
A Retrospective Digital Analysis of Contour Changing after Tooth Extraction with or without Using Less Traumatic Surgical Procedures

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design/Sample
- 18 years old or older;
- signed and informed consent form for data processing;
- single intercalate tooth extraction in the back area (bicuspid and molar teeth);
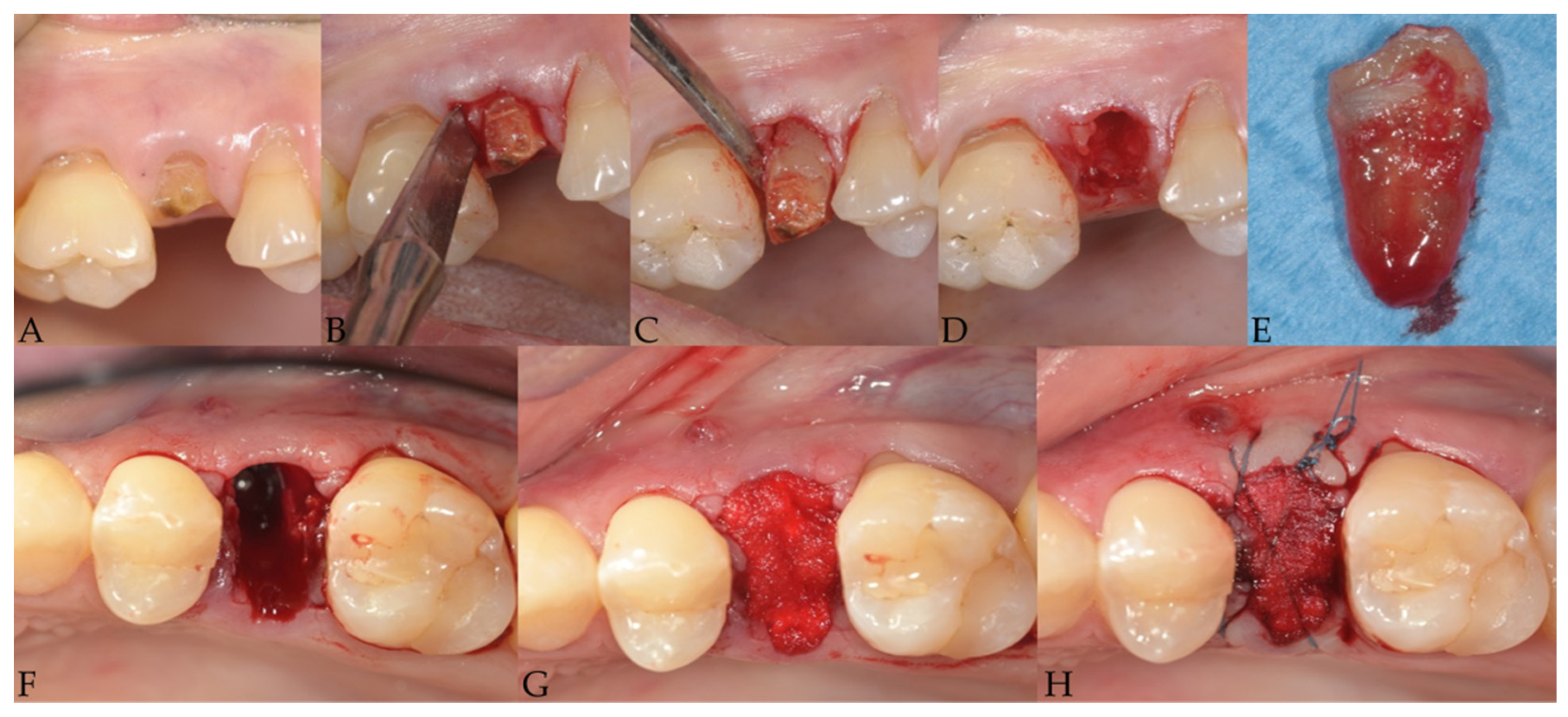
- presence of an uncorrupted dataset of two three-dimensional scans (file.stl) in the collected records, representing intraoperative views on just treated sites (acquired during tooth extraction surgery just after the filling of the alveolar socket with a sterile fast re-absorbable gelatin sponge) and on healed postsurgical areas (around 4 months later).
- history of systemic diseases contraindicating oral surgical intervention;
- any report for bisphosphonate therapy;
- history of bone resection or radiation therapy (as part of an oncological treatment);
- lost or corrupted .stl file of the virtual models.
