkow, R.P.; Cantor, S.B.; Chang, G.J.; Katz, M.H.; Bentrem, D.J.; Bilimoria, K.Y.; Crane, C.H.; Varadhachary, G.R.; et al. The Cost-Effectiveness of Neoadjuvant Chemoradiation Is Superior to a Surgery-First Approach in the Treatment of Pancreatic Head Adenocarcinoma. Ann. Surg. Oncol. 2013, 20 (Suppl. 3), S500–S508. [Google Scholar] [CrossRef]
- Denost, Q.; Laurent, C.; Adam, J.-P.; Capdepont, M.; Vendrely, V.; Collet, D.; Cunha, A.S. Pancreaticoduodenectomy Following Chemoradiotherapy for Locally Advanced Adenocarcinoma of the Pancreatic Head. HPB Oxf. 2013, 15, 716–723. [Google Scholar] [CrossRef] [Green Version]
- Habermehl, D.; Kessel, K.; Welzel, T.; Hof, H.; Abdollahi, A.; Bergmann, F.; Rieken, S.; Weitz, J.; Werner, J.; Schirmacher, P.; et al. Neoadjuvant Chemoradiation with Gemcitabine for Locally Advanced Pancreatic Cancer. Radiat. Oncol. 2012, 7, 28. [Google Scholar] [CrossRef] [Green Version]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Del Chiaro, M.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021, 19, 439–457. [Google Scholar] [CrossRef]
- Welsch, T.; Kleeff, J.; Friess, H. Molecular Pathogenesis of Pancreatic Cancer: Advances and Challenges. Curr. Mol. Med. 2007, 7, 504–521. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Ryan, D.P.; Hong, T.S.; Bardeesy, N. Pancreatic Adenocarcinoma. New Engl. J. Med. 2014, 371, 1039–1049. [Google Scholar] [CrossRef]
- He, J.; Ahuja, N.; Makary, M.A.; Cameron, J.L.; Eckhauser, F.E.; Choti, M.A.; Hruban, R.H.; Pawlik, T.M.; Wolfgang, C.L. 2564 Resected Periampullary Adenocarcinomas at a Single Institution: Trends over Three Decades. HPB Oxf. 2014, 16, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of Adjuvant Gemcitabine and Capecitabine with Gemcitabine Monotherapy in Patients with Resected Pancreatic Cancer (ESPAC-4): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Dunn, J.A.; Stocken, D.D.; Almond, J.; Link, K.; Beger, H.; Bassi, C.; Falconi, M.; Pederzoli, P.; Dervenis, C.; et al. Adjuvant Chemoradiotherapy and Chemotherapy in Resectable Pancreatic Cancer: A Randomised Controlled Trial. Lancet 2001, 358, 1576–1585. [Google Scholar] [CrossRef]
- Ioka, T.; Furuse, J.; Fukutomi, A.; Mizusawa, J.; Nakamura, S.; Hiraoka, N.; Ito, Y.; Katayama, H.; Ueno, M.; Ikeda, M.; et al. Randomized Phase II Study of Chemoradiotherapy with versus without Induction Chemotherapy for Locally Advanced Pancreatic Cancer: Japan Clinical Oncology Group Trial, JCOG1106. Jpn. J. Clin. Oncol. 2021, 51, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Trevisan, F.; Cabiddu, M.; Sgroi, G.; Bruschieri, L.; Rausa, E.; Ghidini, M.; Turati, L. Total Neoadjuvant Therapy in Rectal Cancer: A Systematic Review and Meta-Analysis of Treatment Outcomes. Ann. Surg. 2020, 271, 440–448. [Google Scholar] [CrossRef]