2.2. Surgery Procedures
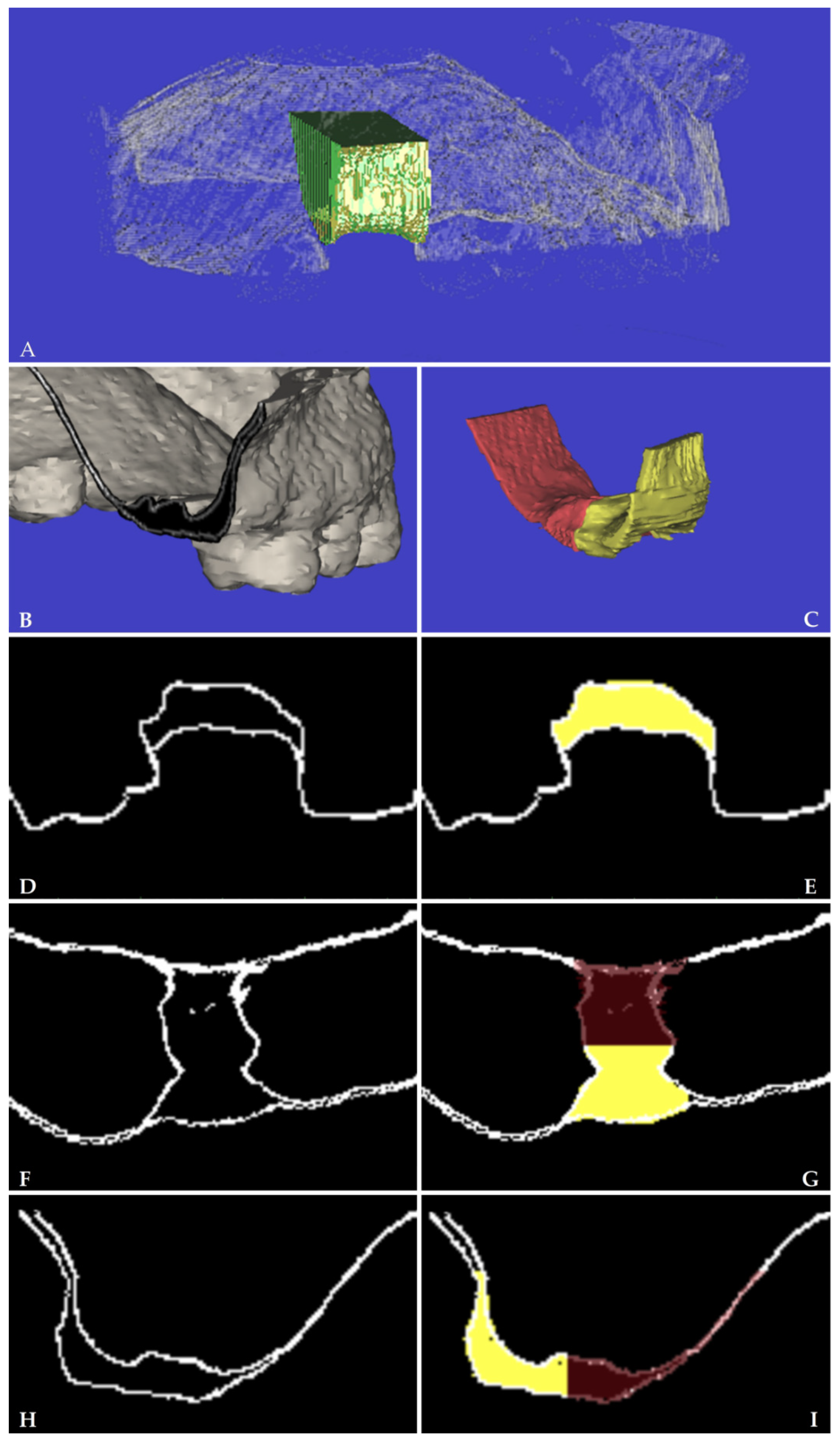
2.3. Outcomes
- test group “ltr”, less traumatic tooth extraction; control group “con”, conventional tooth extraction.
- Secondary predictor variable
- Tooth site: premolar versus molar; aspect: buccal versus palatal
2.4. Statistical Analysis
3. Results
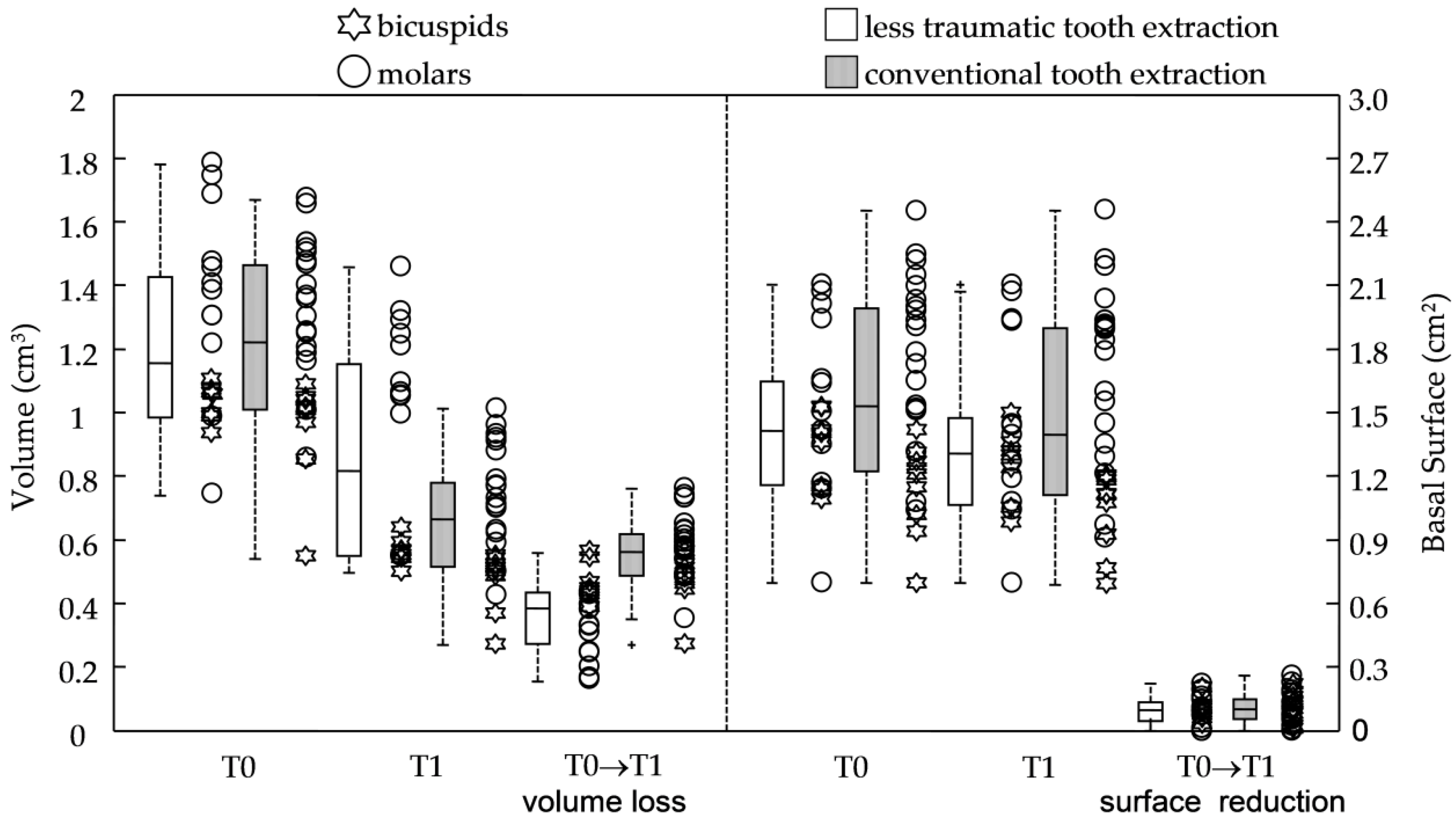
3.1. Primary Predictors: Procedures
3.2. Secondary Predictors: Tooth Aspect and Site
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LTETs | Less Traumatic Extraction Techniques |
| .stl | stereolithographic |
| VOI | Volume Of Interest |
| V | Volume of alveolar ridge |
| BS | Basal Surface |
| ltr | less traumatic tooth extraction group |
| con | conventional tooth extraction group |
Appendix A
Appendix B
References
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Van derWeijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef] [PubMed]
- Marconcini, S.; Denaro, M.; Cosola, S.; Gabriele, M.; Toti, P.; Mijiritsky, E.; Proietti, A.; Basolo, F.; Giammarinaro, E.; Covani, U. Myofibroblast Gene Expression Profile after Tooth Extraction in the Rabbit. Materials 2019, 12, 3697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.T.; Wilson, T.G., Jr.; Hämmerle, C.H. Immediate or early placement of implants following tooth extraction: Review of biologic basis, clinical procedures, and outcomes. Int. J. Oral Maxillofac. Implant. 2004, 19, 12–25. [Google Scholar]
- De Santis, D.; Sinigaglia, S.; Pancera, P.; Faccioni, P.; Portelli, M.; Luciano, U.; Cosola, S.; Penarrocha, D.; Bertossi, D.; Nocini, R.; et al. An overview of socket preservation. J. Biol. Regul. Homeost. Agents 2019, 33 (Suppl. 1), 55–59. [Google Scholar]
- Ten Heggeler, J.M.; Slot, D.E.; Van der Weijden, G.A. Effect of socket preservation therapies following tooth extraction in non-molar regions in humans: A systematic review. Clin. Oral Implant. Res. 2011, 22, 779–788. [Google Scholar] [CrossRef]
- Oghli, A.A.; Steveling, H. Ridge preservation following tooth extraction: A comparison between atraumatic extraction and socket seal surgery. Quintessence Int. 2010, 41, 605–609. [Google Scholar]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef]
- Quayle, A.A. Atraumatic removal of teeth and root fragments in dental implantology. Int. J. Oral Maxillofac. Implant. 1990, 5, 293–296. [Google Scholar]
- Babbush, C.A. A new atraumatic system for tooth removal and immediate implant restoration. Implant Dent. 2007, 16, 139–145. [Google Scholar] [CrossRef]
- Dym, H.; Weiss, A. Exodontia: Tips and techniques for better outcomes. Dent. Clin. 2012, 56, 245–266. [Google Scholar] [CrossRef]
- Hämmerle, C.H.; Chen, S.T.; Wilson, T.G., Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Niemiec, B.A. Extraction techniques. Top. Companion Anim. Med. 2008, 23, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Leblebicioglu, B.; Hegde, R.; Yildiz, V.O.; Tatakis, D.N. Immediate effects of tooth extraction on ridge integrity and dimensions. Clin. Oral Investig. 2015, 19, 1777–1784. [Google Scholar] [CrossRef] [PubMed]