- Taghian, A.G.; Abi-Raad, R.; Assaad, S.I.; Casty, A.; Ancukiewicz, M.; Yeh, E.; Molokhia, P.; Attia, K.; Sullivan, T.; Kuter, I.; et al. Paclitaxel Decreases the Interstitial Fluid Pressure and Improves Oxygenation in Breast Cancers in Patients Treated with Neoadjuvant Chemotherapy: Clinical Implications. J. Clin. Oncol. 2005, 23, 1951–1961. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Grainger, J.; Harrison, M.; Ostler, P.; Makris, A. Neoadjuvant Chemotherapy Prior to Preoperative Chemoradiation or Radiation in Rectal Cancer: Should We Be More Cautious? Br. J. Cancer 2006, 94, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, S.; Rana, V.; Janjan, N.A.; Varadhachary, G.R.; Abbruzzese, J.L.; Das, P.; Delclos, M.E.; Gould, M.S.; Evans, D.B.; Wolff, R.A.; et al. Induction Chemotherapy Selects Patients with Locally Advanced, Unresectable Pancreatic Cancer for Optimal Benefit from Consolidative Chemoradiation Therapy. Cancer 2007, 110, 47–55. [Google Scholar] [CrossRef]
- Mayo, S.C.; Austin, D.F.; Sheppard, B.C.; Mori, M.; Shipley, D.K.; Billingsley, K.G. Adjuvant Therapy and Survival after Resection of Pancreatic Adenocarcinoma: A Population-Based Analysis. Cancer 2010, 116, 2932–2940. [Google Scholar] [CrossRef]
- Kalser, M.H.; Ellenberg, S.S. Pancreatic Cancer. Adjuvant Combined Radiation and Chemotherapy Following Curative Resection. Arch. Surg. 1985, 120, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Smeenk, H.G.; van Eijck, C.H.J.; Hop, W.C.; Erdmann, J.; Tran, K.C.K.; Debois, M.; van Cutsem, E.; van Dekken, H.; Klinkenbijl, J.H.; Jeekel, J. Long-Term Survival and Metastatic Pattern of Pancreatic and Periampullary Cancer after Adjuvant Chemoradiation or Observation: Long-Term Results of EORTC Trial 40891. Ann. Surg. 2007, 246, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Hurt, C.N.; Bridgewater, J.; Falk, S.; Cummins, S.; Wasan, H.; Crosby, T.; Jephcott, C.; Roy, R.; Radhakrishna, G.; et al. Gemcitabine-Based or Capecitabine-Based Chemoradiotherapy for Locally Advanced Pancreatic Cancer (SCALOP): A Multicentre, Randomised, Phase 2 Trial. Lancet Oncol. 2013, 14, 317–326. [Google Scholar] [CrossRef] [Green Version]
- Versteijne, E.; Vogel, J.A.; Besselink, M.G.; Busch, O.R.C.; Wilmink, J.W.; Daams, J.G.; van Eijck, C.H.J.; Groot Koerkamp, B.; Rasch, C.R.N.; van Tienhoven, G.; et al. Meta-Analysis Comparing Upfront Surgery with Neoadjuvant Treatment in Patients with Resectable or Borderline Resectable Pancreatic Cancer. Br. J. Surg. 2018, 105, 946–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References | Publication Year | Centre | Country | Study Design | Inclusion Period | No. of Patients |
|---|---|---|---|---|---|---|
| Kim et al. [18] | 2021 | Medical College of Wisconsin | USA | Retrospective | 2009–2019 | 89 |
| Truty et al. [19] | 2021 | Mayo Clinical College of Medicine | USA | Retrospective | 2010–2017 | 254 |
| Hayashi et al. [20] | 2019 | Hokkaido Pancreas Study Group (HOPS) | JAPAN | Prospective | 2013–2015 | 45 |
| Murphy et al. [21] | 2019 | Massachusetts General Hospital | USA | Prospective | 2013–2018 | 49 |
| Murphy et al. [22] | 2018 | Massachusetts General Hospital | USA | Prospective | 2012–2016 | 48 |