- Fabrizio, F.; Grusovin, M.G.; Gavatta, M.; Vercellotti, T. Clinical efficacy of a new fully piezoelectric technique for third molar root extraction without using manual tools: A clinical randomized controlled study. Quintessence Int. 2020, 51, 406–414. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Martuscelli, R.; Guidetti, F.; Porzio, M.; Sbordone, L. Evaluation of volumetric dimensional changes in posterior extraction sites with and without ARP using a novel imaging device. Clin. Implant Dent. Relat. Res. 2017, 19, 1044–1053. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, V.; Rompen, E.; Lecloux, G.; Rues, S.; Schmitter, M.; Lambert, F. A methodological approach to assessing alveolar ridge preservation procedures in humans: Soft tissue profile. Clin. Oral Implant. Res. 2014, 25, 304–309. [Google Scholar] [CrossRef]
- Coomes, A.M.; Mealey, B.L.; Huynh-Ba, G.; Barboza-Arguello, C.; Moore, W.S.; Cochran, D.L. Buccal bone formation after flapless extraction: A randomized, controlled clinical trial comparing recombinant human bone morphogenetic protein 2/absorbable collagen carrier and collagen sponge alone. J. Periodontol. 2014, 85, 525–535. [Google Scholar] [CrossRef]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L. Relationship between the buccal bone plate thickness and the healing of postextraction sockets with/without ridge preservation. Int. J. Periodontics Restor. Dent. 2014, 34, 211–217. [Google Scholar] [CrossRef]
- Walker, C.J.; Prihoda, T.J.; Mealey, B.L.; Lasho, D.J.; Noujeim, M.; Huynh-Ba, G. Evaluation of Healing at Molar Extraction Sites With and Without Ridge Preservation: A Randomized Controlled Clinical Trial. J. Periodontol. 2017, 88, 241–249. [Google Scholar] [CrossRef]
- Saund, D.; Dietrich, T. Minimally-invasive tooth extraction: Doorknobs and strings revisited! Dent. Updat. 2013, 40, 325–326. [Google Scholar] [CrossRef] [Green Version]
- Crespi, R.; Capparè, P.; Gherlone, E.F. Electrical mallet in implants placed in fresh extraction sockets with simultaneous osteotome sinus floor elevation. Int. J. Oral Maxillofac. Implant. 2013, 28, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Bruschi, G.B.; Capparé, P.; Gherlone, E. The utility of the electric mallet. J. Craniofac. Surg. 2014, 25, 793–795. [Google Scholar] [CrossRef]
- Michelinakis, G.; Apostolakis, D.; Kamposiora, P.; Papavasiliou, G.; Özcan, M. The direct digital workflow in fixed implant prosthodontics: A narrative review. BMC Oral Health 2021, 21, 37. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, R.; Galli, M.; Chen, Z.; Mendonça, G.; Meirelles, L.; Wang, H.L.; Chan, H.L. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: A systematic review. Clin. Oral Investig. 2021, 25, 6517–6531. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Toti, P.; Menchini-Fabris, G.B.; Derchi, G.; Marconcini, S.; Covani, U. Extra oral digital scanning and imaging superimposition for volume analysis of bone remodeling after tooth extraction with and without 2 types of particulate porcine mineral insertion: A randomized controlled trial. Clin. Implant Dent. Relat. Res. 2017, 19, 750–759. [Google Scholar] [CrossRef]
- Menchini-Fabris, G.B.; Toti, P.; Crespi, G.; Covani, U.; Furlotti, L.; Crespi, R. Effect of Different Timings of Implant Insertion on the Bone Remodeling Volume around Patients’ Maxillary Single Implants: A 2–3 Years Follow-Up. Int. J. Environ. Res. Public Health 2020, 17, 6790. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Fabris, G.B.M.; Crespi, G.; Toti, P.; Marconcini, S.; Covani, U. Effects of different loading protocols on the bone remodeling volume of immediate maxillary single implants: A 2- to 3-year follow-up. Int. J. Oral Maxillofac. Implant. 2019, 34, 953–962. [Google Scholar] [CrossRef]
- Herrmann, I.; Lekholm, U.; Holm, S.; Kultje, C. Evaluation of patient and implant characteristics as potential prognostic factors for oral implant failures. Int. J. Oral Maxillofac. Implant. 2005, 20, 220–230. [Google Scholar]
- Regev, E.; Lustmann, J.; Nashef, R. Atraumatic teeth extraction in bisphosphonate-treated patients. J. Oral Maxillofac. Surg. 2008, 66, 1157–1161. [Google Scholar] [CrossRef]
- Muska, E.; Walter, C.; Knight, A.; Taneja, P.; Bulsara, Y.; Hahn, M.; Desai, M.; Dietrich, T. Atraumatic vertical tooth extraction: A proof of principle clinical study of a novel system. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Nevins, M.; Camelo, M.; De Paoli, S.; Friedland, B.; Schenk, R.K.; Parma-Benfenati, S.; Simion, M.; Tinti, C.; Wagenberg, B. A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots. Int. J. Periodontics Restor. Dent. 2006, 26, 19–29. [Google Scholar] [CrossRef]
- Moya-Villaescusa, M.J.; Sánchez-Pérez, A. Measurement of ridge alterations following tooth removal: A radiographic study in humans. Clin. Oral Implant. Res. 2010, 21, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Aldini, N.N.; Fini, M.; Giardino, R.; Calvo Guirado, J.L.; Covani, U. Xenograft versus extraction alone for ridge preservation after tooth removal: A clinical and histomorphometric study. J. Periodontol. 2008, 79, 1370–1377. [Google Scholar] [CrossRef]
- Araújo, M.G.; da Silva, J.C.C.; de Mendonça, A.F.; Lindhe, J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin. Oral Implant. Res. 2015, 26, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Jambhekar, S.; Kernen, F.; Bidra, A.S. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: A systematic review of randomized controlled clinical trials. J. Prosthet. Dent. 2015, 113, 371–382. [Google Scholar] [CrossRef]
- Iorio-Siciliano, V.; Ramaglia, L.; Blasi, A.; Bucci, P.; Nuzzolo, P.; Riccitiello, F.; Nicolò, M. Dimensional changes following alveolar ridge preservation in the posterior area using bovine-derived xenografts and collagen membrane compared to spontaneous healing: A 6-month randomized controlled clinical trial. Clin. Oral Investig. 2020, 24, 1013–1023. [Google Scholar] [CrossRef]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implant. Res. 2013, 24, 1231–1237. [Google Scholar] [CrossRef]