| Takahashi et al. [23] | 2018 | Osaka International Cancer Institute | JAPAN | Prospective | Not specified | 38 |
| Pietrasz et al. [14] | 2018 | Paul Brousse Hospital | FRANCE | Retrospective | 2010–2015 | 203 |
| Grose et al. [24] | 2017 | Beatson West of Scotland Cancer Centre | UK | Retrospective | 2012–2015 | 85 |
| Fiore et al. [25] | 2017 | Campus Bio-Medico University Rome | ITALY | Prospective | 2012–2015 | 41 |
| Abbott et al. [26] | 2013 | University of Cincinnati School of Medicine | USA | Retrospective | Not specified | 164 |
| Denost et al. [27] | 2012 | University Hospital Centre (CHU) Bordeaux | FRANCE | Retrospective | 2004–2009 | 111 |
| Habermehl et al. [28] | 2012 | University Hospital of Heidelberg | GERMANY | Retrospective | 2001–2010 | 215 |
| References | No. of Patients | Accurate Description of IC | Accurate Description of CRT | Accurate Description of Safety and Tolerance to IC + CRT | Accurate Description of Surgical Procedure | Newcastle–Ottawa Score | |||
|---|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Outcome | Score | ||||||
| Kim et al., 2021 [18] | 89 | Yes | Yes | No | Yes | **** | * | *** | 8 |
| Truty et al., 2021 [19] | 254 | Yes | Yes | Yes | Yes | *** | - | *** | 6 |
| Hayashi et al., 2019 [20] | 45 | Yes | Yes | No | Yes | *** | - | *** | 6 |
| Murphy et al., 2019 [21] | 49 | Yes | Yes | Yes | Yes | *** | - | *** | 6 |
| Murphy et al., 2018 [22] | 48 | Yes | Yes | Yes | Yes | *** | - | *** | 6 |
| Takahashi et al., 2018 [23] | 38 | Yes | Yes | Yes | Yes | *** | - | *** | 6 |
| Pietrasz et al. [14] | 203 | Yes | Yes | No | Yes | **** | * | *** | 8 |
| Grose et al., 2017 [24] | 85 | Yes | Yes | Yes | No | **** | * | *** | 8 |
| Fiore et al., 2017 [25] | 41 | Yes | Yes | Yes | No | **** | * | *** | 8 |
| Abbott et al., 2013 [26] | 164 | Yes | Yes | No | No | **** | * | *** | 8 |
| Denost et al., 2012 [27] | 111 | Yes | Yes | No | Yes | **** | * | *** | 8 |
| Habermehl et al., 2012 [28] | 215 | Yes | Yes | Yes | No | *** | - | *** | 6 |
| Induction Chemotherapy (IC) | Patients Received CRT after or before IC, N (%) | ChemoRadioTherapy (CRT) | Surgery after IC + CRT | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference, Year | Number of Patients, N | Classification of Tumor, N | Regimen, N (%) | Cycles, N | Completion of IC ***, N (%) | Grade 3 or Greater Toxicity ****, N (%) | PD during IC, N (%) | Regimen | Radiotherapy Dose | PD during CRT, N (%) | Patients Undergoing Pancreatic Resection after IC + CRT, N (%) | Patients Undergoing only Surgical Exploration, N (%) | |
| Kim et al., 2021 [18] | 89 | R 22, BR 67 | FOLFIRINOX 66 (74), Gem/Nab 17 (19) | 8 * | 64 (72) | Ns | 19 (21) | 86 (97) | Cap or Gem | 50.4 Gy in 28 fractions | 19 (22) | 64 (72) | Ns |
| Truty et al., 2021 [19] | 194 | LA 71, BR 123 | FOLFIRINOX 165 (85) or Gem/Nab 65 (34) | 6 ** | 71 (37) | 32 (14) | 25(10) | 194 (100) | Cap or 5FU or Gem | 50.4 Gy in 28 fractions | Ns | 194 (100) | 0 |