- Tellisi, N.; Ashammakhi, N.A.; Billi, F.; Kaarela, O. Three Dimensional Printed Bone Implants in the Clinic. J. Craniofac. Surg. 2018, 29, 2363–2367. [Google Scholar] [CrossRef]
- Wegmüller, L.; Halbeisen, F.; Sharma, N.; Kühl, S.; Thieringer, F.M. Consumer vs. High-End 3D Printers for Guided Implant Surgery—An In Vitro Accuracy Assessment Study of Different 3D Printing Technologies. J. Clin. Med. 2021, 10, 4894. [Google Scholar] [CrossRef]
- Thurzo, A.; Kociš, F.; Novák, B.; Czako, L.; Varga, I. Three-Dimensional Modeling and 3D Printing of Biocompatible Orthodontic Power-Arm Design with Clinical Application. Appl. Sci. 2021, 11, 9693. [Google Scholar] [CrossRef]
- Heinemann, F.; Hasan, I.; Kunert-Keil, C.; Götz, W.; Gedrange, T.; Spassov, A.; Schweppe, J.; Gredes, T. Experimental and histological investigations of the bone using two different oscillating osteotomy techniques compared with conventional rotary osteotomy. Ann. Anat. 2012, 194, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, D.E.; Geminiani, A.; Zahavi, T.; Ercoli, C. Sonosurgery for atraumatic tooth extraction: A clinical report. J. Prosthet. Dent. 2012, 108, 339–343. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | Less Traumatic Tooth Extraction (ltr) | Conventional Tooth Extraction (con) | pF ltr vs. con | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| sample size | 20 | 28 | - | |||||||
| genders F/M | 12/8 | 15/13 | 0.7710 | |||||||
| Ratio Bd/Mr | 8/12 | 9/19 | 0.7603 | |||||||
| Smoke Y/N | 2/18 | 2/26 | 1.0000 | |||||||
| age (range) | 53.4 ± 8.2 (41.0–70.0) | 46.0 ± 10.9 (25.1–63.7) | - | |||||||
| swelling Y/N | 1/19 | 2/26 | 1.0000 | |||||||
| primary predictor: experimental groups | ||||||||||
| N = 20 | pWp times | N = 28 | pWp times | pWu ltr vs. con | ltr vs. con | |||||
| Time X | T0 | T1 | T0 vs. T1 | T0 | T1 | T0 vs. T1 | T0 | T1 | sample size | power |
| (cm3) | 1.22 ± 0.29 | 0.87 ± 0.34 | <0.0001 | 1.22 ± 0.27 | 0.66 ± 0.19 | <0.0001 | 0.9084 | 0.0346 | ||
| pSW (SW) | 0.2156 | 0.0031 | 0.4917 | 0.5950 | ||||||
| BS(cm2) | 1.47 ± 0.37 | 1.37 ± 0.38 | <0.0001 | 1.59 ± 0.47 | 1.49 ± 0.49 | <0.0001 | 0.4207 | 0.6157 | ||
| pSW (SW) | 0.3829 | 0.0983 | 0.5656 | 0.2511 | ||||||
| (cm3) | −0.36 ± 0.12 | −0.56 ± 0.11 | <0.0001 | 17 | 1.00 | |||||
| pSW (SW) | 0.3050 | 0.3042 | ||||||||
| −31.3 ± 13.3 | −46.2 ± 5.8 | 0.0001 | 21 | 0.99 | ||||||
| pSW (SW) | 0.0472 | 0.5962 | ||||||||
| (cm2) | −0.10 ± 0.07 | −0.10 ± 0.07 | 0.7458 | N.D | 0.00 | |||||
| pSW (SW) | 0.3581 | 0.3531 | ||||||||
| −6.8 ± 4.5 | −7.2 ± 5.4 | 0.9583 | 7807 | 0.01 | ||||||
| pSW (SW) | 0.0909 | 0.1936 | ||||||||
| Procedure | Less Traumatic Tooth Extraction (ltr) | Conventional Tooth Extraction (con) | |||||
|---|---|---|---|---|---|---|---|
| Outcome Variables | vs. | ||||||
| correlation coefficient (rs) | 0.3179 | 0.0188 | 0.4664 | −0.7588 | −0.7122 | 0.4412 | |
| significance (two-tailed) | 0.1720 | 0.9373 | 0.0313 | <0.0001 | <0.0001 | 0.0188 | |
| correlation coefficient (rs) | 0.1695 | 0.1061 | 0.1203 | 0.2436 | 0.2573 | −0.3038 | |
| significance (two-tailed) | 0.4750 | 0.6562 | 0.6133 | 0.2115 | 0.1863 | 0.1160 | |
| Group | Less Traumatic Tooth Extraction (ltr) | Conventional Tooth Extraction (con) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| secondary predictor: buccal | ||||||||||
| N = 20 | pWp Times | N = 28 | pWp Times | pWu ltr vs. con | ltr vs. con | |||||
| Time X | T0 | T1 | T0 vs. T1 | T0 | T1 | T0 vs. T1 | T0 | T1 | sample Size | power |
| (cm3) | 0.52 ± 0.15 | 0.35 ± 0.15 | <0.0001 | 0.51 ± 0.14 | 0.24 ± 0.09 | <0.0001 | 0.9084 | 0.0196 | ||
| pSW (SW) | 0.1979 | 0.0434 | 0.2889 | 0.2471 | ||||||
| BS(cm2) | 0.58 ± 0.14 | 0.53 ± 0.13 | 0.0003 | 0.65 ± 0.21 | 0.60 ± 0.21 | <0.0001 | 0.2415 | 0.2499 | ||
| pSW (SW) | 0.9000 | 0.7803 | 0.1869 | 0.1184 | ||||||
| (cm3) | −0.17 ± 0.05 | −0.26 ± 0.07 | <0.0001 | 24 | 0.97 | |||||
| pSW (SW) | 0.6222 | 0.1246 | ||||||||
| −34.4 ± 13.1 | −52.8 ± 7.3 | <0.0001 | 150 | 0.22 | ||||||
| pSW (SW) | 0.8268 | 0.8452 | ||||||||
| (cm2) | −0.05 ± 0.04 | −0.05 ± 0.04 | 0.6444 | N.D | 0.00 | |||||
| pSW (SW) | 0.1914 | 0.0143 | ||||||||
| −8.6 ± 6.7 | −7.8 ± 6.4 | 0.6671 | 3268 | 0.01 | ||||||
| pSW (SW) | 0.2789 | 0.0456 | ||||||||
| secondary predictor:palatal | ||||||||||
| N = 20 | pWp times | N = 28 | pWp times | pWu ltr vs. con | ltr vs. con | |||||
| Time X | T0 | T1 | T0 vs. T1 | T0 | T1 | T0 vs. T1 | T0 | T1 | sample size | power |
| (cm3) | 0.71 ± 0.17 | 0.52 ± 0.19 | <0.0001 | 0.71 ± 0.16 | 0.42 ± 0.13 | <0.0001 | 0.9666 | 0.1549 | ||
| pSW (SW) | 0.0826 | 0.0598 | 0.1458 | 0.9979 | ||||||
| BS(cm2) | 0.89 ± 0.30 | 0.84 ± 0.32 | 0.0002 | 0.94 ± 0.29 | 0.89 ± 0.30 | <0.0001 | 0.4771 | 0.6605 | ||
| pSW (SW) | 0.1706 | 0.0687 | 0.4612 | 0.2866 | ||||||
| (cm3) | −0.20 ± 0.10 | −0.29 ± 0.08 | 0.0014 | 48 | 0.72 | |||||
| pSW (SW) | 0.5916 | 0.3528 | ||||||||
| −28.6 ± 15.1 | −41.5 ± 8.4 | 0.0046 | 149 | 0.22 | ||||||
| pSW (SW) | 0.0289 | 0.7460 | ||||||||
| (cm2) | −0.04 ± 0.04 | −0.06 ± 0.05 | 0.3270 | 261 | 0.11 | |||||
| pSW (SW) | 0.0089 | 0.0129 | ||||||||
| −5.6 ± 5.2 | −6.7 ± 6.1 | 0.5203 | 1338 | 0.02 | ||||||
| pSW (SW) | 0.0021 | 0.0085 | ||||||||
| pWp between buccal and palatal | ||||||||||
| Time X | T0 | T1 | T0 | T1 | ||||||
| (cm3) | 0.0003 | 0.0001 | <0.0001 | <0.0001 | ||||||
| BS(cm2) | 0.0002 | 0.0001 | <0.0001 | <0.0001 | ||||||
| (cm3) | 0.3134 | 0.0855 | ||||||||
| 0.0206 | <0.0001 | |||||||||
| (cm2) | 0.3812 | 0.2584 | ||||||||
| 0.1024 | 0.6567 | |||||||||
| secondary predictor: bicuspids | ||||||||||
| N = 8 | pWp times | N = 9 | pWp times | pWu ltr vs. con | ltr vs. con | |||||
| Time X | T0 | T1 | T0 vs. T1 | T0 | T1 | T0 vs. T1 | T0 | T1 | sample size | power |
| (cm3) | 1.02 ± 0.06 | 0.56 ± 0.04 | 0.0078 | 0.95 ± 0.17 | 0.47 ± 0.09 | 0.0039 | 0.4650 | 0.0058 | ||