| Hayashi et al., 2019 [20] | 45 | BR 45 | Gem 45 (100) | 8 * | 24 (53,3) | Ns | 9 (25) | 43 (95,6) | S-1 | 50.4 Gy in 28 fractions | 4 (8) | 24 (53,3) | 1 (2) |
| Murphy et al., 2019 [21] | 49 | LA 49 | FOLFIRINOX 49 (100) | 8 * | 39 (80) | 25 (51) | 5 (10) | 45 (92) | Cap or 5FU | 50.4 Gy in 28 fractions or 25 GyE in 5GyE | 3 (6) | 34 (69) | 8 (16) |
| Murphy et al., 2018 [22] | 43 | BR 43 | FOLFIRINOX 43 (100) | 8 * | 34 (79) | 9 (19) | 2 (5) | 39 (90) | Cap or 5FU | 50.4 Gy in 28 fractions or 25 GyE in 5GyE | 3 (6) | 29 (67) | 4 (9) |
| Takahashi et al., 2018 [23] | 38 | BR 38 | Gem/Nab 38 (100) | 2 | 30 (78) | 1 (2) | 6 (15) | 30 (78) | Gem/Nab | 60 Gy in 25 fractions | 5 (17) | 24 (80) | Ns |
| Pietrasz et al. 2018 [14] | 102 | BR 49, LA 53 | FOLFIRINOX 102 (100) | 6 * | 24 (23,5) | Ns | Ns | 102 (100) | Cap or Gem | 49 to 59 Gy in 30 fractions | Ns | 102 (100) | 0 |
| Grose et al., 2017 [24] | 85 | BR 45, LA 40 | FOLFIRINOX 65 (76) | 6 * | 33 (50,8) | 7 (10,8) | 16 (24,6) | 33 (38,3) | Cap | 50.4 Gy in 28 fractions | Ns | 17 (51) | 2 (6) |
| Gem-Cap 20 (24) | 3 * | 14 (70) | 3 (10) | 6 (30) | |||||||||
| Fiore et al., 2017 [25] | 34 | LA 27, BR7 | Gem and Oxaliplatin 34 (100) | 4 * | 34 (100) | 3 (8) | 5 (14,7) | 27 (79) | Gem | 54 Gy (BRPC) or 59,4 Gy (LA) in 28 fractions | 5 (18,5) | 15 (55) | 4 (14) |
| Abbott et al., 2013 [26] | 164 | R 164 | Gem 164 (100) | 4 * | 164 (100) | Ns | Ns | 164 (100) | Gem | 30 Gy in 10 fractions | 18 (10) | 116 (71) | 12 (7) |
| Denost et al., 2012 [27] | 39 | LA 39 | Gem or GEMCIS 39 (100) | Ns | Ns | Ns | Ns | 39 (100) | 5FU | 45 Gy in 25 fractions | Ns | 39 (100) | 0 |
| Habermehl et al., 2012 [28] | 198 | LA 198 | Gem 198 (100) | Ns | Ns | Ns | 22 (11) | 198 (100) | Gem | 52,2 Gy (Intraoperative radiotherapy 15 Gy in 26 patients) | Ns | 51 (26) | 53 (28) |
| Pathological Outcomes | Surgical Outcomes | Long-Term Outcomes | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Reference | Patients Undergone Surgery after IC + CRT, N (%) | Type of Surgery, N (%) | Pathological Complete Response, N (%) | Regional Lymph Node Metastases, N (%) | Resection R0, N (%) | Major Complications after Surgery, N (%) | 90 Day Mortality, N (%) | DFS, Median (Months) | OS, Median (Months) |
| Kim et al., 2021 [18] | 64 (72) | PDC 53 (83) DP 6 (9) TP 5 (8) | 5 (8) | 25 (34) | 57 (89) | 36 (56) | Ns | Ns | Ns |
| Truty et al., 2021 [19] | 194 (100) | PDC 122 (63) TP 25 (13) | 0 | 39 (20) | 183 (94) | 69 (36) | 13 (6,7) | 23,5 | 51,1 |
| Hayashi et al., 2019 [20] | 24 (53,3) | PDC 19 DP 4 TP 1 | 0 | 6 (25) | 23 (95,8) | 6 (25) | Ns | 14,8 | 27,9 |
| Murphy et al., 2019 [21] | 34 (69) | Ns | 3 (9) | 9 (26) | 30 (88) | Ns | Ns | 21,3 | 33 |
| Murphy et al., 2018 [22] | 29 (67) | Ns | 0 | 20 (38) | 29 (100) | Ns | Ns | 48,6 | Ns |
| Takahashi et al., 2018 [23] | 24 (80) | PDC 12 DP 12 | 3 (12) | Ns | 23 (96) | 3 (12,5) | 0 | Ns | Ns |
| Pietrasz et al. 2018 [14] | 102 (100) | Ns | 22 (10,8) | 24 (23,5) | 169 (83,3) | Ns | Ns | 17.7 | 47.9 |
| Grose et al., 2017 [24] | 17 (51) | Ns | 3 (17) | 6 (35) | 12 (70,6) | Ns | Ns | Ns | Ns |
| Fiore et al., 2017 [25] | 15 (55) | Ns | 0 | Ns | 15 (100) | Ns | 0 | 35,2 | 37,6 |
| Abbott et al., 2013 [26] | 116 (71) | Ns | Ns | 65 (56) | 104 (90) | 27 (23) | 1 (1) | Ns | Ns |
| Denost et al., 2012 [27] | 39 (100) | PDC 39 (100) | Ns | 16 (41) | 33 (84,6) | 12 (30) | Ns | Ns | Ns |
| Habermehl et al., 2012 [28] | 51 (26) | Ns | Ns | Ns | 20 (39,2) | Ns | Ns | 10,8 | 10,8 |
| Classification of Patients | Patients Undergone Surgery after TNT | Regional Lymph Node Metastases, N (%) | Resection R0, N (%) | 1-Year OS | 2-Years OS | 1-Year DFS | 2-Years DFS |
|---|---|---|---|---|---|---|---|
| Resectable | 116 | 65 (56%) | 104 (90%) | ns | ns | ns | ns |
| Borderline resectable | 94 | 32 (34%) | 64 (68%) | 47 (88%) | 36 (67%) | 22 (76,5%) | 15 (54%) |
| Locally advanced | 124 | 45 (36%) | 83 (66%) | 97 (78%) | 68 (54%) | 86 (69%) | 40 (32%) |
| Pathological Outcomes | Surgical Outcomes | Long-Term Outcomes | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Patients Undergone Surgery after IC + CRT, N (%) | Patients Undergone Surgery after NAT | Pathological Complete Response, N (%) | Regional Lymph Node Metastases, N (%) | Resection R0, N (%) | Major Complications after Surgery, N (%) | 1-Year, 2-Year, 3-Year OS, Percentage | |||||
| TNT | NAT | TNT | NAT | TNT | NAT | TNT | NAT | TNT | NAT | |||
| Kim et al., 2021 [18] | 64 | 322 | 5 (8) | 13 (4) | 25 (34) | 122 (38) | 57 (89) | 275 (85) | 36 (56) | 189 (59) | 87,5%, 60%, Ns | 80%, 52%, 37% |
| Grose et al.,2017 [24] | 17 | 17 | 3 (17) | Ns | 6 (35) | 11 (64) | 12 (70,6) | 7 (47,6) | Ns | Ns | Ns | Ns |
| Pietrasz et al. 2018 [14] | 102 | 101 | 17 (16,7) | 5 (5) | 24 (23,5) | 52 (51,5) | 91 (89,2) | 78 (76,3) | Ns | Ns | 84%, 70%, 60% | 80%, 63%, 44% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Simoni, O.; Scarpa, M.; Soldà, C.; Bergamo, F.; Lonardi, S.; Fantin, A.; Pilati, P.; Gruppo, M. Could Total Neoadjuvant Therapy Followed by Surgical Resection Be the New Standard of Care in Pancreatic Cancer? A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 812. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030812
De Simoni O, Scarpa M, Soldà C, Bergamo F, Lonardi S, Fantin A, Pilati P, Gruppo M. Could Total Neoadjuvant Therapy Followed by Surgical Resection Be the New Standard of Care in Pancreatic Cancer? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(3):812. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030812
Chicago/Turabian StyleDe Simoni, Ottavia, Marco Scarpa, Caterina Soldà, Francesca Bergamo, Sara Lonardi, Alberto Fantin, Pierluigi Pilati, and Mario Gruppo. 2022. "Could Total Neoadjuvant Therapy Followed by Surgical Resection Be the New Standard of Care in Pancreatic Cancer? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 3: 812. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030812