| pSW (SW) | 0.6037 | 0.3417 | 0.0030 | 0.0090 | ||||||
| BS(cm2) | 1.33 ± 0.18 | 1.23 ± 0.18 | 0.0078 | 1.14 ± 0.22 | 1.03 ± 0.19 | 0.0039 | 0.1455 | 0.0879 | ||
| pSW (SW) | 0.1687 | 0.5479 | 0.5263 | 0.0577 | ||||||
| (cm3) | −0.46 ± 0.06 | −0.47 ± 0.08 | 0.3203 | 2597 | 0.01 | |||||
| pSW (SW) | 0.2554 | 0.0134 | ||||||||
| −44.9 ± 4.2 | −50.0 ± 3.4 | 0.0152 | 29 | 0.51 | ||||||
| pSW (SW) | 0.3197 | 0.3687 | ||||||||
| (cm2) | −0.10 ± 0.05 | −0.11 ± 0.07 | 0.6058 | 1926 | 0.01 | |||||
| pSW (SW) | 0.2949 | 0.8733 | ||||||||
| −7.7 ± 3.5 | −9.7 ± 5.8 | 0.4234 | 301 | 0.04 | ||||||
| pSW (SW) | 0.8929 | 0.7720 | ||||||||
| secondary predictor: molars | ||||||||||
| N = 12 | pWp times | N = 19 | pWp times | pWu ltr vs. con | ltr vs. con | |||||
| Time X | T0 | T1 | T0 vs. T1 | T0 | T1 | T0 vs. T1 | T0 | T1 | sample size | power |
| (cm3) | 1.37 ± 0.30 | 1.07 ± 0.28 | 0.0005 | 1.35 ± 0.21 | 0.75 ± 0.16 | 0.0001 | 0.7000 | 0.0015 | ||
| pSW (SW) | 0.5803 | 0.0831 | 0.6063 | 0.7979 | ||||||
| BS(cm2) | 1.56 ± 0.43 | 1.47 ± 0.45 | 0.0039 | 1.80 ± 0.39 | 1.71 ± 0.42 | 0.0003 | 0.1618 | 0.2647 | ||
| pSW (SW) | 0.5858 | 0.4003 | 0.6182 | 0.6248 | ||||||
| (cm3) | −0.30 ± 0.10 | −0.59 ± 0.10 | <0.0001 | 6 | 1.00 | |||||
| pSW (SW) | 0.3988 | 0.3843 | ||||||||
| −22.3 ± 8.4 | −44.3 ± 5.8 | <0.0001 | 5 | 1.00 | ||||||
| pSW (SW) | 0.0282 | 0.6582 | ||||||||
| (cm2) | −0.09 ± 0.08 | −0.10 ± 0.07 | 0.8233 | 2726 | 0.01 | |||||
| pSW (SW) | 0.2942 | 0.3087 | ||||||||
| −6.2 ± 5.2 | −6.0 ± 4.9 | 0.9838 | 31268 | 0.01 | ||||||
| pSW (SW) | 0.0934 | 0.1476 | ||||||||
| pWu between bicuspids and molars | ||||||||||
| Time X | T0 | T1 | T0 | T1 | ||||||
| (cm3) | 0.0096 | 0.0048 | 0.0004 | 0.0004 | ||||||
| BS(cm2) | 0.1425 | 0.2316 | 0.0004 | 0.0004 | ||||||
| (cm3) | 0.0010 | 0.0025 | ||||||||
| 0.0008 | 0.0063 | |||||||||
| (cm2) | 0.6712 | 0.4029 | ||||||||
| 0.5118 | 0.1045 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menchini-Fabris, G.B.; Toti, P.; Crespi, R.; Crespi, G.; Cosola, S.; Covani, U. A Retrospective Digital Analysis of Contour Changing after Tooth Extraction with or without Using Less Traumatic Surgical Procedures. J. Clin. Med. 2022, 11, 922. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11040922
Menchini-Fabris GB, Toti P, Crespi R, Crespi G, Cosola S, Covani U. A Retrospective Digital Analysis of Contour Changing after Tooth Extraction with or without Using Less Traumatic Surgical Procedures. Journal of Clinical Medicine. 2022; 11(4):922. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11040922
Chicago/Turabian StyleMenchini-Fabris, Giovanni Battista, Paolo Toti, Roberto Crespi, Giovanni Crespi, Saverio Cosola, and Ugo Covani. 2022. "A Retrospective Digital Analysis of Contour Changing after Tooth Extraction with or without Using Less Traumatic Surgical Procedures" Journal of Clinical Medicine 11, no. 4: 922. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11040922